Low Galectin-3 Expression Level in Primary Tumors Is Associated with Metastasis in T1 Lung Adenocarcinoma


Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
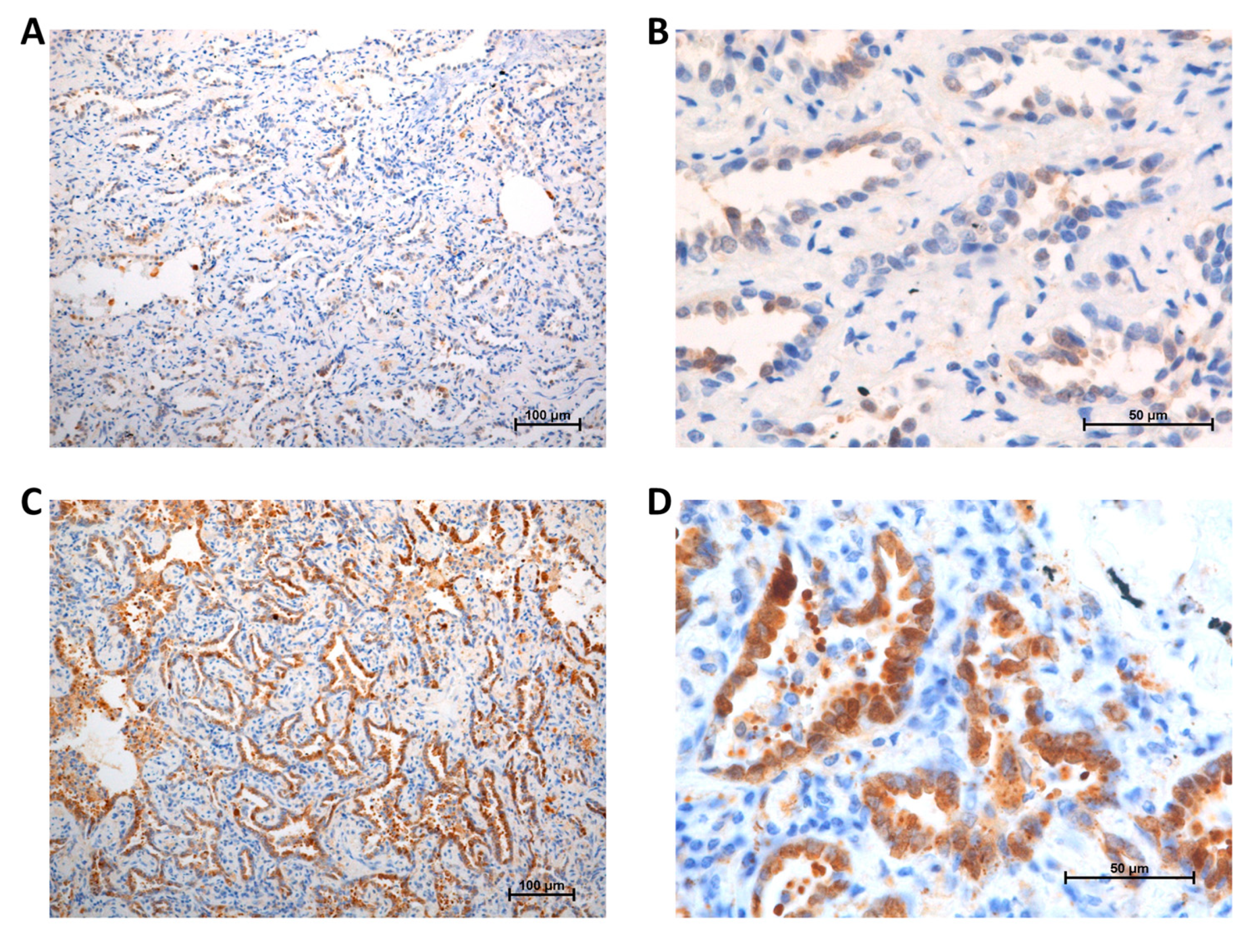
2.2. Immunohistochemical Staining
2.3. Scoring for Gal-3 Expression Level
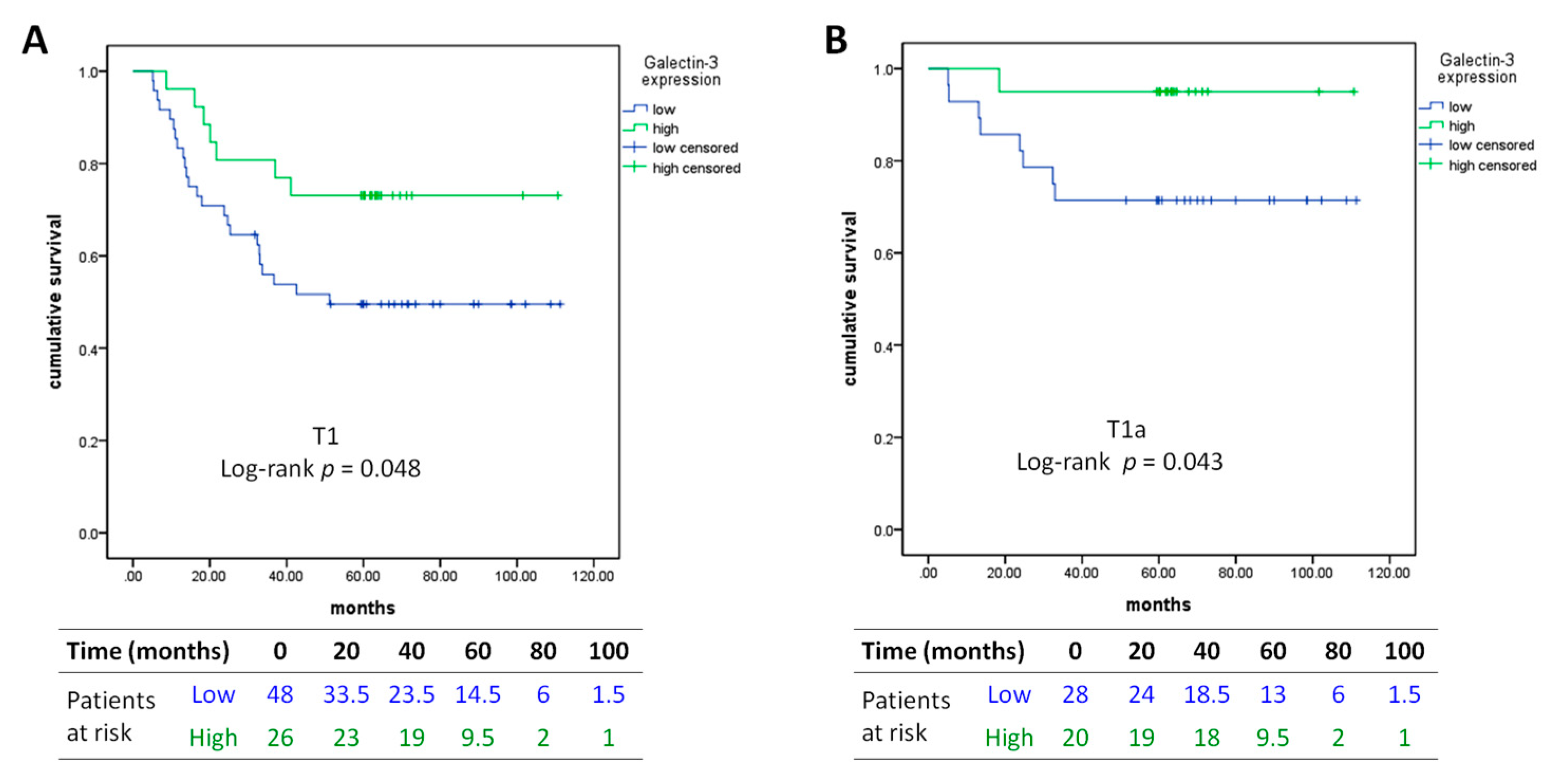
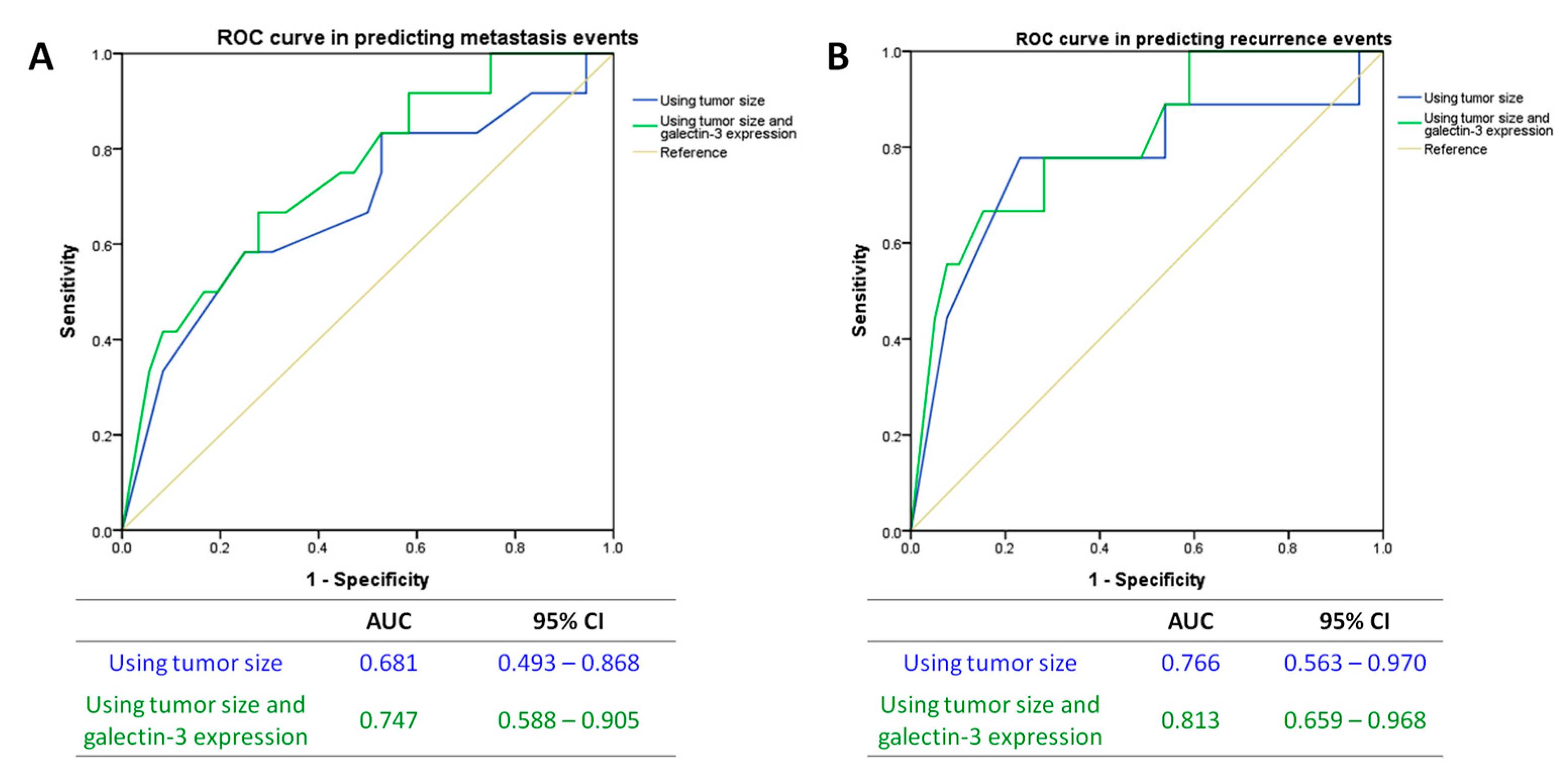
2.4. Data Collection and Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AJCC | American Joint Committee on Cancer |
| AUC | area under curve |
| DAB | 3,3′-diaminobenzidine tetrahydrochloride |
| Gal-3 | Galectin-3 |
| NSCLC | non-small cell lung cancer |
| OS | overall survival |
| RFS | recurrence-free survival |
| ROC | receiver operating characteristic |
| SEER | surveillance, epidemiology, and end results |
| Tregs | regulatory T cells |
References
- Yang, F.; Chen, H.; Xiang, J.; Zhang, Y.; Zhou, J.; Hu, H.; Zhang, J.; Luo, X. Relationship between tumor size and disease stage in non-small cell lung cancer. BMC Cancer 2010, 10, 1–6. [Google Scholar] [CrossRef]
- Ye, B.; Cheng, M.; Li, W.; Ge, X.X.; Geng, J.F.; Feng, J.; Yang, Y.; Hu, D.-Z. Predictive factors for lymph node metastasis in clinical stage IA lung adenocarcinoma. Ann. Thorac. Surg. 2014, 98, 217–223. [Google Scholar] [CrossRef]
- Yuan, P.; Cao, J.L.; Rustam, A.; Zhang, C.; Yuan, X.S.; Bao, F.C.; Lv, W.; Hu, J. Time-to-progression of NSCLC from early to advanced stages: An analysis of data from SEER registry and a single institute. Sci. Rep. 2016, 6, 6–9. [Google Scholar] [CrossRef]
- Ahmed, H.; AlSadek, D.M. Galectin-3 as a potential target to prevent cancer metastasis. Clin. Med. Insights. Oncol. 2015, 9, CMO.S29462-121. [Google Scholar] [CrossRef]
- Cardoso, A.C.; Andrade, L.N.; Bustos, S.O.; Chammas, R. Galectin-3 determines tumor cell adaptive strategies in stressed tumor microenvironments. Front. Oncol. 2016, 6, 127. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, A.H.; Alalawi, Z.; Mirandola, L.; Rakhshanda, R.; Dahlbeck, S.; Nguyen, D.; Jenkins, M.; Grizzi, F.; Cobos, E.; Figueroa, J.A. Galectins in cancer: Carcinogenesis, diagnosis and therapy. Ann. Transl. Med. 2014, 2, 88. [Google Scholar] [PubMed]
- Chang, W.A.; Tsai, M.J.; Kuo, P.L.; Hung, J.Y. Role of galectins in lung cancer. Oncol. Lett. 2017, 14, 5077–5084. [Google Scholar] [PubMed]
- Szoke, T.; Kayser, K.; Trojan, I.; Kayser, G.; Furak, J.; Tiszlavicz, L.; Baumhäkel, J.-D.; Gabius, H.-J. The role of microvascularization and growth/adhesion-regulatory lectins in the prognosis of non-small cell lung cancer in stage II. Eur. J. Cardiothorac. Surg. 2007, 31, 783–787. [Google Scholar] [CrossRef] [PubMed]
- Puglisi, F.; Minisini, A.M.; Barbone, F.; Intersimone, D.; Aprile, G.; Puppin, C.; Damanted, G.; Parond, I.; Telle, G.; Piga, A. Galectin-3 expression in non-small cell lung carcinoma. Cancer Lett. 2004, 212, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, A.; Saal, I.; Vuckovic, A.; Ransy, V.; Vereerstraten, P.; Kaltner, H.; Gabius, H.-J.; Kiss, R.; Decaestecker, C.; Salmon, I.; et al. Nuclear galectin-3 expression is an independent predictive factor of recurrence for adenocarcinoma and squamous cell carcinoma of the lung. Mod. Pathol. 2005, 18, 1264–1271. [Google Scholar] [CrossRef]
- Kataoka, Y.; Igarashi, T.; Ohshio, Y.; Fujita, T.; Hanaoka, J. Predictive importance of galectin-3 for recurrence of non-small cell lung cancer. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Martini, N.; Melamed, M.R. Multiple primary lung cancers. J. Thorac. Cardiovasc. Surg. 1975, 70, 606–612. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, J.; Li, L.; Yin, G.; Zhang, J.; Zheng, S.; Cheung, H.; Wu, N.; Lu, N.; Mao, X.; et al. Genomic heterogeneity of multiple synchronous lung cancer. Nat. Commun. 2016, 7, 13200. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Crowley, J.; Chansky, K.; Giroux, D.J.; Groome, P.A.; Rami-Porta, R.; Postmus, P.E.; Rusch, V.W.; Sobin, L. The IASLC lung cancer staging project: Proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J. Thorac. Oncol. 2007, 2, 706–714. [Google Scholar] [CrossRef]
- Sica, G.; Yoshizawa, A.; Sima, C.S.; Azzoli, C.G.; Downey, R.J.; Rusch, V.W.; Travis, W.D.; Moreira, A.L. A grading system of lung adenocarcinomas based on histologic pattern is predictive of disease recurrence in stage I tumors. Am. J. Surg. Pathol. 2010, 34, 1155–1162. [Google Scholar] [CrossRef]
- Lee, H.Y.; Jeong, J.Y.; Lee, K.S.; Kim, H.J.; Han, J.; Kim, B.T.; Kim, J.; Shim, Y.M.; Kim, J.-H. Solitary pulmonary nodular lung adenocarcinoma: Correlation of histopathologic scoring and patient survival with imaging biomarkers. Radiology 2012, 264, 884–893. [Google Scholar] [CrossRef]
- Farhad, M.; Rolig, A.S.; Redmond, W.L. The role of Galectin-3 in modulating tumor growth and immunosuppression within the tumor microenvironment. Oncoimmunology 2018, 7, e1434467. [Google Scholar] [CrossRef]
- Califice, S.; Castronovo, V.; Bracke, M.; Van den Brule, F. Dual activities of galectin-3 in human prostate cancer: Tumor suppression of nuclear galectin-3 vs tumor promotion of cytoplasmic galectin-3. Oncogene 2004, 23, 7527–7536. [Google Scholar] [CrossRef]
- Van den Brule, F.A.; Waltregny, D.; Liu, F.T.; Castronovo, V. Alteration of the cytoplasmic/nuclear expression pattern of galectin-3 correlates with prostate carcinoma progression. Int. J. Cancer. 2000, 89, 361–367. [Google Scholar] [CrossRef]
- Braeuer, R.R.; Zigler, M.; Kamiya, T.; Dobroff, A.S.; Huang, L.; Choi, W.; McConkey, D.J.; Shoshan, E.; Mobley, A.K.; Song, R.; et al. Galectin-3 contributes to melanoma growth and metastasis via regulation of NFAT1 and autotaxin. Cancer Res. 2012, 72, 5757–5766. [Google Scholar] [CrossRef]
- Hayashi, Y.; Jia, W.; Kidoya, H.; Muramatsu, F.; Tsukada, Y.; Takakura, N. Galectin-3 inhibits cancer metastasis by negatively regulating integrin beta3 expression. Am. J. Pathol. 2019, 189, 900–910. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.H.; Lee, H.W.; Han, J.H.; Kang, S.Y.; Choi, J.H.; Jung, Y.M.; Choi, H.; Oh, Y.T.; Park, K.J.; Hwang, S.; et al. Low expression of Bax predicts poor prognosis in resected non-small cell lung cancer patients with non-squamous histology. Jpn. J. Clin. Oncol. 2008, 38, 661–669. [Google Scholar] [CrossRef]
- Buttery, R.; Monaghan, H.; Salter, D.M.; Sethi, T. Galectin-3: Differential expression between small-cell and non-small-cell lung cancer. Histopathology 2004, 44, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Alfoldi, R.; Balog, J.A.; Farago, N.; Halmai, M.; Kotogany, E.; Neuperger, P.; Nagy, L.I.; Fehér, L.Z.; Szebeni, G.J.; Puskás, L.G. Single cell mass cytometry of non-small cell lung cancer cells reveals complexity of in vivo and three-dimensional models over the petri-dish. Cells 2019, 8, 1903. [Google Scholar] [CrossRef] [PubMed]
- Castronovo, V.; Van Den Brule, F.A.; Jackers, P.; Clausse, N.; Liu, F.T.; Gillet, C.; Sobel, M.E. Decreased expression of galectin-3 is associated with progression of human breast cancer. J. Pathol. 1996, 179, 43–48. [Google Scholar] [CrossRef]
- Abraham, E.K.; George, P.S.; Nimi, G.K.; Sujathan, K.; Somanathan, T.; Remani, P. Down regulation of galectin-3 in primary tumor tissues of breast predict axillary lymph node metastasis. J. Cancer Res. Exp. Oncol. 2011, 3, 37–49. [Google Scholar]
- Kosacka, M.; Piesiak, P.; Kowal, A.; Golecki, M.; Jankowska, R. Galectin-3 and cyclin D1 expression in non-small cell lung cancer. J Exp Clin Cancer Res. 2011, 30, 1–17. [Google Scholar] [CrossRef]
- Carvalho, R.S.; Fernandes, V.C.; Nepomuceno, T.C.; Rodrigues, D.C.; Woods, N.T.; Suarez-Kurtz, G.; Chammas, R.; Monteiro, A.N.A.; Carvalho, M.A. Characterization of LGALS3 (galectin-3) as a player in DNA damage response. Cancer Biol. Ther. 2014, 15, 840–850. [Google Scholar] [CrossRef]
- Sano, H.; Hsu, D.K.; Yu, L.; Apgar, J.R.; Kuwabara, I.; Yamanaka, T.; Hirashima, M.; Liu, F.-T. Human galectin-3 is a novel chemoattractant for monocytes and macrophages. J. Immunol. 2000, 165, 2156–2164. [Google Scholar] [CrossRef]
- Sano, H.; Hsu, D.K.; Apgar, J.R.; Yu, L.; Sharma, B.B.; Kuwabara, I.; Izui, S.; Liu, F.-T. Critical role of galectin-3 in phagocytosis by macrophages. J. Clin. Invest. 2003, 112, 389–397. [Google Scholar] [CrossRef]
- Nieminen, J.; St-Pierre, C.; Sato, S. Galectin-3 interacts with naive and primed neutrophils, inducing innate immune responses. J. Leukoc. Biol. 2005, 78, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Bernardes, E.S.; Silva, N.M.; Ruas, L.P.; Mineo, J.R.; Loyola, A.M.; Hsu, D.K.; Liu, F.-T.; Chammas, R.; Roque-Barreira, M.C. Toxoplasma gondii infection reveals a novel regulatory role for galectin-3 in the interface of innate and adaptive immunity. Am. J. Pathol. 2006, 168, 1910–1920. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.B.; Yoon, H.J.; Chang, C.Y.; Koh, H.S.; Jeon, S.H.; Park, E.J. Galectin-3 exerts cytokine-like regulatory actions through the JAK-STAT pathway. J. Immunol. 2010, 185, 7037–7046. [Google Scholar] [CrossRef]
- Breuilh, L.; Vanhoutte, F.; Fontaine, J.; Van Stijn, C.M.; Tillie-Leblond, I.; Capron, M.; Faveeuw, C.; Jouault, T.; Van Die, I.; Gosset, P.; et al. Galectin-3 modulates immune and inflammatory responses during helminthic infection: Impact of galectin-3 deficiency on the functions of dendritic cells. Infect. Immun. 2007, 75, 5148–5157. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.R.; Al Rasebi, Z.; Mensah-Brown, E.; Shahin, A.; Xu, D.; Goodyear, C.S.; Fukada, S.Y.; Liu, F.-T.; Liew, F.Y.; Lukic, M.L. Galectin-3 deficiency reduces the severity of experimental autoimmune encephalomyelitis. J. Immunol. 2009, 182, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Blidner, A.G.; Mendez-Huergo, S.P.; Cagnoni, A.J.; Rabinovich, G.A. Re-wiring regulatory cell networks in immunity by galectin-glycan interactions. FEBS Lett. 2015, 589, 3407–3418. [Google Scholar] [CrossRef]
- Hayes, D.F. Biomarker validation and testing. Mol. Oncol. 2015, 9, 960–966. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Galectin-3 Expression | Low n = 48 | High n = 26 | p-Value |
|---|---|---|---|
| Age (Year) | 63 (55–70) | 62.5 (57.5–69.5) | 0.738 |
| Gender, Female | 26 (54.2) | 20 (76.9) | 0.079 |
| T Stage * | 0.132 | ||
| T1a (≤ 2 cm) | 28 (58.3) | 20 (76.9) | |
| T1b (2–3 cm) | 20 (41.7) | 6 (23.1) | |
| Subtype Score | 4 (3–7.5) | 4 (3–4) | 0.924 |
| Lymphovascular Invasion | 9 (18.8) | 2 (7.7) | 0.309 |
| Outcomes | |||
| Metastasis, All Kinds | 28 (58.3) | 8 (30.8) | 0.03 |
| Metastasis, Nodal | 15 (31.3) | 5 (19.2) | 0.411 |
| Metastasis, Distant | 25 (52.1) | 5 (19.2) | 0.007 |
| Recurrence | 24 (50) | 7 (26.7) | 0.084 |
| Mortality | 14 (29.2) | 2 (7.7) | 0.04 |
| Univariable Analysis | Overall Survival | Recurrence-Free Survival | ||||
| Variables | Hazard Ratio | 95% Confidence Interval | p-Value | Hazard Ratio | 95% Confidence Interval | p-Value |
| Age (Year) | 1.036 | 0.986–1.089 | 0.159 | 1.002 | 0.970–1.035 | 0.91 |
| Gender (Male vs. Female) | 8.473 | 2.412–29.765 | 0.001 | 3.201 | 1.562–6.562 | 0.001 |
| T Stage (T1b vs. T1a) * | 6.229 | 2.123–18.275 | 0.001 | 7.822 | 3.542–17.274 | <0.0001 |
| Subtype Score | 1.897 | 1.234–2.917 | 0.004 | 1.478 | 1.063–2.054 | 0.02 |
| Lymphovascular Invasion (Yes vs. No) | 17.162 | 5.778–50.972 | <0.0001 | 3.476 | 1.533–7.884 | 0.003 |
| Galectin-3 (High vs. Low) | 0.254 | 0.057–1.122 | 0.071 | 0.441 | 0.2–0.97 | 0.042 |
| Multivariable Analysis | Overall Survival | Recurrence-Free Survival | ||||
| Variables | Hazard Ratio | 95% Confidence Interval | p-Value | Hazard Ratio | 95% Confidence Interval | p-Value |
| Gender (Male vs. Female) | 2.563 | 0.608–10.798 | 0.200 | 2.346 | 1.034–5.324 | 0.041 |
| T Stage (T1b vs. T1a) * | 2.641 | 0.719–9.704 | 0.143 | 6.884 | 2.735–17.324 | <0.0001 |
| Subtype Score | 1.845 | 1.052–3.233 | 0.032 | 0.888 | 0.581–1.357 | 0.583 |
| Lymphovascular Invasion (Yes vs. No) | 23.934 | 4.882–117.344 | <0.0001 | 1.493 | 0.608–3.664 | 0.382 |
| Galectin-3 (High vs. Low) | 0.193 | 0.038–0.975 | 0.047 | 0.794 | 0.330–1.908 | 0.606 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kao, M.-W.; Su, Y.-C.; Liang, P.-I.; Wu, Y.-Y.; Hong, T.-M. Low Galectin-3 Expression Level in Primary Tumors Is Associated with Metastasis in T1 Lung Adenocarcinoma. J. Clin. Med. 2020, 9, 1990. https://doi.org/10.3390/jcm9061990
Kao M-W, Su Y-C, Liang P-I, Wu Y-Y, Hong T-M. Low Galectin-3 Expression Level in Primary Tumors Is Associated with Metastasis in T1 Lung Adenocarcinoma. Journal of Clinical Medicine. 2020; 9(6):1990. https://doi.org/10.3390/jcm9061990
Chicago/Turabian StyleKao, Ming-Wei, Yue-Chiu Su, Peir-In Liang, Yi-Ying Wu, and Tse-Ming Hong. 2020. "Low Galectin-3 Expression Level in Primary Tumors Is Associated with Metastasis in T1 Lung Adenocarcinoma" Journal of Clinical Medicine 9, no. 6: 1990. https://doi.org/10.3390/jcm9061990
APA StyleKao, M.-W., Su, Y.-C., Liang, P.-I., Wu, Y.-Y., & Hong, T.-M. (2020). Low Galectin-3 Expression Level in Primary Tumors Is Associated with Metastasis in T1 Lung Adenocarcinoma. Journal of Clinical Medicine, 9(6), 1990. https://doi.org/10.3390/jcm9061990