
Role of Antimicrobial Susceptibility Testing before First-Line Treatment Containing Clarithromycin for Helicobacter pylori Eradication in the Clinical Setting

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Isolation and Culture of H. pylori
2.3. Determination of the Minimum Inhibitory Concentration (MIC)
2.4. 13C-Urea Breath Test
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Outcomes
3.3. Antimicrobial Susceptibility
3.4. Second-line Treatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global prevalence of Helicobacter pylori infection: Systematic review and meta-analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef]
- Lee, J.H.; Choi, K.D.; Jung, H.Y.; Baik, G.H.; Park, J.K.; Kim, S.S.; Kim, B.W.; Hong, S.J.; Lim, H.; Shin, C.M.; et al. Seroprevalence of Helicobacter pylori in Korea: A multicenter, nationwide study conducted in 2015 and 2016. Helicobacter 2018, 23, e12463. [Google Scholar] [CrossRef]
- McColl, K.E. Clinical practice. Helicobacter pylori infection. N. Engl. J. Med. 2010, 362, 1597–1604. [Google Scholar] [CrossRef]
- Lim, J.H.; Kim, N.; Lim, S.H.; Kwon, J.W.; Shin, C.M.; Chang, Y.S.; Kim, J.S.; Jung, H.C.; Cho, S.H. Inverse relationship between Helicobacter pylori infection and asthma among adults younger than 40 years: A cross-sectional study. Medicine (Baltim.) 2016, 95, e2609. [Google Scholar] [CrossRef] [PubMed]
- de Korwin, J.D.; Ianiro, G.; Gibiino, G.; Gasbarrini, A. Helicobacter pylori infection and extragastric diseases in 2017. Helicobacter 2017, 22, e12411. [Google Scholar] [CrossRef] [PubMed]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG clinical guideline: Treatment of Helicobacter pylori infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef]
- Scott, D.; Weeks, D.; Melchers, K.; Sachs, G. The life and death of Helicobacter pylori. Gut 1998, 43, S56–S60. [Google Scholar] [CrossRef]
- Mizoguchi, H.; Fujioka, T.; Nasu, M. Evidence for viability of coccoid forms of Helicobacter pylori. J. Gastroenterol. 1999, 34, 32–36. [Google Scholar]
- Graham, D.Y.; Shiotani, A. New concepts of resistance in the treatment of Helicobacter pylori infections. Nat. Clin. Pract. Gastroenterol. Hepatol. 2008, 5, 321–331. [Google Scholar] [CrossRef]
- Ierardi, E.; Losurdo, G.; Fortezza, R.F.L.; Principi, M.; Barone, M.; Leo, A.D. Optimizing proton pump inhibitors in Helicobacter pylori treatment: Old and new tricks to improve effectiveness. World J. Gastroenterol. 2019, 25, 5097–5104. [Google Scholar] [CrossRef]
- Kim, S.G.; Jung, H.K.; Lee, H.L.; Jang, J.Y.; Lee, H.; Kim, C.G.; Shin, W.G.; Shin, E.S.; Lee, Y.C.; Korean College of Helicobacter and Upper Gastrointestinal Research; et al. Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. Korean J. Gastroenterol. 2013, 62, 3–26. [Google Scholar] [CrossRef]
- Leung, W.K.; Graham, D.Y. Clarithromycin for Helicobacter pylori infection. Expert Opin. Pharmacother. 2000, 1, 507–514. [Google Scholar] [CrossRef]
- Peterson, W.L.; Graham, D.Y.; Marshall, B.; Blaser, M.J.; Genta, R.M.; Klein, P.D.; Stratton, C.W.; Drnec, J.; Prokocimer, P.; Siepman, N. Clarithromycin as monotherapy for eradication of Helicobacter pylori: A randomized, double-blind trial. Am. J. Gastroenterol. 1993, 88, 1860–1864. [Google Scholar]
- Bang, C.S.; Baik, G.H. Attempts to enhance the eradication rate of Helicobacter pylori infection. World J. Gastroenterol. 2014, 20, 5252–5262. [Google Scholar] [CrossRef]
- Kim, S.Y.; Choi, D.J.; Chung, J.W. Antibiotic treatment for Helicobacter pylori: Is the end coming? World J. Gastrointest. Pharmacol. Ther. 2015, 6, 183–198. [Google Scholar] [CrossRef]
- Shin, W.G.; Lee, S.W.; Baik, G.H.; Huh, K.C.; Lee, S.I.; Chung, J.W.; Jung, W.T.; Park, M.I.; Jung, H.K.; Kim, H.U.; et al. Eradication rates of Helicobacter pylori in Korea over the past 10 years and correlation of the amount of antibiotics use: Nationwide survey. Helicobacter 2016, 21, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Hwang, T.J.; Kim, N.; Kim, H.B.; Lee, B.H.; Nam, R.H.; Park, J.H.; Lee, M.K.; Park, Y.S.; Lee, D.H.; Jung, H.C.; et al. Change in antibiotic resistance of Helicobacter pylori strains and the effect of A2143G point mutation of 23S rRNA on the eradication of H. pylori in a single center of Korea. J. Clin. Gastroenterol. 2010, 44, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef]
- Kjoller, M.; Fischer, A.; Justesen, T. Transport conditions and number of biopsies necessary for culture of Helicobacter pylori. Eur. J. Clin. Microbiol. Infect. Dis. 1991, 10, 166–167. [Google Scholar] [CrossRef]
- Cammarota, G.; Ianiro, G.; Bibbo, S.; Di Rienzo, T.A.; Masucci, L.; Sanguinetti, M.; Gasbarrini, A. Culture-guided treatment approach for Helicobacter pylori infection: Review of the literature. World J. Gastroenterol. 2014, 20, 5205–5211. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI). Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria, 3rd ed.; CLSI Guideline M45; CLSI: Wayne, PA, USA, 2015. [Google Scholar]
- Kim, J.M.; Kim, J.S.; Jung, H.C.; Kim, N.; Song, I.S. Antibiotic resistance of Helicobacter pylori isolated from Korean patients in 2003. Korean J. Gastroenterol. 2004, 44, 126–135. [Google Scholar]
- Kim, J.M.; Kim, J.S.; Jung, H.C.; Kim, N.; Kim, Y.J.; Song, I.S. Distribution of antibiotic MICs for Helicobacter pylori strains over a 16-year period in patients from Seoul, South Korea. Antimicrob. Agents Chemother. 2004, 48, 4843–4847. [Google Scholar] [CrossRef]
- Zullo, A.; Rinaldi, V.; Winn, S.; Meddi, P.; Lionetti, R.; Hassan, C.; Ripani, C.; Tomaselli, G.; Attili, A.F. A new highly effective short-term therapy schedule for Helicobacter pylori eradication. Aliment. Pharmacol. Ther. 2000, 14, 715–718. [Google Scholar] [CrossRef]
- Liou, J.M.; Chen, C.C.; Chen, M.J.; Chen, C.C.; Chang, C.Y.; Fang, Y.J.; Lee, J.Y.; Hsu, S.J.; Luo, J.C.; Chang, W.H.; et al. Sequential versus triple therapy for the first-line treatment of Helicobacter pylori: A multicentre, open-label, randomised trial. Lancet 2013, 381, 205–213. [Google Scholar] [CrossRef]
- Gatta, L.; Scarpignato, C.; Fiorini, G.; Belsey, J.; Saracino, I.M.; Ricci, C.; Vaira, D. Impact of primary antibiotic resistance on the effectiveness of sequential therapy for Helicobacter pylori infection: Lessons from a 5-year study on a large number of strains. Aliment. Pharmacol. Ther. 2018, 47, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kim, N.; Nam, R.H.; In Choi, S.; Lee, J.W.; Lee, D.H. Primary and secondary antibiotic resistance of Helicobacter pylori in Korea from 2003 to 2018. Helicobacter 2019, 24, e12660. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Ahn, J.Y.; Choi, K.D.; Jung, H.Y.; Kim, J.M.; Baik, G.H.; Kim, B.W.; Park, J.C.; Jung, H.K.; Cho, S.J.; et al. Nationwide antibiotic resistance mapping of Helicobacter pylori in Korea: A prospective multicenter study. Helicobacter 2019, 24, e12592. [Google Scholar] [CrossRef]
- Boyanova, L.; Hadzhiyski, P.; Kandilarov, N.; Markovska, R.; Mitov, I. Multidrug resistance in Helicobacter pylori: Current state and future directions. Expert Rev. Clin. Pharmacol. 2019, 12, 909–915. [Google Scholar] [CrossRef]
- Kim, J.S.; Kim, B.W.; Ham, J.H.; Park, H.W.; Kim, Y.K.; Lee, M.Y.; Ji, J.S.; Lee, B.I.; Choi, H. Sequential therapy for Helicobacter pylori infection in korea: Systematic review and meta-analysis. Gut Liver 2013, 7, 546–551. [Google Scholar] [CrossRef][Green Version]
- O’Connor, J.P.; Taneike, I.; O’Morain, C. Improving compliance with Helicobacter pylori eradication therapy: When and how? Therap. Adv. Gastroenterol. 2009, 2, 273–279. [Google Scholar] [CrossRef]
- Jaka, H.; Mueller, A.; Kasang, C.; Mshana, S.E. Predictors of triple therapy treatment failure among H. pylori infected patients attending at a tertiary hospital in Northwest Tanzania: A prospective study. BMC Infect. Dis. 2019, 19, 447. [Google Scholar] [CrossRef]
- El-Halfawy, O.M.; Valvano, M.A. Antimicrobial heteroresistance: An emerging field in need of clarity. Clin. Microbiol. Rev. 2015, 28, 191–207. [Google Scholar] [CrossRef]
- Lee, M.; Kemp, J.A.; Canning, A.; Egan, C.; Tataronis, G.; Farraye, F.A. A randomized controlled trial of an enhanced patient compliance program for Helicobacter pylori therapy. Arch. Intern. Med. 1999, 159, 2312–2316. [Google Scholar] [CrossRef]
- Matteo, M.J.; Granados, G.; Olmos, M.; Wonaga, A.; Catalano, M. Helicobacter pylori amoxicillin heteroresistance due to point mutations in PBP-1A in isogenic isolates. J. Antimicrob. Chemother. 2008, 61, 474–477. [Google Scholar] [CrossRef]
- Kim, B.J.; Yang, C.H.; Song, H.J.; Jeon, S.W.; Kim, G.H.; Kim, H.S.; Kim, T.H.; Shim, K.N.; Chung, I.K.; Park, M.I.; et al. Online registry for nationwide database of Helicobacter pylori eradication in Korea: Correlation of antibiotic use density with eradication success. Helicobacter 2019, 24, e12646. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.H.; Kim, S.G.; Song, J.H.; Hwang, J.J.; Lee, D.H.; Han, J.P.; Hong, S.J.; Kim, J.H.; Jeon, S.W.; Kim, G.H.; et al. Efficacy of levofloxacin-based third-line therapy for the eradication of Helicobacter pylori in peptic ulcer disease. Gut Liver 2017, 11, 226–231. [Google Scholar] [CrossRef]
- An, B.; Moon, B.S.; Kim, H.; Lim, H.C.; Lee, Y.C.; Lee, G.; Kim, S.H.; Park, M.; Kim, J.B. Antibiotic resistance in Helicobacter pylori strains and its effect on H. pylori eradication rates in a single center in Korea. Ann. Lab. Med. 2013, 33, 415–419. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Calvet, X. Review article: Rifabutin in the treatment of refractory Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2012, 35, 209–221. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TOTAL | Susceptibility-Guided Therapy | Empirical Therapy | P-Value | |
|---|---|---|---|---|
| Number | 257 | 103 | 154 | |
| Age (mean ± SD) | 58.3 ± 10.6 | 57.6 ± 10.5 | 58.8 ± 10.7 | 0.41 |
| Male (%) | 147 (57.2%) | 59 (57.3%) | 88 (57.1%) | 0.98 |
| Smoking (%) | 41 (16.0%) | 17 (16.5%) | 24 (15.6%) | 0.86 |
| Alcohol (%) | 126 (49.0%) | 49 (47.6%) | 77 (50.0%) | 0.80 |
| Indications | 0.34 | |||
| Early gastric cancer (%) | 166 (64.6%) | 69 (67.0%) | 97 (63.0%) | |
| Atrophic gastritis (%) | 24 (9.3%) | 10 (9.7%) | 14 (9.1%) | |
| MALT lymphoma (%) | 24 (9.3%) | 7 (6.8%) | 17 (11.0%) | |
| Gastric adenoma (%) | 19 (7.4%) | 7 (6.8%) | 12 (7.8%) | |
| Peptic ulcer (%) | 6 (2.3%) | 0 (0%) | 6 (3.9%) | |
| Functional dyspepsia (%) | 6 (2.3%) | 4 (3.9%) | 2 (1.3%) | |
| Others (%) | 12 (4.7%) | 5 (4.9%) | 6 (3.9%) | |
| Resistance | ||||
| CLR-R (%) | 63 (24.9%) | 0 (0%) | 64 (41.6%) | <0.01 |
| AMX-R (%) | 18 (7.0%) | 6 (5.8%) | 12 (7.8%) | 0.55 |
| MDZ-R (%) | 89 (34.6%) | 31 (30.1%) | 58 (37.7%) | 0.21 |
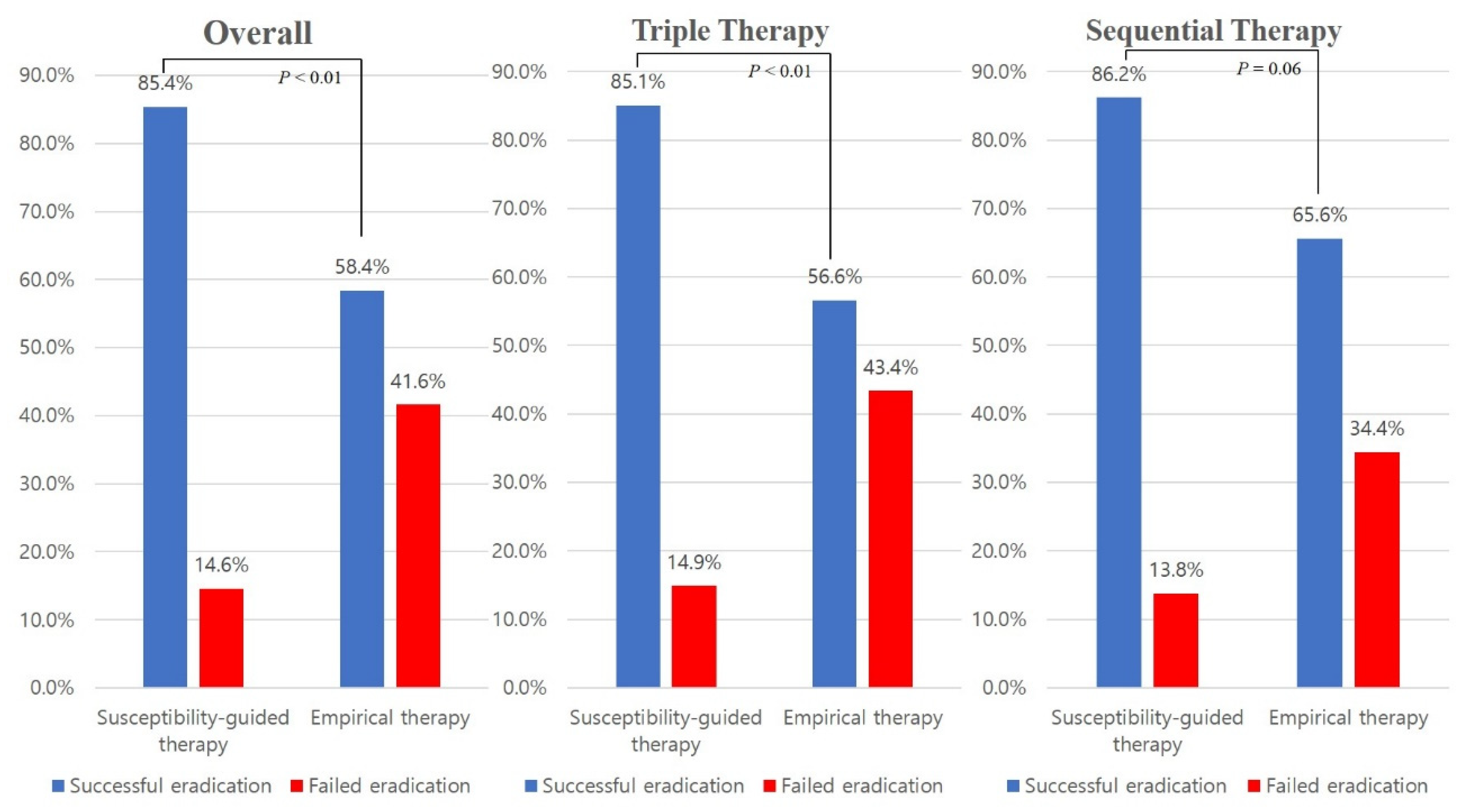
| Eradication | TOTAL | Susceptibility-Guided Therapy | Empirical Therapy | P-Value |
|---|---|---|---|---|
| Overall (n = 257) | 103 | 154 | ||
| Success (%) | 178 (69.3%) | 88 (85.4%) | 90 (58.4%) | <0.01 |
| Failure (%) | 79 (30.7%) | 15 (14.6%) | 64 (41.6%) | |
| TT (n = 196) | 74 | 122 | ||
| Success (%) | 132 (67.3%) | 63 (85.1%) | 69 (56.6%) | <0.01 |
| Failure (%) | 64 (32.7%) | 11 (14.9%) | 53 (43.4%) | |
| SET (n = 61) | 29 | 32 | ||
| Success (%) | 46 (75.4%) | 25 (86.2%) | 21 (65.6%) | 0.06 |
| Failure (%) | 15 (24.6%) | 4 (13.8%) | 11 (34.4%) |
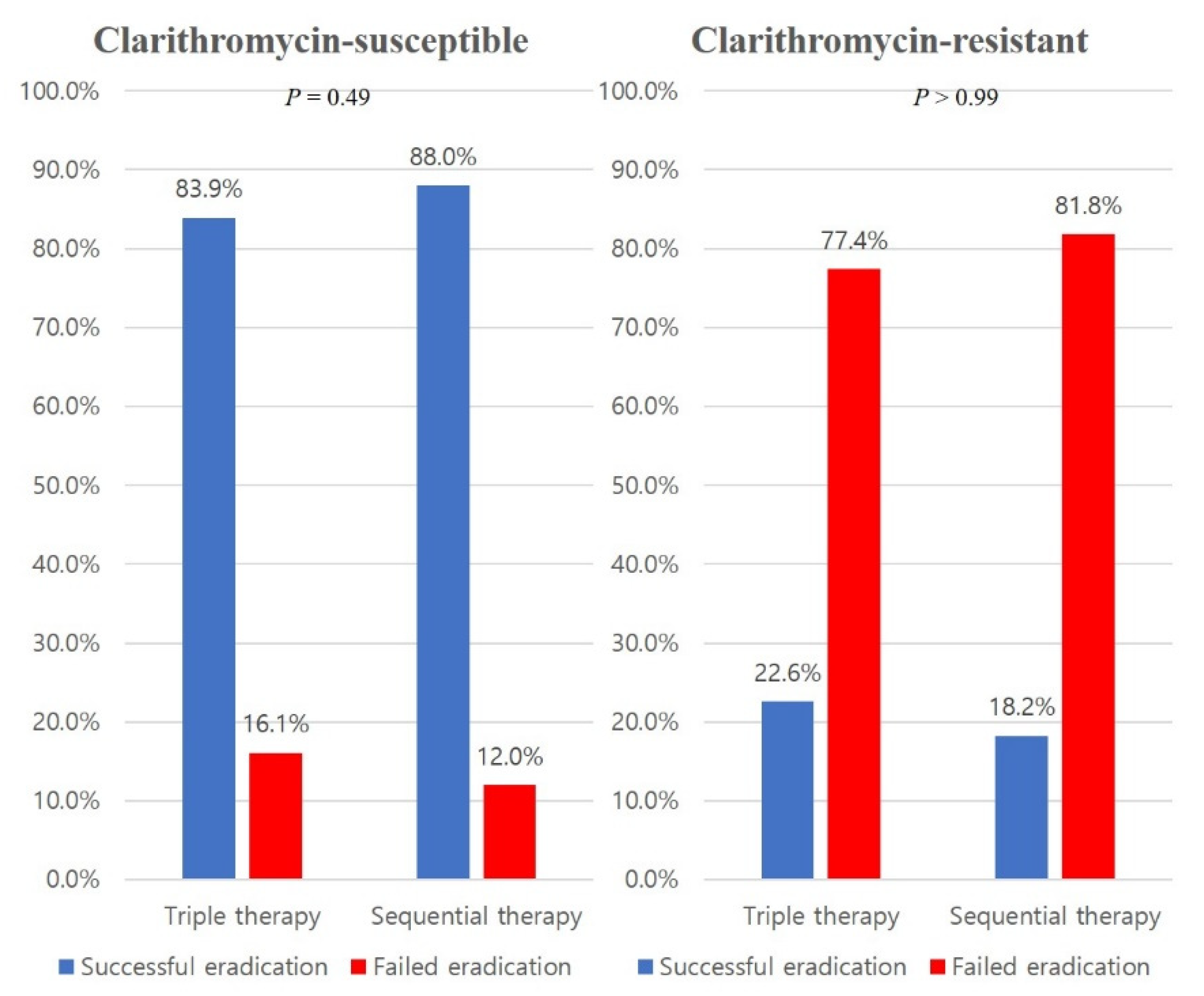
| Antimicrobial Susceptibility Testing in TT | Number (%) of Successful Eradication | |||
|---|---|---|---|---|
| Clarithromycin | Amoxicillin | |||
| S | S | 115/136 (84.6) | ||
| S | R | 5/7 (71.4) | ||
| R | S | 11/44 (25.0) | ||
| R | R | 1/9 (11.1) | ||
| Antimicrobial susceptibility testing in SET | Number (%) of successful eradication | |||
| Clarithromycin | Amoxicillin | Metronidazole | ||
| S | S | S | 34/38 (89.5) | |
| S | S | R | 8/10 (80.0) | |
| S | R | S | 1/1 (100) | |
| S | R | R | 1/1 (100) | |
| R | S | S | 2/4 (50.0) | |
| R | S | R | 0/7 (0) | |
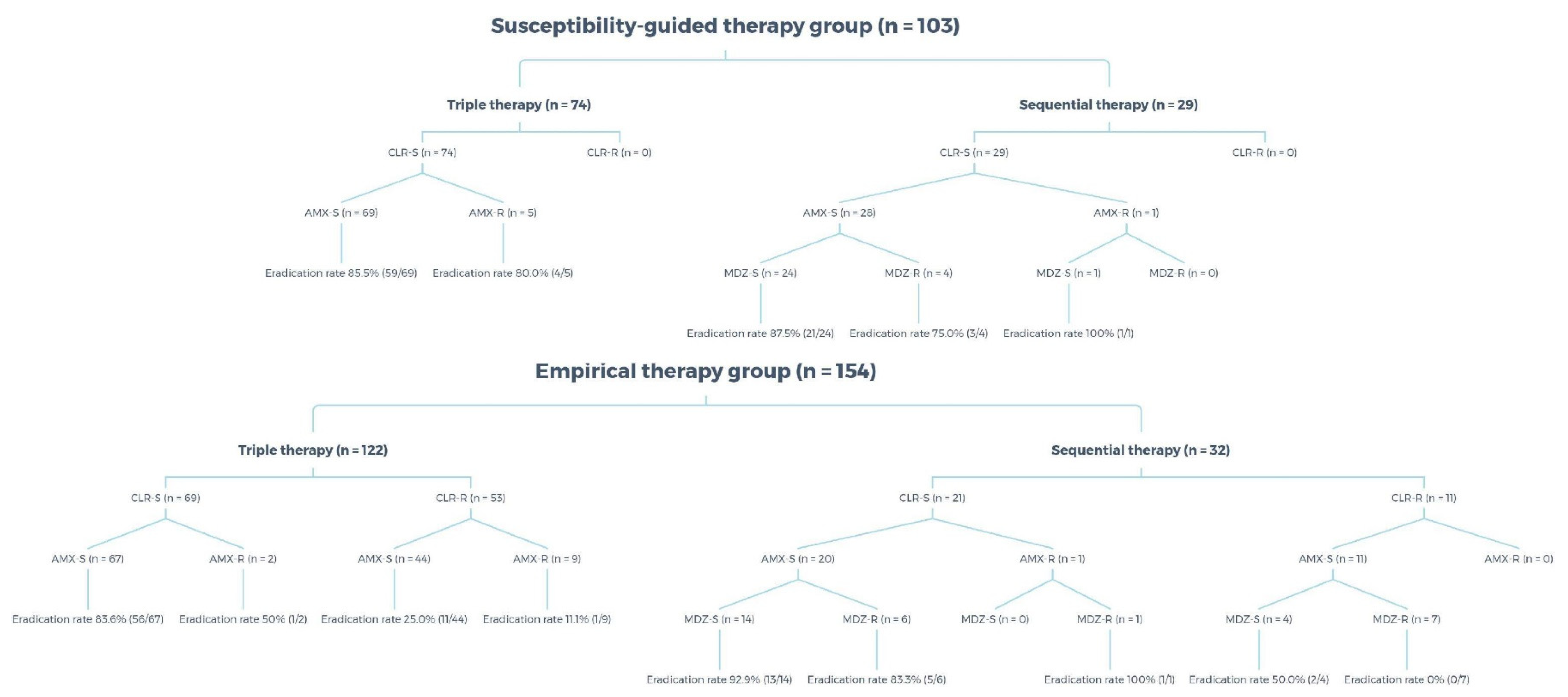
| Antimicrobial Susceptibility | Eradication Rate |
|---|---|
| Susceptibility-guided therapy group | n = 103 |
| Triple therapy | n = 74 |
| CLR-S and AMX-S | 85.5% (59/69) |
| CLR-S and AMX-R | 80.0% (4/5) |
| Sequential therapy | n = 29 |
| CLR-S and AMX-S and MDZ-S | 87.5% (21/24) |
| CLR-S and AMX-S and MDZ-R | 75.0% (3/4) |
| CLR-S and AMX-R and MDZ-S | 100.0% (1/1) |
| Empirical therapy group | n = 154 |
| Triple therapy | n = 122 |
| CLR-S and AMX-S | 83.6% (56/67) |
| CLR-S and AMX-R | 50.0% (1/2) |
| CLR-R and AMX-S | 25.0% (11/44) |
| CLR-R and AMX-R | 11.1% (1/9) |
| Sequential therapy | n = 32 |
| CLR-S and AMX-S and MDZ-S | 92.9% (13/14) |
| CLR-S and AMX-S and MDZ-R | 83.3% (5/6) |
| CLR-S and AMX-R and MDZ-R | 100% (1/1) |
| CLR-R and AMX-S and MDZ-S | 50.0% (2/4) |
| CLR-R and AMX-S and MDZ-R | 0% (0/7) |
| Treatment | Success | Failure | Loss to Follow-Up |
|---|---|---|---|
| Total (n = 56) | 40 (71.4%) | 9 (16.1%) | 7 (12.5%) |
| Quadruple (n = 48) | 35 (72.9%) | 7 (14.6%) | 6 (12.5%) |
| PBAMT (n = 5) | 4 (80.0%) | 1 (20.0%) | 0 |
| Others (n = 3) | 1 (33.3%) | 2 (66.7%) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, S.; Kim, Y.; Ahn, J.Y.; Jung, H.-Y.; Kim, N.; Na, H.K.; Lee, J.H.; Jung, K.W.; Kim, D.H.; Choi, K.D.; et al. Role of Antimicrobial Susceptibility Testing before First-Line Treatment Containing Clarithromycin for Helicobacter pylori Eradication in the Clinical Setting. Antibiotics 2021, 10, 214. https://doi.org/10.3390/antibiotics10020214
Kang S, Kim Y, Ahn JY, Jung H-Y, Kim N, Na HK, Lee JH, Jung KW, Kim DH, Choi KD, et al. Role of Antimicrobial Susceptibility Testing before First-Line Treatment Containing Clarithromycin for Helicobacter pylori Eradication in the Clinical Setting. Antibiotics. 2021; 10(2):214. https://doi.org/10.3390/antibiotics10020214
Chicago/Turabian StyleKang, Seokin, Yuri Kim, Ji Yong Ahn, Hwoon-Yong Jung, Nayoung Kim, Hee Kyong Na, Jeong Hoon Lee, Kee Wook Jung, Do Hoon Kim, Kee Don Choi, and et al. 2021. "Role of Antimicrobial Susceptibility Testing before First-Line Treatment Containing Clarithromycin for Helicobacter pylori Eradication in the Clinical Setting" Antibiotics 10, no. 2: 214. https://doi.org/10.3390/antibiotics10020214
APA StyleKang, S., Kim, Y., Ahn, J. Y., Jung, H.-Y., Kim, N., Na, H. K., Lee, J. H., Jung, K. W., Kim, D. H., Choi, K. D., Song, H. J., & Lee, G. H. (2021). Role of Antimicrobial Susceptibility Testing before First-Line Treatment Containing Clarithromycin for Helicobacter pylori Eradication in the Clinical Setting. Antibiotics, 10(2), 214. https://doi.org/10.3390/antibiotics10020214