
Spirituality as a Predictor of Well-Being, Mental Distress or Both: A Four-Week Follow-Up Study in a Sample of Dutch and Belgian Adults

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Method
2.1. Sampling
2.2. Participants
2.3. Instruments
2.4. Statistics
- Step 1: taking demographic covariates into account, spirituality at T1 was used as independent variable;
- Step 2: taking demographic covariates as well as baseline mental distress into account, mental distress at T1 was added as an independent variable;
- Step 3: taking demographic covariates as well as baseline well-being into account, mental distress at T1 was exchanged for T1 well-being; and
- Step 4: take demographic covariates as well as baseline mental distress and baseline well-being into account.
3. Results
3.1. Sample Characteristics
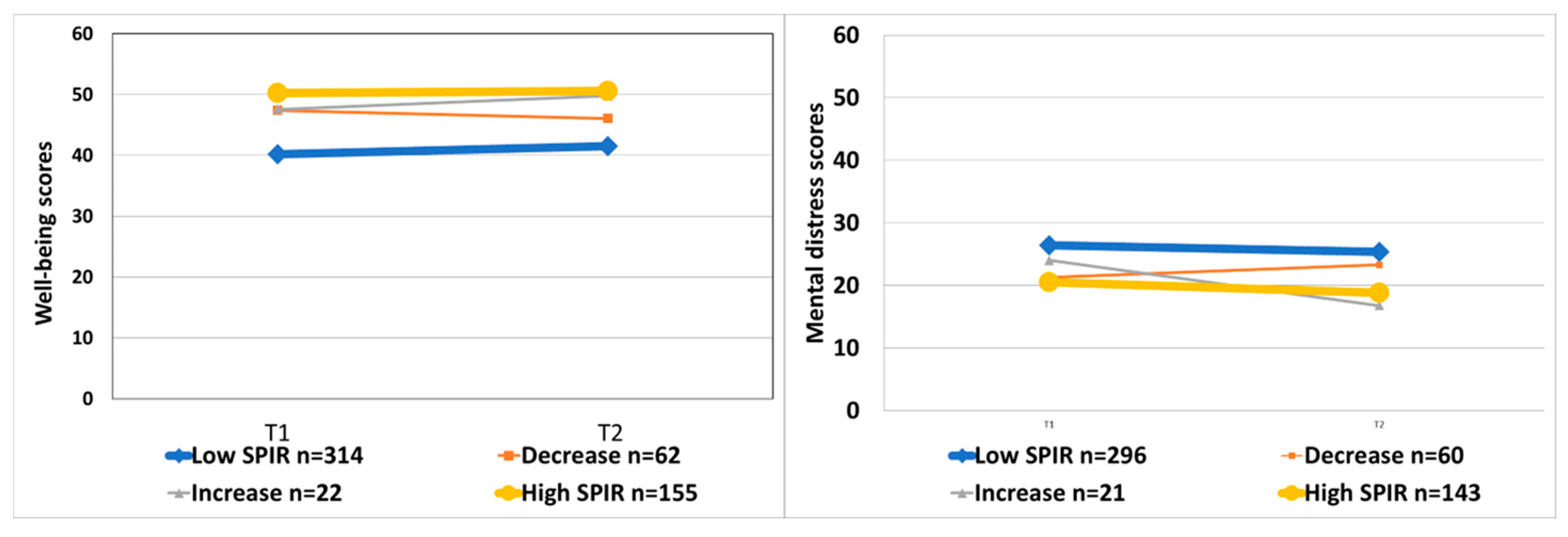
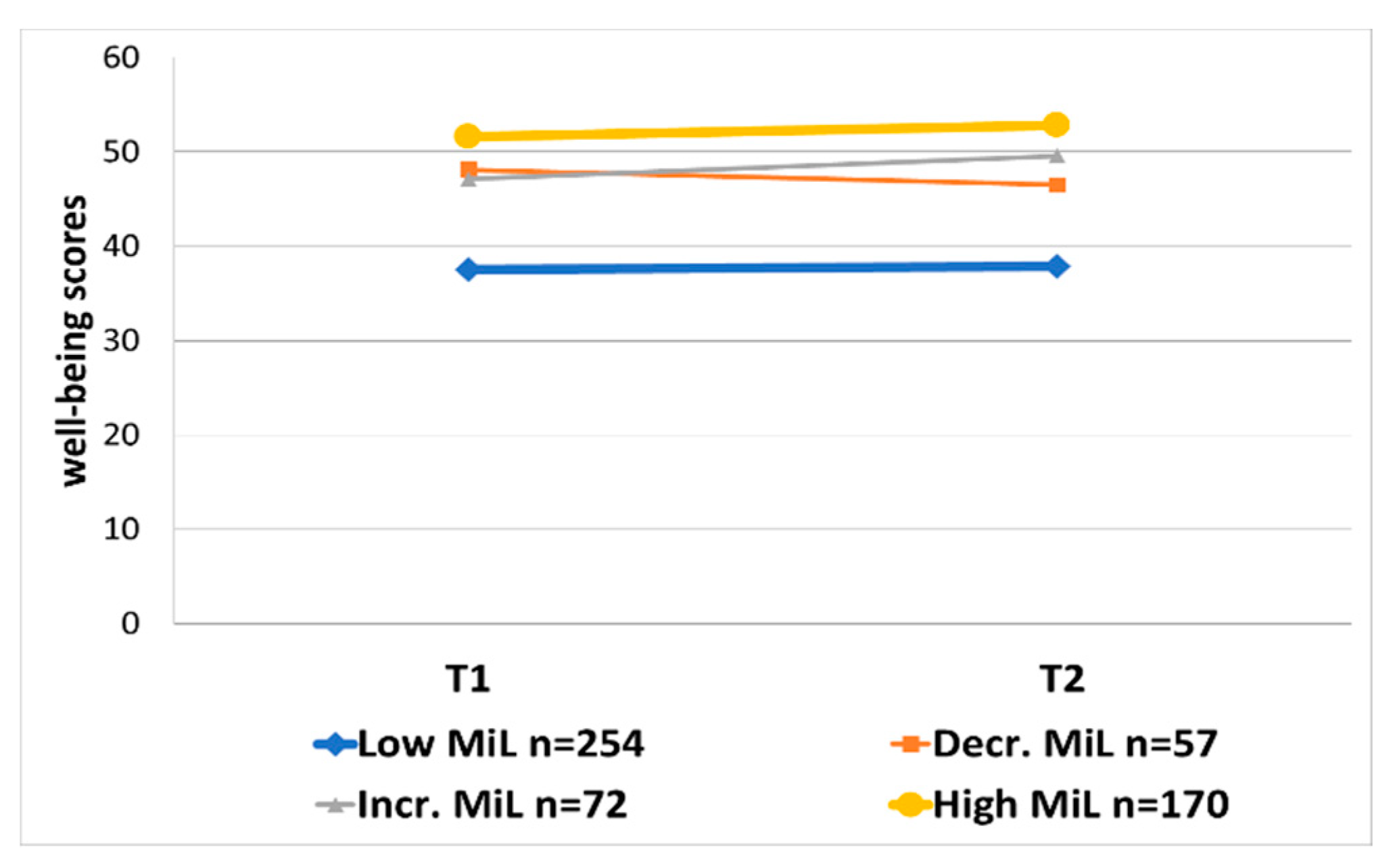
3.2. Prospective Association between Spirituality and Well-Being
3.3. Prospective Association between Spirituality and Mental Distress
3.4. Additional Analyses: Possible Modification by Age, Education or Well-Being
4. Discussion
4.1. Practical Implications
4.2. Limitations
5. Further Research and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bartlett, Susan J., Ralph Piedmont, Andrew Bilderback, Alan K. Matsumoto, and Joan M. Bathon. 2003. Spirituality, well-being, and quality of life in people with rheumatoid arthritis. Arthritis Rheum 49: 778–83. [Google Scholar] [CrossRef]
- Bauereiß, Natalie, Stefanie Obermaier, Selçuk Erol Özünal, and Harald Baumeister. 2018. Effects of existential interventions on spiritual, psychological, and physical well-being in adult patients with cancer: Systematic review and meta-analysis of randomized controlled trials. Psychooncology 27: 2531–45. [Google Scholar] [CrossRef]
- Bohlmeijer, Ernst, Filip Smit, and Pim Cuijpers. 2003. Effects of reminiscence and life review on late-life depression: A meta-analysis. International Journal of Geriatric Psychiatry 18: 1088–94. [Google Scholar] [CrossRef]
- Bohlmeijer, Ernst, Marte Roemer, Pim Cuijpers, and Filip Smit. 2007. The effects of reminiscence on psychological well-being in older adults: A meta-analysis. Aging & Mental Health 11: 291–300. [Google Scholar] [CrossRef]
- Braam, Arjan W., and Harold G. Koenig. 2019. Religion, spirituality and depression in prospective studies: A systematic review. Journal of Affective Disorders 257: 428–38. [Google Scholar] [CrossRef]
- Breitbart, William, Hayley Pessin, Barry Rosenfeld, Allison J. Applebaum, Wendy G. Lichtenthal, Yuelin Li, Rebecca M. Saracino, Allison M. Marziliano, Melissa Mastersonm Kristen Tobias, and Natalie Fenn. 2018. Individual meaning-centered psychotherapy for the treatment of psychological and existential distress: A randomized controlled trial in patients with advanced cancer. Cancer 124: 3231–39. [Google Scholar] [CrossRef]
- Carlier, Ingird, Yvonne Schulte-Van Maaren, Klaas Wardenaar, Erik Giltay, Martijn Van Noorden, Peter Vergeer, and Frans Zitman. 2012. Development and validation of the 48-item Symptom Questionnaire (SQ-48) in patients with depressive, anxiety and somatoform disorders. Psychiatry Research 200: 904–10. [Google Scholar] [CrossRef] [PubMed]
- de Jager Meezenbroek, Eltica, Bert Garssen, Machteld van den Berg, Dirk van Dierendonck, Adriaan Visser, and Wilmar B. Schaufeli. 2012. Measuring spirituality as a universal human experience: A review of spirituality questionnaires. Journal of Religion and Health 51: 336–54. [Google Scholar] [CrossRef] [PubMed]
- Deluga, Alina, Beata Dobrowolska, Krzysztof Jurek, Barbara Ślusarska, Grzegorz Nowicki, and Alvisa Palese. 2020. Nurses’ spiritual attitudes and involvement-Validation of the Polish version of the Spiritual Attitude and Involvement List. PLoS ONE 15: e0239068. [Google Scholar] [CrossRef] [PubMed]
- Garssen, Bert, Anja Visser, and Grieteke Pool. 2021. Does Spirituality or Religion Positively Affect Mental Health? Meta-analysis of Longitudinal Studies. The International Journal for the Psychology of Religion 31: 4–20. [Google Scholar] [CrossRef]
- Helliwell, John F., Richard Layard, and Jeffrey D. Sachs. 2019. World Happiness Report 2019. Available online: https://worldhappiness.report/ed/2019/ (accessed on 20 March 2019).
- Keyes, Corey L. M. 2002. The mental health continuum: From languishing to flourishing in life. Journal of Health and Social Behavior 43: 207–22. [Google Scholar] [CrossRef]
- Kim, Jookyoung. 2018. Consideration of the applicability of person-centered therapy to culturally varying clients, focusing on the actualizing tendency and self-actualization—From East Asian perspective. Person-Centered & Experiential Psychotherapies 17: 201–23. [Google Scholar] [CrossRef]
- Koenig, Harold G. 2010. Spirituality and mental health. International Journal of Applied Psychoanalytic Studies 7: 116–22. [Google Scholar] [CrossRef]
- Koltko-Rivera, Mark E. 2006. Rediscovering the Later Version of Maslow’s Hierarchy of Needs: Self-Transcendence and Opportunities for Theory, Research, and Unification. Review of General Psychology 10: 302–17. [Google Scholar] [CrossRef]
- Kotzé, Zacharias. 2014. Jung, Individuation, and Moral Relativity in Qohelet 7:16—17. Journal of Religion and Health 53: 511–19. Available online: http://www.jstor.org.ezproxy.elib11.ub.unimaas.nl/stable/24485101 (accessed on 30 November 2023). [CrossRef]
- Lamers, Sanne M. A., Gerben J. Westerhof, Ernst T. Bohlmeijer, Peter M. ten Klooster, and Corey L. M. Keyes. 2011. Evaluating the psychometric properties of the mental health Continuum-Short Form (MHC-SF). Journal of Clinical Psychology 67: 99–110. [Google Scholar] [CrossRef]
- Lifshitz, Rinat, Galit Nimrod, and Yaacov G. Bachner. 2019. Spirituality and wellbeing in later life: A multidimensional approach. Aging & Mental Health 23: 984–91. [Google Scholar] [CrossRef]
- Lucchetti, Giancarlo, Harold G. Koenig, and Alessandra Lamas Granero Lucchetti. 2021. Spirituality, religiousness, and mental health: A review of the current scientific evidence. Journal of Clinical Cases 9: 7620–31. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, Douglas A. 2000. Spirituality: Description, measurement, and relation to the five factor model of personality. Journal of Personality 68: 153–97. [Google Scholar] [CrossRef]
- MacDonald, Douglas A., Harris L. Friedman, Jacek Brewczynski, Daniel Holland, Kiran Kumar K. Salagame, K. Krishna Mohan, Zuzana Ondriasova Gubrij, and Hye Wook Cheong. 2015. Spirituality as a scientific construct: Testing its universality across cultures and languages. PLoS ONE 10: e0117701. [Google Scholar] [CrossRef]
- McClintock, Clayton H., Elsa Lau, and Lisa Miller. 2016. Phenotypic Dimensions of Spirituality: Implications for Mental Health in China, India, and the United States [Original Research]. Frontiers in Psychology 7: 1600. [Google Scholar] [CrossRef] [PubMed]
- Michaelson, Valerie, Fiona Brooks, Ivo Jirásek, Jo Inchley, Ross Whitehead, Nathan King, Sophie Walsh, Colleen M. Davison, Joanna Mazur, William Pickett, and et al. 2016. Developmental patterns of adolescent spiritual health in six countries. SSM-Population Health 2: 294–303. [Google Scholar] [CrossRef] [PubMed]
- Nolan, Steve, Philip Saltmarsh, and Carlo Leget. 2011. Spiritual care in palliative care: Working towards an EAPC Task Force. European Public Law 18: 86–89. [Google Scholar]
- Noy, Chaim. 2008. Sampling Knowledge: The Hermeneutics of Snowball Sampling in Qualitative Research. International Journal of Social Research Methodology 11: 327–44. [Google Scholar] [CrossRef]
- Paloutzian, Raymond F., and Crystal L. Park. 2014. Handbook of the Psychology of Religion and Spirituality. New York: Guilford Publications. [Google Scholar]
- Pargament, Kenneth I., Harold G. Koenig, Nalini Tarakeshwar, and June Hahn. 2001. Religious Struggle as a Predictor of Mortality Among Medically Ill Elderly Patients: A 2-Year Longitudinal Study. Archives of Internal Medicine 161: 1881–85. [Google Scholar] [CrossRef] [PubMed]
- Park, Crystal L. 2010. Making sense of the meaning literature: An integrative review of meaning making and its effects on adjustment to stressful life events. Psychol Bull 136: 257–301. [Google Scholar] [CrossRef]
- Park, Crystal L., James E. Pustejovsky, Kelly Trevino, Allen C. Sherman, Craig Esposito, Mark Berendsen, and John M. Salsman. 2019. Effects of psychosocial interventions on meaning and purpose in adults with cancer: A systematic review and meta-analysis. Cancer 125: 2383–93. [Google Scholar] [CrossRef]
- Pennachio, John. 1992. Gnostic Inner Illumination and Carl Jung’s Individuation. Journal of Religion and Health 31: 237–45. Available online: http://www.jstor.org.ezproxy.elib11.ub.unimaas.nl/stable/27510698 (accessed on 30 November 2023). [CrossRef]
- Pinquart, Martin. 2002. Creating and Maintaining Purpose in Life in Old Age: A Meta-Analysis. Ageing International 27: 90–114. [Google Scholar] [CrossRef]
- Puchalski, Christina M., Robert Vitillo, Sharon K. Hull, and Nancy Reller. 2014. Improving the spiritual dimension of whole person care: Reaching national and international consensus. Journal of Palliative Medicine 17: 642–56. [Google Scholar] [CrossRef]
- Rayner, Mark, and Diego Vitali. 2016. Short-Term Existential Psychotherapy in Primary Care A Quantitative Report. The Journal of Humanistic Psychology 56: 357–72. [Google Scholar] [CrossRef]
- Reed, Pamela G. 1992. An emerging paradigm for the investigation of spirituality in nursing. Research in Nursing & Health 15: 349–57. [Google Scholar] [CrossRef]
- Schulenberg, Stefan E., Robert R. Hutzell, Carrie Nassif, and Julius M. Rogina. 2008. Logotherapy for clinical practice. Psychotherapy 45: 447–63. [Google Scholar] [CrossRef]
- Spek, Nadia van der, Vincent Willemsen, Kitty Knipscheer-Kuipers, Irma Verdonck-de Leeuw, William S. Breitbart, and Shannon R. Poppito, eds. 2017. Behandelprotocol Zingevingsgerichte Groepstherapie voor Mensen met Kanker: Handleiding voor Therapeuten. Houten: Bohn Stafleu Van Loghum. [Google Scholar]
- Thauvoye, Evalyne, Siebrecht Vanhooren, Anna Vandenhoeck, and Jessie Dezutter. 2018. Spirituality and Well-Being in Old Age: Exploring the Dimensions of Spirituality in Relation to Late-Life Functioning. Journal of Religion and Health 57: 2167–81. [Google Scholar] [CrossRef]
- Tomás, José Manuel, Patricia Sancho, Laura Galiana, and Amparp Oliver. 2016. A Double Test on the Importance of Spirituality, the “Forgotten Factor”, in Successful Aging. Social Indicators Research 127: 1377–89. [Google Scholar] [CrossRef]
- Visser, Anja, Bert Garssen, and Ad Vingerhoets. 2010. Spirituality and well-being in cancer patients: A review. Psycho-Oncology 19: 565–72. [Google Scholar] [CrossRef] [PubMed]
- Vos, Joël, Meghan Craig, and Mick Cooper. 2015. Existential therapies: A meta-analysis of their effects on psychological outcomes. Journal of Consulting and Clinical Psychology 83: 115–28. [Google Scholar] [CrossRef] [PubMed]
- Waterman, Alan S. 1993. Two Conceptions of Happiness: Contrasts of Personal Expressiveness (Eudaimonia) and Hedonic Enjoyment. Journal of Personality and Social Psychology 64: 678–91. [Google Scholar] [CrossRef]
- Westerhof, Gerben. J. 2019. Life review: Lifespan development, meaning processes, and interventions. In International Perspectives on Reminiscence, Life Review and Life Story Work. Edited by Faith Gibson. London: Jessica Kingsley. [Google Scholar]
- Westerhof, Gerben J., and Corey L. M. Keyes. 2010. Mental Illness and Mental Health: The Two Continua Model Across the Lifespan. Journal of Adult Development 17: 110–19. [Google Scholar] [CrossRef] [PubMed]
- White, Michael, and David Epston. 1990. Narrative Means to Therapeutic Ends. New York: W. W. Norton and Co. [Google Scholar]
- WHO. 2014. Mental Health: A State of Well-Being. Available online: https://www.who.int/mental_health/who_urges_investment/en/#:~:text=Mental%20health%20is%20defined%20as,to%20her%20or%20his%20community (accessed on 18 May 2014).
- Wong, Paul T. P. 2010. Meaning Therapy: An Integrative and Positive Existential Psychotherapy. Journal of Contemporary Psychotherapy 40: 85–93. [Google Scholar] [CrossRef]
- Yamada, Ann-Marie, David Lukoff, Caroline S. F. Lim, and Laura L. Mancuso. 2020. Integrating spirituality and mental health: Perspectives of adults receiving public mental health services in California. Psychology of Religion and Spirituality 12: 276–87. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Completers (n = 560) | Dropouts (n = 314) | Completers vs. Dropouts | |
|---|---|---|---|
| Age M (SD) | 48.4 (13.9) | 44.0 (14.7) | t(872) = 4.38 * |
| Gender: | |||
| Female (%) | 66.1 | 65.0 | χ2(1) = 0.11 |
| Male (%) | 33.9 | 35.0 | |
| Relation: | |||
| No (%) | 24.8 | 29.9 | χ2(1) = 2.7 |
| Yes (%) | 75.2 | 70.1 | |
| Paid job: | |||
| No (%) | 20.2 | 19.7 | χ2(1) = 0.02 |
| Yes (%) | 79.8 | 80.3 | |
| Education: | |||
| Professional (%) | 27.7 | 26.4 | χ2(1) = 0.16 |
| Scientific (%) | 72.3 | 73.6 | |
| Kids: | |||
| No (%) | 61.5 | 55.3 | χ2(1) = 3.2 |
| Yes (%) | 38.4 | 44.7 | |
| Spirituality T1 M (SD) | 102.2 (16.7) | 101.9 (15.5) | t(863) = 0.29 |
| Well-being T1 M (SD) | 44.1 (12) | 43.8 (11.6) | t(865) = 0.40 |
| Mental distress T1 M (SD) | 24 (18) | 24.1 (16.3) | t(791) = −0.06 |
| Spirituality T2 M (SD) a | 99.7 (16.9) | ||
| Well-being T2 M (SD) a | 44.8 (12.2) | ||
| Mental distress T2 M (SD) a | 23.1 (18.8) |
| Well- Being T1 | Spirituality T1 | Mental Distress T1 | Well Being T2 | Spirituality T2 | Mental Distress T2 | |
|---|---|---|---|---|---|---|
| Well-being T1 | 1 | 0.50 ** | −0.43 ** | 0.82 ** | 0.51 ** | −0.44 ** |
| Spirituality T1 | 1 | −0.23 ** | 0.46 ** | 0.86 ** | −0.23 ** | |
| Mental distress T1 | 1 | −0.47 ** | −0.23 ** | 0.83 ** | ||
| Well-being T2 | 1 | 0.50 ** | −0.54 ** | |||
| Spirituality T2 | 1 | −0.26 ** | ||||
| Mental distress T2 | 1 |
| Step 1 | Step 2 | Step 3 | Step 4 | |
|---|---|---|---|---|
| β | β | β | β | |
| R2 = 0.22 ** | R2 = 0.36 ** ΔR2 = 0.14 | R2 = 0.67 ** ΔR2 = 0.31 | R2 = 0.68 ** ΔR2 = 0.01 | |
| Gender 1 | 0.01 | −0.01 | 0.02 | 0.02 |
| Age | −0.05 | −0.10 * | −0.03 | −0.04 |
| Relation 2 | 0.01 | 0.02 | 0.00 | 0.00 |
| Paid job 3 | 0.10 * | 0.07 | 0.03 | 0.03 |
| Education 4 | −0.04 | 0.00 | 0.01 | 0.02 |
| Home living child 5 | −0.03 | −0.05 | −0.01 | −0.02 |
| Spirituality T1 | 0.48 ** | 0.39 ** | 0.04 | 0.04 |
| Mental distress T1 | −0.38 ** | −0.12 ** | ||
| Well-being T1 | 0.80 ** | 0.74 ** |
| Step 1 | Step 5 | |
|---|---|---|
| β | β | |
| R2 = 0.45 | R2 = 0.69 | |
| Gender 1 | −0.08 * | 0.00 |
| Age | −0.05 | −0.04 |
| Relation 2 | −0.03 | −0.00 |
| Paid job 3 | 0.00 | 0.01 |
| Education 4 | −0.01 | 0.03 |
| Home living child 5 | −0.03 | −0.02 |
| Mental distress T1 | −0.04 | |
| Well-being T1 | 0.69 ** | |
| 7 Subscales of the Spirituality Attitude and Interest List questionnaire (SAIL) | ||
| Meaningfulness | 0.44 ** | 0.11 * |
| Trust | 0.30 ** | 0.07 |
| Acceptance | −0.06 | 0.02 |
| Concern for others | 0.05 | 0.01 |
| Connectedness with nature | 0.03 | 0.01 |
| Transcendent experiences | 0.02 | −0.03 |
| Spiritual activities | −0.08 | −0.06 |
| Step 1 | Step 2 | Step 3 | Step 4 | |
|---|---|---|---|---|
| β | β | β | β | |
| R2 = 0.09 ** | R2 = 0.23 ** ΔR2 = 0.14 | R2 = 0.70 ** ΔR2 = 0.47 | R2 = 0.70 ** ΔR2 = 0.00 | |
| Gender 1 | −0.10 * | −0.11 ** | −0.02 ** | −0.02 |
| Age | −0.18 ** | −0.18 ** | −0.08 * | −0.08 ** |
| Relation 2 | 0.04 | 0.06 | 0.01 | 0.01 |
| Paid job 3 | −0.09 | −0.05 | −0.01 | −0.00 |
| Education 4 | 0.02 | 0.01 | 0.01 | 0.01 |
| Home living child 5 | −0.08 | −0.10 * | −0.05 | −0.06 * |
| Spirituality T1 | −0.20 ** | 0.03 | −0.01 | 0.03 |
| Well-being T1 | −0.44 ** | −0.09 ** | ||
| Mental distress T1 | 0.81 ** | 0.78 ** |
| Step 1 | Step 5 | |
|---|---|---|
| β | β | |
| R2 = 0.42 | R2 = 0.71 | |
| Gender 1 | 0.03 | 0.00 |
| Age | −0.16 ** | −0.09 * |
| Relation 2 | 0.07 | 0.02 |
| Paid job 3 | −0.01 | 0.00 |
| Education 4 | 0.00 | 0.01 |
| Home-living child 5 | −0.08 * | −0.06 * |
| Mental distress T1 | 0.71 ** | |
| Well-being T1 | −0.06 | |
| 7 Subscales of the Spirituality Attitude and Interest List questionnaire (SAIL) | ||
| Meaningfulness | −0.35 ** | −0.04 |
| Trust | −0.42 ** | −0.11 * |
| Acceptance | 0.09 * | 0.01 |
| Concern for others | 0.11 * | 0.02 |
| Connectedness with nature | 0.01 | 0.00 |
| Transcendent experiences | 0.22 ** | 0.08 * |
| Spiritual activities | 0.03 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huijs, T.; Braam, A.W.; Kruizinga, R.; Jacobs, N.; Reijnders, J.; Simons, M. Spirituality as a Predictor of Well-Being, Mental Distress or Both: A Four-Week Follow-Up Study in a Sample of Dutch and Belgian Adults. Religions 2024, 15, 179. https://doi.org/10.3390/rel15020179
Huijs T, Braam AW, Kruizinga R, Jacobs N, Reijnders J, Simons M. Spirituality as a Predictor of Well-Being, Mental Distress or Both: A Four-Week Follow-Up Study in a Sample of Dutch and Belgian Adults. Religions. 2024; 15(2):179. https://doi.org/10.3390/rel15020179
Chicago/Turabian StyleHuijs, Thijs, Arjan W. Braam, Renske Kruizinga, Nele Jacobs, Jennifer Reijnders, and Marianne Simons. 2024. "Spirituality as a Predictor of Well-Being, Mental Distress or Both: A Four-Week Follow-Up Study in a Sample of Dutch and Belgian Adults" Religions 15, no. 2: 179. https://doi.org/10.3390/rel15020179
APA StyleHuijs, T., Braam, A. W., Kruizinga, R., Jacobs, N., Reijnders, J., & Simons, M. (2024). Spirituality as a Predictor of Well-Being, Mental Distress or Both: A Four-Week Follow-Up Study in a Sample of Dutch and Belgian Adults. Religions, 15(2), 179. https://doi.org/10.3390/rel15020179