
Designing a National Veterinary Prescribing Champion Programme for Welsh Veterinary Practices: The Arwain Vet Cymru Project


Abstract
1. Introduction
Aim and Objectives
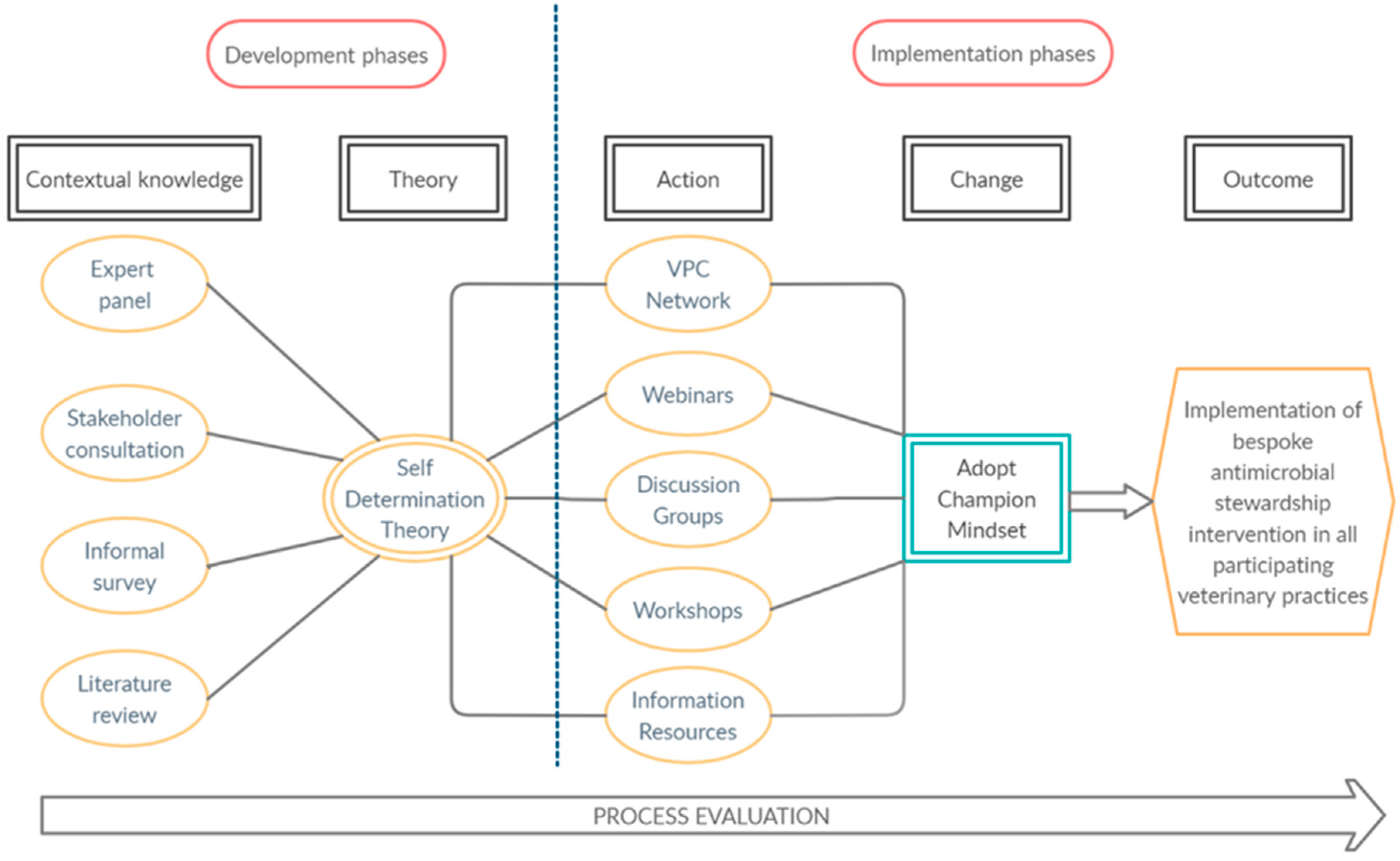
- The process through which this national AMS scheme was appropriately contextualised, involving the integration of complementary knowledge pathways in the development of intervention goals;
- How intervention goals were subsequently grounded within a theoretical framework, by identifying operational SDT conditions and associated guiding principles relevant and applicable to VPC participation; and
- How the individual components of the AVC programme can lead to improved prescribing practice.
2. Methods
2.1. Study Setting
2.2. Theoretical Basis
2.3. Engagement through Key Collaborators
2.4. Designing a National Stewardship Programme
2.4.1. Phase One: Contextual Knowledge
2.4.2. Phase Two: Integrating Theory
3. Results
3.1. Participation of VPCs
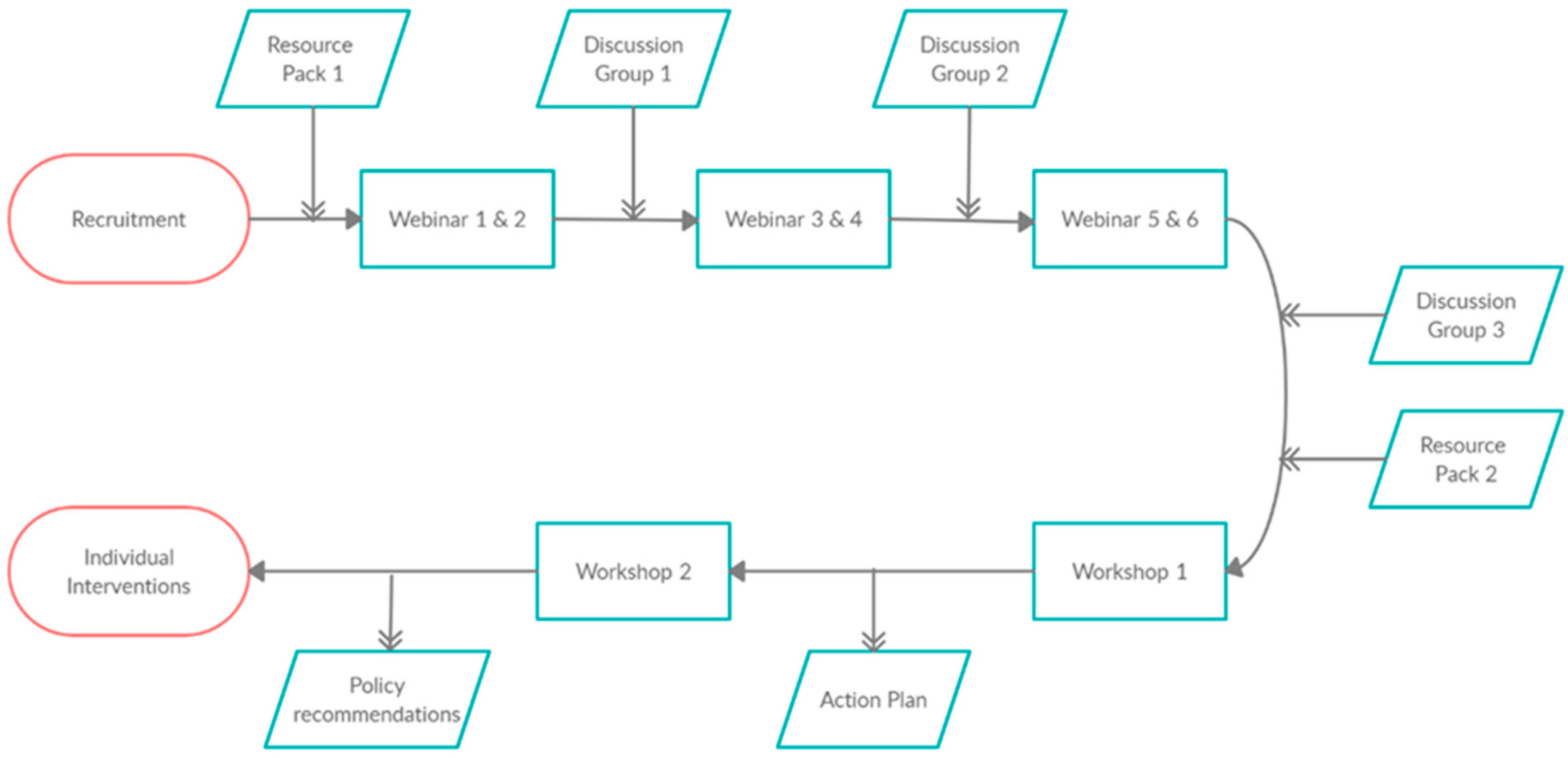
3.2. Defining the AVC Intervention Structure
- -
- Recruit and train one VPC from each farm animal veterinary practice in Wales.
- -
- Improve VPCs’ knowledge of AMS, the evidence base for prescribing decisions and the evidence base for legal and regulatory frameworks, human behaviour change, and species-specific considerations.
- -
- Foster a sense of group identity as well as of community and collaboration between Champions.
- -
- Encourage Champions to disseminate AMS messages within their practices.
- -
- Facilitate the autonomous development, by each individual participant, of individual practical, fit-for-purpose stewardship interventions at each participating practice.
3.3. Enactment of the AVC Network: Combining Intervention Goals and Theoretical Drivers
3.4. Webinars
3.5. Discussion Groups
3.6. Workshops
3.6.1. Stewardship Intervention Design Workshop
- -
- Reorganise the practice veterinary medicine dispensary to make certain antimicrobials more difficult to reach and/or more easily identified as second or third choice.
- -
- Schedule training and improve communication with veterinary reception and dispensing staff at the practice to ensure all staff members are delivering a unified message around antimicrobial prescribing and dispensing.
- -
- Begin to benchmark antimicrobial use among practice farms and include discussion of antimicrobial use in annual herd or flock health planning.
- -
- Introduce on-farm medicine cupboard “health checks” into the annual herd or flock health planning.
3.6.2. Policy Workshop
3.7. Stewardship Intervention Implementation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Antimicrobial Resistance: A Manual for Developing National Action Plans; Version 1; WHO: Geneve, Switzerland, 2016. Available online: https://apps.who.int/iris/handle/10665/2044702016 (accessed on 20 October 2020).
- World Health Organisation. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneve, Switzerland, 2015. Available online: http://www.who.int/iris/handle/10665/193736 (accessed on 20 October 2020).
- O’Neill, J. Tackling Drug Resistant Infections Globally: Final Report and Recommendations. The Review on Antimicrobial Resistance; Government of the United Kingdom: London, UK, 2016.
- Davey, P.; Peden, C.; Charani, E.; Marwick, C.; Michie, S. Time for action-Improving the design and reporting of behaviour change interventions for antimicrobial stewardship in hospitals: Early findings from a systematic review. Int. J. Antimicrob. Agents 2015, 45, 203–212. [Google Scholar] [CrossRef]
- Johnson, A.P.; Ashiru-Oredope, D.; Beech, E. Antibiotic Stewardship Initiatives as Part of the UK 5-Year Antimicrobial Resistance Strategy. Antibiotics 2015, 4, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Ashiru-Oredope, D.; Doble, A.; Akpan, M.R.; Hansraj, S.; Shebl, N.A.; Ahmad, R.; Hopkins, S. Antimicrobial Stewardship Programmes in Community Healthcare Organisations in England: A Cross-Sectional Survey to Assess Implementation of Programmes and National Toolkits. Antibiotics 2018, 7, 97. [Google Scholar] [CrossRef]
- Howard, P.; Pulcini, C.; Levy Hara, G.; West, R.M.; Gould, I.M.; Harbarth, S.; Nathwani, D. An international cross-sectional survey of antimicrobial stewardship programmes in hospitals. J. Antimicrob. Chemother. 2015, 70, 1245–1255. [Google Scholar] [CrossRef] [PubMed]
- Hardefeldt, L.Y.; Gilkerson, J.R.; Billman-Jacobe, H.; Stevenson, M.A.; Thursky, K.; Bailey, K.E.; Browning, G.F. Barriers to and enablers of implementing antimicrobial stewardship programs in veterinary practices. J. Vet. Intern. Med. 2018, 32, 1092–1099. [Google Scholar] [CrossRef] [PubMed]
- UK-VARSS. Veterinary Antibiotic Resistance and Sales Surveillance Report (UK-VARSS 2019); Addlestone Veterinary Medicines Directorate: Addlestone, UK, 2020. [Google Scholar]
- RUMA. Targets Task Force Report 2020 Responsible Use of Antibiotics in UK Farming Progress against 2020 Targets New Targets 2021–2024. Available online: https://www.ruma.org.uk/wp-content/uploads/2020/11/RUMA-Targets-Task-Force-Report-2020_download.pdf (accessed on 20 October 2020).
- Welsh Government. Antimicrobial Resistance in Animals and the Environment: Five Year Implementation Plan for Wales 2019–2024; Welsh Government: Cardiff, UK, 2019.
- HM Government. Tackling antimicrobial resistance 2019–2024: The UK’s 5-Year National Action Plan; HM Government: London, UK, 2019.
- Government of Wales Act 2006, Schedule 7. Available online: https://www.legislation.gov.uk/ukpga/2006/32/contents (accessed on 20 October 2020).
- Welsh Government. Agriculture in Wales; Welsh Government: Cardiff, UK, 2019.
- Schweitzer, V.A.; van Werkhoven, C.H.; Rodriguez Bano, J.; Bielicki, J.; Harbarth, S.; Hulscher, M.; Huttner, B.; Islam, J.; Little, P.; Pulcini, C.; et al. Optimizing design of research to evaluate antibiotic stewardship interventions: Consensus recommendations of a multinational working group. Clin. Microbiol. Infect. 2020, 26, 41–50. [Google Scholar] [CrossRef]
- MRC. Developing and Evaluating Complex Interventions: New Guidance; Medical Research Council: London, UK, 2019.
- Colquhoun, H.L.; Squires, J.E.; Kolehmainen, N.; Fraser, C.; Grimshaw, J.M. Methods for designing interventions to change healthcare professionals’ behaviour: A systematic review. Implement. Sci. 2017, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- O’Cathain, A.; Croot, L.; Duncan, E.; Rousseau, N.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019, 9, e029954. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “What” and “Why” of Goal Pursuits: Human Needs and the Self-Determination of Behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Royal College of Veterinary Surgeons (2020) Code of Professional Conduct for Veterinary Surgeons. Available online: https://www.rcvs.org.uk/setting-standards/advice-and-guidance/code-of-professional-conduct-for-veterinary-surgeons/ (accessed on 20 October 2020).
- Rees, G.M.; Barrett, D.C.; Buller, H.; Mills, H.L.; Reyher, K.K. Storage of prescription veterinary medicines on UK dairy farms: A cross-sectional study. Vet. Rec. 2018, 184, 153. [Google Scholar] [CrossRef] [PubMed]
- Rees, G.M.; Barrett, D.C.; Sánchez-Vizcaíno, F.; Reyher, K.K. Measuring antimicrobial use on dairy farms: A method comparison cohort study. J. Dairy Sci. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Van den Broeck, A.; Ferris, D.L.; Chang, C.-H.; Rosen, C.C. A Review of Self-Determination Theory’s Basic Psychological Needs at Work. J. Manag. 2016, 42, 1195–1229. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Intrinsic and Extrinsic Motivations: Classic Definitions and New Directions. Contemp. Educ. Psychol. 2000, 25, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and wellbeing. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Silva, M.N.; Marques, M.M.; Teixeira, P.J. Testing theory in practice: The example of self-determination theory-based interventions. Eur. Health Psychol. 2014, 16, 171–180. [Google Scholar]
- Erskine, R.G. Attunement and involvement: Therapeutic responses to relational needs. In Relational Patterns, Therapeutic Presence Concepts and Practice of Integrative Psychotherapy; Routledge: London, UK, 2015; Chapter 3. [Google Scholar]
- Kossak, M.S. Therapeutic attunement: A transpersonal view of expressive arts therapy. Arts Psychother. 2009, 36, 13–18. [Google Scholar] [CrossRef]
- Doran, G.T. There’s a S.M.A.R.T. way to write management’s goals and objectives. Manag. Rev. 1981, 70, 35–36. [Google Scholar]
- Gozdzielewska, L.; King, C.; Flowers, P.; Mellor, D.; Dunlop, P.; Price, L. Scoping review of approaches for improving antimicrobial stewardship in livestock farmers and veterinarians. Prev. Vet. Med. 2020, 180, 105025. [Google Scholar] [CrossRef]
- Golding, S.E.; Ogden, J.; Higgins, H.M. Shared Goals, Different Barriers: A Qualitative Study of UK Veterinarians’ and Farmers’ Beliefs About Antimicrobial Resistance and Stewardship. Front. Vet. Sci. 2019, 6, 132. [Google Scholar] [CrossRef]
- Gender Statistics about Veterinary Surgeons in the UK. Available online: https://www.vetfutures.org.uk/download/gender-statistics-about-veterinary-surgeons-in-the-uk/ (accessed on 20 October 2020).
- Fletcher, A.; Jamal, F.; Moore, G.; Evans, R.E.; Murphy, S.; Bonell, C. Realist complex intervention science: Applying realist principles across all phases of the Medical Research Council framework for developing and evaluating complex interventions. Evaluation 2016, 22, 286–303. [Google Scholar] [CrossRef]
- Michie, S.; Atkins, L.; Gainforth, H.L. Changing Behaviour to Improve Clinical Practice and Policy. In Novos Desafios, Novas Competências: Contributos Atuais da Psicologia; Axiom: Stepney, Australia, 2016; pp. 41–60. [Google Scholar]
- Children’s Health Queensland. Antibiotic Champion Network. Available online: https://www.childrens.health.qld.gov.au/chq/health-professionals/antimicrobial-stewardship/antibiotic-champion-network/2020 (accessed on 20 October 2020).
- BSAC. Healthcare Students—Antibiotic Guardian Champion Badge. Available online: https://antibioticguardian.com/Resources/healthcare-students-ag-champion-badge/2020 (accessed on 20 October 2020).
- College of Medicine and Integrated Health. National Social Prescribing Student Champion Scheme the Social Prescribing Network, the College of Medicine, and NHS England. Available online: https://collegeofmedicine.org.uk/national-social-prescribing-student-champion-scheme-the-social-prescribing-network-the-college-of-medicine-and-nhs-england/ (accessed on 20 October 2020).
- Diabetes UK. The Clinical Champions Programme. Available online: https://www.diabetes.org.uk/professionals/resources/clinical-champions-and-networks (accessed on 20 October 2020).
- Carlin, L.; Musson, H.; Adams, E. Evaluation of the Clinical Champions’ Physical Activity Training programme. OSF Prepr. 2020. preprint. [Google Scholar]
- Institute of Health Visiting. Perinatal Mental Health Champions Training. Available online: https://ihv.org.uk/training-and-events/training-programme/courses/perinatal-depression-champions-training/ (accessed on 20 October 2020).
- NHS Digital. Digital Champions for Health: A Blueprint for Success. Available online: https://digital.nhs.uk/about-nhs-digital/our-work/transforming-health-and-care-through-technology/empower-the-person-formerly-domain-a/widening-digital-participation/digital-champions-for-health2020 (accessed on 20 October 2020).
- Lave, J.; Wenger, E. Situated Learning: Legitimate Peripheral Participation; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar]
- Wenger, E. Communities of Practice: Learning, Meaning, and Identity; Cambridge University Press: New York, NY, USA, 1998. [Google Scholar]
- McKellar, K.A.; Pitzul, K.B.; Yi, J.Y.; Cole, D.C. Evaluating communities of practice and knowledge networks: A systematic scoping review of evaluation frameworks. Ecohealth 2014, 11, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Ranmuthugala, G.; Plumb, J.J.; Cunningham, F.C.; Georgiou, A.; Westbrook, J.I.; Braithwaite, J. How and why are communities of practice established in the healthcare sector? A systematic review of the literature. BMC Health Serv. Res. 2011, 11, 273. [Google Scholar] [CrossRef] [PubMed]
- Bartunek, J.M. Intergroup relationships and quality improvement in healthcare. BMJ Qual. Saf. 2011, 20 (Suppl. S1), i62–i66. [Google Scholar] [CrossRef]
- Mann, T.; de Ridder, D.; Fujita, K. Self-regulation of health behavior: Social psychological approaches to goal setting and goal striving. Health Psychol. 2013, 32, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Atkins, L.; Chadborn, T.; Bondaronek, P.; Ashiru-Oredope, D.; Beech, E.; Herd, N.; de la Morinière, V.; González-Iraizoz, M.; Hopkins, S.; McNulty, C. Content and Mechanism of Action of National Antimicrobial Stewardship Interventions on Management of Respiratory Tract Infections in Primary and Community Care. Antibiotics 2020, 9, 512. [Google Scholar] [CrossRef] [PubMed]
- Opadeyi, A.O.; Fourrier-Reglat, A.; Isah, A.O. Educational intervention to improve the knowledge, attitude and practice of healthcare professionals regarding pharmacovigilance in South-South Nigeria. Ther. Adv. Drug Saf. 2019, 10, 2042098618816279. [Google Scholar] [CrossRef] [PubMed]
- Kamarudin, G.; Penm, J.; Chaar, B.; Moles, R. Educational interventions to improve prescribing competency: A systematic review. BMJ Open 2013, 3, e003291. [Google Scholar] [CrossRef] [PubMed]
- Magrini, N.; Formoso, G.; Capelli, O.; Maestri, E.; Nonino, F.; Paltrinieri, B.; del Giovane, C.; Voci, C.; Magnano, L.; Daya, L.; et al. Long term effectiveness on prescribing of two multifaceted educational interventions: Results of two large scale randomized cluster trials. PLoS ONE 2014, 9, e109915. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Zhang, Z.; Walley, J.D.; Hicks, J.P.; Zeng, J.; Deng, S.; Zhou, Y.; Yin, J.; Newell, J.N.; Sun, Q.; et al. Effect of a training and educational intervention for physicians and caregivers on antibiotic prescribing for upper respiratory tract infections in children at primary care facilities in rural China: A cluster-randomised controlled trial. Lancet Glob. Health 2017, 5, e1258–e1267. [Google Scholar] [CrossRef]
- Maki, G.; Smith, I.; Paulin, S.; Kaljee, L.; Kasambara, W.; Mlotha, J.; Chuki, P.; Rupali, P.; Singh, D.R.; Bajracharya, D.C.; et al. Feasibility Study of the World Health Organization Health Care Facility-Based Antimicrobial Stewardship Toolkit for Low- and Middle-Income Countries. Antibiotics 2020, 9, 556. [Google Scholar] [CrossRef] [PubMed]
- Rocha-Pereira, N.; Lafferty, N.; Nathwani, D. Educating healthcare professionals in antimicrobial stewardship: Can online-learning solutions help? J. Antimicrob. Chemother. 2015, 70, 3175–3177. [Google Scholar] [CrossRef] [PubMed]
- Little, P.; Stuart, B.; Francis, N.; Douglas, E.; Tonkin-Crine, S.; Anthierens, S.; Cals, J.W.L.; Melbye, H.; Santer, M.; Moore, M.; et al. Effects of internet-based training on antibiotic prescribing rates for acute respiratory-tract infections: A multinational, cluster, randomised, factorial, controlled trial. Lancet 2013, 382, 1175–1182. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Craig, P.; Simpson, S.; Moore, L. Developing and evaluating complex interventions: Updating Medical Research Council guidance to take account of new methodological and theoretical approaches. Lancet 2018, 392, S2. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| SDT Construct | Operational Condition | Guiding Principle |
|---|---|---|
| Support for autonomy | Relevance | Provide a clear and meaningful rationale for both AVC and AMS activities throughout all inputs and training elements of the AVC programme (Figure 1), aiming to facilitate self-endorsement of activities by VPCs. |
| Respect | Seek to actively acknowledge VPCs’ perspectives, feelings, and agendas within network activities. Thoughtfully integrate opportunities within the programme for individuals to contribute to, shape, and offer reflection on the intervention process, foci, and goals as they unfold. | |
| Choice | Embed engagement with AVC activities with a sense of choice wherever possible, by providing varied options for process engagement (i.e., in educational training and network meeting participation) and encourage VPCs to follow their own interests, ideas, and goals in the selection, adoption, and implementation of AMS intervention activities. | |
| Avoidance of control | Commitment by those leading AVC to avoid directive, coercive, or authoritarian management of VPCs within the network; ensuring this ethos leads to the selection of collaborative partners who contribute to practical programme delivery (such as external facilitators). | |
| Support for competence | Clarity of expectations | Ensuring that through recruitment, inputs and training activities within the AVC programme (Figure 1) discussion of what to expect and what not to expect from AVC participation is facilitated. Set up processes that encourage the setting of realistic and achievable behaviour change goals by VPCs in their adoption and integration of AMS options. |
| Optimal challenge | Seek to encourage VPCs to select behaviour change goals where the challenge of the activity is highly balanced with their ability to successfully perform the behaviour (i.e., the change is a good fit for their practice and context, is something that they have the appropriate skill set to enact, and that is neither too easy nor too difficult for the VPC to implement). | |
| Feedback | Ensure VPCs have the opportunity to access relevant and non-judgmental feedback on their practice interventions throughout design and implementation processes, both individually (through accessibility of contact with G.R. as project lead) and in-group meetings where this is facilitated peer-to-peer within the network (i.e., workshops and discussion groups). | |
| Skills training | Commitment to providing education, training, guidance and support in key areas of AMS as identified through knowledge pathways in Phase One of intervention design, to ensure VPCs feel adequately equipped to identify and set their own AMS behaviour change goal(s). | |
| Support for relatedness | Empathy | Ensuring group meetings (discussion groups, workshops) offer opportunities for VPCs to explore and reflect on their colleagues’ perspectives at both peer-to-peer and group levels. Facilitate alternate perspective taking on any contentious issues if they arise within the group. |
| Affection | Those coordinating the AVC scheme taking care to convey a sense of care and concern for participants prescribing and AMS challenges, in addition to genuine appreciation for VPC engagement. | |
| Attunement | Careful attention to, gathering knowledge about and responding to VPC perspectives both (i) by those coordinating the AVC scheme and (ii) facilitated peer-to-peer within the AVC network, to ensure VPCs needs to feel validated, accepted, affirmed, and significant within AVC are met [28], and to generate a felt sense of union with other VPCs in this process [29]. | |
| Dedication of resources | Emphasising where and how AVC coordinators and wider project collaborators (industry, government) are investing time and energy into the scheme, in addition to creating project opportunities (workshops, discussion groups) where VPCs are connected by volunteering their time and energy to drive the momentum of AVC. | |
| Dependability | Ensuring VPCs feel that support is available to them via AVC in case of need on their AMS behaviour change journey, through guidance on how they can seek the input and advice of the project lead (GR) throughout. |
| Participant Characteristic | All VPCs | North Wales VPCs | South Wales VPCs | |||
|---|---|---|---|---|---|---|
| All VPCs | 43 | 100% | 17 | 100% | 26 | 100% |
| Gender | ||||||
| Male Female | 24 19 | 56% 44% | 11 6 | 65% 35% | 13 13 | 50% 50% |
| Years qualified | ||||||
| <5 years 5–10 years 10–20 years >20 years | 2 8 11 22 | 5% 19% 25% 51% | 0 4 5 8 | 0% 24% 29% 47% | 2 4 6 14 | 8% 15% 23% 54% |
| Position in practice | ||||||
| Business Partner/Director Clinical Director Consultant Salaried Assistant | 19 5 1 18 | 44% 12% 2% 42% | 7 2 1 7 | 41% 12% 6% 41% | 12 3 0 11 | 46% 12% 0% 42% |
| Number of cattle herds served by the practice | ||||||
| <100 101–200 201–300 301–400 >401 | 7 11 12 6 7 | 16% 26% 28% 14% 16% | 4 4 6 1 2 | 24% 24% 35% 6% 11% | 3 7 6 5 5 | 12% 27% 23% 19% 19% |
| Number of farm vets in the practice | ||||||
| 0-5 6–10 11–15 >15 | 7 23 6 7 | 16% 54% 14% 16% | 3 9 2 3 | 18% 53% 11% 18% | 4 14 4 4 | 15% 55% 15% 15% |
| Species cared for | ||||||
| Farm only Mixed species | 7 36 | 16% 84% | 3 14 | 18% 82% | 4 22 | 15% 85% |
| Week | Activity | Topic |
|---|---|---|
| 1 | Webinar | Welcome and introduction to antimicrobial stewardship (AMS) |
| 2 | Webinar | Encouraging behaviour change for AMS |
| 3 | Discussion Group | Developing the “Champion mindset” |
| 4 | Webinar | Prescribing rules, regulations and guidelines in farm animals |
| 5 | Webinar | Sector-specific prescribing: dairy cattle, beef cattle and sheep |
| 6 | Discussion Group | Prescribing conduct and barriers to AMS |
| 7 | Webinar | Evidence-based prescribing and practical approaches to AMS |
| 8 | Webinar | Case studies and practical examples |
| 9 | Discussion Group | The future of the VPC Network |
| 12 | Workshop | Intervention design |
| 13 | Workshop | Policy recommendations |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rees, G.M.; Bard, A.; Reyher, K.K. Designing a National Veterinary Prescribing Champion Programme for Welsh Veterinary Practices: The Arwain Vet Cymru Project. Antibiotics 2021, 10, 253. https://doi.org/10.3390/antibiotics10030253
Rees GM, Bard A, Reyher KK. Designing a National Veterinary Prescribing Champion Programme for Welsh Veterinary Practices: The Arwain Vet Cymru Project. Antibiotics. 2021; 10(3):253. https://doi.org/10.3390/antibiotics10030253
Chicago/Turabian StyleRees, Gwen M., Alison Bard, and Kristen K. Reyher. 2021. "Designing a National Veterinary Prescribing Champion Programme for Welsh Veterinary Practices: The Arwain Vet Cymru Project" Antibiotics 10, no. 3: 253. https://doi.org/10.3390/antibiotics10030253
APA StyleRees, G. M., Bard, A., & Reyher, K. K. (2021). Designing a National Veterinary Prescribing Champion Programme for Welsh Veterinary Practices: The Arwain Vet Cymru Project. Antibiotics, 10(3), 253. https://doi.org/10.3390/antibiotics10030253