Measuring Religiosity/Spirituality: Theoretical Differentiations and Categorization of Instruments




Abstract
: There is a multitude of instruments for measuring religiosity/spirituality. Many of these questionnaires are used or even were developed in the context of studies about the connection between religiosity/spirituality and health. Thus, it seems crucial to note that measures can focus on quite different components along a hypothetical path between stressors and health. We present an instructive model which helps to identify these different components and allows the categorization of instruments of religiosity/spirituality according to their primary measurement intention: intensity/centrality, resources, needs, coping, and quality of life/well-being. Furthermore, we point out possibilities as to how religiosity and spirituality can be differentiated. We argue that the distinction between religiosity and spirituality is important in countries with a more secular background where a growing number of people identify themselves as “spiritual, but not religious”.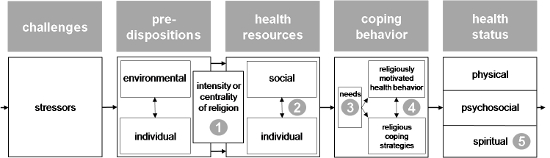
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
Within the last decade, the connection between religiosity/spirituality and health has become a subject of increasing interest particularly within the field of health care [1-3]. A considerable number of quantitative studies have so far found religious/spiritual variables to be modestly but meaningfully associated with mental or even physical health and psychosocial adjustment [2,4,5]. However, the research results are not entirely consistent; null findings and even negative associations were shown as well. This may be due to variations in subjects, stressors, or contextual characteristics and may indicate that religiosity/spirituality, especially religious/spiritual struggle and feelings of shame and guilt [6,7], can also be part of psychosocial problems. Furthermore, varying results may also reflect the breadth of indicators and questionnaires used for measuring religiosity/spirituality.
Measures of religiosity/spirituality can focus on quite different components along a hypothetical path between stressors and health. For instance, many previous studies did not explicitly differentiate between general religiosity/spirituality and religious coping (cf. [8]). General religiosity/spirituality refers to the importance of religiosity/spirituality in one's life and can be viewed as a more or less stable disposition that may constitute a resource in the process of coping with various stressors. In contrast, religious coping as an active process describes how individuals draw on their religious faith and behavior within a specific situation of crisis [8,9]. The separate assessment of both general religiosity/spirituality and religious coping has already proved to be useful: Among members of Christian churches who envisioned serious negative life events, Pargament et al. [11] found that measures of religious coping not only exhibited greater predictive power than more dispositional religious variables but also predicted outcomes above and beyond the contribution of general religiosity. Similar results have emerged from subsequent studies (cf. [9,12,13]).
In this paper we first will present an instructive model which allows us to locate different religious/spiritual components along a hypothetical path between stressors and health. On the basis of this model we then will show how questionnaires of religious/spiritual issues can be categorized according to their primary measurement intention. Due to the focus of this Special Issue of Religions and to the mainstream of contemporary research on religiosity/spirituality and health we concentrate on questionnaires although we are aware that there is a growing body of research using qualitative measures as well [14,15]. In an additional section we will discuss some proposals as to how religiosity and spirituality can be differentiated. We think that both aspects – primary measurement intention and conceptualization of religiosity and spirituality – should thoroughly be reflected, if instruments for measuring religiosity/spirituality have to be selected for a specific study.
2. Integrating Religiosity/Spirituality into the Vulnerability-Stress-Model
In recent years many pathways through which religiosity/spirituality may cause (better) health have been discussed. Among the first, Peterson and Roy [16] suggested three major pathways: Religiosity/spirituality enables the individual to experience positive emotions like hope, optimism, and solace. Religiosity/spirituality also offers many opportunities to find a meaning in one's life. Furthermore, religious communities can provide social support. As further pathways, Argyle [17,18] added religious behavior which fosters a healthy lifestyle (cf. also [19]) and a close relationship with God as a source of comfort and self-esteem. Park [20-23] highlighted in particular the importance of religiosity/spirituality as a meaning system and frame of reference, while Dörr [24] viewed also alternative value orientations (e.g., humility, abstinence, social engagement) as a salutary resource of religiosity/spirituality. Among others, Oman and Thoresen [25] further included the concept of religious coping [9,10,26] in the list of possible pathways. Finally, Koenig, McCullough, and Larson [2] distinguished factors on an individual level (such as self-esteem or meaning-making) and social resources (such as religious communities) from coping strategies which directly try to improve one's health. Additionally, their model includes the occurrence of critical life events and predispositions.
A comprehensive model which would be able to integrate the varieties of pathways mentioned should, on the one hand, include religiosity/spirituality not only as a single erratic factor whose effects are mediated by other determinants like social support or health behavior (e.g., [19]). This would surely ignore the complex dynamics which lie in religiosity/spirituality itself and, thus, would underestimate the effects of religion. Pargament [27] has called this: “explaining religion away”. Instead, a comprehensive model should include different aspects of religiosity/spirituality and demonstrate how these specific facets may interplay and be linked with health. On the other hand, however, a comprehensive model should not solely concentrate on religious/spiritual factors. This would neglect the predispositions and consequences of the multi-shaded religious/spiritual variables (e.g., [19]) and, thus, fail to link the study of religiosity/spirituality to more general models of saluto- or pathogenesis.
To consider both taking the inner dynamics of religiosity/spirituality into account and linking the study of religiosity/spirituality to the mainstream of medical and psychological research, we would like to propose integrating elaborated concepts of religiosity/spirituality into a widely accepted model of pathogenesis, the vulnerability-stress-model [28,29]. The resulting model is depicted in Figure 1 (for more detailed introduction see [30,31]).
The model in Figure 1 can be explicated as follows: According to the vulnerability-stress-model, health is the result of the individual's reactions to diverse challenges like critical life events, daily hassles, and chronic stressors. The result of this process of reactions depends on the interaction of several factors involved. Among these factors are basic predispositions on the environmental level, for instance, the individual's socialization, as well as on the individual level, for instance, the individual's hereditary dispositions. Further, the existence and availability of social and individual resources determine how successfully the challenges can be handled. Regarding religiosity/spirituality, the religious community can be viewed as a social resource, while religious beliefs which generate a basic sense of coherence may represent an individual resource. Even religious entities like God, the Virgin Mary, angels or non-Christian entities like Buddha can function as social resources on an imaginative level [11] – whether they really exist or not does not matter here because the very impression that they guide and help may already yield (healthy) effects. Whereas predispositions and resources do not concretely deal with challenges, specific coping strategies are the active processes to handle the burden of the challenges more directly. As a result, the complex interplay between the different types of factors determines the individual's status of health or illness. Besides the two groundbreaking dimensions of health or well-being – i.e., the physical status and the psychosocial or mental status – some authors introduced the concept of spiritual well-being as a further dimension [32,33]. This concept may involve various aspects such as faith, peace, and meaning [34,35], or may be divided into four domains: personal, communal, environmental, and transcendental [36,37].
In consideration of the multitude of findings already supporting a positive correlation between general religiosity and mental health (e.g., [38]), the intensity or centrality of religiosity [39,40] is prominently integrated into our model. Intensity/centrality of religiosity can be perceived as both a personality trait and a resource for coping. Consequently, our model introduces intensity/centrality as an overlapping construct in between predispositions and health resources. It should be noted that intensity/centrality of religiosity encompasses several distinct expressions of religious life, in particular an intellectual dimension, ideology, public and private practice, and religious experience [39,41,42]. The more differentiated religious expressions a person has developed the stronger his or her general religiosity is.
Within the religious coping behavior, three main components can roughly be distinguished: Coping behavior may be triggered by religious/spiritual needs and can be separated into a healthy lifestyle influenced by specific religious precepts or ethics on the one hand (more preventive), and, on the other hand, religious coping activities which directly try to cope with manifest health problems (more intervening).
3. Relating Measures of Religiosity/Spirituality to Components of the Model
On the basis of the model depicted in Figure 1 questionnaires of religiosity/spirituality can be related to distinct components of our model and, thus, categorized according to their primary measurement intention (cf [43]): intensity/centrality, resources, needs, coping, and quality of life/well-being (see No. 1–5 in Figure 1):
Intensity/centrality (see No. 1 in Figure 1)
In this area, the intensity/centrality of religiosity/spirituality is brought into focus. Thus, measures in this area have to address the question: How religious/spiritual is the respondent? To answer this question a great variety of questionnaires of diverse provenience were proposed. The presumably most classical example is the intrinsic subscale of Allport's Religious Orientation Scale (ROS; [44]) which is often used not only as a measure of intrinsic religiousness as opposed to extrinsic religiousness but also as an indicator of religiosity in general [45]. A well-elaborated and conceptual very clear operationalization of the intensity/centrality aspect is the Centrality Scale (C-Scale) recently developed by Huber [39,46] which combines Allport's concept of intrinsic religiousness with Glock's idea of several distinct expressions of religious life. Though many other scales also intend to measure the aspect of intensity/centrality, they often address another component or even several other components of our model as well. Insofar as these measures essentially mix up diverse aspects, they cannot – strictly speaking – be considered as unequivocal operationalizations of intensity/centrality. Finally, it should be pointed out that there are scales which focus on specific expressions of intensity/centrality. In particular, the dimension of religious experience has often been operationalized separately (e.g., [47,48]). Scales for the assessment of religious/spiritual experience inquire to what extent religious/spiritual experiences have been encountered.
Resources (see No. 2 in Figure 1)
Religious/spiritual scales related to the area of resources should primarily focus on global supporting functions of religiosity/spirituality. The central question is: How and to what extent does the respondent's religiosity/spirituality provide resources for coping with burden? Social resources (e.g., support by the religious congregation) can be distinguished from individual resources (e.g., a close relationship with God, the Divine, etc.). An example for a scale which includes both of these aspects is the System of Belief Inventory (SBI; [49]) which comprises a subscale “Social Support from a Religious Community” and another subscale “Beliefs and Practices” measuring the relationship with God. Many other scales deal with individual resources only, for instance the Theistic Spiritual Outcome Scale (TSOS; [50]).
Needs (see No. 3 in Figure 1)
Scales operationalizing religious/spiritual needs highlight the question: Does a person who is already suffering experience religious or spiritual needs? The fulfillment of religious/spiritual needs, e.g. by healthcare professionals, can enhance religious coping behavior and thus improve a person's well-being, especially his or her religious/spiritual well-being. Examples of scales measuring religious/spiritual needs are the Spiritual Needs Inventory (SNI; [51]) and the Spiritual Needs Questionnaire (SpNQ; [52,53]).
Coping (see No. 4 in Figure 1)
Scales measuring religious coping try to identify concrete religious/spiritual strategies and activities which are used to deal with current problems, in particular critical life events and experiences of severe illness. The central questions in this area are: How does the person concerned use religiosity/spirituality to cope with his or her burden? Does he or she use specific religious coping strategies? Several scales measuring facets of religious coping have been developed in recent years; the most prominent ones are those of Pargament and colleagues: the Brief Measure of Religious Coping (Brief RCOPE; [54]), the extended Religious Coping Scales (RCOPE; [55]), and the Religious Problem Solving Scale (RPSS; [56]) which differentiates three specific religious coping styles.
Quality of Life and Well-being (see No. 5 in Figure 1)
Scales in this area focus on religious/spiritual well-being and quality of life as an aspect of general well-being or quality of life. The underlying central question is: How can someone's religiosity/spirituality – before or after an intervention or within the process of illness and recovery – be described as a facet of his or her subjective health? Examples for scales in this area are the Spiritual Well-Being Scale (SWBS; [57,33]), the Spiritual Well-Being Questionnaire (SWBQ; [58,59]), and The Functional Assessment of Chronic Illness Therapy – Spiritual Well-Being Scale (FACIT-Sp; [60,61]). However, if such scales are used as outcome measures for religious/spiritual interventions, their contents have to be discussed very precisely to avoid an overestimation of salutogenetic effects due to tautological reasoning [cf. 62,63].
If a questionnaire for measuring religiosity/spirituality is to be selected for use in a specific study, it should be considered which component of the suggested model should be addressed and which instrument relates to the respective component as clearly as possible. One has to recognize that all instruments may measure just a specific facet of a complex construct. Thus, it is also worthwhile to select more than one instrument in order to study the interplay of several components. The identification of an appropriate measure is not always an easy task. Questionnaires may actually represent a mixture of several components and, furthermore, the labeling of the scales may be misleading. In these cases only a careful inspection of the wording of the items can give more precise information about the primary measurement intention of the instrument.
4. Religiosity vs. Spirituality
In their instructive article, Zinnbauer and Pargament [64] discuss several possibilities how to differentiate religion/religiosity and spirituality. In essence, they show that either religion or spirituality can reasonably be understood as the broader construct, depending on the concrete definitions and interrelations of the respective concepts. This highlights the necessity of explicit and clear definitions of the phenomena which are to be assessed. We do not want to repeat the arguments and would like to refer interested readers to the discussion of Zinnbauer and Pargament [64] as well as to complementary statements of other authors [e.g., 65-67]. Instead, what should be pointed out here is that there is a growing number of persons, in particular in the so-called Western world, who identify themselves as “spiritual” or even as “spiritual, but not religious”. If these individuals are to be surveyed, concepts of spirituality are needed which encompass non-religious beliefs and practices. Some considerations for a corresponding model are discussed below.
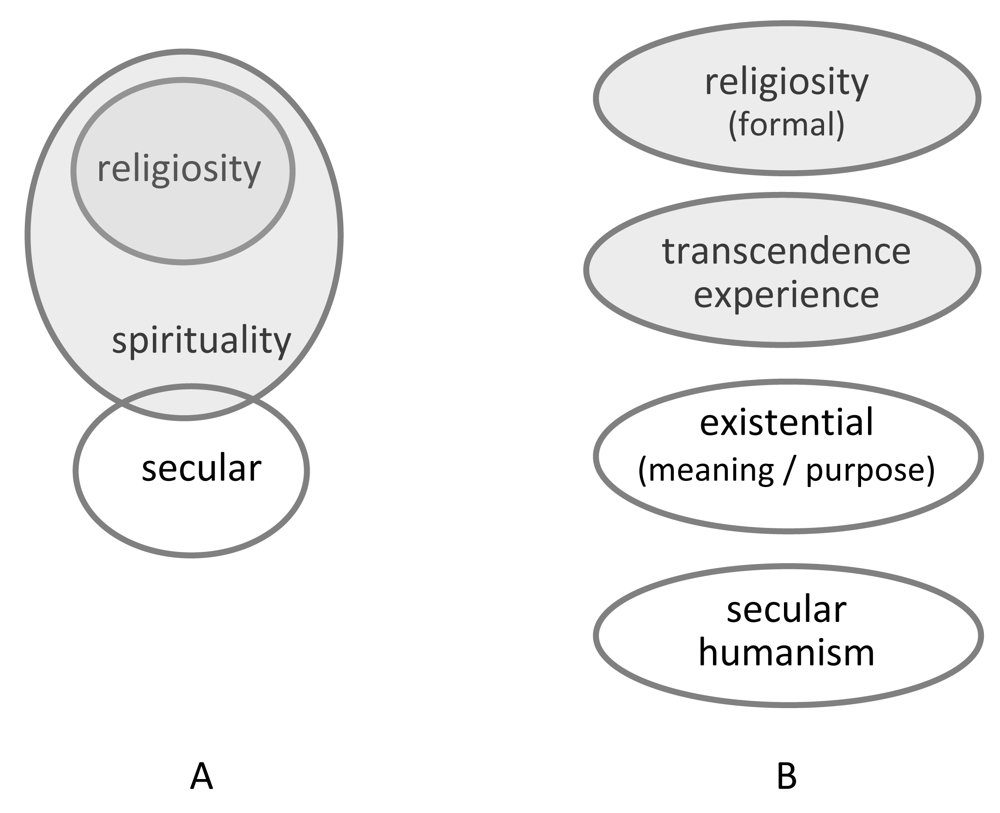
Koenig [62] raised concerns about measuring spirituality in research. He stated that spirituality was traditionally “a subset of deeply religious people”, while today it is “including religion but expanding beyond it”. In fact, spirituality is often understood today as a broader and also changing concept which may overlap with secular concepts (cf. Figure 1A) such as humanism, existentialism, and probably also with specific esoteric views. Particularly in Western societies we have to acknowledge people who regard themselves as “spiritual, but not religious”. Several of them follow more individual and pluralistic approaches. Some might be offended by institutional religiosity and thus are not belonging to a particular traditional religious system.
With respect to a self-categorization of German patients with chronic pain diseases for example (82% with a Christian denomination), 50% would not regard themselves as religious, i.e., 42% regard themselves as neither religious nor spiritual (R−S−), 8% as not religious but spiritual (R−S+), while 32% regard themselves as religious but not spiritual (R+S−) and 18% as both religious and spiritual (R+S+) [68]. It is not surprising that spiritual/religious convictions and attitudes (i.e., Search for support / access to a spiritual source or Trust in a higher source) and specific forms of practices (religious, spiritual, existential, humanistic) differ significantly between these self-categorizations [69,70]. Indeed, Trust was expressed as highly significant in both religious and spiritual patients (R+S+, R+ S−,R−S+) and accordingly correlated strongly with conventional religious practices and gratitude/reverence, while Search was expressed highly only in spiritual (R+S+ and R−S+) individuals and correlated best with both conventional religious and spiritual (mind-body) practices.
Lazenby [71] suggested differentiating between “religions” (implying individuals who follow different religious traditions) on the one hand, and the concepts “religion” and “spirituality” on the other hand, which are regarded as immediate reactions to life. For example, the Brief RCOPE “uses language that selects for people who identify with a specific religious tradition”, and thus it “studies only those who belong to an object under the concept of ‘religions’” [71]. In contrast, the Faith subscale of the FACIT-Sp is regarded to be associated with the concept of “religions”, while the Peace/Meaning subscale measures an independent dimension which Lazenby [71] calls “spirituality”.
Today, religion is often understood as an institutional and culturally determined approach which organizes the collective experiences of people into a closed system of beliefs and practices [72]. Profound spiritual experiences, however, are often highly individual and not easily communicated and shared by a group of people. Thus, spirituality is a complex and multi-dimensional issue, and can be defined as an individual and open approach in the search for meaning and purpose in life [73]. Puchalski et al. [74] also attributed the existential search for meaning and purpose to the concept of spirituality: “…the aspect of humanity that refers to the way individuals seek and express meaning and purpose and the way they experience their connectedness to the moment, to the self, to others, to nature, and to the significant or sacred.” Spirituality can then be found through religious engagement, through an individual experience of the divine, and/or through a connection to nature [62]. Thus, particularly in secular societies one should be aware that there are people which experience spirituality in religion (which takes place within religious traditions and their institutions) while others experience spirituality as opposed to religion (which rejects organized religiosity).
One cannot ignore that broader conceptualizations of spirituality may be less specific for particular religious denominations. To overcome this problem, one could differentiate various aspects of spirituality which are either relevant for (or even shared by) distinct religious traditions or particularly by secular people. To measure a wide variety of important aspects of spirituality, Büssing [75] analyzed the answers of expert representatives of various spiritual orientations which aspects of spirituality are relevant to them (i.e., Catholics, Protestants, members of the Anthroposophic “Christengemeinschaft”, Bahá'í, Muslims, Jews, Buddhists, and atheists). The identified motifs were condensed to a questionnaire which primarily differentiates seven core factors, i.e., Religious Orientation (prayer, trust in God, shelter); Insight, awareness and wisdom; Transcendence conviction; Compassion, generosity and patience; Conscious interactions; Gratitude, reverence and respect; and Equanimity [76]. Finally, one can differentiate four main categories: (1) Religious orientation (i.e., praying, trust in God, feeling guided/sheltered etc.) (2) Search for insight/wisdom (i.e., philosophical and existential views), (3) Conscious interactions (i.e., relational consciousness, compassion, generosity) and (4) Transcendence conviction (i.e., rebirth, higher powers/beings, higher dimension, etc.) [77]. Similar attempts to measure different aspects of spirituality can be found in the FACIT-Sp which differentiates Faith, Meaning and Peace [60], in the SWBQ which differentiates Personal, Transcendental, Environmental, and Communal Well-being [58], in the SpNQ which differentiates Religious Needs, Inner Peace, Existential Needs (Reflection/Meaning), and Actively Giving [53], and in several other instruments.
Therefore, spirituality could be viewed as a general concept which may include specific views and practices of formal religiosity, which may nevertheless share aspects of secular humanism and existentialism (Figure 2A). To capture a wide variety of spiritual convictions and attitudes, these dimensions could be measured independently, i.e., formal religiosity, experiential aspects of spirituality (transcendence experience), existential aspects, and secular humanism (Figure 2B). While this differentiation can be important in countries with a more secular background (i.e., Europe), this distinction might be meaningless in countries with conservative but vital religious beliefs.
5. Concluding Remarks
In this paper we first suggested that the well-known vulnerability-stress-model [28,29] can appropriately be used for locating different religious/spiritual components along a hypothetical path between stressors and health. This may serve as a reasonable basis for categorizing measures of religiosity/spirituality according to their primary measurement intention. Before choosing a questionnaire for use in a specific study it should thoroughly be reflected which religious/spiritual component or components should be addressed and which instruments ensure conceptually clear-cut operationalizations. In many cases, reliable information about the primary measurement intention of the instrument can only be derived through a careful inspection of the wording of the items.
The wording of the items is also important when decisions have to be made between instruments using a specific religious terminology and instruments referring to a broader variety of worldviews. Thus, instruments with a very particular religious perspective and traditional religious terminology are less suited for individuals with an atheistic or agnostic background, who nevertheless may appreciate pluralistic forms of spirituality. Beyond the differentiations between religiosity and spirituality, it is crucial to ensure that the respondents understand the items and consider the contents to be appropriate. We argue that the distinction between religiosity and spirituality is especially important in countries with a more secular background where a growing number of people identify themselves as “spiritual, but not religious”.
Of course, in selecting appropriate questionnaires, many more issues should also be considered, amongst others psychometric properties, length of the instruments, and the possibility for comparisons with prior studies [43]. We do not argue that these more technical criteria should be neglected. But sometimes it seems to be worthwhile to step back and reflect about measurement intentions and item wording. This should help to choose questionnaires tailored to the specific study design as well as to respondents.


References
- C. Klein, H. Berth, and F. Balck, eds. Gesundheit – Religion – Spiritualität. Konzepte, Befunde und Erklärungsansätze. Weinheim, Germany: Juventa, 2011.
- H.G. Koenig, M.E. McCullough, and D.B. Larson, eds. Handbook of Religion and Health. New York, NY, USA: Oxford University Press, 2001.
- T.G. Plante, and A.C. Sherman, eds. Faith and Health. Psychological Perspectives. New York, NY, USA: Guilford, 2001.
- L. Miller, and B.S. Kelley. Relationships of religiosity and spirituality with mental health and psychopathology. In Handbook of the Psychology of Religion and Spirituality. Edited by R.F. Paloutzian, and C.L. Park. New York, NY, USA: Guilford, 2005, pp. 460–478. [Google Scholar]
- Y. Chida, A. Steptoe, and L.H. Powell. “Religiosity/spirituality and mortality.” Psychother. Psychosom. 78 (2009): 81–90. [Google Scholar]
- J.J. Exline. “The picture is getting clearer, but is the scope too limited? Three overlooked questions in the psychology of religion.” Psychol. Inq. 13 (2002): 245–247. [Google Scholar]
- J.J. Exline, and E. Rose. Religious and spiritual struggles. In Handbook of the Psychology of Religion and Spirituality. Edited by R.F. Paloutzian, and C.L. Park. New York, NY, USA: Guilford, 2005, pp. 315–330. [Google Scholar]
- A.C. Sherman, and S. Simonton. Religious involvement among cancer patients. Associations with adjustment and quality of life. In Faith and Health. Psychological Perspectives. Edited by T.G. Plante, and A.C. Sherman. New York, NY, USA: Guilford, 2001, pp. 167–194. [Google Scholar]
- K.I. Pargament. The Psychology of Religion and Coping. Theory, Research, Practice. New York, NY, USA: Guilford, 1997. [Google Scholar]
- K.I. Pargament, G.G. Ano, and A.B. Wachholtz. The religious dimension of coping: Advances in theory, research, and practice. In Handbook of the Psychology of Religion and Spirituality. Edited by R.F. Paloutzian, and C.L. Park. New York, NY, USA: Guilford, 2005, pp. 479–495. [Google Scholar]
- K.I. Pargament, D.S. Ensing, K. Falgout, H. Olsen, B. Reilly, K. Van Haitsma, and R. Warren. “God help me: (I): Religious coping efforts as predictors of the outcomes to significant negative life events.” Am. J. Community Psychol. 18 (1990): 793–824. [Google Scholar]
- U. Winter, D. Hauri, S. Huber, J. Jenewein, U. Schnyder, and B. Kraemer. “The psychological outcome of religious coping with stressful life events in a Swiss sample of church attendees.” Psychother. Psychosom. 78 (2009): 240–244. [Google Scholar]
- C. Zwingmann, C. Müller, J. Körber, and S. Murken. “Religious commitment, religious coping and anxiety: A study in German patients with breast cancer.” Eur. J Cancer Care 17 (2008): 361–370. [Google Scholar]
- J.A. Belzen, and R.W. Hood. “Methodological issues in the psychology of religion. Toward another paradigm? ” J. Psychol. 140 (2006): 5–28. [Google Scholar]
- D.M. Wulff. Empirical research on religion: Perspectives from the psychology of religion. In Religion: Immediate Experience and the Mediacy of Research. Interdisciplinary Studies in Objectives, Concepts and Methodology of Empirical Research in Religion. Edited by H.-G. Heimbrock, and C. Scholtz. Göttingen, Germany: Vandenhoeck & Ruprecht, 2007, pp. 259–273. [Google Scholar]
- L.R. Peterson, and A. Roy. “Religiosity, anxiety, and meaning and purpose.” Rev. Relig. Res. 27 (1985): 49–62. [Google Scholar]
- M. Argyle. Causes and correlates of happiness. In Well-Being: The Foundations of Hedonic Psychology. Edited by D. Kahneman, E. Diener, and N. Schwarz. New York, NY, USA: Russell Sage Foundation, 1999, pp. 353–373. [Google Scholar]
- M. Argyle. Psychology and Religion. An Introduction. London, UK: Routledge, 2000. [Google Scholar]
- J.E. Bower, E. Epel, and J.T. Moskowitz. Biological correlates: How psychological components of benefit finding may lead to physiological benefits. In Medical Illness and Positive Life Change. Can Crisis Lead to Personal Transformation? Edited by C.L. Park, S.C. Lechner, M.H. Antoni, and A.L. Stanton. Washington, DC, USA: American Psychological Association, 2009, pp. 155–172. [Google Scholar]
- C.L. Park. Religion and meaning. In Handbook of the Psychology of Religion and Spirituality. Edited by R.F. Paloutzian, and C.L. Park. New York, NY, USA: Guilford, 2005, pp. 295–314. [Google Scholar]
- C.L. Park. “Religion as a meaning-making framework in coping with life stress.” J. Soc. Issues 61 (2005): 707–729. [Google Scholar]
- C.L. Park. “Religiousness/spirituality and health: A meaning systems perspective.” J. Behav. Med. 30 (2007): 319–328. [Google Scholar]
- C.L. Park, and S. Folkman. “Meaning in the context of stress and coping.” Rev. Gen. Psychol. 1 (1997): 115–144. [Google Scholar]
- A. Dörr. Religiosität und psychische Gesundheit. Zur Zusammenhangsstruktur spezifischer religiöser Konzepte. Hamburg, Germany: Kovac, 2001. [Google Scholar]
- D. Oman, and C.E. Thoresen. Do religion and spirituality influence health? In Handbook of the Psychology of Religion and Spirituality. Edited by R.F. Paloutzian, and C.L. Park. New York, NY, USA: Guilford, 2005, pp. 435–459. [Google Scholar]
- K.I. Pargament. Spiritually Integrated Psychotherapy. Understanding and Addressing the Sacred. New York, NY, USA: Guilford, 2007. [Google Scholar]
- K.I. Pargament. “Is religion nothing but.? Explaining religion versus explaining religion away.” Psychol. Inq. 13 (2002): 239–244. [Google Scholar]
- R.E. Ingram, and J.M. Price. Vulnerability to Psychopathology. Risk Across the Lifespan. New York, NY, USA: Guilford, 2001. [Google Scholar]
- M. Zuckerman. Vulnerability to Psychopathology. A Biosocial Model. Washington, DC, USA: American Psychological Association, 1999. [Google Scholar]
- C. Klein, and C. Albani. Religiosität und psychische Gesundheit – empirische Befunde und Erklärungsansätze. In Gesundheit – Religion – Spiritualität. Konzepte, Befunde und Erklärungsansätze. Edited by C. Klein, H. Berth, and F. Balck. Weinheim, Germany: Juventa, 2011, pp. 212–242. [Google Scholar]
- C. Klein, and C. Albani. “Die Bedeutung von Religion für die psychische Befindlichkeit: Mögliche Erklärungsansätze und allgemeines Wirkmodell.” Zeitschrift für Nachwuchswissenschaftler, 2011. http://www.nachwuchswissenschaftler.org/2011/1/20. [Google Scholar]
- D.O. Moberg. Spiritual Well-Being: Background and Issues. Washington, DC, USA: White House Conference on Aging, 1971. [Google Scholar]
- R.F. Paloutzian, and C.W. Ellison. Loneliness, spiritual well-being and the quality of life. In Loneliness: A Sourcebook of Current Theory, Research and Therapy. Edited by L.A. Peplau, and D. Perlman. New York, NY, USA: Wiley, 1982, pp. 224–237. [Google Scholar]
- A.L. Canada, P.E. Murphy, G. Fitchett, A.H. Peterman, and L.R. Schover. “A 3-factor model for the FACIT-Sp.” Psychooncology 17 (2008): 908–916. [Google Scholar]
- H.S. Whitford, and I.N. Olver. “The multidimensionality of spiritual wellbeing: Peace, meaning, and faith and their association with quality of life and coping in oncology.” Psychooncology, 2011. [Google Scholar] [CrossRef]
- J.W. Fisher, L.J. Francis, and P. Johnson. “Assessing spiritual health via four domains of well-being: The SH4DI.” Pastoral Psychol. 49 (2000): 133–145. [Google Scholar]
- J. Fisher. “Development and application of a spiritual well-being questionnaire called SHALOM.” Religions 1 (2010): 105–121. [Google Scholar]
- C.H. Hackney, and G.S. Sanders. “Religiosity and mental health: A meta-analysis of recent studies.” J. Sci. Stud. Relig. 42 (2003): 43–55. [Google Scholar]
- S. Huber. Zentralität und Inhalt. Ein neues multidimensionales Messmodell der Religiosität. Opladen, Germany: Leske & Budrich, 2003. [Google Scholar]
- S. Huber. “Kerndimensionen, Zentralität und Inhalt. Ein interdisziplinäres Modell der Religiosität.” Journal für Psychologie, 2008, 16. Article 05, http://www.journal-fuer-psychologie.de/jfp-3-2008-05.html. [Google Scholar]
- C.Y. Glock. “On the study of religious commitment.” Relig. Educ. 57 (1962): 98–110. [Google Scholar]
- R. Stark, and C.Y. Glock. American Piety: The Nature of Religious Commitment. Berkeley, CA, USA: University of California Press, 1968. [Google Scholar]
- C. Zwingmann, C. Klein, and V. Höfling. Messung von Religiosität/Spiritualität im Rahmen der Gesundheitsforschung: Ein Überblick über deutschsprachige Fragebogenskalen. In Gesundheit – Religion – Spiritualität. Konzepte, Befunde und Erklärungsansätze. Edited by C. Klein, H. Berth, and F. Balck. Weinheim, Germany: Juventa, 2011, pp. 65–91. [Google Scholar]
- G.W. Allport, and J.M. Ross. “Personal religious orientation and prejudice.” J. Pers. Soc. Psychol. 5 (1967): 432–443. [Google Scholar]
- Fetzer Institute, Ed. Commitment. In Multidimensional Measurement of Religiousness/Spirituality for Use in Health Research: A Report of the Fetzer Institute / National Institute on Aging Working Group. Fetzer Institute, Ed. KalamazMI, USA: Fetoo, zer Institute, 2003, pp. 71–74. [Google Scholar]
- D. Lehr, C. Klein, and S. Huber. “Zentralität der Religiosität in der Persönlichkeit. Teststatistische Prüfung und Normierung der Zentralitätsskala Z7 in Deutschland, Österreich und der Schweiz.” Diagnostica, 2011. Forthcoming. [Google Scholar]
- R.W. Hood. “The construction and preliminary validation of a measure of reported mystical experience.” J. Sci. Stud. Relig. 14 (1975): 29–41. [Google Scholar]
- R.L. Piedmont. “Does spirituality represent the sixth factor of personality? Spiritual transcendence and the five-factor model.” J. Pers. 67 (1999): 985–1013. [Google Scholar]
- J.C. Holland, K.M. Kash, S. Passik, M.K. Gronert, A. Sison, M. Lederberg, S.M. Russak, L. Baider, and B. Fox. “A brief spiritual beliefs inventory for use in quality of life research in lifethreatening illness.” Psychooncology 7 (1998): 460–469. [Google Scholar]
- P.S. Richards, T.B. Smith, M. Schowalter, M. Richard, M.E. Berrett, and R.K. Hardman. “Development and validation of the theistic spiritual outcome survey.” Psychother. Res. 15 (2005): 457–469. [Google Scholar]
- C. Hermann. “Development and testing of the spiritual needs inventory for patients near the end of life.” Oncol. Nurs. Forum 33 (2006): 737–744. [Google Scholar]
- A. Büssing, H.J. Balzat, and P. Heusser. “Spirituelle Bedürfnisse von Patienten mit chronischen Schmerz- und Tumorerkrankungen.” Perioperative Medizin 1 (2009): 248. [Google Scholar]
- A. Büssing, H.J. Balzat, and P. Heusser. “Spiritual needs of patients with chronic pain diseases and cancer – Validation of the Spiritual Needs Questionnaire.” Eur. J. Med. Res. 15 (2010): 266–273. [Google Scholar]
- K.I. Pargament, B.W. Smith, H.G. Koenig, and L.M. Perez. “Patterns of positive and negative religious coping with major life stressors.” J. Sci. Stud. Relig. 37 (1998): 710–724. [Google Scholar]
- K.I. Pargament, H.G. Koenig, and L.M. Perez. “The many methods of religious coping: Development and initial validation of the RCOPE.” J. Clin. Psychol. 56 (2000): 519–543. [Google Scholar]
- K.I. Pargament, J. Kennell, W. Hathaway, N. Grevengoed, J. Newman, and W. Jones. “Religion and the problem-solving process: Three styles of coping.” J. Sci. Stud. Relig. 27 (1988): 90–104. [Google Scholar]
- C.W. Ellison. “Spiritual well-being: Conceptualization and measurement.” J. Psychol. Theol. 11 (1983): 330–340. [Google Scholar]
- R. Gomez, and J.W. Fisher. “Domains of spiritual well-being and development and validation of the Spiritual Well-Being Questionnaire.” Pers. Individ. Dif. 35 (2003): 1975–1991. [Google Scholar]
- R. Gomez, and J.W. Fisher. “The Spiritual Well-Being Questionnaire: Testing for model applicability, measurement and structural equivalencies and latent mean differences across gender.” Pers. Individ. Dif. 39 (2005): 1383–1393. [Google Scholar]
- A.H. Peterman, G. Fitchett, M.J. Brady, L. Hernandez, and D. Cella. “Measuring spiritual well-being in people with cancer: The Functional Assessment of Chronic Illness Therapy – Spiritual Well-being Scale (FACIT-Sp).” Ann. Behav. Med. 24 (2002): 49–58. [Google Scholar]
- J.M. Bredle, J.M. Salsman, S.M. Debb, B.J. Arnold, and D. Cella. “Spiritual Well-Being as a component of health-related quality of life: The Functional Assessment of Chronic Illness Therapy – Spiritual Well-Being Scale (FACIT-Sp).” Religions 2 (2011): 77–94. [Google Scholar]
- H.G. Koenig. “Concerns about measuring “spirituality” in research.” J. Nerv. Ment. Dis. 196 (2008): 349–355. [Google Scholar]
- R.P. Sloan, E. Bagiella, and T. Powell. “Religion, spirituality, and medicine.” Lancet 353 (1999): 664–667. [Google Scholar]
- B.J. Zinnbauer, and K.I. Pargament. Religiousness and spirituality. In Handbook of the Psychology of Religion and Spirituality. Edited by R.F. Paloutzian, and C.L. Park. New York, NY, USA: Guilford, 2005, pp. 21–42. [Google Scholar]
- R. Fuller. Spiritual, but not Religious. Understanding Unchurched America. New York, NY, USA: Oxford University Press, 2001. [Google Scholar]
- R.W. Hood. Spirituality and religion. In Religion Critical Approaches to Drawing Bounderies between Sacred and Secular. Edited by A.L. Greil, and D.G. Bromley. Amsterdam, The Netherlands: Elsevier, 2003, pp. 241–264. [Google Scholar]
- M. Utsch, and C. Klein. Religion, Religiosität, Spiritualität. Bestimmungsversuche für komplexe Begriffe. In Gesundheit – Religion – Spiritualität. Konzepte, Befunde und Erklärungsansätze. Edited by C. Klein, H. Berth, and F. Balck. Weinheim, Germany: Juventa, 2011, pp. 25–45. [Google Scholar]
- A. Büssing, A. Michalsen, H.J. Balzat, R.A. Grünther, T. Ostermann, E.A.M. Neugebauer, and P.F. Matthiessen. “Are spirituality and religiosity resources for patients with chronic pain conditions? ” Pain Med. 10 (2009): 327–339. [Google Scholar]
- A. Büssing, P.F. Matthiessen, and T. Ostermann. “Engagement of patients in religious and spiritual practices: Confirmatory results with the SpREUK-P 1.1 questionnaire as a tool of quality of life research.” Health Qual. Life Out. 3 (2005): 53. [Google Scholar]
- A. Büssing. “The SpREUK-SF10 questionnaire as a rapid measure of spiritual search and religious trust in patients with chronic diseases.” Zhong Xi Yi Jie He Xue Bao 8 (2010): 832–841. [Google Scholar]
- J.M. Lazenby. “On “spirituality,” “religion,” and “religions”: A concept analysis.” Palliat. Support. Care 8 (2010): 469–476. [Google Scholar]
- P.S. Mueller, D.J. Plevak, and T.A. Rummans. “Religious involvement, spirituality, and medicine: Implications for clinical practice.” Mayo Clin. Proc. 76 (2001): 1225–1235. [Google Scholar]
- A. Büssing, T. Ostermann, and P.F. Matthiessen. “Role of religion and spirituality in medical patients: Confirmatory results with the SpREUK questionnaire.” Health Qual. Life Out. 3 (2005): 10. [Google Scholar]
- C. Puchalski, B. Ferrell, R. Virani, S. Otis-Green, P. Baird, J. Bull, H. Chochinov, G. Handzo, H. Nelson-Becker, M. Prince-Paul, K. Pugliese, and D. Sulmasy. “Improving the quality of spiri-tual care as a dimension of palliative care: The report of the consensus conference.” J. Palliat. Med. 12 (2009): 885–904. [Google Scholar]
- A. Büssing. “Spiritualität” – Worüber reden wir? In Spiritualität, Krankheit und Heilung – Bedeutung und Ausdrucksformen der Spiritualität in der Medizin. Edited by A. Büssing, T. Ostermann, M. Glöckler, and P.F. Matthiessen. Frankfurt am Main, Germany: Verlag für Akademische Schriften, 2006, pp. 11–24. [Google Scholar]
- A. Büssing, T. Ostermann, and P.F. Matthiessen. “Distinct expressions of vital spirituality. The ASP questionnaire as an explorative research tool.” J. Relig Health 46 (2007): 267–286. [Google Scholar]
- A. Büssing, A. Föller-Mancini, J. Gidley, and P. Heusser. “Aspects of spirituality in adolescents.” Int. J. Child. Spiritual. 15 (2010): 25–44. [Google Scholar]
© 2011 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zwingmann, C.; Klein, C.; Büssing, A. Measuring Religiosity/Spirituality: Theoretical Differentiations and Categorization of Instruments. Religions 2011, 2, 345-357. https://doi.org/10.3390/rel2030345
Zwingmann C, Klein C, Büssing A. Measuring Religiosity/Spirituality: Theoretical Differentiations and Categorization of Instruments. Religions. 2011; 2(3):345-357. https://doi.org/10.3390/rel2030345
Chicago/Turabian StyleZwingmann, Christian, Constantin Klein, and Arndt Büssing. 2011. "Measuring Religiosity/Spirituality: Theoretical Differentiations and Categorization of Instruments" Religions 2, no. 3: 345-357. https://doi.org/10.3390/rel2030345
APA StyleZwingmann, C., Klein, C., & Büssing, A. (2011). Measuring Religiosity/Spirituality: Theoretical Differentiations and Categorization of Instruments. Religions, 2(3), 345-357. https://doi.org/10.3390/rel2030345