
Molecular Characterization of Carbapenem-Resistant Acinetobacter baumannii Isolated from the Intensive Care Unit in a Tertiary Teaching Hospital in Malaysia

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Overview of Patients with CRAB Cases
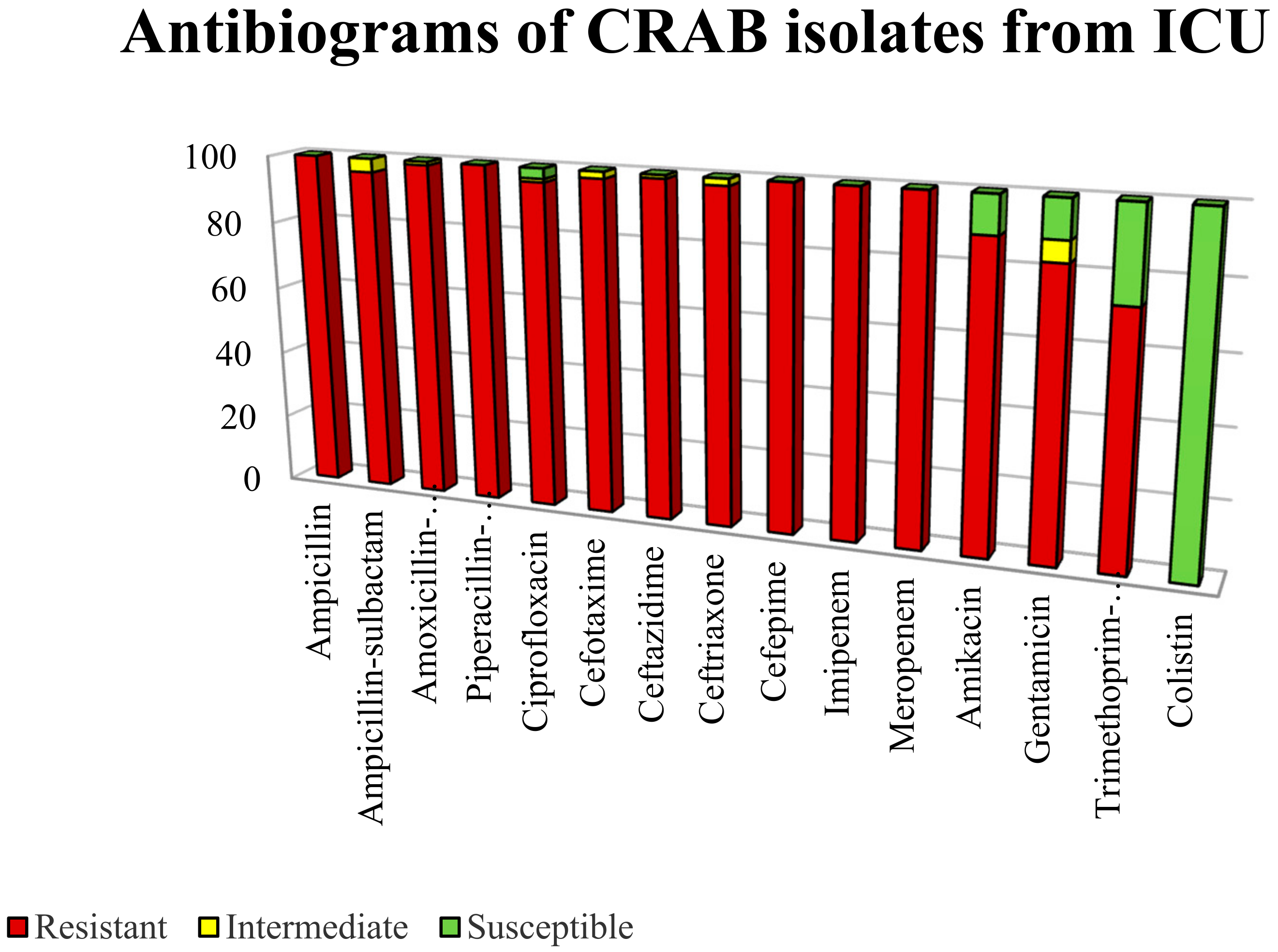
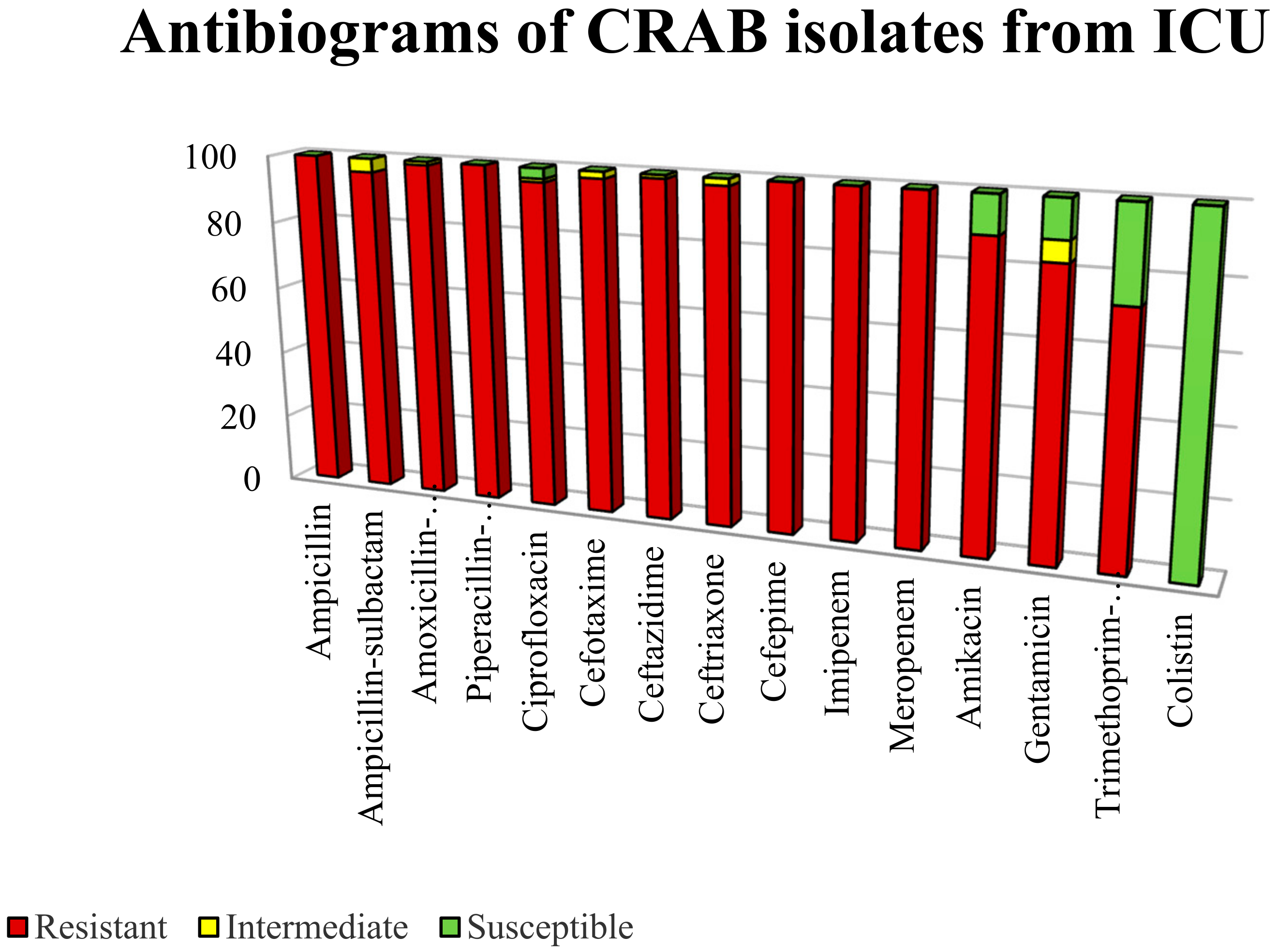
2.2. Antimicrobial Susceptibility Profiles
2.3. Screening of Carbapenemase and Extended-Spectrum β-Lactamases (ESBL) Genes
2.4. Carbapenem-Associated Outer Membrane Protein (CarO) Gene Analysis
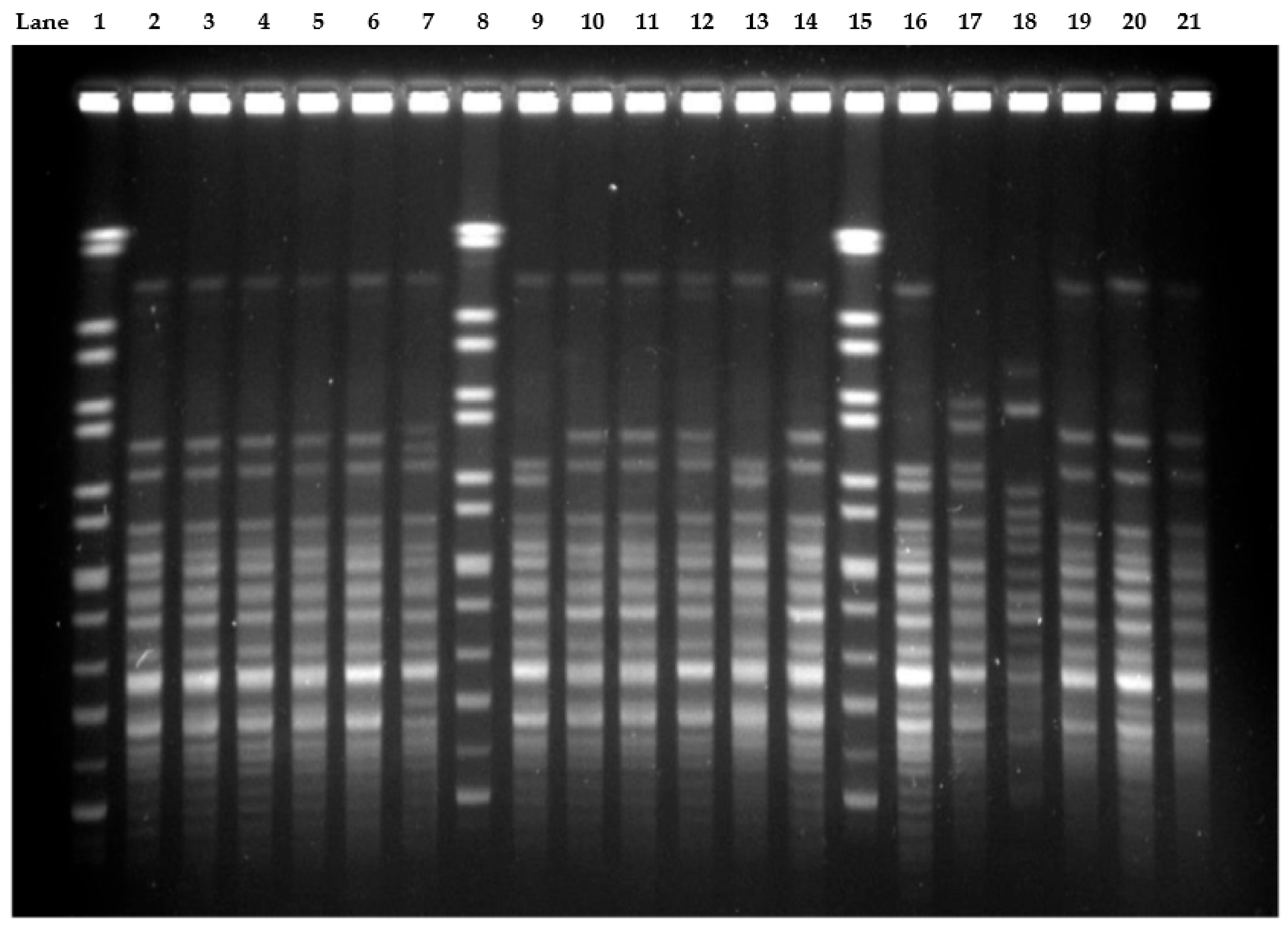
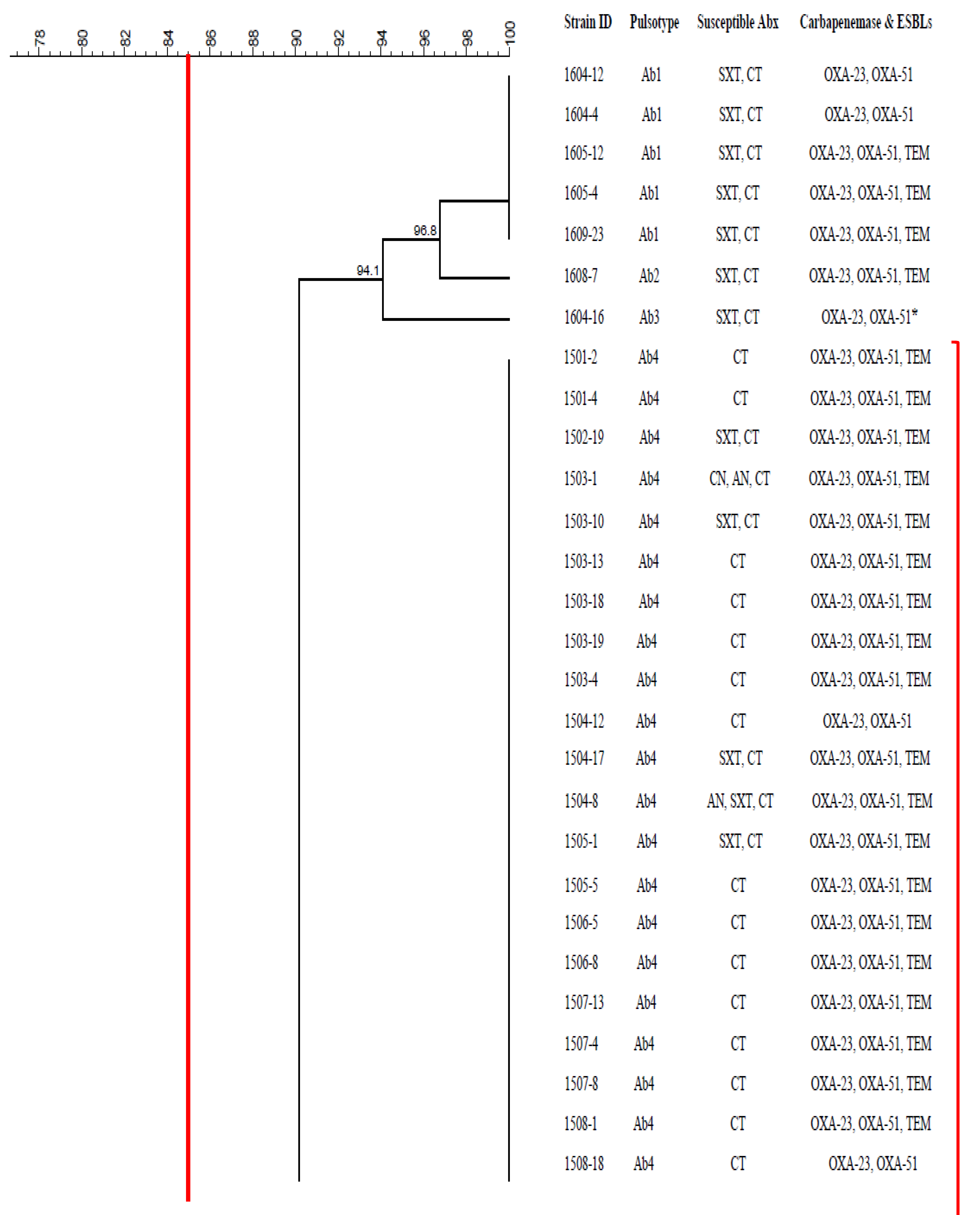
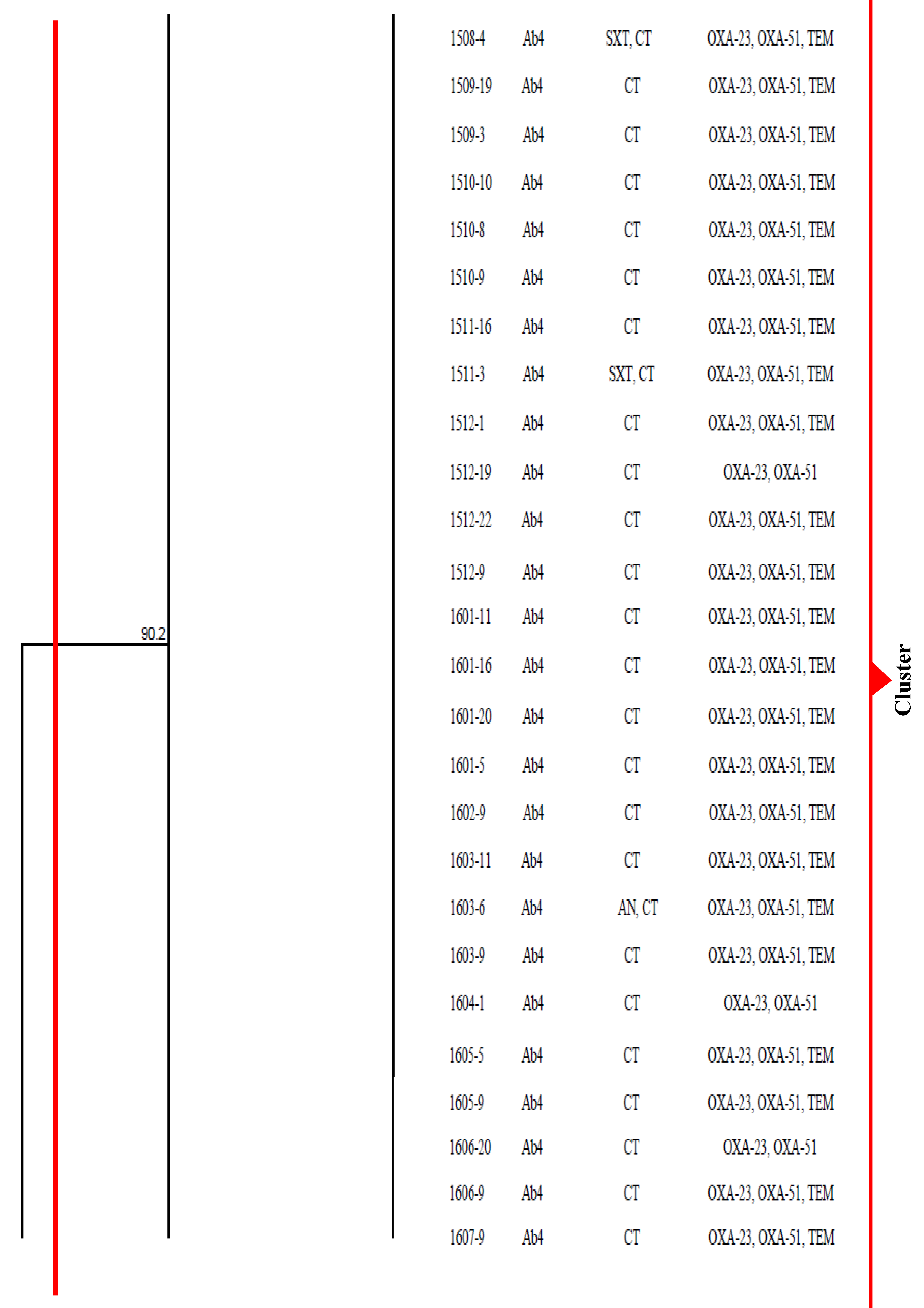
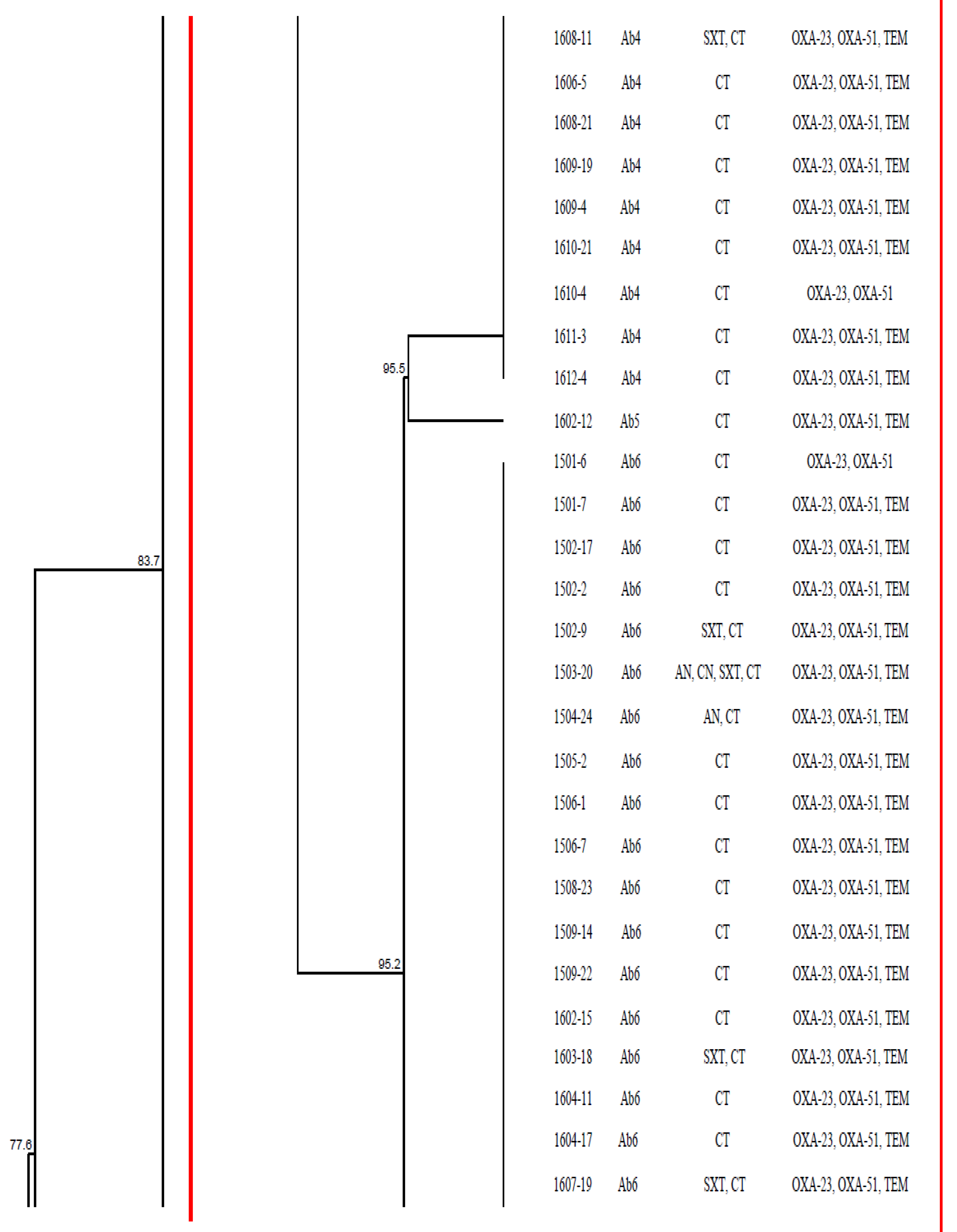
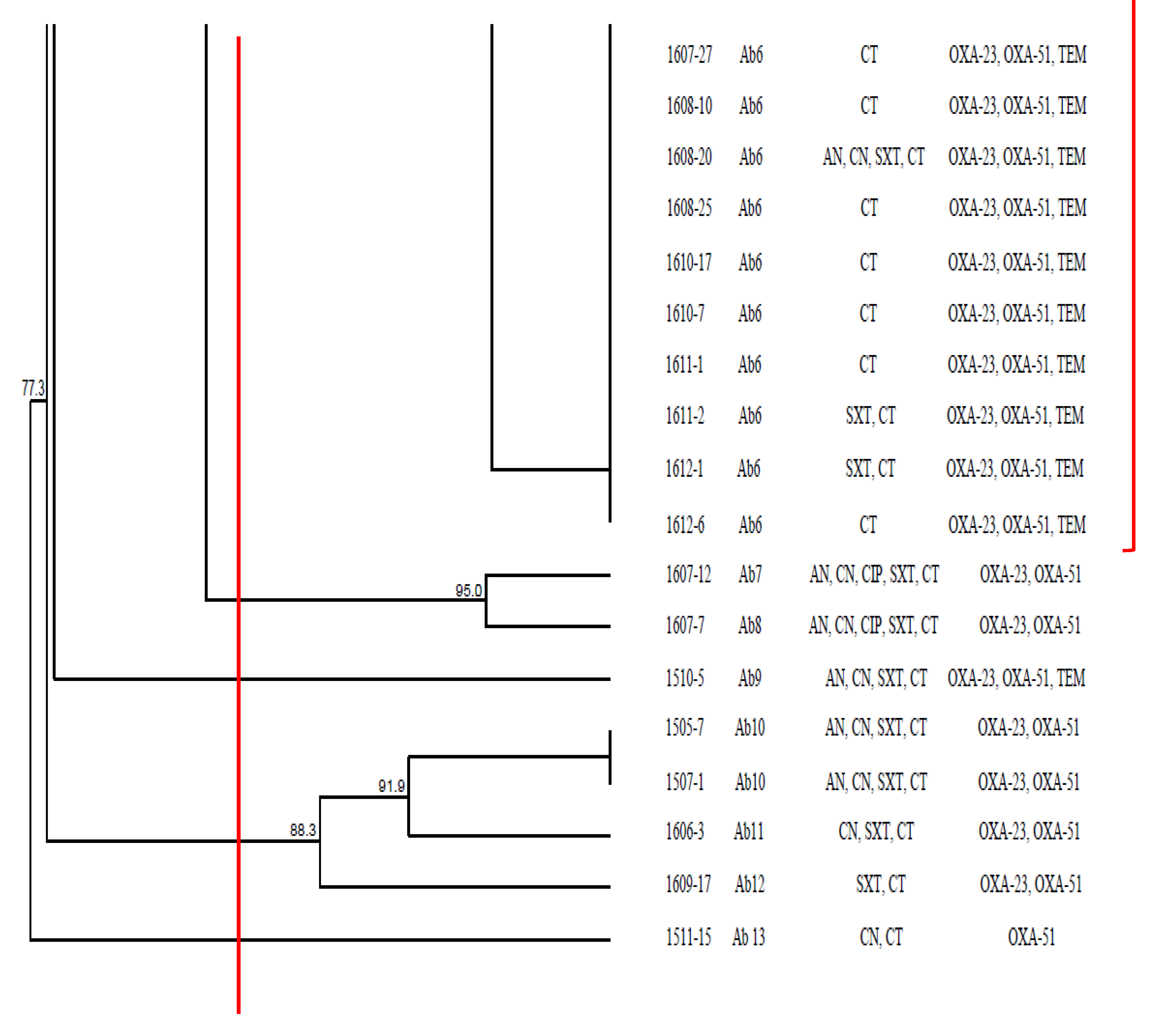
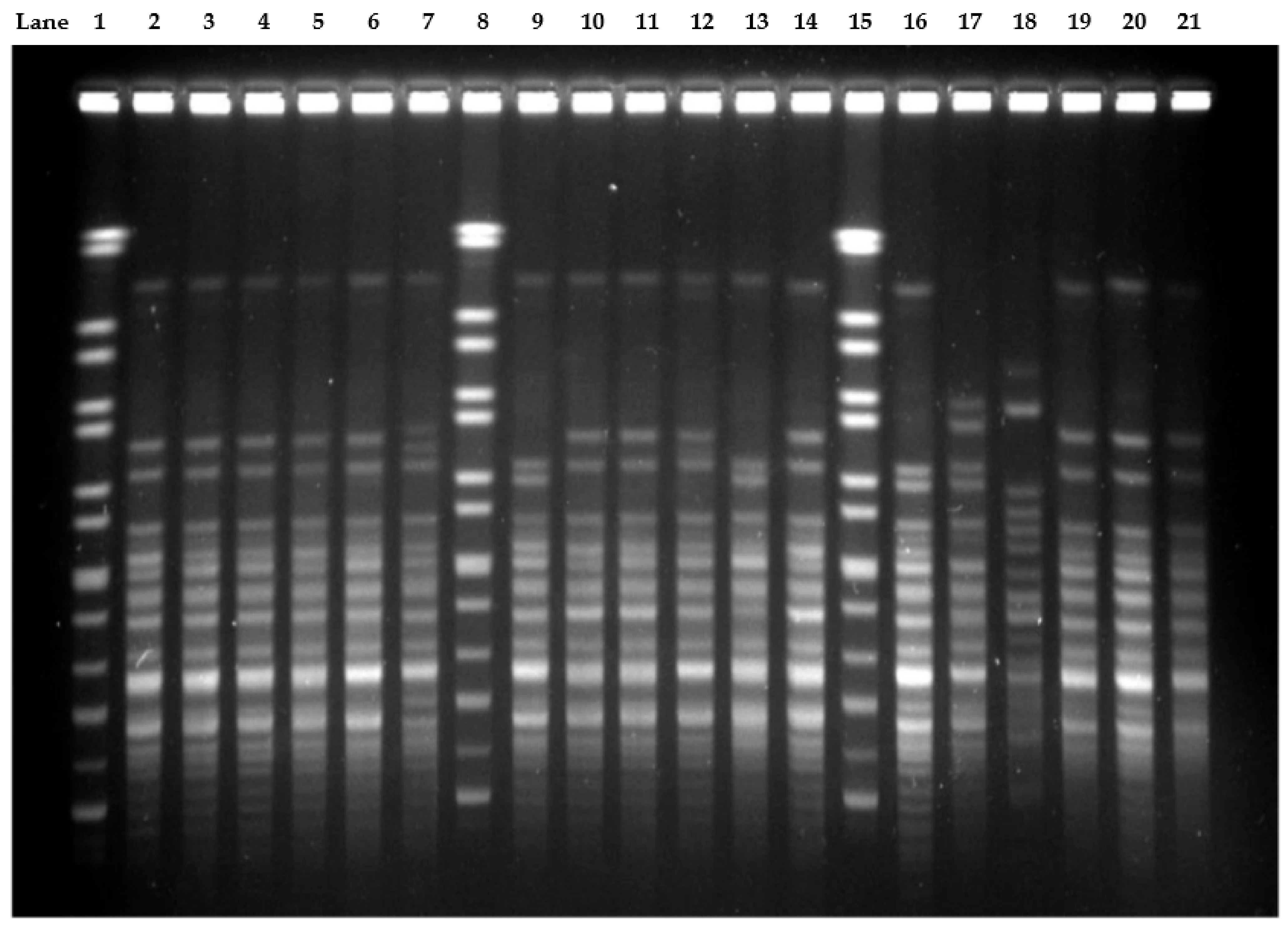
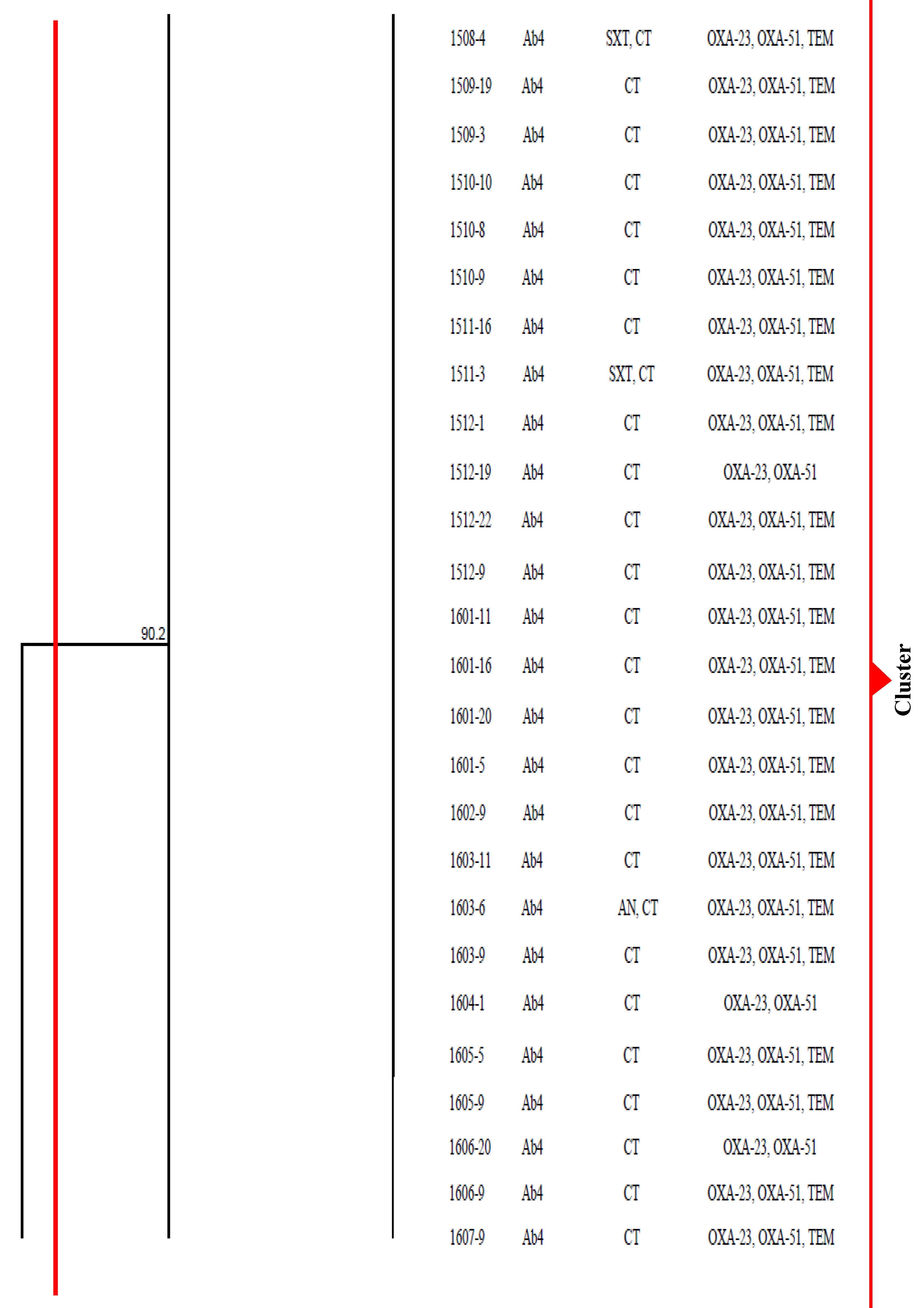
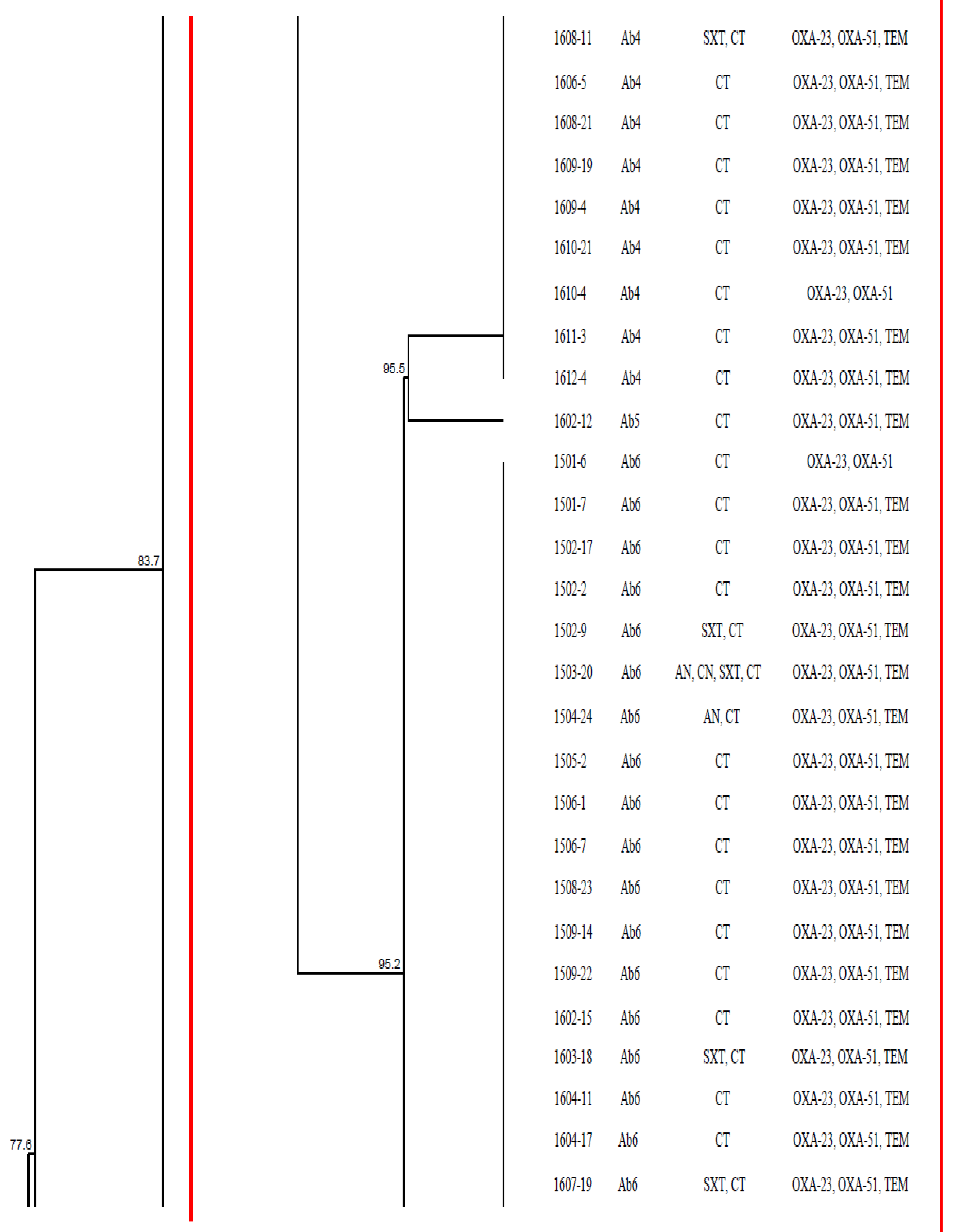
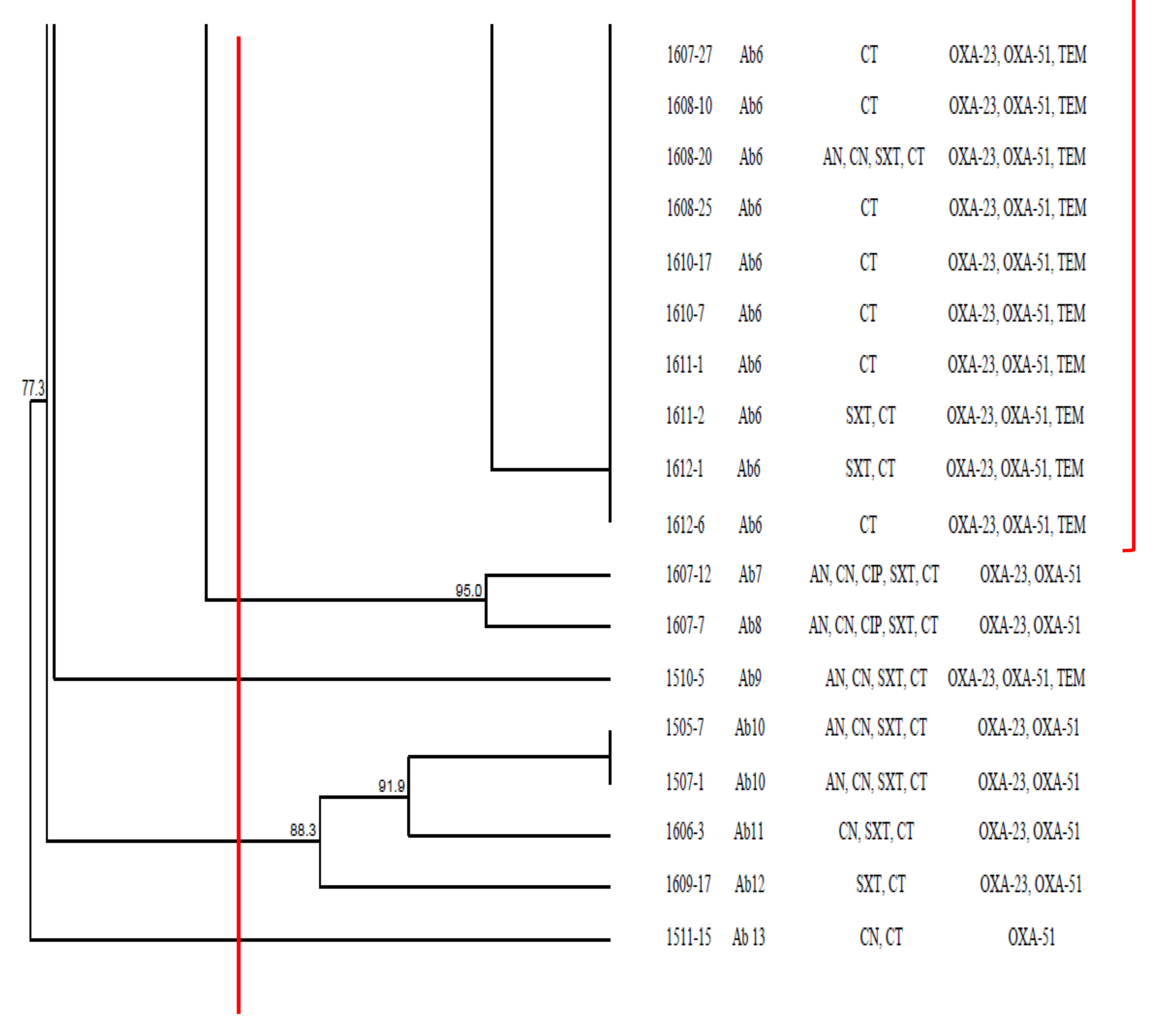
2.5. Genetic Relatedness of CRAB Isolates
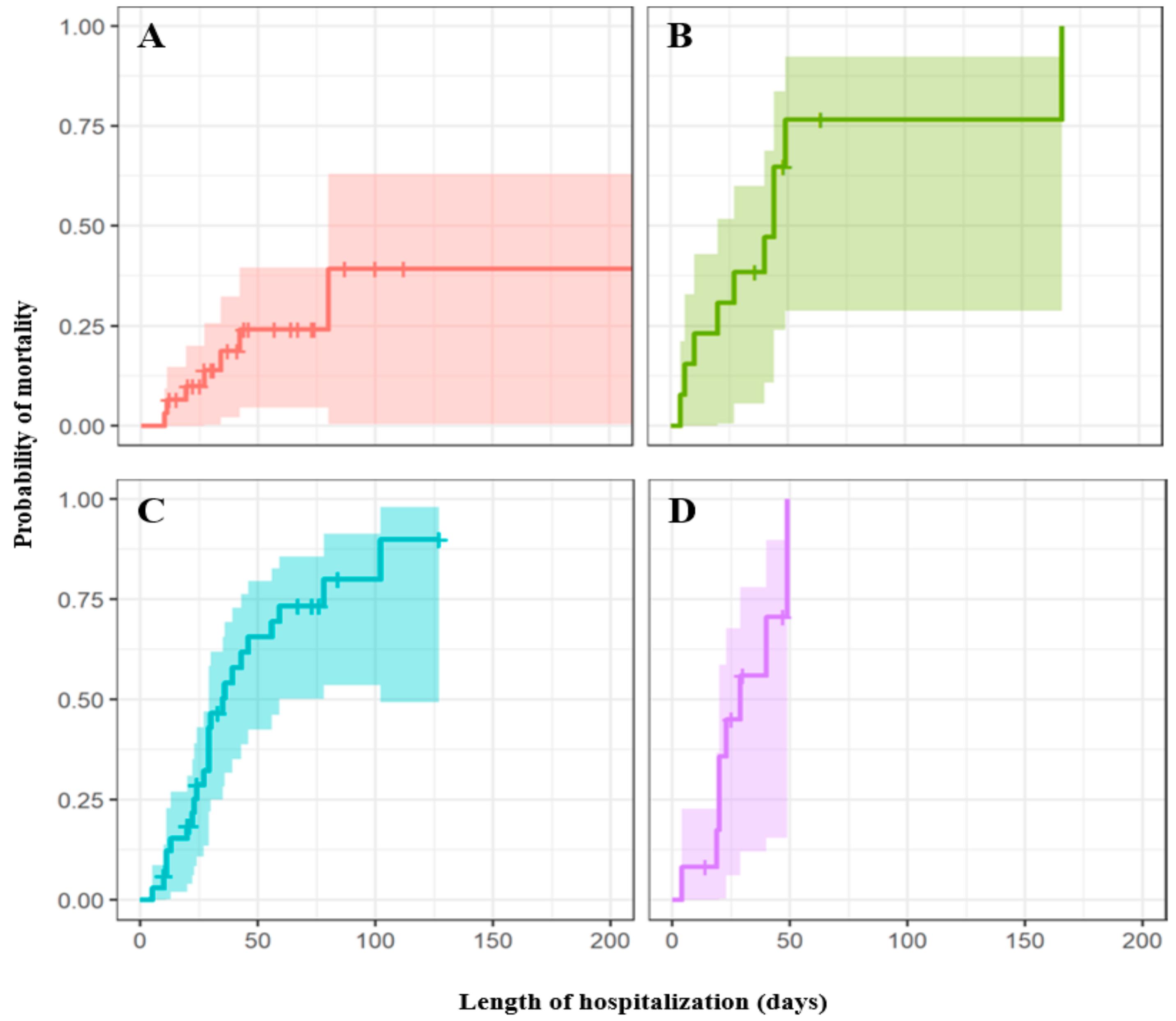
2.6. Cox Proportional Hazards Regression Model for Risk Factors Analysis
3. Discussion
4. Materials and Methods
4.1. Ethical Clearance
4.2. Study Setting, Bacterial Strain Collection and Identification
4.3. Antimicrobial Susceptibility Testing
4.4. Carbapenemase and Extended-Spectrum β-Lactamase Genes Screening (ESBL)
4.5. CarO Gene Screening and Amino Acid Sequence Alignment
4.6. Pulsed-Field Gel Electrophoresis (PFGE)
4.7. Clinical Data Collection and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Brink, A.J. Epidemiology of carbapenem-resistant Gram-negative infections globally. Curr. Opin. Infect. Dis. 2019, 32, 609–616. [Google Scholar] [CrossRef]
- Wong, D.; Nielsen, T.B.; Bonomo, R.A.; Pantapalangkoor, P.; Luna, B.; Spellberg, B. Clinical and pathophysiological overview of Acinetobacter infections: A century of challenges. Clin. Microbiol. Rev. 2017, 30, 409–447. [Google Scholar] [CrossRef] [Green Version]
- Liang, C.A.; Lin, Y.C.; Lu, P.L.; Chen, H.C.; Chang, H.L.; Sheu, C.C. Antibiotic strategies and clinical outcomes in critically ill patients with pneumonia caused by carbapenem-resistant Acinetobacter baumannii. Clin. Microbiol. Infect. 2018, 24, 908.e1–908.e7. [Google Scholar] [CrossRef] [Green Version]
- Du, X.; Xu, X.; Yao, J.; Deng, K.; Chen, S.; Shen, Z.; Yang, L.; Feng, G. Predictors of mortality in patients infected with carbapenem-resistant Acinetobacter baumannii: A systematic review and meta-analysis. Am. J. Infect. Control 2019, 47, 1140–1145. [Google Scholar] [CrossRef] [Green Version]
- Piperaki, E.T.; Tzouvelekis, L.; Miriagou, V.; Daikos, G. Carbapenem-resistant Acinetobacter baumannii: In pursuit of an effective treatment. Clin. Microbiol. Infect. 2019, 25, 951–957. [Google Scholar] [CrossRef]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. World health organization releases global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. J. Medic. Soc. 2018, 32, 76. [Google Scholar] [CrossRef]
- Gonzalez-Villoria, A.M.; Valverde-Garduno, V. Antibiotic-resistant Acinetobacter baumannii increasing success remains a challenge as a nosocomial pathogen. J. Pathog. 2016, 2016, 7318075. [Google Scholar] [CrossRef] [Green Version]
- Rahman, A.; Iza, N.; Ismail, S.; Alattraqchi, A.G.; Cleary, D.W.; Clarke, S.C.; Yeo, C.C. Acinetobacter spp. infections in Malaysia: A review of antimicrobial resistance trends, mechanisms and epidemiology. Front. Microbiol. 2017, 8, 2479. [Google Scholar]
- Peleg, A.Y.; Seifert, H.; Paterson, D.L. Acinetobacter baumannii: Emergence of a successful pathogen. Clin. Microbiol. Rev. 2008, 21, 538–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vijayakumar, S.; Mathur, P.; Kapil, A.; Das, B.K.; Ray, P.; Gautam, V.; Sistla, S. Molecular characterization & epidemiology of carbapenem-resistant Acinetobacter baumannii collected across India. Indian J. Med. Res. 2019, 149, 240. [Google Scholar] [PubMed]
- Zowawi, H.M.; Sartor, A.L.; Sidjabat, H.E.; Balkhy, H.H.; Walsh, T.R.; Al Johani, S.M.; Al Jindan, R.Y.; Alfaresi, M.; Ibrahim, E.; Al-Jardani, A.; et al. Molecular epidemiology of carbapenem-resistant Acinetobacter baumannii isolates in the Gulf Cooperation Council States: Dominance of OXA-23-type producers. J. Clin. Microbiol. 2015, 53, 896–903. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Guo, Q.; Wang, P.; Zhu, D.; Ye, X.; Wu, S. Wang, M. Clonal dissemination of extensively drug-resistant Acinetobacter baumannii producing an OXA-23 β-lactamase at a teaching hospital in Shanghai, China. J. Microbiol. Immunol. 2015, 48, 101–108. [Google Scholar]
- Wieland, K.; Chhatwal, P.; Vonberg, R.P. Nosocomial outbreaks caused by Acinetobacter baumannii and Pseudomonas aeruginosa: Results of a systematic review. Am. J. Infect. Control 2018, 46, 643–648. [Google Scholar] [CrossRef]
- Saharman, Y.R.; Karuniawati, A.; Sedono, R.; Aditianingsih, D.; Sudarmono, P.; Goessens, W.H.; Klaassen, C.H.; Verbrugh, H.A.; Severin, J.A. Endemic carbapenem-nonsusceptible Acinetobacter baumannii-calcoaceticus complex in intensive care units of the national referral hospital in Jakarta, Indonesia. Antimicrob. Resist. Infect. Control 2018, 7, 5. [Google Scholar] [CrossRef] [Green Version]
- Schultz, M.B.; Thanh, D.P.; Do Hoan, N.T.; Wick, R.R.; Ingle, D.J.; Hawkey, J.; Edwards, D.J.; Kenyon, J.J.; Lan, N.P.H.; Campbell, J.I.; et al. Repeated local emergence of carbapenem-resistant Acinetobacter baumannii in a single hospital ward. Microb. Genom. 2016, 2, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ning, N.Z.; Liu, X.; Bao, C.M.; Chen, S.M.; Cui, E.B.; Huang, J.; Chen, F.H.; Li, T.; Qu, F.; Wang, H. Molecular epidemiology of bla OXA-23-producing carbapenem-resistant Acinetobacter baumannii in a single institution over a 65-month period in north China. BMC. Infect. Dis. 2017, 17, 14. [Google Scholar] [CrossRef] [Green Version]
- Lean, S.S.; Yeo, C.C.; Suhaili, Z.; Thong, K.L. Whole-genome analysis of an extensively drug-resistant clinical isolate of Acinetobacter baumannii AC12: Insights into the mechanisms of resistance of an ST195 clone from Malaysia. Int. J. Antimicrob. Agents 2015, 45, 178–182. [Google Scholar] [CrossRef]
- Lean, S.S.; Yeo, C.C.; Suhaili, Z.; Thong, K.L. Comparative genomics of two ST 195 carbapenem-resistant Acinetobacter baumannii with different susceptibility to polymyxin revealed underlying resistance mechanism. Front. Microbiol. 2016, 6, 1445. [Google Scholar] [CrossRef] [Green Version]
- Weinberg, S.; Villedieu, A.; Bagdasarian, N.; Karah, N.; Teare, L.; Elamin, W. Control and management of multidrug resistant Acinetobacter baumannii: A review of the evidence and proposal of novel approaches. Infect. Prev. Pract. 2020, 100077. [Google Scholar] [CrossRef]
- Wang, J.; Niu, H.; Wang, R.; Cai, Y. Safety and efficacy of colistin alone or in combination in adults with Acinetobacter baumannii infection: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2019, 53, 383–400. [Google Scholar] [CrossRef] [PubMed]
- University of Malaya Medical Centre. UMMC On-Line Antibiotic Guideline 2020. Available online: https://farmasi.ummc.edu.my/ummc-on-line-antibiotic-guideline (accessed on 28 June 2021).
- Takebayashi, Y.; Findlay, J.; Heesom, K.J.; Warburton, P.J.; Avison, M.B.; Evans, B.A. Variability in carbapenemase activity of intrinsic OxaAb (OXA-51-like) β-lactamase enzymes in Acinetobacter baumannii. J. Antimicrob. Chemother. 2021, 76, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Hsu, L.Y.; Apisarnthanarak, A.; Khan, E.; Suwantarat, N.; Ghafur, A.; Tambyah, P.A. Carbapenem-resistant Acinetobacter baumannii and Enterobacteriaceae in south and southeast Asia. Clin. Microbiol. Rev. 2017, 30, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aghamali, M.; Bialvaei, A.Z.; Aghazadeh, M.; Asgharzadeh, M.; Kafil, H.S. Carbapenemase inhibitors. Rev. Med. Microbiol. 2017, 28, 104–113. [Google Scholar] [CrossRef]
- Wong, M.H.Y.; Chan, B.K.W.; Chan, E.W.C.; Chen, S. Over-expression of ISAba1-linked intrinsic and exogenously acquired OXA type carbapenem-hydrolyzing-class D-ß-lactamase-encoding genes is key mechanism underlying carbapenem resistance in Acinetobacter baumannii. Front. Microbiol. 2019, 10, 2809. [Google Scholar] [CrossRef] [Green Version]
- Sen, B.; Joshi, S. Studies on Acinetobacter baumannii involving multiple mechanisms of carbapenem resistance. J. Appl. Microbiol. 2016, 120, 619–629. [Google Scholar] [CrossRef]
- Catel-Ferreira, M.; Coadou, G.; Molle, V.; Mugnier, P.; Nordmann, P.; Siroy, A.; Jouenne, T.; De, E. Structure–function relationships of CarO, the carbapenem resistance-associated outer membrane protein of Acinetobacter baumannii. J. Antimicrob. Chemother. 2011, 66, 2053–2056. [Google Scholar] [CrossRef] [Green Version]
- Lu, P.L.; Doumith, M.; Livermore, D.M.; Chen, T.P.; Woodford, N. Diversity of carbapenem resistance mechanisms in Acinetobacter baumannii from a Taiwan hospital: Spread of plasmid-borne OXA-72 carbapenemase. J. Antimicrob. Chemother. 2009, 63, 641–647. [Google Scholar] [CrossRef]
- Mussi, M.A.; Limansky, A.S.; Viale, A.M. Acquisition of resistance to carbapenems in multidrug-resistant clinical strains of Acinetobacter baumannii: Natural insertional inactivation of a gene encoding a member of a novel family of β-barrel outer membrane proteins. Antimicrob. Agents. Chemother. 2005, 49, 1432–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fonseca, E.L.; Scheidegger, E.; Freitas, F.S.; Cipriano, R.; Vicente, A.C.P. Carbapenem-resistant Acinetobacter baumannii from Brazil: Role of car O alleles expression and bla OXA-23 gene. BMC Microbiol. 2013, 13, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Metan, G.; Zarakolu, P.; Otlu, B.; Tekin, I.; Aytaç, H.; Bölek, E.Ç.; Metin, B.C.; Arsava, E.M.; Unal, S. Emergence of colistin and carbapenem-resistant Acinetobacter calcoaceticus-Acinetobacter baumannii (CCR-Acb) complex in a neurological intensive care unit followed by successful control of the outbreak. J. Infect. Public. Health 2020, 13, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Al-Hamad, A.; Pal, T.; Leskafi, H.; Abbas, H.; Hejles, H.; Alsubikhy, F.; Darwish, D.; Ghazawi, A.; Sonnevend, A. Molecular characterization of clinical and environmental carbapenem resistant Acinetobacter baumannii isolates in a hospital of the Eastern Region of Saudi Arabia. J. Infect. Public Health 2020, 13, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Neoh, H.M.; Tan, X.E.; Sapri, H.F.; Tan, T.L. Pulsed-field gel electrophoresis (PFGE): A review of the “gold standard” for bacteria typing and current alternatives. Infect. Genet. Evol. 2019, 74, 103935. [Google Scholar] [CrossRef]
- Dhanoa, A.; Rajasekaram, G.; Lean, S.S.; Cheong, Y.M.; Thong, K.L. Endemicity of Acinetobacter calcoaceticus-baumannii complex in an intensive care unit in Malaysia. J. Pathog. 2015, 2015. [Google Scholar] [CrossRef] [Green Version]
- Kong, B.H.; Hanifah, Y.A.; Yusof, M.Y.M.; Thong, K.L. Antimicrobial susceptibility profiling and genomic diversity of multidrug-resistant Acinetobacter baumannii isolates from a teaching hospital in Malaysia. Jpn. J. Infect. Dis. 2011, 64, 337–340. [Google Scholar]
- Timsit, J.F.; Bassetti, M.; Cremer, O.; Daikos, G.; De Waele, J.; Kallil, A.; Kipnis, E.; Kollef, M.; Laupland, K.; Paiva, J.A.; et al. Rationalizing antimicrobial therapy in the ICU: A narrative review. Intens. Care. Med. 2019, 45, 172–189. [Google Scholar] [CrossRef] [PubMed]
- Suranadi, I.W.; Fatmawati, N.; Aryabiantara, I.W.; Sinardja, C.D.; Saputra, D.J.; Senapathi, T.G.A.; Widnyana, I.M.G.; Nada, I.K.W.; Astuti, M.K.; Kumara, V.; et al. Acinetobacter baumannii is an opportunistic pathogen as an MDRO in ICU. Bali. J. Anesthesiol. 2019, 3, 150–153. [Google Scholar] [CrossRef] [Green Version]
- Ababneh, Q.; Abulaila, S.; Jaradat, Z. Isolation of extensively drug resistant Acinetobacter baumannii from environmental surfaces inside intensive care units. Am. J. Infect. Control 2021. [Google Scholar] [CrossRef]
- Hassan, W.M.N.W.; Puzizer, M.S.; Deris, Z.Z.; Zaini, R.H.M. Carbapenem resistant Acinetobacter Species infection in intensive care unit: The outcome and risk factors of mortality. Bangladesh. J. Med. Sci. 2020, 19, 98–104. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Yao, Y.; Zhu, B.; Ren, D.; Yang, Q.; Fu, Y.; Yu, Y.; Zhou, J. Risk factors for acquisition and mortality of multidrug-resistant Acinetobacter baumannii bacteremia: A retrospective study from a Chinese hospital. Medicine 2019, 98, e14937. [Google Scholar] [CrossRef]
- Lemos, E.; de La Hoz, F.; Einarson, T.; McGhan, W.; Quevedo, E.; Castañeda, C.; Kawai, K. Carbapenem resistance and mortality in patients with Acinetobacter baumannii infection: Systematic review and meta-analysis. Clin. Microbiol. Infect. 2014, 20, 416–423. [Google Scholar] [CrossRef] [Green Version]
- Karakonstantis, S.; Gikas, A.; Astrinaki, E.; Kritsotakis, E.I. Excess mortality due to pandrug-resistant Acinetobacter baumannii infections in hospitalized patients. J. Hosp. Infect. 2020, 106, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Falciglia, M.; Freyberg, R.W.; Almenoff, P.L.; D’Alessio, D.A.; Render, M.L. Hyperglycemia-related mortality in critically ill patients varies with admission diagnosis. Crit. Care. Med. 2009, 37, 3001. [Google Scholar] [CrossRef]
- Lee, I.R.; Molton, J.S.; Wyres, K.L.; Gorrie, C.; Wong, J.; Hoh, C.H.; Teo, J.; Kalimuddin, S.; Lye, D.C.; Archuleta, S.; et al. Differential host susceptibility and bacterial virulence factors driving Klebsiella liver abscess in an ethnically diverse population. Sci. Rep. 2016, 6, 1–12. [Google Scholar]
- Garnacho-Montero, J.; Amaya-Villar, R. Multiresistant Acinetobacter baumannii infections: Epidemiology and management. Curr. Opin. Infect. Dis. 2010, 23, 332–339. [Google Scholar] [CrossRef]
- Sileem, A.E.; Said, A.M.; Meleha, M.S. Acinetobacter baumannii in ICU patients: A prospective study highlighting their incidence, antibiotic sensitivity pattern and impact on ICU stay and mortality. Egypt. J. Chest. Dis. Tuberc. 2017, 66, 693–698. [Google Scholar] [CrossRef]
- Chen, T.L.; Siu, L.K.; Wu, R.C.; Shaio, M.F.; Huang, L.Y.; Fung, C.P.; Lee, C.M.; Cho, W.L. Comparison of one-tube multiplex PCR, automated ribotyping and intergenic spacer (ITS) sequencing for rapid identification of Acinetobacter baumannii. Clin. Microbiol. Infect. 2007, 13, 801–806. [Google Scholar] [CrossRef] [Green Version]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 27th ed.; CLSI supplement M100; Clinical and Laboratory Standard Institute: Wayne, PA, USA, 2017; Available online: https://clsi.org/media/1469/m100s27_sample.pdf (accessed on 31 May 2021).
- Alyamani, E.J.; Khiyami, M.A.; Booq, R.Y.; Alnafjan, B.M.; Altammami, M.A.; Bahwerth, F.S. Molecular characterization of extended-spectrum beta-lactamases (ESBLs) produced by clinical isolates of Acinetobacter baumannii in Saudi Arabia. Ann. Clin. Microbiol. Antimicrob. 2015, 14, 38. [Google Scholar]
- Shoja, S.; Moosavian, M.; Rostami, S.; Abbasi, F.; Tabatabaiefar, M.A.; Peymani, A. Characterization of Oxacillinase and Metallo-β-Lactamas genes and molecular typing of clinical isolates of Acinetobacter baumannii in Ahvaz, south-west of Iran. Jundishapur. J. Microb. 2016, 9, e32388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn. Microbiol. Infect. Dis. 2011, 70, 119–123. [Google Scholar] [CrossRef]
- Woodford, N.; Ellington, M.J.; Coelho, J.M.; Turton, J.F.; Ward, M.E.; Brown, S.; Amyes, S.G.; Livermore, D.M. Multiplex PCR for genes encoding prevalent OXA carbapenemases in Acinetobacter spp. Int. J. Antimicrob. Agents 2006, 27, 351–353. [Google Scholar] [CrossRef] [PubMed]
- Seifert, H.; Dolzani, L.; Bressan, R.; van der Reijden, T.; van Strijen, B.; Stefanik, D.; Heersma, H.; Dijkshoorn, L. Standardization and interlaboratory reproducibility assessment of pulsed-field gel electrophoresis-generated fingerprints of Acinetobacter baumannii. J. Clin. Microbiol. 2005, 43, 4328–4335. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Factors | In-Hospital Mortality | p-Value 1 | |
|---|---|---|---|
| Survivor (n = 41) | Non-Survivor (n = 48) | ||
| Gender | 0.309 | ||
| Male | 29 (50.0%) | 29 (50.0%) | |
| Female | 12 (38.7%) | 19 (61.3%) | |
| Classification of isolates | 0.006 2 | ||
| Colonization | 21 (65.5%) | 11 (34.5%) | |
| Infection | 20 (35.1%) | 37 (64.9%) | |
| Age | 0.003 | ||
| ≤50 years old | 23 (65.7%) | 12 (34.3%) | |
| >50 years old | 18 (33.3%) | 36 (66.7%) | |
| Septic shock during CRAB isolation | 0.501 | ||
| Yes | 21 (42.9%) | 28 (57.1%) | |
| No | 20 (50.0%) | 20 (50.0%) | |
| Ethnicity | |||
| Chinese | 7 (28.0%) | 18 (72.0%) | 0.033 |
| Malay | 12 (44.4%) | 15 (55.6%) | 0.839 |
| Indian | 14 (48.3%) | 15 (51.7%) | 0.771 |
| Others | 8 (100%) | 0 | 0.001 |
| Specimen source | |||
| Respiratory | 29 (49.2%) | 30 (50.8%) | 0.413 |
| Urinary | 3 (75.0%) | 1 (25.0%) | 0.235 |
| Blood | 5 (31.3%) | 11 (68.7%) | 0.189 |
| Skin and soft tissue | 4 (57.1%) | 3 (42.9%) | 0.540 |
| Others | 0 | 3 (100%) | 0.103 |
| Comorbidity | |||
| No known medical illness | 15 (68.2%) | 7 (31.8%) | 0.016 |
| Diabetes mellitus | 14 (31.1%) | 31 (68.9%) | 0.004 |
| Hypertension | 19 (37.3%) | 32 (62.7%) | 0.053 |
| Malignancy | 3 (27.3%) | 8 (72.7%) | 0.182 |
| Kidney disease | 9 (39.1%) | 14 (60.9%) | 0.438 |
| Cardiovascular disease | 3 (18.8%) | 13 (81.2%) | 0.015 |
| Endocrine and metabolic disorder | 6 (42.9%) | 8 (57.1%) | 0.793 |
| Respiratory disease | 2 (20.0%) | 8 (80.0%) | 0.079 |
| Skin disease | 1 (100%) | 0 | 0.277 |
| Bone and joint disease | 1 (50.0%) | 1 (50.0%) | 0.910 |
| Brain and neurological disorder | 1 (20.0%) | 4 (80.0%) | 0.229 |
| Liver and pancreas disease | 1 (50.0%) | 1 (50.0%) | 0.910 |
| Gastrointestinal disease | 1 (100%) | 0 | 0.277 |
| Blood and immune disease | 2 (50.0%) | 2 (50.0%) | 0.872 |
| Empiric treatment (n = 57) | |||
| Beta-lactamase/Beta-lactamase inhibitor | 10 (41.7%) | 14 (58.3%) | 0.375 |
| Tetracycline | 1 (100%) | 0 | 0.170 |
| Trimethoprim–sulfamethoxazole | 1 (33.3%) | 2 (66.7%) | 0.948 |
| Carbapenem | 8 (23.5%) | 26 (76.5%) | 0.026 |
| Colistin | 0 | 4 (100%) | 0.127 |
| Definitive treatment (n = 57) | 0.700 | ||
| Within 3 days | 2 (28.6%) | 5 (71.4%) | |
| More than 3 days | 18 (36.0%) | 32 (64.0%) | |
| Length of hospitalization stay | 51.66 ± 38.317 | 33.65 ± 28.312 | 0.003 |
| Length of ICU stay | 20.10 ± 15.043 | 21.06 ± 16.015 | 0.699 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio (HR) | 95% CI for HR | p Value | Odds Ratio | 95% CI for HR | p Value | |
| Gender | 0.94 | 0.52–1.70 | 0.83 | |||
| Classification of isolates | 1.60 | 0.83–3.20 | 0.15 | |||
| Age group | 0.45 | 0.23–0.86 | 0.016 | |||
| Septic shock during CRAB isolation | 1.40 | 0.80–2.50 | 0.24 | |||
| Ethnic | ||||||
| Chinese | 1.90 | 1.10–3.50 | 0.032 | 2.13 | 1.17–3.89 | 0.014 |
| Malay | 1.10 | 0.57–2.00 | 0.85 | |||
| Indian | 0.83 | 0.44–1.50 | 0.55 | |||
| Others | 1.30 × 10−8 | 0.00–lnF | 1.00 | |||
| Specimen source | 1.20 | 0.95–1.50 | 0.12 | |||
| Comorbidity | ||||||
| No known medical illness | 0.46 | 0.21–1.00 | 0.06 | |||
| Diabetes mellitus | 2.40 | 1.30–4.40 | 0.0045 | 2.59 | 1.40–4.78 | 0.002 |
| Hypertension | 1.60 | 0.88–2.90 | 0.12 | |||
| Malignancy | 1.70 | 0.78–3.60 | 0.19 | |||
| Kidney disease | 1.40 | 0.75–2.60 | 0.30 | |||
| Cardiovascular disease | 2.30 | 1.20–4.30 | 0.013 | |||
| Endocrine and metabolic disorder | 0.98 | 0.46–2.10 | 0.96 | |||
| Respiratory disease | 1.40 | 0.63–3.00 | 0.43 | |||
| Skin disease | 3.00 × 10−7 | 0.00–lnF | 1.00 | |||
| Bone and joint disease | 0.80 | 0.11–5.80 | 0.82 | |||
| Brain and neurological disorder | 2.30 | 0.83–6.60 | 0.11 | |||
| Liver and pancreatic disease | 1.50 | 0.21–11.0 | 0.68 | |||
| Gastrointestinal disease | 1.10 ×10−7 | 0.00–lnF 1 | 1.00 | |||
| Blood and immune disease | 1.10 | 0.26–4.50 | 0.92 | |||
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio (HR) | 95% CI for HR | p Value | Odds Ratio | 95% CI for HR | p Value | |
| Gender | 0.98 | 0.50–1.90 | 0.94 | |||
| Age group | 0.78 | 0.37–1.60 | 0.51 | |||
| Septic shock during CRAB isolation | 1.50 | 0.74–3.00 | 0.27 | |||
| Ethnic | ||||||
| Chinese | 1.60 | 0.82–3.20 | 0.17 | |||
| Malay | 0.93 | 0.46–1.90 | 0.83 | |||
| Indian | 0.91 | 0.44–1.90 | 0.79 | |||
| Others | 1.30 × 10−8 | 0.00–lnF | 1.00 | |||
| Specimen source | 1.10 | 0.89–1.40 | 0.30 | |||
| Comorbidity | ||||||
| No known medical illness | 0.52 | 0.20–1.30 | 0.18 | |||
| Diabetes mellitus | 1.80 | 0.91–3.70 | 0.091 | |||
| Hypertension | 1.50 | 0.75–3.00 | 0.25 | |||
| Malignancy | 2.40 | 0.97–6.10 | 0.057 | 3.297 | 1.098–9.897 | 0.0334 |
| Kidney disease | 1.70 | 0.86–3.50 | 0.12 | |||
| Cardiovascular disease | 3.50 | 1.50–8.20 | 0.003 | 5.804 | 2.315–14.553 | 0.0002 |
| Endocrine and metabolic disorder | 1.10 | 0.44–2.60 | 0.88 | |||
| Respiratory disease | 1.10 | 0.46–2.70 | 0.81 | |||
| Skin disease | 8.10 × 10−7 | 0.00–lnF 1 | 1.00 | |||
| Bone and joint disease | 1.50 | 0.20–11.0 | 0.71 | |||
| Brain and neurological disorder | 17.0 | 3.30–89.0 | 0.00072 | 42.614 | 7.34–247.406 | 0.00003 |
| Liver and pancreatic disease | 3.80 | 0.50–29.0 | 0.20 | |||
| Blood and immune disease | 7.60 | 1.60–35.0 | 0.01 | 7.232 | 1.237–41.089 | 0.0256 |
| Empiric treatment | ||||||
| Β-lactam/Β-lactam inhibitor | 0.61 | 0.30–1.20 | 0.17 | |||
| Tetracycline | 3.90 × 10−8 | 0.00–lnF | 1.00 | |||
| Trimethoprim–sulfamethoxazole | 1.10 ×10−8 | 0.00–lnF | 1.00 | |||
| Carbapenem | 1.80 | 0.85–3.70 | 0.13 | |||
| Colistin | 1.90 | 0.67–5.60 | 0.22 | |||
| Appropriate treatment with 3 days | 1.10 | 0.41–2.80 | 0.89 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woon, J.J.; Teh, C.S.J.; Chong, C.W.; Abdul Jabar, K.; Ponnampalavanar, S.; Idris, N. Molecular Characterization of Carbapenem-Resistant Acinetobacter baumannii Isolated from the Intensive Care Unit in a Tertiary Teaching Hospital in Malaysia. Antibiotics 2021, 10, 1340. https://doi.org/10.3390/antibiotics10111340
Woon JJ, Teh CSJ, Chong CW, Abdul Jabar K, Ponnampalavanar S, Idris N. Molecular Characterization of Carbapenem-Resistant Acinetobacter baumannii Isolated from the Intensive Care Unit in a Tertiary Teaching Hospital in Malaysia. Antibiotics. 2021; 10(11):1340. https://doi.org/10.3390/antibiotics10111340
Chicago/Turabian StyleWoon, Jia Jie, Cindy Shuan Ju Teh, Chun Wie Chong, Kartini Abdul Jabar, Sasheela Ponnampalavanar, and Nuryana Idris. 2021. "Molecular Characterization of Carbapenem-Resistant Acinetobacter baumannii Isolated from the Intensive Care Unit in a Tertiary Teaching Hospital in Malaysia" Antibiotics 10, no. 11: 1340. https://doi.org/10.3390/antibiotics10111340
APA StyleWoon, J. J., Teh, C. S. J., Chong, C. W., Abdul Jabar, K., Ponnampalavanar, S., & Idris, N. (2021). Molecular Characterization of Carbapenem-Resistant Acinetobacter baumannii Isolated from the Intensive Care Unit in a Tertiary Teaching Hospital in Malaysia. Antibiotics, 10(11), 1340. https://doi.org/10.3390/antibiotics10111340