
Religious Coping as Moderator of Psychological Responses to Stressful Events: A Longitudinal Study

Abstract
:1. Introduction
2. Method
2.1. Design
2.2. Participants
2.3. Instruments
2.4. Procedure
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Annick Shaw, Stephen Joseph, and P. Alex Linley. “Religion, spirituality, and posttraumatic growth: A systematic review.” Mental Health, Religion & Culture 8 (2005): 1–11. [Google Scholar]
- Darío Páez, Nekane Basabe, Serena Bosco, Myriam Campos, and Silvia Ubillos. “Afrontamiento y violencia colectiva (Coping and collective violence).” In Superando la Violencia Colectiva y Construyendo Cultura de Paz (Overcoming Collective Violence and Building a Culture of Peace). Madrid: Fundamentos, 2011, pp. 279–309. [Google Scholar]
- Richard G. Tedeschi, and Lawrence G. Calhoun. “The Posttraumatic Growth Inventory: Measuring the positive legacy of trauma.” Journal of Traumatic Stress 9 (1996): 455–71. [Google Scholar] [CrossRef] [PubMed]
- Vicki S. Helgeson, Kerry A. Reynolds, and Patricia L. Tomich. “A meta-analytic review of benefit finding and growth.” Journal of Consulting and Clinical Psychology 74 (2006): 797–816. [Google Scholar] [CrossRef] [PubMed]
- Gabriele Prati, and Luca Pietrantoni. “Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: A meta-analysis.” Journal of Loss and Trauma 14 (2009): 364–88. [Google Scholar] [CrossRef]
- Kenya R. Urcuyo, Amy E. Boyers, Charles S. Carver, and Michael H. Antoni. “Finding benefit in breast cancer: Relations with personality, coping, and concurrent well-being.” Psychology & Health 20 (2005): 175–92. [Google Scholar]
- Julia Vigna Bosson, Mary Lou Kelley, and Glenn N. Jones. “Deliberate cognitive processing mediates the relation between positive religious coping and posttraumatic growth.” Journal of Loss and Trauma 17 (2012): 439–51. [Google Scholar] [CrossRef]
- Felipe E. García, Darío Páez-Rovira, Giordana Cartes Zurtia, Héctor Neira Martel, and Alejandro Reyes Reyes. “Religious coping, social support and subjective severity as predictors of posttraumatic growth in people affected by the earthquake in Chile on 27/2/2010.” Religions 5 (2014): 1132–45. [Google Scholar] [CrossRef]
- Anna Wlodarczyk, Nekane Basabe, Darío Páez, Alberto Amutio, Felipe E. García, Carlos Reyes, and Loreto Villagrán. “Positive effects of communal coping in the aftermath of a collective trauma: The case of the 2010 Chilean earthquake.” European Journal of Education and Psychology 9 (2016): 9–19. [Google Scholar] [CrossRef]
- Kenneth Pargament, Margaret Feuille, and Donna Burdzy. “The Brief RCOPE: Current psychometric status of a short measure of religious coping.” Religions 2 (2011): 51–76. [Google Scholar] [CrossRef]
- Kenneth I. Pargament, Bruce W. Smith, Harold G. Koenig, and Lisa Perez. “Patterns of positive and negative religious coping with major life stressors.” Journal for the Scientific Study of Religion, 1998, 710–24. [Google Scholar] [CrossRef]
- Harold G. Koenig, Kenneth I. Pargament, and Julie Nielsen. “Religious coping and health status in medically ill hospitalized older adults.” The Journal of Nervous and Mental Disease 186 (1998): 513–21. [Google Scholar] [CrossRef] [PubMed]
- George Fitchett, Bruce D. Rybarczyk, Gail A. DeMarco, and John J. Nicholas. “The role of religion in medical rehabilitation outcomes: A longitudinal study.” Rehabilitation Psychology 44 (1999): 333–53. [Google Scholar] [CrossRef]
- Kenneth I. Pargament, Harold G. Koenig, Nalini Tarakeshwar, and June Hahn. “Religious coping methods as predictors of psychological, physical and spiritual outcomes among medically ill elderly patients: A two-year longitudinal study.” Journal of Health Psychology 9 (2004): 713–30. [Google Scholar] [CrossRef] [PubMed]
- J. Irene Harris, Christopher R. Erbes, Brian E. Engdahl, Henry Ogden, Raymond H.A. Olson, Ann Marie M. Winskowski, Kelsey Campion, and Saari Mataas. “Religious distress and coping with stressful life events: A longitudinal study.” Journal of Clinical Psychology 68 (2012): 1276–86. [Google Scholar] [CrossRef] [PubMed]
- Monica M. Gerber, Adriel Boals, and Darnell Schuettler. “The unique contributions of positive and negative religious coping to posttraumatic growth and PTSD.” Psychology of Religion and Spirituality 3 (2011): 298. [Google Scholar] [CrossRef]
- Amber M. Henslee, Scott F. Coffey, Julie A. Schumacher, Melissa Tracy, Fran H. Norris, and Sandro Galea. “Religious coping and psychological and behavioral adjustment after Hurricane Katrina.” The Journal of Psychology 149 (2015): 630–42. [Google Scholar] [CrossRef] [PubMed]
- Samuel R. Weber, and Kenneth I. Pargament. “The role of religion and spirituality in mental health.” Current Opinion in Psychiatry 27 (2014): 358–63. [Google Scholar] [CrossRef] [PubMed]
- Charlotte vanOyen Witvliet, Karl A. Phipps, Michelle F. Dennis, and Jean C. Beckham. “Posttraumatic mental and physical health correlates of forgiveness and religious coping in military veterans.” Journal of Traumatic Stress 17 (2004): 269–73. [Google Scholar] [CrossRef] [PubMed]
- Avinash Thombre, Allen C. Sherman, and Stephanie Simonton. “Religious coping and posttraumatic growth among family caregivers of cancer patients in India.” Journal of Psychosocial Oncology 28 (2010): 173–88. [Google Scholar] [CrossRef] [PubMed]
- Amy L. Ai, Daniel Hall, Kenneth Pargament, and Terrence N. Tice. “Posttraumatic growth in patients who survived cardiac surgery: The predictive and mediating roles of faith-based factors.” Journal of Behavioral Medicine 36 (2013): 186–98. [Google Scholar] [CrossRef] [PubMed]
- Gregory D. Zimet, Nancy W. Dahlem, Sara G. Zimet, and Gordon K. Farley. “The multidimensional scale of perceived social support.” Journal of Personality Assessment 52 (1988): 30–41. [Google Scholar] [CrossRef]
- Michael J. Doane. “The association between religiosity and subjective well-being: The unique contribution of religious service attendance and the mediating role of perceived religious social support.” The Irish Journal of Psychology 34 (2013): 49–66. [Google Scholar] [CrossRef]
- Kelly M. McConnell, Kenneth I. Pargament, Christopher G. Ellison, and Kevin J. Flannelly. “Examining the links between spiritual struggles and symptoms of psychopathology in a national sample.” Journal of Clinical Psychology 62 (2006): 1469–84. [Google Scholar] [CrossRef] [PubMed]
- Paola Avilés Maldonado, Félix Cova Solar, Claudio Bustos, and Felipe E. García. “Afrontamiento y rumiación frente a eventos adversos y crecimiento postraumático en estudiantes universitarios (Coping and rumination against adverse events and posttraumatic growth in university students).” Liberabit 20 (2014): 281–92. [Google Scholar]
- Felipe E. García, Carolyn Jaramillo, Ana María Martínez, Ivonne Valenzuela, and Felix Cova Solar. “Respuestas psicológicas ante un desastre natural: Estrés y crecimiento postraumático (Psychological responses to a natural disaster: Stress and post-traumatic growth).” Liberabit 20 (2014): 121–30. [Google Scholar]
- Felipe E. García, Félix Cova, Paulina Rincón, and Carmelo Vázquez. “Trauma or growth after a natural disaster? The mediating role of rumination processes.” European Journal of Psychotraumatology 6 (2015): 1–10. [Google Scholar] [CrossRef] [PubMed]
- Felipe E. García, Félix Cova, Paulina Rincón, Carmelo Vázquez, and Darío Páez. “Coping, rumination and posttraumatic growth in people affected by an earthquake.” Psicothema 28 (2016): 59–65. [Google Scholar] [PubMed]
- Jane Shakespeare-Finch, and Janine Lurie-Beck. “A meta-analytic clarification of the relationship between posttraumatic growth and symptoms of posttraumatic distress disorder.” Journal of Anxiety Disorders 28 (2014): 223–29. [Google Scholar] [CrossRef] [PubMed]
- Gil Zukerman, and Liat Korn. “Post-Traumatic Stress and World Assumptions: The Effects of Religious Coping.” Journal of Religion and Health 53 (2014): 1676–90. [Google Scholar] [CrossRef] [PubMed]
- Rebekah Bradley, Ann C. Schwartz, and Nadine J. Kaslow. “Posttraumatic stress disorder symptoms among low-income, African American women with a history of intimate partner violence and suicidal behaviors: Self-esteem, social support, and religious coping.” Journal of Traumatic Stress 18 (2005): 685–96. [Google Scholar] [CrossRef] [PubMed]
- Elizabeth Thomas, and Sarah Savoy. “Relationships between traumatic events, religious coping style, and posttraumatic outcomes.” Traumatology: An International Journal 20 (2014): 84–90. [Google Scholar] [CrossRef]
- Joshua J. Ahles, Amy H. Mezulis, and Melissa R. Hudson. “Religious coping as a moderator of the relationship between stress and depressive symptoms.” Psychology of Religion and Spirituality 8 (2016): 228–34. [Google Scholar] [CrossRef]
- Fran H. Norris, Jessica L. Hamblen, Lisa M. Brown, and John A. Schinka. “Validation of the Short Posttraumatic Stress Disorder Rating Interview (expanded version, Sprint-E) as a measure of postdisaster distress and treatment need.” American Journal of Disaster Medicine 3 (2007): 201–12. [Google Scholar]
- Arnie Cann, Lawrence G. Calhoun, Richard G. Tedeschi, Kanako Taku, Tanya Vishnevsky, Kelli N. Triplett, and Suzanne C. Danhauer. “A short form of the Posttraumatic Growth Inventory.” Anxiety, Stress, & Coping 23 (2010): 127–37. [Google Scholar]
- Felipe E. García, and Anna Wlodarczyk. “Psychometric Properties of the Posttraumatic Growth Inventory–Short Form Among Chilean Adults.” Journal of Loss and Trauma 21 (2016): 303–14. [Google Scholar] [CrossRef]
- Marcelo Leiva-Bianchi, and Ismael Gallardo Cuadra. “Validation of the short posttraumatic stress disorder rating interview (SPRINT-E) in a sample of people affected by 27-F Chilean earthquake and tsunami.” Anales de Psicología (Annals of Psychology) 29 (2013): 328–34. [Google Scholar]
- Armando Rivera-Ledesma, and María Montero. “Espiritualidad y religiosidad en adultos mayores mexicanos (Spirituality and religiosity in Mexican elderly people).” Salud Mental 28 (2005): 51–58. [Google Scholar]
- Charles S. Carver. “You want to measure coping but your protocol’too long: Consider the brief cope.” International Journal of Behavioral Medicine 4 (1997): 92–100. [Google Scholar] [CrossRef] [PubMed]
- Consuelo Morán, René Landero, and Mónica Teresa González. “COPE-28: Un análisis psicométrico de la versión en español del Brief COPE (COPE-28: A psychometric analysis of the Spanish version of the Brief COPE).” Universitas Psychologica 9 (2010): 543–52. [Google Scholar]
- Carolina Alzugaray, Felipe E. García, Alejandro Reyes, and Rodolfo Alvarez. “Propiedades psicométricas de una versión breve de la Escala de Rumiación Relacionada a un Evento en población chilena afectada por eventos altamente estresantes (Psychometric properties of a short form of the Event Related Rumination Inventory in Chilean population affected by stressful events).” Ajayu 13 (2015): 183–98. [Google Scholar]
- César Pérez López, and César Pérez López. Técnicas de Muestreo Estadístico: Teoría, Práctica y Aplicaciones Informáticas (Statistical Sampling Techniques: Theory, Practice and Computer Applications). Madrid: Ra-Ma, 2000. [Google Scholar]
- John M. Gottman, and Lowell J. Krokoff. “Marital interaction and satisfaction: A longitudinal view.” Journal of Consulting and Clinical Psychology 57 (1989): 47–52. [Google Scholar] [CrossRef] [PubMed]
- Andrew F. Hayes. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New York: Guilford Press, 2013. [Google Scholar]
- Kenneth A. Bollen, and J. Scott Long. Testing Structural Equation Models. Newbury Park: Sage, 1993, vol. 154. [Google Scholar]
- Gene G. Ano, and Erin B. Vasconcelles. “Religious coping and psychological adjustment to stress: A meta-analysis.” Journal of Clinical Psychology 61 (2005): 461–80. [Google Scholar] [CrossRef] [PubMed]
- Kenneth I. Pargament. The Psychology of Religion and Coping: Theory, Research, Practice. New York: Guilford Press, 2001. [Google Scholar]

{kind=link}
{kind=link}
| Minimum | Maximum | Mean | SD | Skewness | Kurtosis | α | |
|---|---|---|---|---|---|---|---|
| Subjective severity T1 | 0 | 12 | 6.59 | 3.09 | −0.24 | −0.69 | 0.86 |
| Social support T1 | 0 | 12 | 5.58 | 3.33 | 0.14 | −0.85 | 0.82 |
| Positive RC T1 | 0 | 21 | 8.82 | 6.94 | 0.19 | −1.25 | 0.95 |
| Negative RC T1 | 0 | 15 | 2.69 | 3.61 | 1.46 | 1.58 | 0.83 |
| PTS T1 | 0 | 36 | 10.37 | 7.44 | 0.80 | 0.77 | 0.91 |
| PTG T1 | 0 | 50 | 26.57 | 12.77 | −0.43 | −0.62 | 0.92 |
| PTS T2 | 0 | 35 | 9.48 | 7.41 | 0.65 | 0.30 | 0.92 |
| PTG T2 | 0 | 50 | 25.15 | 12.17 | −0.05 | −0.55 | 0.94 |
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Subjective severity T1 | 0.16 * | 0.17 * | 0.24 *** | 0.13 | 0.07 | 0.07 | 0.44 *** | 0.26 *** | 0.18 ** |
| 2. Positive RC T1 | - | 0.09 | 0.27 *** | 0.49 *** | 0.30 *** | 0.22 *** | 0.10 | 0.07 | 0.04 |
| 3. Negative RC T1 | - | 0.11 | −0.03 | 0.08 | −0.11 | 0.40 *** | 0.31 *** | 0.09 | |
| 4. Social support T1 | - | 0.27 *** | 0.14* | 0.15 * | 0.27 *** | 0.13 | 0.15 * | ||
| 5. PTG T1 | - | 0.53 *** | 0.52 *** | 0.09 | 0.01 | 0.08 | |||
| 6. PTG T2 | - | −0.45 *** | 0.07 | 0.04 | 0.03 | ||||
| 7. Change in PTG | - | 0.02 | −0.02 | 0.05 | |||||
| 8. PTS T1 | - | 0.49 *** | 0.51 *** | ||||||
| 9. PTS T2 | - | −0.50 *** | |||||||
| 10. Change in PTS | - |
| Unstandardized Coefficients | Typified Coefficients | T | p | |||
|---|---|---|---|---|---|---|
| B | SE | Β | ||||
| Step 1 | R2 = 0.02. ΔR2 = 0.02, p = 0.034 | |||||
| (Constant) | −1.55 | 1.62 | −0.959 | 0.339 | ||
| Social support T1 | 0.53 | 0.25 | 0.15 | 2.140 | 0.034 | |
| Step 2 | R2 = 0.08. ΔR2 = 0.06, p = 0.003 | |||||
| (Constant) | −2.60 | 1.77 | −1.467 | 0.144 | ||
| Social support T1 | 0.39 | 0.25 | 0.11 | 1.530 | 0.127 | |
| Positive RC T1 | 0.35 | 0.12 | 0.20 | 2.890 | 0.004 | |
| Negative RC T1 | −0.46 | 0.23 | −0.14 | −2.047 | 0.042 | |
| Step 3 | R2 = 0.11. ΔR2 = 0.05, p = 0.005 | |||||
| (Constant) | −7.03 | 2.33 | −3.021 | 0.003 | ||
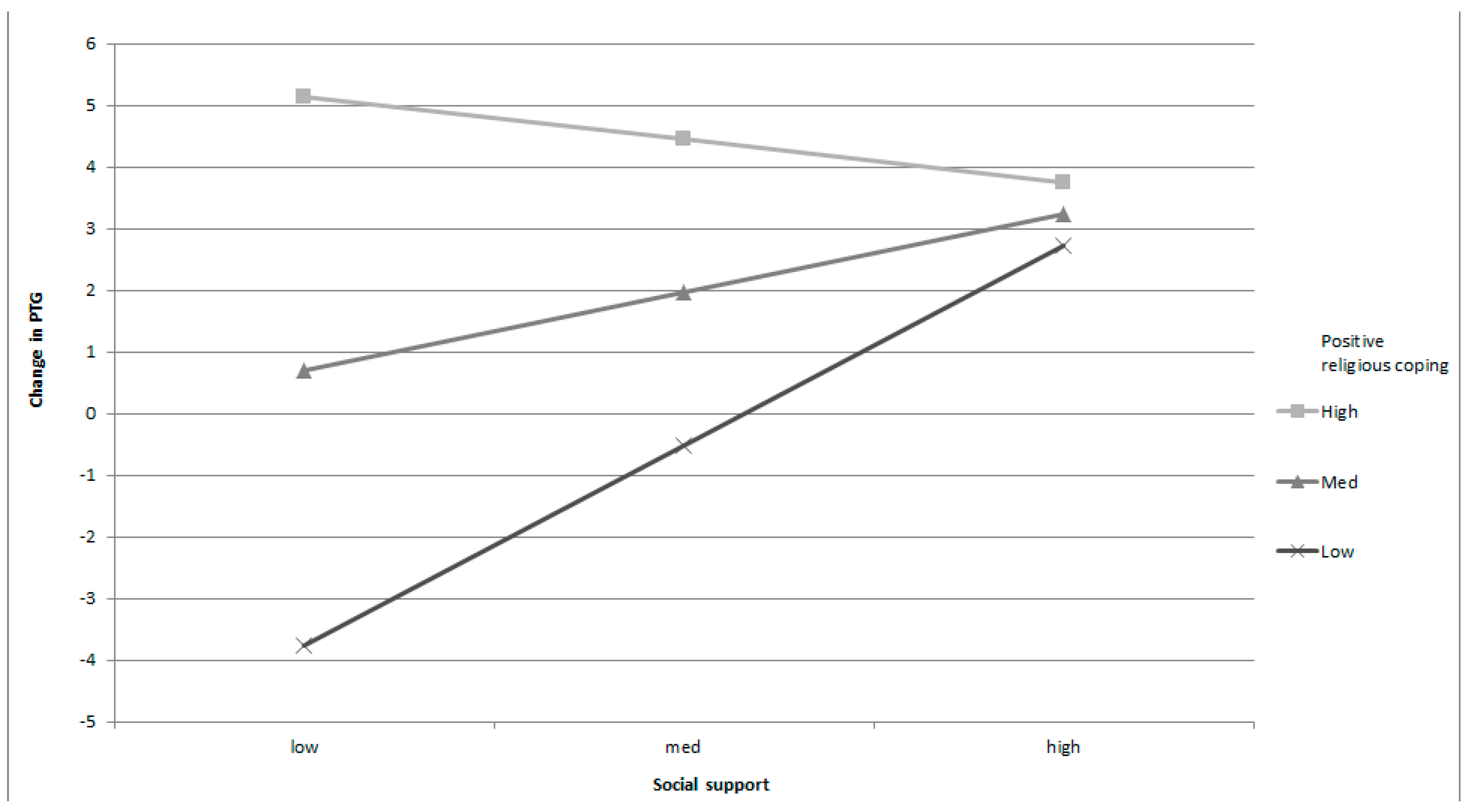
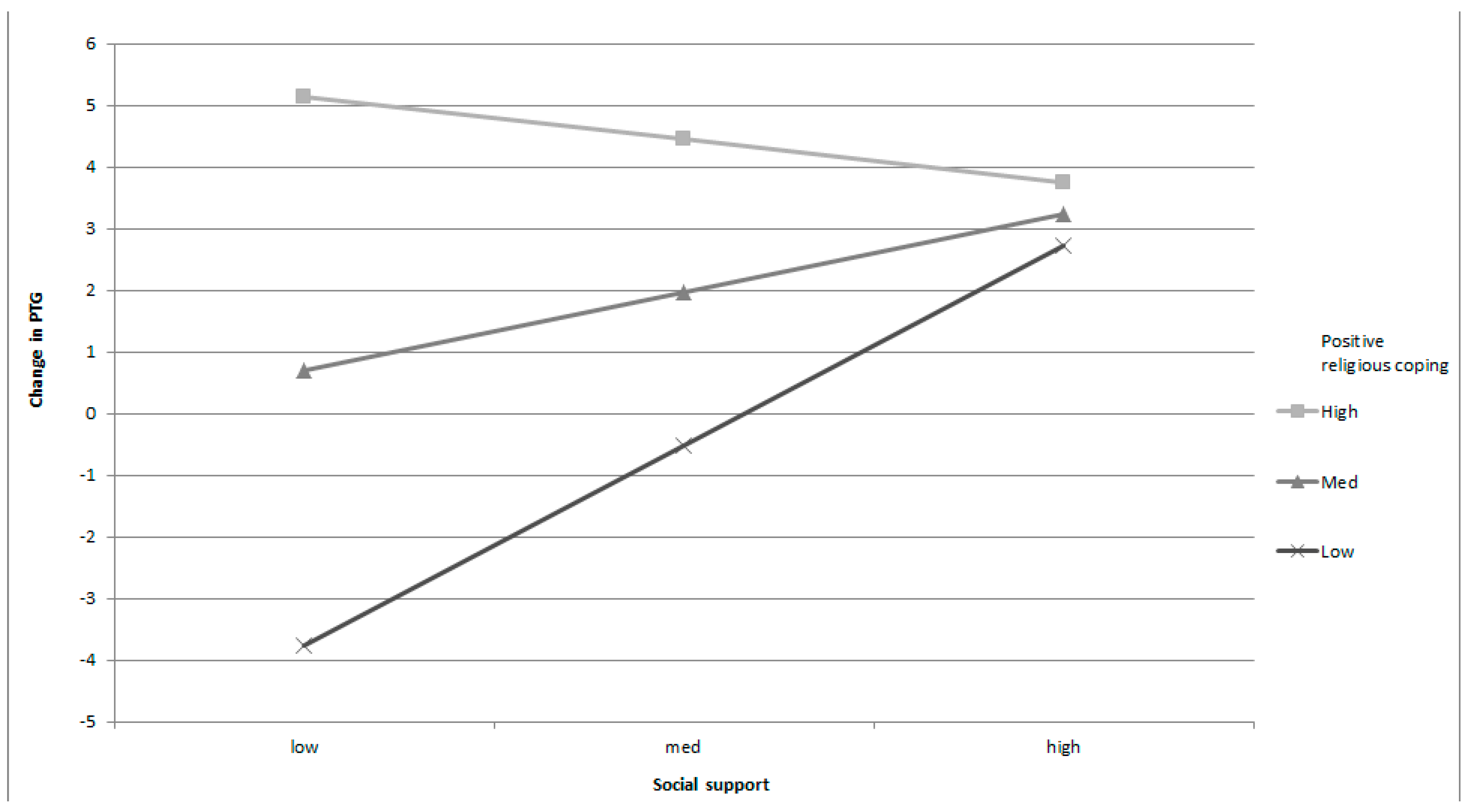
| Social support T1 | 1.29 | 0.40 | 0.35 | 3.216 | 0.002 | |
| Positive RC T1 | 0.91 | 0.23 | 0.52 | 3.982 | 0.000 | |
| Negative RC T1 | −0.55 | 0.22 | −0.16 | −2.437 | 0.016 | |
| Social support × Positive RC | −0.10 | 0.03 | −0.49 | −2.871 | 0.005 | |
| Positive Religious Coping | B | SE | T | p | 95% del IC | |
|---|---|---|---|---|---|---|
| LL CI | UL CI | |||||
| Low (1.89) | 0.97 | 0.35 | 2.755 | 0.006 | 0.277 | 1.671 |
| Moderate (8.82) | 0.38 | 0.25 | 1.523 | 0.132 | −0.116 | 0.878 |
| High (15.76) | −0.21 | 0.33 | −0.638 | 0.524 | −0.867 | −0.443 |
| Model | Unstandardized Coefficients | Typified Coefficients | T | p | ||
|---|---|---|---|---|---|---|
| B | SE. | Β | ||||
| Step 1 | R2 = 0.03. ΔR2 = 0.03. p = 0.01 | |||||
| (Constant) | −1.96 | 1.20 | −1.629 | 0.105 | ||
| Subjective severity T1 | 0.43 | 0.17 | 0.18 | 2.611 | 0.010 | |
| Step 2 | R2 = 0.04. ΔR2 = 0.003. p = 0.70 | |||||
| (Constant) | −2.18 | 1.31 | −1.660 | 0.098 | ||
| Subjective severity T1 | 0.41 | 0.17 | 0.17 | 2.381 | 0.018 | |
| Positive RC T1 | 0.01 | 0.08 | 0.01 | 0.097 | 0.923 | |
| Negative RC T1 | 0.12 | 0.14 | 0.06 | 0.841 | 0.401 | |
| Step 3 | R2 = 0.06. ΔR2 = 0.03. p = 0.02 | |||||
| (Constant) | −0.45 | 1.48 | −0.305 | 0.760 | ||
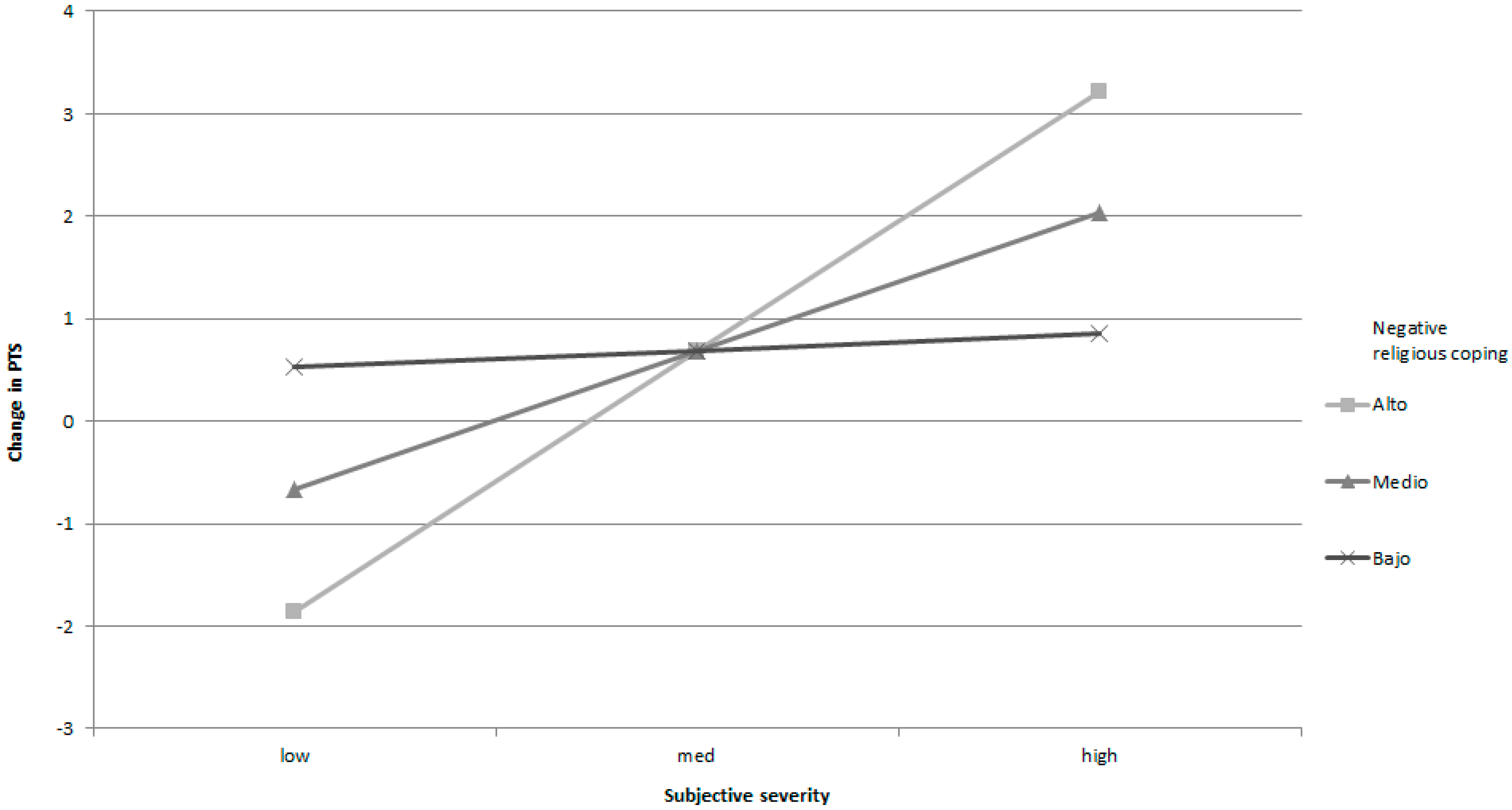
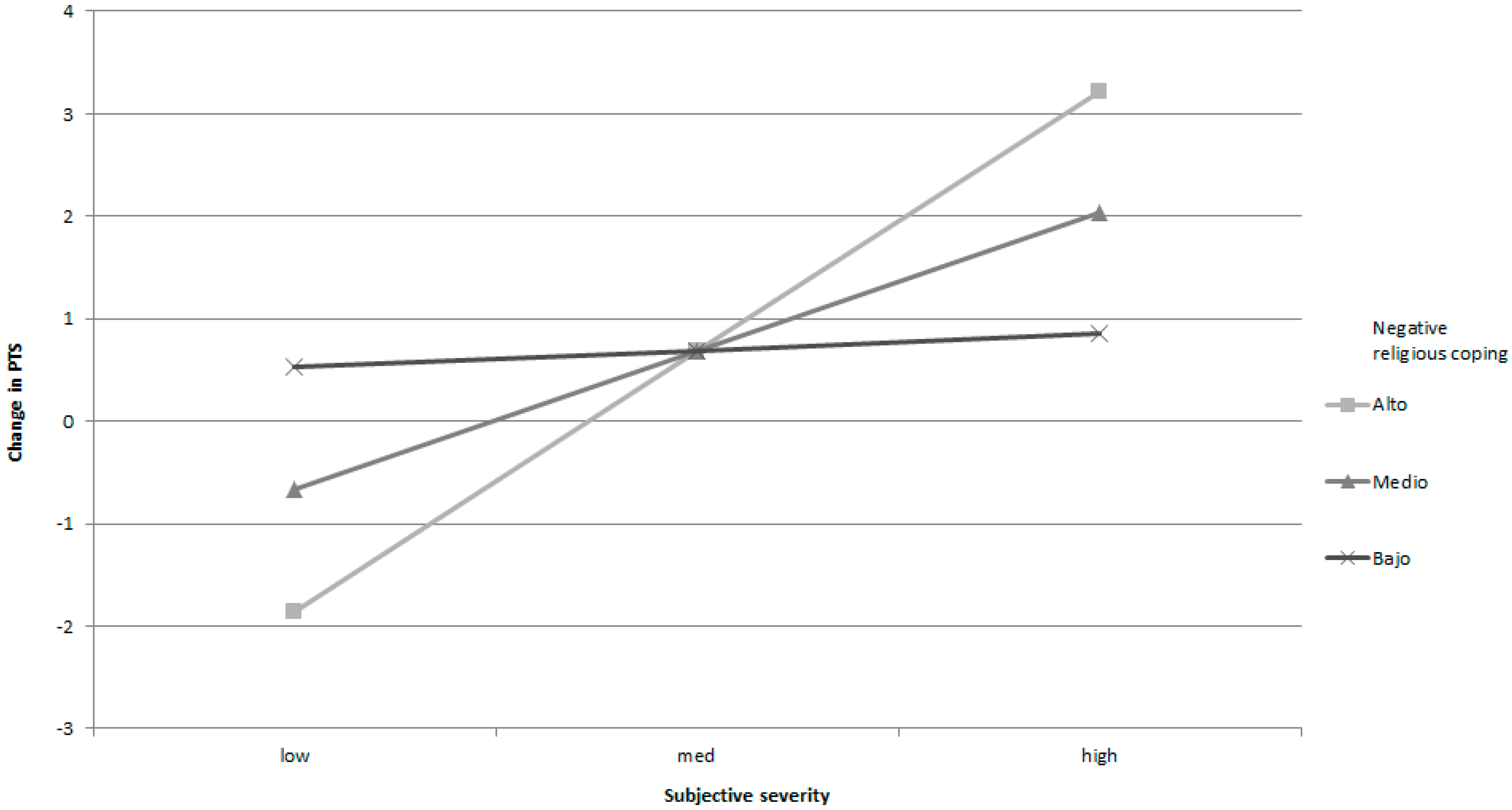
| Subjective severity T1 | 0.14 | 0.20 | 0.06 | 0.674 | 0.501 | |
| Positive RC T1 | 0.03 | 0.08 | 0.03 | 0.391 | 0.696 | |
| Negative RC T1 | −0.73 | 0.38 | −0.35 | −1.918 | 0.056 | |
| Subjective severity × Negative RC | 0.11 | 0.05 | 0.47 | 2.420 | 0.016 | |
| Negative Religious Coping | B | SE | t | p | 95% del IC | |
|---|---|---|---|---|---|---|
| LL CI | UL CI | |||||
| Low (−0.92) | 0.05 | 0.22 | 0.239 | 0.812 | −0.386 | 0.491 |
| Moderate (2.69) | 0.44 | 0.17 | 2.631 | 0.009 | 0.110 | 0.767 |
| High (6.30) | 0.82 | 0.24 | 3.428 | 0.001 | 0.350 | 1.297 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García, F.E.; Páez, D.; Reyes-Reyes, A.; Álvarez, R. Religious Coping as Moderator of Psychological Responses to Stressful Events: A Longitudinal Study. Religions 2017, 8, 62. https://doi.org/10.3390/rel8040062
García FE, Páez D, Reyes-Reyes A, Álvarez R. Religious Coping as Moderator of Psychological Responses to Stressful Events: A Longitudinal Study. Religions. 2017; 8(4):62. https://doi.org/10.3390/rel8040062
Chicago/Turabian StyleGarcía, Felipe E., Darío Páez, Alejandro Reyes-Reyes, and Rodolfo Álvarez. 2017. "Religious Coping as Moderator of Psychological Responses to Stressful Events: A Longitudinal Study" Religions 8, no. 4: 62. https://doi.org/10.3390/rel8040062
APA StyleGarcía, F. E., Páez, D., Reyes-Reyes, A., & Álvarez, R. (2017). Religious Coping as Moderator of Psychological Responses to Stressful Events: A Longitudinal Study. Religions, 8(4), 62. https://doi.org/10.3390/rel8040062