
Insufficient Stability of Clavulanic Acid in Widely Used Child-Appropriate Formulations

 , and
, and
Abstract
1. Introduction
2. Results
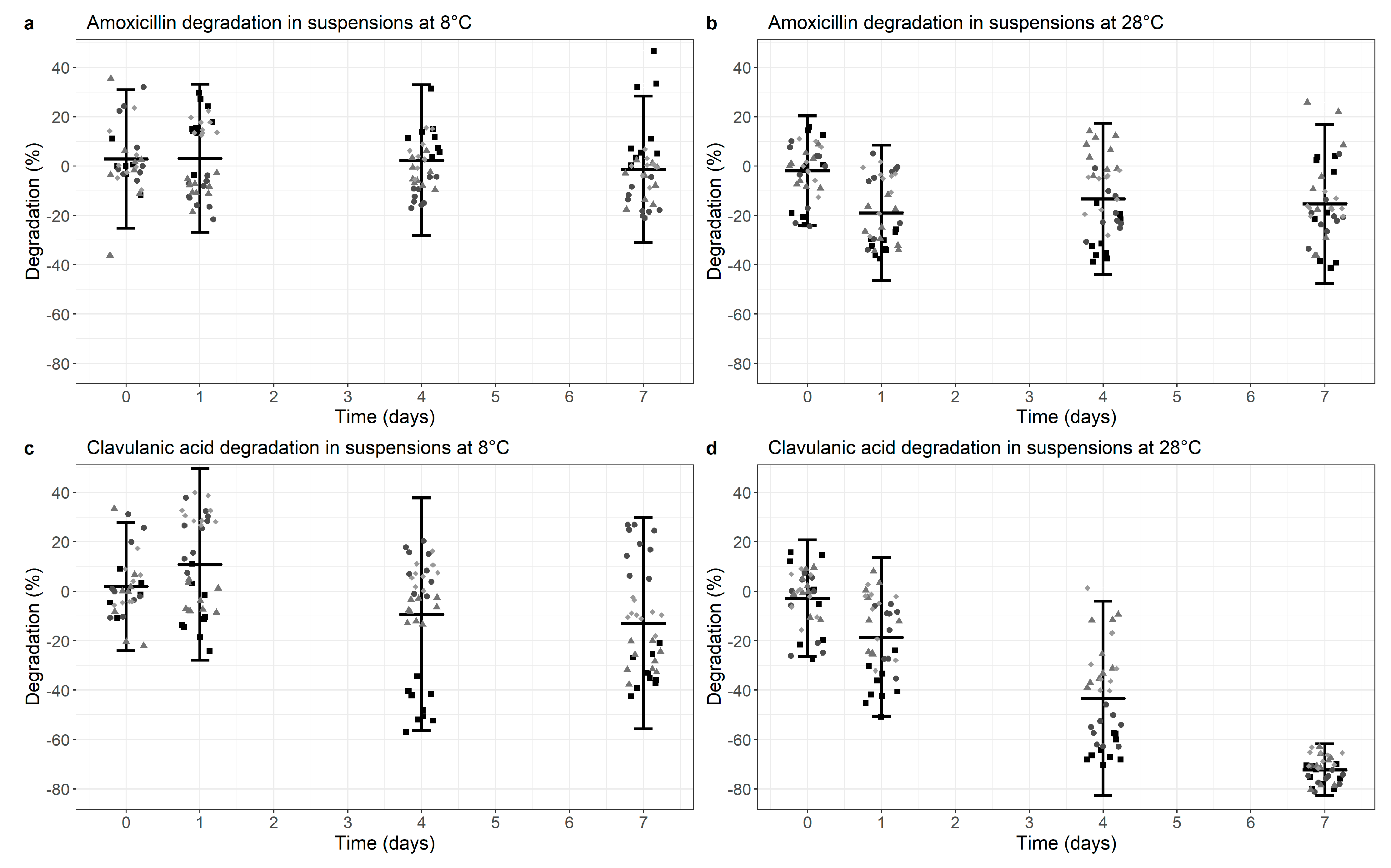
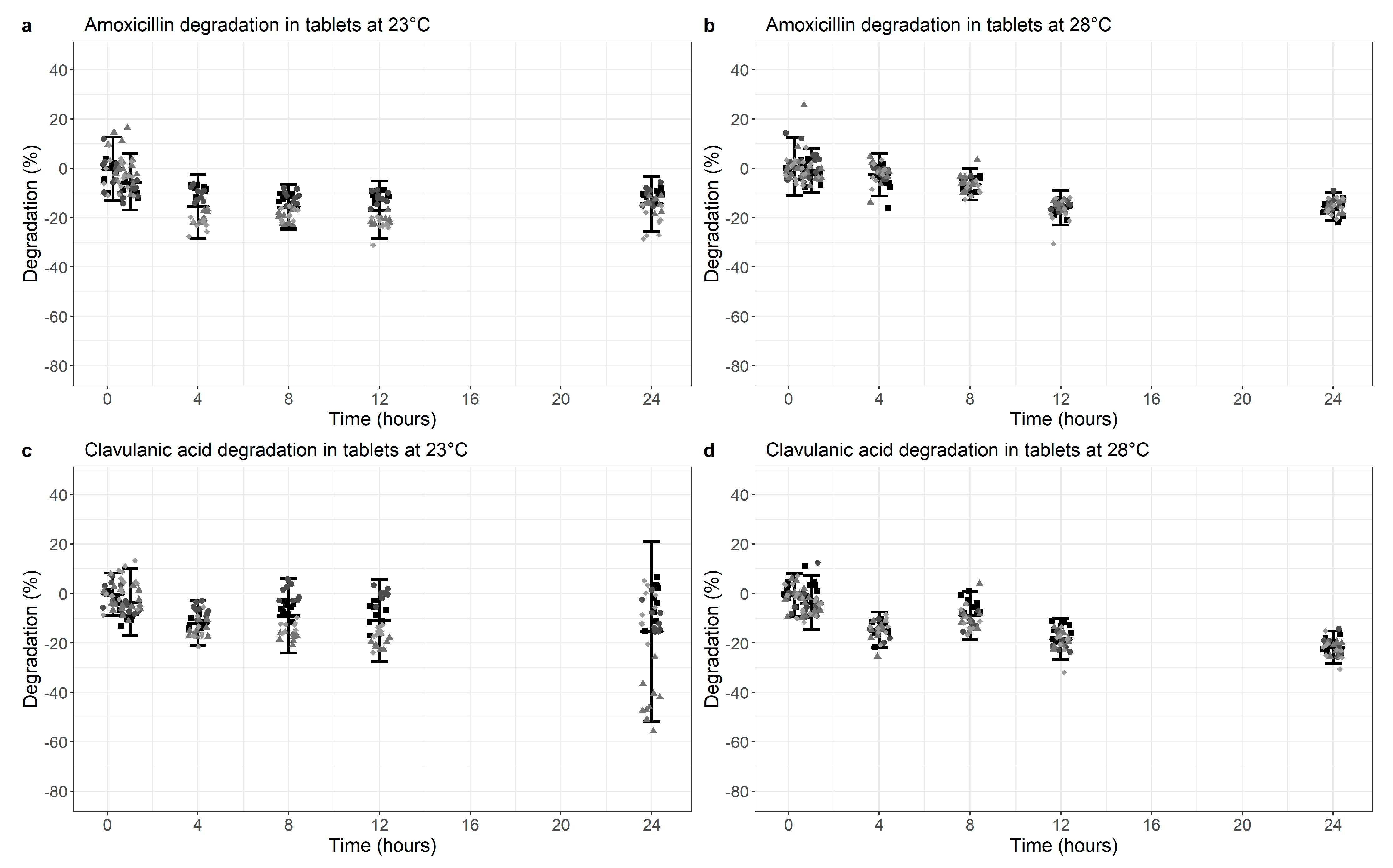
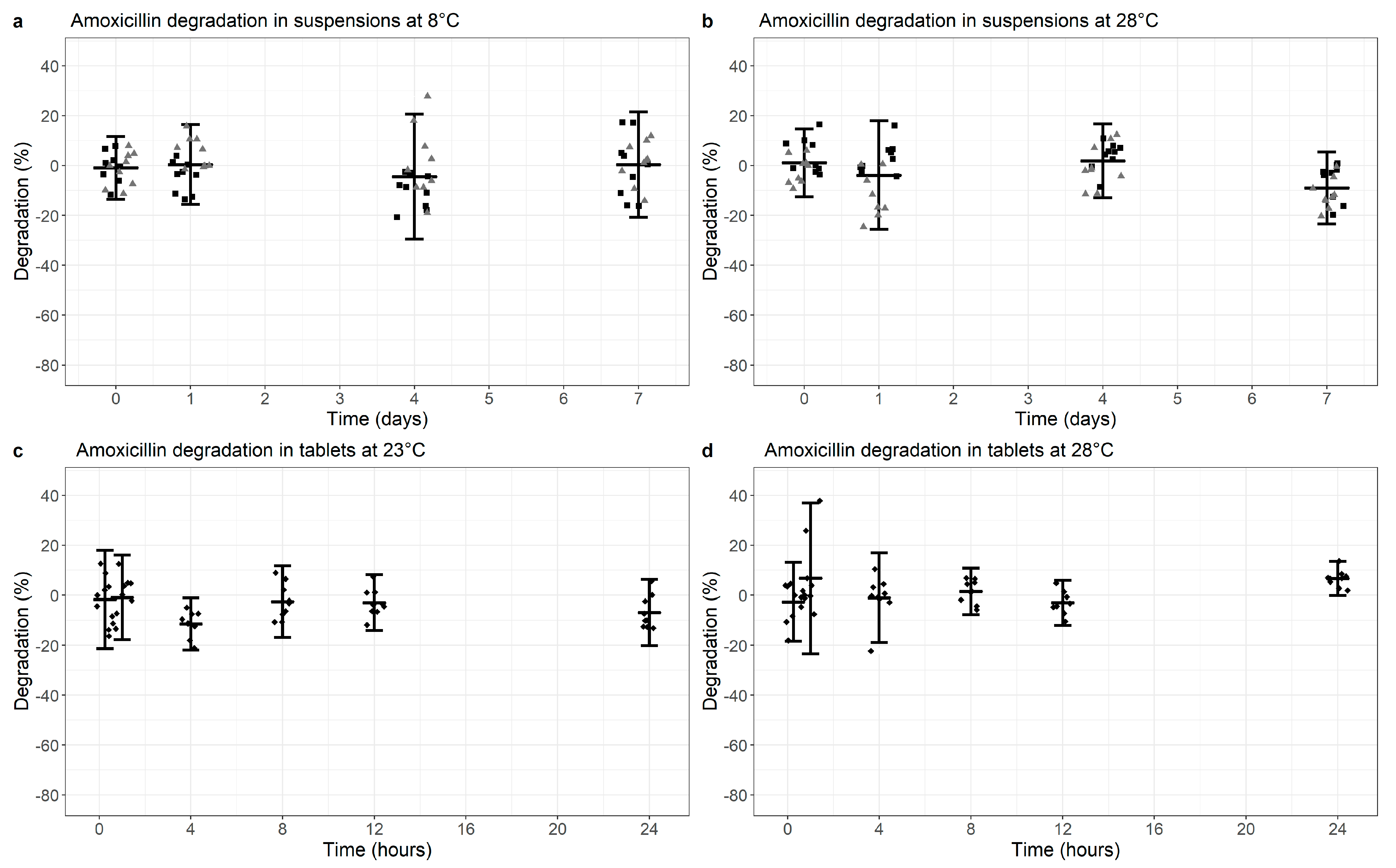
2.1. Stability Data
2.1.1. Amoxicillin-Clavulanic Acid: Co-Formulated Suspensions
2.1.2. Amoxicillin-Clavulanic Acid: Co-Formulated Dispersible Tablets
2.1.3. Amoxicillin: Suspensions and Dispersible Tablets
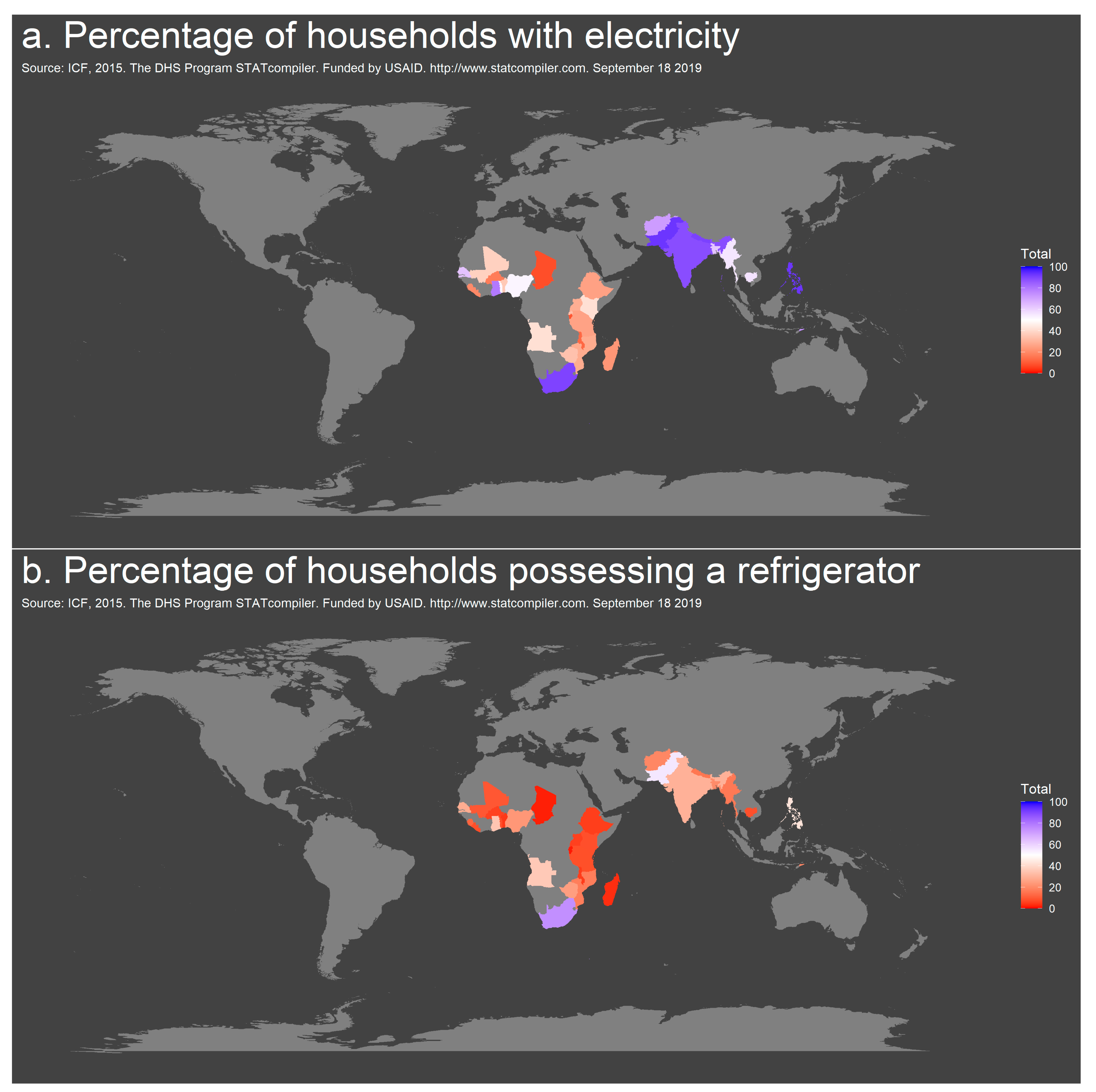
2.2. DHS Data on Access to Electricity and Refrigeration
3. Discussion
4. Materials and Methods
4.1. Degradation Kinetics of Clavulanic Acid and Amoxicillin
4.2. Data Analysis and Visualization
4.3. DHS Data on Access to Electricity and Refrigeration
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jackson, C.; Hsia, Y.; Bielicki, J.A.; Ellis, S.; Stephens, P.; Wong, I.C.K.; Sharland, M. Estimating global trends in total and childhood antibiotic consumption, 2011–2015. BMJ Glob. Health 2019, 4, e001241. [Google Scholar] [CrossRef]
- WHO 20th Essential Medicines List (2017). Available online: https://www.who.int/medicines/publications/essentialmedicines/en/ (accessed on 30 May 2019).
- Sharland, M.; Pulcini, C.; Harbarth, S.; Zeng, M.; Gandra, S.; Mathur, S.; Magrini, N. Classifying antibiotics in the WHO Essential Medicines List for optimal use-be AWaRe. Lancet Infect. Dis. 2018, 18, 18–20. [Google Scholar] [CrossRef]
- O’Donell, P.B.; Bokser, A.D. Stability of pharmaceutical products. In Remington: The Science and Practice of Pharmacy, 21st ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- USAID-funded Demographic and Health Survey Statcompiler. Available online: www.statcompiler.com (accessed on 8 August 2019).
- Huttner, A.; Bielicki, J.; Clements, M.N.; Frimodt-Møller, N.; Muller, A.E.; Paccaud, J.P.; Mouton, J.W. Oral amoxicillin and amoxicillin-clavulanic acid: Properties, indications and usage. Clin. Microbiol Infect. 2020, 26, 871–879. [Google Scholar] [CrossRef]
- Cook, B.; Hill, S.; Lynn, B. The stability of amoxycillin sodium in intravenous infusion fluids. Clin. Hosp. Pharm. 1982, 7, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Sylvestri, M.; Moakoid, M.; Frost, G. Stability of Amoxicillin Trihydrate Oral Suspension in Clear Plastic Unit Dose Syringes. Drug Dev. Ind. Pharm. 1988, 14, 819–830. [Google Scholar] [CrossRef]
- Mehta, A.; Hart-Davies, S.; Payne, J.; Lacey, R.W. Stability of amoxycillin and potassium clavulanate in co-amoxiclav oral suspension. J. Clin. Pharm. Ther. 1994, 19, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Peace, N.; Olubukola, O.; Moshood, A. Stability of reconstituted amoxicillin clavulanate potassium under simulated in-home storage conditions. J. Appl. Pharm. Sci. 2012, 2, 28–31. [Google Scholar]
- Haginaka, J.; Nakagawa, T.; Uno, T. Stability of clavulanic acid in aqueous solutions. Chem. Pharm. Bull. 1981, 29, 3334–3341. [Google Scholar] [CrossRef]
- European Medicines Agency (EMA) International Council for Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) Guidelines. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-q-4-b-annex-6-note-evaluation-recommendation-pharmacopoeial-texts-use-ich-regions-uniformity_en.pdf (accessed on 15 January 2021).
- Revised WHO Classification and Treatment of Childhood Pneumonia at health Facilities—Evidence Summaries. 2014. Available online: https://www.who.int/maternal_child_adolescent/documents/child-pneumonia-treatment/en/ (accessed on 11 June 2019).
- Maiwada, J.; Said, M.M. Postreconstitution Stability of Amoxicillin–Clavulanic Acid Suspensions at Tropical Room Temperature. J. Pediatric Infect. Dis Soc. 2019, 8, 368–369. [Google Scholar] [CrossRef] [PubMed]
- Rewar, S.; Singh, C.J.; Bansal, B.K.; Pareek, R.; Sharma, A.K. Oral dispersible tablets: An overview; development, technologies and evaluation. IJRDPL 2014, 3, 1223–1235. [Google Scholar]
- Unicef Amoxicillin Dispersible Tablets: Market and Supply Update. Available online: https://www.unicef.org/supply/files/Amoxicillin_DT_Supply_Update.pdf (accessed on 30 May 2019).
- Unicef Supply Catalogue. Available online: https://supply.unicef.org/all-materials.html (accessed on 27 October 2020).
- South African Department of Health supply catalogue. Available online: http://www.health.gov.za/index.php/2015-05-15-12-36-34 (accessed on 27 October 2020).
- Swiss Drug Compendium. Available online: www.compendium.ch (accessed on 24 September 2019).
- Country Classification by the World Bank. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 27 October 2020).
- Naidoo, K.K.; Nompuku, P.; Mkalali, S.N.; Shabangu, K.; Nkabinde, L.; Singh, V. Post-marketing stability surveillance: Amoxicillin. Off. J. S. Afr. Acad. Fam. Pract./Prim. Care 2006, 48, 14–14d. [Google Scholar] [CrossRef]
- Sharland, M. Lower respiratory tract infections. In Manual of Childhood Infections, The Blue Book, 4th ed.; Oxford Unversity Press: Oxford, UK, 2016; pp. 210–219. [Google Scholar]
- Harris, M.; Clark, J.; Coote, N.; Fletcher, P.; Harnden, A.; McKean, M.; Thomson, A. British Thoracic Society guidelines for the management of community acquired pneumonia in children: Update 2011. Thorax 2011, 66, ii1–ii23. [Google Scholar] [CrossRef] [PubMed]
- Le Saux, N.; Robinson, J.L. Uncomplicated pneumonia in healthy Canadian children and youth: Practice points for management. Paediatr. Child Health 2015, 20, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Cohen, R.; Domingo, J.D.; Pecurariu, O.F.; Greenberg, D.; Heininger, U.; Knuf, M.; Lutsar, I.; Principi, N.; Rodrigues, F.; et al. Antibiotic therapy for pediatric community-acquired pneumonia: Do we know when, what and for how long to treat? Pediatr. Infect. Dis. J. 2012, 31, e78–e85. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.S.; Byington, C.L.; Shah, S.S.; Alverson, B.; Carter, E.R.; Harrison, C.; Kaplan, S.L.; Mace, S.E.; McCracken, G.H.; Moore, M.R.; et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: Clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin. Infect. Dis. 2011, 53, e25–e76. [Google Scholar] [CrossRef]
- Rehm, S.; Rentsch, K.M. A 2D HPLC-MS/MS method for several antibiotics in blood plasma, plasma water, and diverse tissue samples. Anal. Bioanal. Chem. 2020, 412, 715–725. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Manufacturer | Product |
|---|---|
| Spirig HealthCare (Egerkingen, Switzerland) | Aziclav Duo (400 mg, 57 mg/mL) Aziclav Forte (250 mg, 62.5 mg/5mL) |
| GlaxoSmithKline (Brentford, United Kingdom) | Augmentin Duo (400 mg, 57 mg/5mL) Augmentin Trio Forte (250 mg, 62.5 mg/5mL) |
| Mepha Pharma (Basel, Switzerland) | Amoxi-Mepha (200 mg/4mL) Co-Amoxi-Mepha Dispersible 1000 mg (875 mg/125 mg) Co-Amoxi-Mepha Dispersible 625 mg (500 mg/125 mg) |
| Sandoz Pharmaceuticals (Rotkreuz, Switzerland) | Amoxicillin Sandoz (200 mg Amoxicillin/4 mL) Amoxicillin Sandoz 1000 (1000 mg Amoxicillin per tablet) Co-Amoxicillin Sandoz 625 (500 mg/125 mg per tablet) Co-Amoxicillin Sandoz 1 g (875 mg/125 mg per tablet) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mack, I.; Sharland, M.; Brussee, J.M.; Rehm, S.; Rentsch, K.; Bielicki, J. Insufficient Stability of Clavulanic Acid in Widely Used Child-Appropriate Formulations. Antibiotics 2021, 10, 225. https://doi.org/10.3390/antibiotics10020225
Mack I, Sharland M, Brussee JM, Rehm S, Rentsch K, Bielicki J. Insufficient Stability of Clavulanic Acid in Widely Used Child-Appropriate Formulations. Antibiotics. 2021; 10(2):225. https://doi.org/10.3390/antibiotics10020225
Chicago/Turabian StyleMack, Ines, Mike Sharland, Janneke M. Brussee, Sophia Rehm, Katharina Rentsch, and Julia Bielicki. 2021. "Insufficient Stability of Clavulanic Acid in Widely Used Child-Appropriate Formulations" Antibiotics 10, no. 2: 225. https://doi.org/10.3390/antibiotics10020225
APA StyleMack, I., Sharland, M., Brussee, J. M., Rehm, S., Rentsch, K., & Bielicki, J. (2021). Insufficient Stability of Clavulanic Acid in Widely Used Child-Appropriate Formulations. Antibiotics, 10(2), 225. https://doi.org/10.3390/antibiotics10020225