
Measuring Discrimination against Older People Applying the Fraboni Scale of Ageism


Abstract
:1. Introduction
2. Theoretical Background
2.1. The Concept of Ageism
2.2. Measurement of Ageism
2.3. The Fraboni Scale of Ageism
3. Methodology
Data Collection and Sample
4. Results
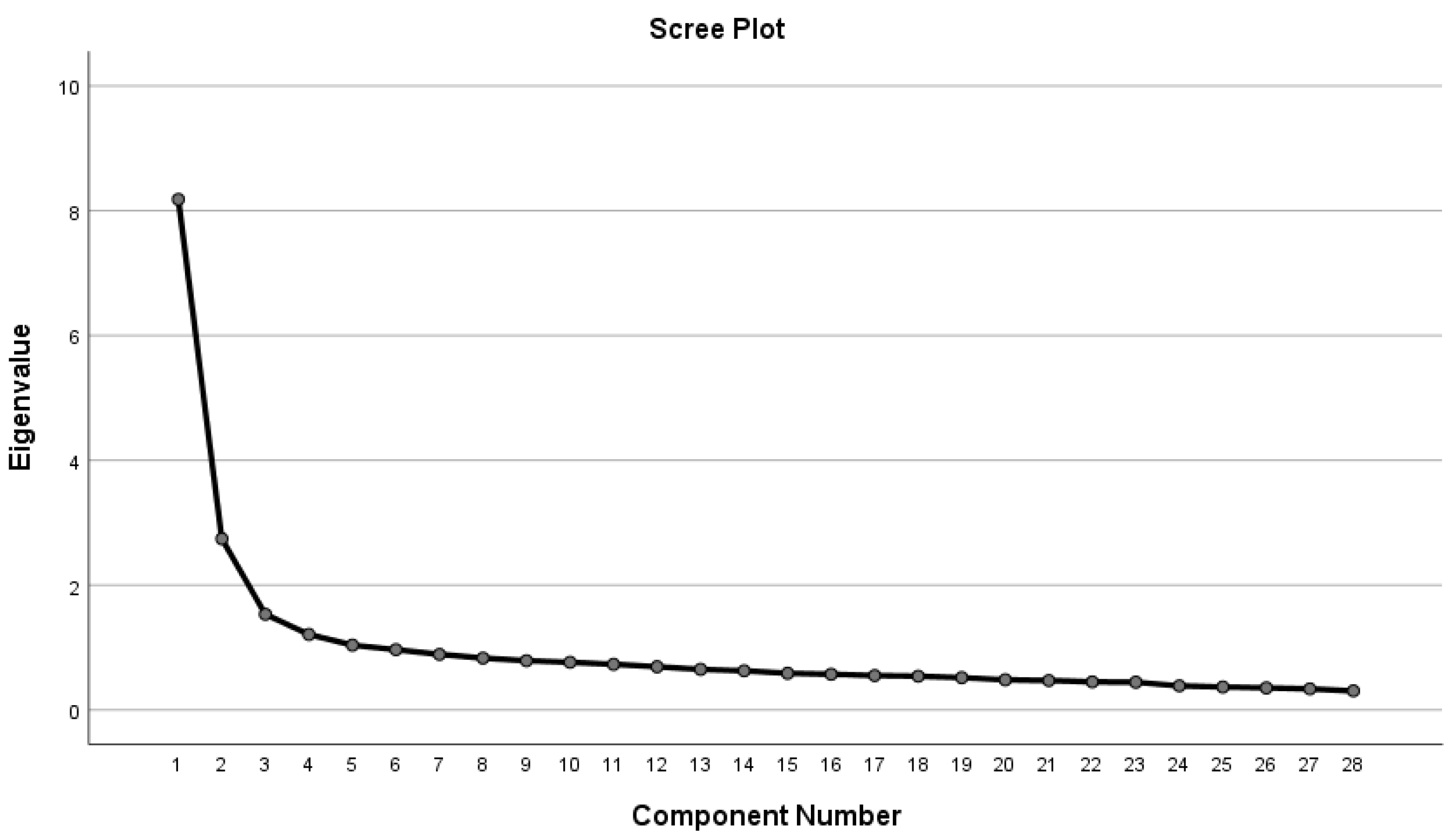
4.1. FSA Factor Structure and Construct Validity
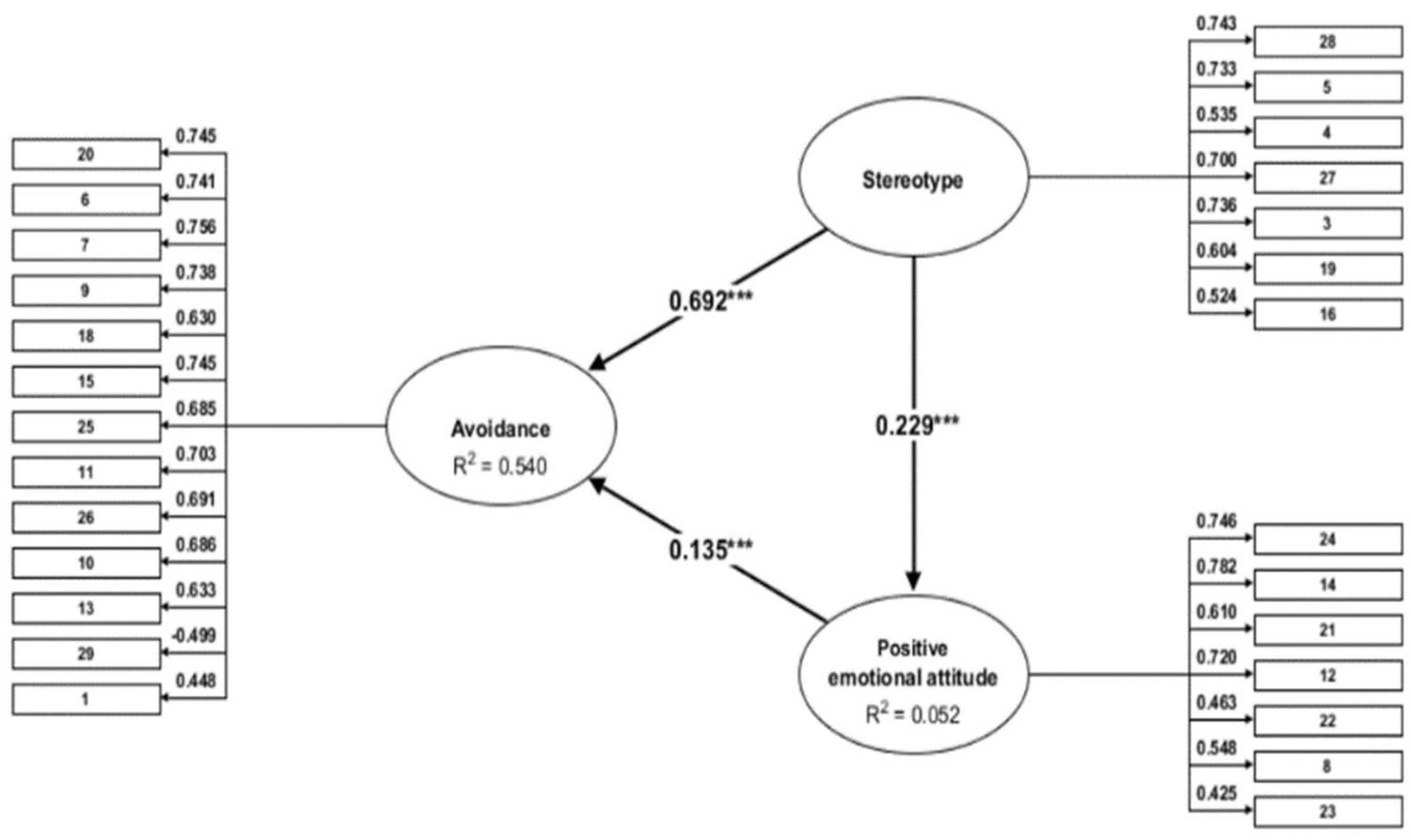
4.2. Construct Validity
5. Discussion and Conclusions
6. Limitation and Implication for Further Studies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Central Statistical Office. A Népesség a Születéskori Lakóhely, a Tényleges Lakóhely Településtípusa és Korcsoport Szerint. 2020. Available online: http://www.ksh.hu/nepszamlalas/tablak_demografia (accessed on 10 September 2021).
- Van Den Heuwe, W.J.; Van Santvoort, M.M. Experienced discrimination amongst European old citizens. Eur. J. Ageing 2011, 8, 291–299. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3225618/ (accessed on 1 August 2021). [CrossRef] [Green Version]
- Eurobarometer 437 2015, Discrimination in the EU in 2015. Available online: https://data.europa.eu/euodp/hu/data/dataset/S2077_83_4_437_ENG (accessed on 15 July 2021).
- Jászberényi, J. Az Aktív Időskor Lehetőségei Magyarországon (Bevezetés a Geronto-Andragógiába); Jaffa: Budapest, Hungary, 2009. [Google Scholar]
- Csizmadia, S.; Szabó, R.; Kovács, N. Az idős fogyasztók és a tv reklámok Magyaroszágon. Mark. Menedzsment 2015, 49, 50–67. [Google Scholar]
- Wilson, D.M.; Errasti-Ibarrondo, B.; Low, G. Where are we now in relation to determining the prevalence of ageism in this era of escalating population ageing? Ageing Res. Rev. 2019, 51, 78–84. [Google Scholar] [CrossRef]
- Kotter-Grühn, D. Changing Negative Views of Aging: Implications for Intervention and Translational Research. Annu. Rev. Gerontol. Geriatr. 2015, 35, 167–186. [Google Scholar] [CrossRef]
- Butler, R.N. Age-Ism: Another form of bigotry. Gerontologist 1969, 9, 243–246. [Google Scholar] [CrossRef]
- Palmore, E.B. Ageism: Negative and Positive, 2nd ed.; Springer Publishing Company: New York, NY, USA, 1999; pp. 3–18. [Google Scholar]
- Levy, B.R.; Banaji, M.R. Implicit ageism. In Ageism: Stereotyping and Prejudice against Older Persons; Nelson, T.D., Ed.; MIT Press: Cambridge, MA, USA, 2002; pp. 49–75. [Google Scholar]
- Iversen, T.N.; Larsen, L.; Solem, P.E. A conceptual analysis of Ageism. Nord. Psychol. 2009, 61, 4–22. [Google Scholar] [CrossRef]
- Donizzetti, A.R. Ageism in an Aging Society: The Role of Knowledge, Anxiety about Aging, and Stereotypes in Young People and Adults. Int. J. Environ. Res. Public Health 2019, 16, 1329. [Google Scholar] [CrossRef] [Green Version]
- Ayalon, L.; Tesch-Römer, C. (Eds.) Introduction to the section: Ageism-concept and origins. In Contemporary Perspectives on Ageism; International Perspectives on Aging, Springer Open: New York, NY, USA, 2018; Volume 19, ISBN 978-3-319-73819-2. [Google Scholar]
- Levy, B.R. Stereotype embodiment: A psychosocial approach to aging. Curr. Dir. Psychol. Sci. 2009, 18, 332–336. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2927354/pdf/nihms155298.pdf (accessed on 1 August 2021).
- Wurm, S.; Diehl, M.; Kornadt, A.; Westerhof, G.J.; Wahl, H.-W. How do views on aging affect health outcomes in adulthood and late life? Explanations for an established connection. Dev. Rev. 2017, 46, 27–43. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.R.; Slade, M.D.; Chang, E.-S.; Kannoth, S. Ageism amplifies cost and prevalence of health conditions. Gerontologist 2020, 60, 174–181. [Google Scholar] [CrossRef] [Green Version]
- Wurm, S.; Benyamini, Y. Optimism buffers the detrimental effect of negative self-perceptions of ageing on physical and mental health. Psychol. Health 2014, 29, 832–848. [Google Scholar] [CrossRef]
- Allen, M.J.O. Ageism as a risk factor for chronic disease. Gerontologist 2016, 56, 610–614. [Google Scholar] [CrossRef] [Green Version]
- Vitman, A.; Iecovich, E.; Alfasi, N. Ageism and social integration of older adults in their neighborhoods in Israel. Gerontologist 2014, 54, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Lamont, R.A.; Swift, H.J.; Abrams, D. A review and meta-analysis of age-based stereotype threat: Negative stereotypes, not facts, do the damage. Psychol. Aging 2015, 3, 180–193. [Google Scholar] [CrossRef]
- Tuckman, J.; Lorge, I. Attitudes toward old people. J. Soc. Psychol. 1953, 37, 249–260. [Google Scholar]
- Golde, A.P.; Kogan, P.N. A sentence completion procedure for assessing attitudes toward old people. J. Gerontol. 1959, 14, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Kogan, N. Attitudes toward old people: The development of a scale and an examination of correlates. J. Abnorm. Soc. Psychol. 1961, 62, 44–54. [Google Scholar] [CrossRef]
- Rosencranz, P.H.A.; McNevin, M.T.E. A factor analysis of attitudes toward the aged. Gerontologist 1969, 9, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Ayalon, L.; Dolberg, P.; Mikulionienė, S.; Perek-Białas, J.; Rapolienė, G.; Stypinska, J.; Willińska, M.; de la Fuente-Núñez, V. A systematic review of existing ageism scales. Ageing Res. Rev. 2019, 54, 100919. [Google Scholar] [CrossRef]
- Palmore, E. The ageism survey: First findings. Gerontologist 2001, 41, 572–575. [Google Scholar] [CrossRef] [Green Version]
- Cherry, K.E.; Allen, P.D.; Denver, J.Y.; Holland, K.R. Contributions of social desirability to self-reported ageism. J. Appl. Gerontol. 2015, 34, 712–733. [Google Scholar] [CrossRef]
- Greenwald, A.G.; McGhee, D.E.; Schwartz, J.L.K. Measuring individual differences in implicit cognition: The implicit association test. J. Pers. Soc. Psychol. 1998, 74, 1464–1480. [Google Scholar] [CrossRef]
- Sarkisian, C.A.; Hays, R.D.; Berry, S.H.; Mangione, C.M. Expectations regarding aging among older adults and physicians who care for older adults. Med. Care 2001, 39, 1025–1036. [Google Scholar] [CrossRef]
- Klusmann, V.; Notthoff, N.; Beyer, A.-K.; Blawert, A.; Gabrian, M. The assessment of views on ageing: A review of self-report measures and innovative extensions. Eur. J. Ageing 2020, 17, 403–433. [Google Scholar] [CrossRef] [Green Version]
- Löckenhoff, C.E.; De Fruyt, F.; Terracciano, A.; McCrae, R.R.; De Bolle, M.; Costa, P.T.; Aguilar-Vafaie, M.E.; Ahn, C.-K.; Ahn, H.-N.; Alcalay, L.; et al. Perceptions of aging across 26 cultures and their culture-level associates. Psychol. Aging 2009, 24, 941–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voss, P.; Kornadt, A.E.; Hess, T.M.; Fung, H.H.-L.; Rothermund, K. A world of difference? Domain-specific views on aging in China, the US, and Germany. Psychol. Aging 2018, 33, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Fraboni, M.; Saltstone, R.; Hughes, S. The fraboni scale of ageism (FSA): An attempt at a more precise measure of ageism. Can. J. Aging La Rev. Can. Vieil. 1990, 9, 56–66. [Google Scholar] [CrossRef]
- Rupp, D.E.; Vodanovich, S.J.; Crede, M. The multidimensional nature of ageism: Construct validity and group differences. J. Soc. Psychol. 2005, 145, 335–362. [Google Scholar] [CrossRef]
- Bodner, E.; Lazar, A. Ageism among Israeli students: Structure and demographic influences. Int. Psychogeriatr. 2008, 20, 1046–1058. [Google Scholar] [CrossRef]
- Boudjemad, V.; Gana, K. L’âgisme: Adaptation française d’une mesure et test d’un modèle structural des effets de l’empathie, l’orientation à la dominance sociale et le dogmatisme sur l’âgisme. Can. J. Aging La Rev. Can. Vieil. 2009, 28, 371–389. [Google Scholar] [CrossRef]
- Donizetti, A.R. Misurare il pregiudizio verso gli anziani: Validazione italiana della fraboni scale of ageism e analisi delle differenze pergenere ed età. G. Psicol. 2010, 4, 262–274. [Google Scholar]
- Sum, S.; Emamian, S.; Sefidchian, A. Aging educational program to reduce ageism: Intergenerational approach. Elderly Health J. 2016, 2, 33–38. [Google Scholar]
- Fan, J.-Y.; Zhao, H.-M.; Liu, Y.-T.; Kong, L.-L.; Mao, J.; Li, J. Psychometric properties of a Chinese version of the Fraboni scale of ageism: Evidence from medical students sample. BMC Med. Educ. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Kutlu, Y.; Küçük, L.; Findik, U.Y. Psychometric properties of the Turkish version of the fraboni scale of ageism. Nurs. Health Sci. 2012, 14, 464–471. [Google Scholar] [CrossRef]
- Kolos, K.; Kenesei, Z.; Kiss, K.; Kovács, E.; Michalkó, G.; Pinke-Sziva, I. Az ageizmus kialakulására ható tényezők a magyar fiatalok és idősek körében. Demográfia 2020, 63, 5–34. [Google Scholar] [CrossRef]
- Allan, L.J.; Johnson, J.A. Undergraduate attitudes toward the elderly: The role of knowledge, contact and aging anxiety. Educ. Gerontol. 2008, 35, 1–14. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hofstede, G. Culture’s Consequences: Comparing Values, Behaviors, Institutions, and Organizations Across Nations, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Rueckert, L.; Naybar, N. Gender differences in empathy: The role of the right hemisphere. Brain Cogn. 2008, 67, 162–167. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Men | 379 | 48.8 |
| Women | 397 | 51.2 |
| 18–29 years | 173 | 22.3 |
| 30–39 years | 187 | 24.1 |
| 40–49 years | 157 | 20.2 |
| 50–65 years | 259 | 33.3 |
| Primary education | 362 | 46.6 |
| Secondary education | 266 | 34.3 |
| Higher education | 148 | 19.1 |
| Budapest | 139 | 17.9 |
| Town | 403 | 51.9 |
| Village | 234 | 30.2 |
| Middle-Hungarian Region | 235 | 30.3 |
| West-Hungarian Region | 238 | 30.6 |
| East-Hungarian Region | 303 | 39.1 |
| Item | Table 1 Item Loading for Principal Component Analysis and Factor Structure | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|---|
| 20 | It is best that elderly people live where they won’t bother anyone | 0.762 | 0.107 | 0.119 | 1.68 | 1.104 | 1.218 | 0.840 |
| 6 | I sometimes avoid eye contact with elderly people when I see them | 0.736 | 0.189 | 0.010 | 1.74 | 1.136 | 1.290 | |
| 7 | I don’t like it when elderly people try to make conversation with me | 0.669 | 0.242 | 0.117 | 1.93 | 1.187 | 1.409 | |
| 9 | Complex and interesting conversation cannot be expected from most elderly people | 0.605 | 0.324 | 0.220 | 2.04 | 1.217 | 1.481 | |
| 18 | Most elderly people should not be trusted to take care of infants | 0.603 | 0.173 | 0.025 | 2.14 | 1.231 | 1.515 | |
| 15 | I personally would not want to spend much time with an elderly person | 0.602 | 0.326 | 0.182 | 2.23 | 1.244 | 1.548 | |
| 25 | Most elderly people would be considered to have poor personal hygiene | 0.598 | 0.291 | 0.020 | 2.00 | 1.177 | 1.386 | |
| 11 | Elderly people should find friends their own age | 0.591 | 0.336 | 0.056 | 2.16 | 1.238 | 1.534 | |
| 26 | I would prefer not to live with an elderly person | 0.510 | 0.380 | 0.193 | 2.52 | 1.329 | 1.766 | |
| 10 | Feeling depressed when around elderly people is probably a common feeling | 0.474 | 0.460 | 0.061 | 2.46 | 1.295 | 1.677 | |
| 13 | I would prefer not to go to an open house at a senior’s club if invited | 0.442 | 0.357 | 0.135 | 2.75 | 1.416 | 2.005 | |
| 29 | Elderly people do not need much money to meet their needs | −0.440 | −0.225 | 0.077 | 3.63 | 1.312 | 1.721 | |
| 1 | Teenage suicide is more tragic than suicide among the elderly | 0.302 | 0.298 | 0.053 | 2.70 | 1.548 | 2.396 | |
| 28 | Elderly people complain more than other people | 0.329 | 0.575 | 0.099 | 3.11 | 1.286 | 1.654 | 0.770 |
| 5 | Many elderly people just live in the past | 0.343 | 0.550 | 0.130 | 3.02 | 1.224 | 1.497 | |
| 4 | Many elderly people are not interested in making new friends, preferring instead the circle of friends they have had for years | 0.112 | 0.525 | 0.028 | 3.33 | 1.197 | 1.433 | |
| 27 | Most elderly people can be irritating because they tell the same stories over and over again | 0.344 | 0.510 | 0.088 | 2.84 | 1.222 | 1.493 | |
| 3 | Many elderly people are stingy and hoard their money and possessions | 0.415 | 0.479 | 0.035 | 2.61 | 1.255 | 1.574 | |
| 19 | Many elderly people are happiest when they are with people their own age | 0.336 | 0.412 | −0.086 | 3.12 | 1.216 | 1.478 | |
| 16 | Most elderly people should not be allowed to renew their drivers’ licenses | 0.293 | 0.323 | −0.002 | 3.24 | 1.336 | 1.784 | |
| 24 | Most elderly people are interesting, individualistic people | 0.032 | 0.107 | 0.738 | 2.24 | 1.075 | 1.155 | 0.723 |
| 14 | Elderly people can be very creative | 0.029 | 0.188 | 0.710 | 2.37 | 1.115 | 1.243 | |
| 21 | The company of most elderly people is quite enjoyable | −0.054 | 0.151 | 0.605 | 2.51 | 1.075 | 1.156 | |
| 12 | Elderly people should feel welcome at social gatherings of young people | 0.175 | 0.059 | 0.542 | 2.17 | 1.103 | 1.216 | |
| 22 | It is sad to hear about the plight of the elderly in our society these days | 0.142 | −0.109 | 0.411 | 1.97 | 1.137 | 1.292 | |
| 8 | Elderly people deserve the same rights and freedoms as other members of our society | 0.349 | −0.188 | 0.386 | 1.41 | 0.869 | 0.756 | |
| 23 | Elderly people should be encouraged to speak out politically | 0.005 | 0.050 | 0.340 | 2.86 | 1.348 | 1.816 | |
| 2 | There should be special clubs set aside within sports facilities so that the elderly can compete at their own level | 0.041 | 0.214 | −0.264 | 3.42 | 1.305 | 1.706 | - |
| Original FSA Statement Number | Present Study Hungary | Fraboni et al. 1990 Canada | Rupp et al. 2005 USA | Bodner-Lazar 2008 Israel | Kutlu et al. 2012 Turkey | Fan et al. 2020 China |
|---|---|---|---|---|---|---|
| 7 | Avoidance | Avoidance | Separation | Stereotype | Discrimination | Avoidance |
| 6 | Avoidance | Avoidance | Separation | Omitted | Avoidance | Avoidance |
| 20 | Avoidance | Discrimination | Separation | Omitted | Dicrimination | Avoidance |
| 15 | Avoidance | Avoidance | Affective attitude | Avoidance | Avoidance | Excluded |
| 9 | Avoidance | Antilocution | Separation | Omitted | Discrimination | Excluded |
| 11 | Avoidance | Avoidance | Separation | Avoidance | Discrimination | Excluded |
| 10 | Avoidance | Avoidance | Separation | Avoidance | Discrimination | Excluded |
| 13 | Avoidance | Avoidance | Stereotypes | Contribution | Avoidance | Excluded |
| 26 | Avoidance | Avoidance | Omitted | Omitted | Avoidance | Avoidance |
| 18 | Avoidance | Discrimination | Stereotype | Avoidance | Stereotypes | Stereotype |
| 25 | Avoidance | Antilocution | Stereotype | Avoidance | Stereotype | Avoidance |
| 1 | Avoidance | Antilocution | Stereotype | Stereotype | Stereotype | Omitted |
| 29 | Avoidance | Antilocution | Omitted | Avoidance | Stereotype | Omitted |
| 27 | Stereotype | Antilocution | Stereotype | Contribution | Stereotype | Stereotypes |
| 4 | Stereotype | Antilocution | Stereotype | Contribution | Stereotype | Stereotype |
| 28 | Stereotype | Antilocution | Stereotype | Omitted | Stereotype | Stereotype |
| 5 | Stereotype | Antilocution | Stereotype | Stereotype | Stereotype | Stereotype |
| 19 | Stereotype | Avoidance | Stereotype | Contribution | Stereotype | Stereotypes |
| 3 | Stereotype | Antilocution | Stereotypes | Stereotype | Stereotype | Stereotype |
| 16 | Stereotype | Antilocution | Omitted | Omitted | Stereotype | Stereotype |
| * 21 | Positive emotional attitude | Discrimination | Affective attitude | Contribution | Avoidance | Excluded |
| * 24 | Positive emotional | Discrimination | Affective attitude | Omitted | Avoidance | Exluded |
| * 14 | Positive emotionattitude | Avoidance | Omitted | Avoidance | Avoidance | Avoidance |
| 12 | Positive emotional attitude | Avoidance | Separation | Contribution | Avoidance | Exluded |
| * 22 | Positive emotional attitude | Discrimination | Affective attitude | Omitted | Omitted | Omitted |
| * 8 | Positive emotional attitude | Discrimination | Omitted | Avoidance | Omitted | Omitted |
| 2 | Omitted | Antilocution | Omitted | Omitted | Omitted | Omitted |
| * 23 | Positive emotional attitude | Dicrimination | Affecrive attitude | Avoidance | Discrimination | Avoidance |
| 17 | Omitted | Discrimination | Omitted | Omitted | Omitted | Avoidance |
| FSA Dimensions | Mean | SD | Range | Average Sum of Scores | SD |
|---|---|---|---|---|---|
| Avoidance | 2.309 | 0.750 | 13–61 | 30.01 | 9.736 |
| Stereotype | 3.017 | 0.801 | 7–35 | 21.12 | 5.601 |
| Positive emotional attitude | 2.215 | 0.671 | 7–35 | 15.51 | 4.694 |
| FSA total | 2.502 | 0.578 | 32–128 | 70.06 | 16.195 |
| β | Indirect Effect | Total Effect | Cohen’s f2 | |
|---|---|---|---|---|
| Stereotype -> Avoidance | 0.6921 | 0.0308 | 0.7229 | 0.9863 |
| Stereotype -> Positive emotional attitude | 0.2285 | 0.2285 | 0.0551 | |
| Positive emotional attitude -> Avoidance | 0.1348 | 0.1348 | 0.0374 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofmeister-Tóth, Á.; Neulinger, Á.; Debreceni, J. Measuring Discrimination against Older People Applying the Fraboni Scale of Ageism. Information 2021, 12, 458. https://doi.org/10.3390/info12110458
Hofmeister-Tóth Á, Neulinger Á, Debreceni J. Measuring Discrimination against Older People Applying the Fraboni Scale of Ageism. Information. 2021; 12(11):458. https://doi.org/10.3390/info12110458
Chicago/Turabian StyleHofmeister-Tóth, Ágnes, Ágnes Neulinger, and János Debreceni. 2021. "Measuring Discrimination against Older People Applying the Fraboni Scale of Ageism" Information 12, no. 11: 458. https://doi.org/10.3390/info12110458
APA StyleHofmeister-Tóth, Á., Neulinger, Á., & Debreceni, J. (2021). Measuring Discrimination against Older People Applying the Fraboni Scale of Ageism. Information, 12(11), 458. https://doi.org/10.3390/info12110458