
An Integrated Approach of Video Game Therapy®: A Case Study



Abstract

1. Introduction
1.1. Video Game Therapy®
1.2. Video Game Therapy® and Social Isolation (Not in Education, Employment, or Training “NEET”)
1.3. Aims
2. Material and Method
2.1. Participants
2.2. Assessment Instruments
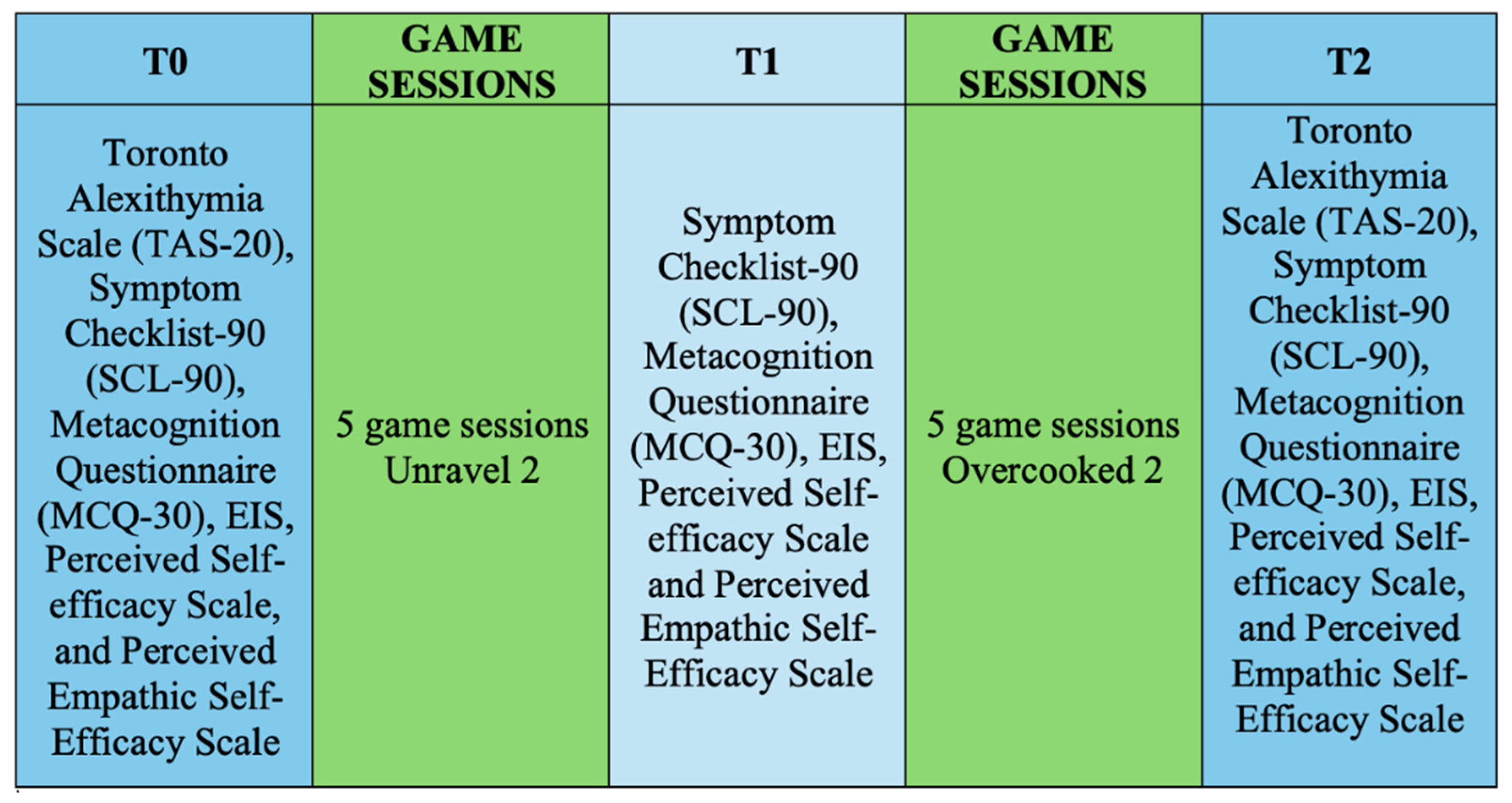
2.3. Procedure
3. Statistical Methods and Results
3.1. Alexithymia
3.2. Metacognition
3.3. Investigation of Psychological and Psychopathological States
3.4. Self-Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GomezRomero-Borquez, J.; Del-Valle-Soto, C.; Del-Puerto-Flores, J.A.; Briseño, R.A.; Varela-Aldás, J. Neurogaming in Virtual Reality: A Review of Video Game Genres and Cognitive Impact. Electronics 2024, 13, 1683. [Google Scholar] [CrossRef]
- de la Fuente Prieto, J.; Lacasa, P.; Martínez-Borda, R. Approaching metaverses: Mixed reality interfaces in youth media platforms. New Techno Humanit. 2022, 2, 136–145. [Google Scholar] [CrossRef]
- Bocci, F.; Sala, E. Il videogioco come strumento creativo e terapeutico in Psicologia Individuale; l’approccio della Video Game Therapy. Riv. Di Psicol. Individ. 2019, 86, 53–65. [Google Scholar]
- Bean, A.M. Working with Video Gamers and Games in Therapy: A Clinician’s Guide; Routledge: London, UK, 2018. [Google Scholar]
- Moreno, J.L. The Essential Moreno: Writings on Psychodrama, Group Method, and Spontaneity; Springer Publishing Company: Berlin/Heidelberg, Germany, 1987. [Google Scholar]
- Bocci, F.; Ferrari, A.; Sarini, M. Putting the gaming experience at the center of the therapy—The Video Game Therapy® approach. Healthcare 2023, 11, 1767. [Google Scholar] [CrossRef] [PubMed]
- Auxier, R. The coming revolution in (higher) education: Process, time, and singularity. In Contemporary Philosophical Proposals for the University: Toward a Philosophy of Higher Education; Palgrave Macmillan: Cham, Switzerland, 2018; pp. 217–260. [Google Scholar]
- Danilina, O.S. To Determine the Feasibility of Serious Videogames for Enhancing Self-Efficacy in Self-Management in People with Psychosis. Ph.D. Thesis, UCL (University College London), London, UK, 2019. [Google Scholar]
- David, O.A.; Predatu, R.; Cardoș, R.A. Effectiveness of the REThink therapeutic online video game in promoting mental health in children and adolescents. Internet Interv. 2021, 25, 100391. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Abbasi, A.Z.; Kazmi, S.F.; Hooi, T.D.; Rehman, U.; Hlavacs, H.; Arslan, F.S. Serious video games and psychological support: A depression intervention among young cancer patients. Entertain. Comput. 2022, 41, 100479. [Google Scholar] [CrossRef]
- Moraes, T.M.; Zaninotto, A.L.; Neville, I.S.; Hayashi, C.Y.; Paiva, W.S. Immersive virtual reality in patients with moderate and severe traumatic brain injury: A feasibility study. Health Technol. 2021, 11, 1035–1044. [Google Scholar] [CrossRef]
- Yuan, R.Y.; Chen, S.C.; Peng, C.W.; Lin, Y.N.; Chang, Y.T.; Lai, C.H. Effects of interactive video-game–based exercise on balance in older adults with mild-to-moderate Parkinson’s disease. J. Neuroeng. Rehabil. 2020, 17, 91. [Google Scholar] [CrossRef] [PubMed]
- Di Tore, S.; Fulgione, M.; Sibilio, M. Dislessia e videogames: Il potenziale didattico dei videogiochi. Mediterr. J. Soc. Sci. 2014, 5, 1165–1171. [Google Scholar] [CrossRef]
- Crepaldi, M.; Colombo, V.; Baldassini, D.; Mottura, S.; Antonietti, A. Supporting rehabilitation of ADHD children with serious games and enhancement of inhibition mechanisms. In Proceedings of the Virtual Reality and Augmented Reality: 14th EuroVR International Conference, EuroVR 2017, Laval, France, 12–14 December 2017; Proceedings 14. Springer International Publishing: Berlin/Heidelberg, Germany, 2017; pp. 167–181. [Google Scholar]
- Crepaldi, M.; Colombo, V.; Mottura, S.; Baldassini, D.; Sacco, M.; Cancer, A.; Antonietti, A. Antonyms: A computer game to improve inhibitory control of impulsivity in children with attention deficit/hyperactivity disorder (ADHD). Information 2020, 11, 230. [Google Scholar] [CrossRef]
- Evans, S.W.; Beauchaine, T.P.; Chronis-Tuscano, A.; Becker, S.P.; Chacko, A.; Gallagher, R.; Hartung, C.M.; Kofler, M.J.; Schultz, B.K.; Tamm, L.; et al. The efficacy of cognitive videogame training for ADHD and what FDA clearance means for clinicians. Evid. -Based Pract. Child Adolesc. Ment. Health 2021, 6, 116–130. [Google Scholar] [CrossRef]
- Sokolov, A.A.; Collignon, A.; Bieler-Aeschlimann, M. Serious video games and virtual reality for prevention and neurorehabilitation of cognitive decline because of aging and neurodegeneration. Curr. Opin. Neurol. 2020, 33, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Csikszentmihalyi, M. Flow: The Psychology of Optimal Experience; HarperCollins: New York, NY, USA, 1990. [Google Scholar]
- Zavaleta, D.; Samuel, K. Social Isolation: A Conceptual and Measurement Proposal; OPHI: Oxford, UK, 2014. [Google Scholar]
- Perissinotto, C.M.; Cenzer, I.S.; Covinsky, K.E. Loneliness in older persons: A predictor of functional decline and death. Arch. Intern. Med. 2012, 172, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- House, J.S.; Landis, K.R.; Umberson, D. Social relationships and health. Science 1988, 241, 540–545. [Google Scholar] [CrossRef]
- Courtin, E.; Knapp, M. Social isolation, loneliness and health in old age: A scoping review. Health Soc. Care Community 2017, 25, 799–812. [Google Scholar] [CrossRef]
- Martin, G.N.; Carlson, N.R.; Buskist, W. Psychology; Pearson Education: London, UK, 2010. [Google Scholar]
- Ripamonti, E. School-to-work transition: Putting non-cognitive skills in context. The case of NEET and suggestions for policy. Int. J. Educ. Vocat. Guid. 2023, 1–22. [Google Scholar] [CrossRef]
- Goldman-Mellor, S.; Caspi, A.; Arseneault, L.; Ajala, N.; Ambler, A.; Danese, A.; Moffitt, T.E. Committed to work but vulnerable: Self-perceptions and mental health in NEET 18-year olds from a contemporary British cohort. J. Child Psychol. Psychiatry 2016, 57, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Ellena, A.M.; Marta, E.; Simões, F.; Fernandes-Jesus, M.; Petrescu, C. Soft skills and psychological well-being: A study on Italian rural and urban NEETs. Calitatea Vieții 2021, 32, 352–370. [Google Scholar] [CrossRef]
- Straand, I.J.; Følstad, A.; Bjørnestad, J.R. Exploring a gaming-based intervention for unemployed young adults: Thematic analysis. JMIR Hum. Factors 2024, 11, e44423. [Google Scholar] [CrossRef] [PubMed]
- Capogna, S. Empowerment Organizzativo e Competenze Trasversali tra Retorica e Virtù; Sviluppo & Organizzazione: Milan, Italy, 2019. [Google Scholar]
- Čekrlija, Đ.; Dijana, Đ.; Biljana, M. Validation of Adlerian inferiority (COMPIN) and superiority (SUCOMP) complex shortened scales. Civitas 2017, 7, 13–35. [Google Scholar] [CrossRef]
- Derogatis, L.R. SCL-90-R: Administration, scoring and procedures manual-II for the (revised) version and other instruments of the psychopathology rating scale series. Clin. Psychom. Res. 1992, 1–16. [Google Scholar]
- Taylor, G.J.; Bagby, M.; Parker, J.D. The Revised Toronto Alexithymia Scale: Some reliability, validity, and normative data. Psychother. Psychosom. 1992, 57, 34–41. [Google Scholar] [CrossRef]
- Quattropani, M.C.; Lenzo, V.; Mucciardi, M.; Toffle, M.E. Psychometric properties of the Italian version of the Short Form of the Metacognitions Questionnaire (MCQ-30). BPA-Appl. Psychol. Bull. (Boll. Di Psicol. Appl.) 2014, 62, 29–41. [Google Scholar]
- Cartwright-Hatton, S.; Wells, A. Beliefs about worry and intrusions: The Meta-Cognitions Questionnaire and its correlates. J. Anxiety Disord. 1997, 11, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.A.; Marsh, H.W. Development and validation of a scale to measure optimal experience: The Flow State Scale. J. Sport Exerc. Psychol. 1996, 11, 17–35. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M.; Hall, L.E.; Haggerty, D.J.; Cooper, J.T.; Golden, C.J.; Dornheim, L. Development and validation of a measure of emotional intelligence. Personal. Individ. Differ. 1998, 25, 167–177. [Google Scholar] [CrossRef]
- Caprara, G.V. La Valutazione Dell’autoefficacia. Costrutti e Strumenti; Edizioni Erickson: Trento, Italy, 2001. [Google Scholar]
- La Ferlita, V.; Bonadies, M.; Solano, L.; De Gennaro, L.; Gonini, P. Alessitimia e adolescenza: Studio preliminare di validazione della TAS-20 su un campione di 360 adolescenti italiani. Infanz. E Adolesc. 2007, 6, 131–144. [Google Scholar]
- Sarno, I.; Preti, E.; Prunas, A.; Madeddu, F. SCL-90-R Symptom Checklist-90-R Adattamento Italiano; Giunti, Organizzazioni Speciali: Firenze, Italy, 2011. [Google Scholar]
- Bandura, A. Social cognitive theory: An agentic perspective. Asian J. Soc. Psychol. 1999, 2, 21–41. [Google Scholar] [CrossRef]
- King, G.; Keohane, R.O.; Verba, S. Designing Social Inquiry: Scientific Inference in Qualitative Research; Princeton University Press: Princeton, NJ, USA, 2021. [Google Scholar]
- Verschuren, P. Case study as a research strategy: Some ambiguities and opportunities. Int. J. Soc. Res. Methodol. 2003, 6, 121–139. [Google Scholar] [CrossRef]
- Yin, R.K. Case Study Research: Design and Methods; Sage: Newcastle upon Tyne, UK, 2009. [Google Scholar]

{kind=link}
{kind=link}
| Participant | Normative | ||
|---|---|---|---|
| Mean | Mean | SD | |
| TAS_0 | 52.00 | 52.36 | 11.37 |
| TAS_T2 | 46.00 | ||
| MCQ_Total T0 | 80.00 | 60.34 | 12.37 |
| MCQ_Total T1 | 71.00 | ||
| MCQ_Total T2 | 74.00 | ||
| MCQ_CC T0 | 22.00 | 9.55 | 4.11 |
| MCQ_CC T1 | 20.00 | ||
| MCQ_CC T2 | 19.00 | ||
| MCQ_CS T0 | 17.00 | 16.79 | 3.42 |
| MCQ_CS T1 | 13.00 | ||
| MCQ_CS T2 | 14.00 | ||
| MCQ_NB T0 | 15.00 | 11.04 | 3.65 |
| MCQ_NB T1 | 12.00 | ||
| MCQ_NB T2 | 11.00 | ||
| Self-efficacy emotion_T0 | 20.00 | 29.12 | 4.16 |
| Self-efficacy emotion_T1 | 21.00 | ||
| Self-efficacy emotion_T2 | 21.00 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crepaldi, M.; Bocci, F.; Sarini, M.; Greco, A. An Integrated Approach of Video Game Therapy®: A Case Study. Information 2025, 16, 68. https://doi.org/10.3390/info16010068
Crepaldi M, Bocci F, Sarini M, Greco A. An Integrated Approach of Video Game Therapy®: A Case Study. Information. 2025; 16(1):68. https://doi.org/10.3390/info16010068
Chicago/Turabian StyleCrepaldi, Maura, Francesco Bocci, Marcello Sarini, and Andrea Greco. 2025. "An Integrated Approach of Video Game Therapy®: A Case Study" Information 16, no. 1: 68. https://doi.org/10.3390/info16010068
APA StyleCrepaldi, M., Bocci, F., Sarini, M., & Greco, A. (2025). An Integrated Approach of Video Game Therapy®: A Case Study. Information, 16(1), 68. https://doi.org/10.3390/info16010068