Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Experimental Section
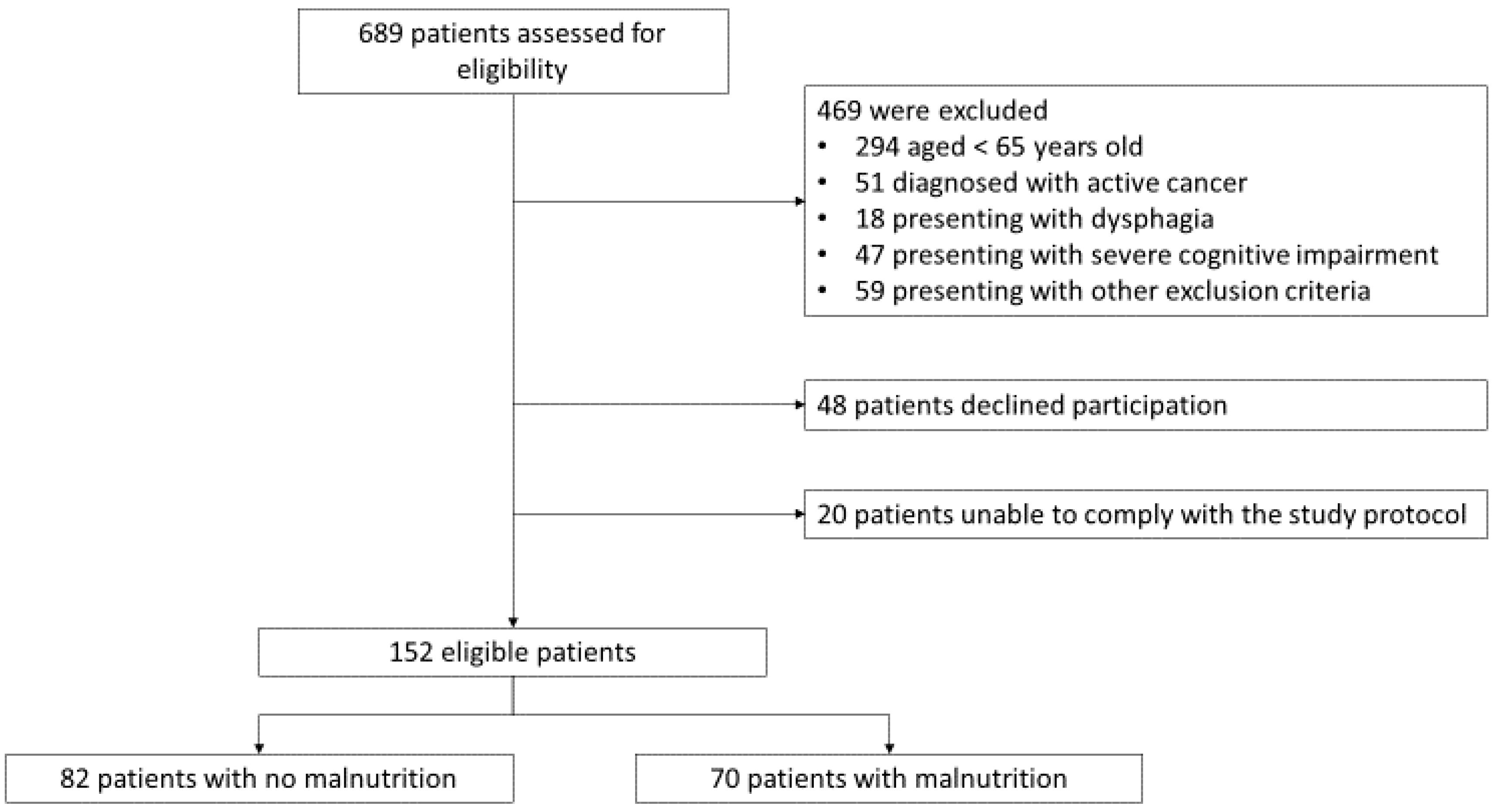
2.1. Study Design and Participants
2.2. Biochemical Analysis, Anthropometric Measurements and Body Composition Evaluation
2.3. Tools for Screening of Nutritional Status
2.4. Diagnostic Criteria for Malnutrition and Sarcopenia
2.5. Statistical Analysis
3. Results
3.1. Patients Characteristics
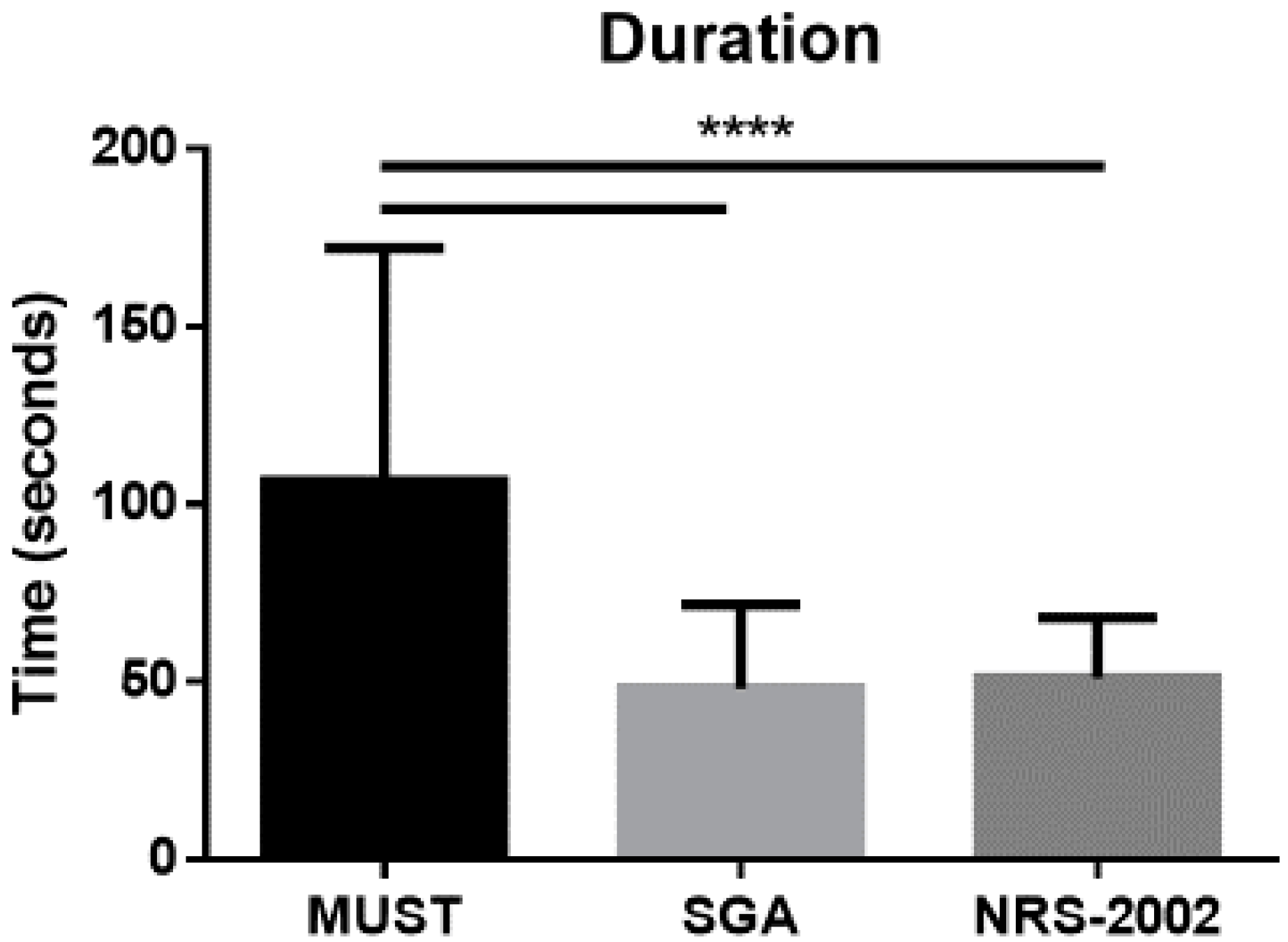
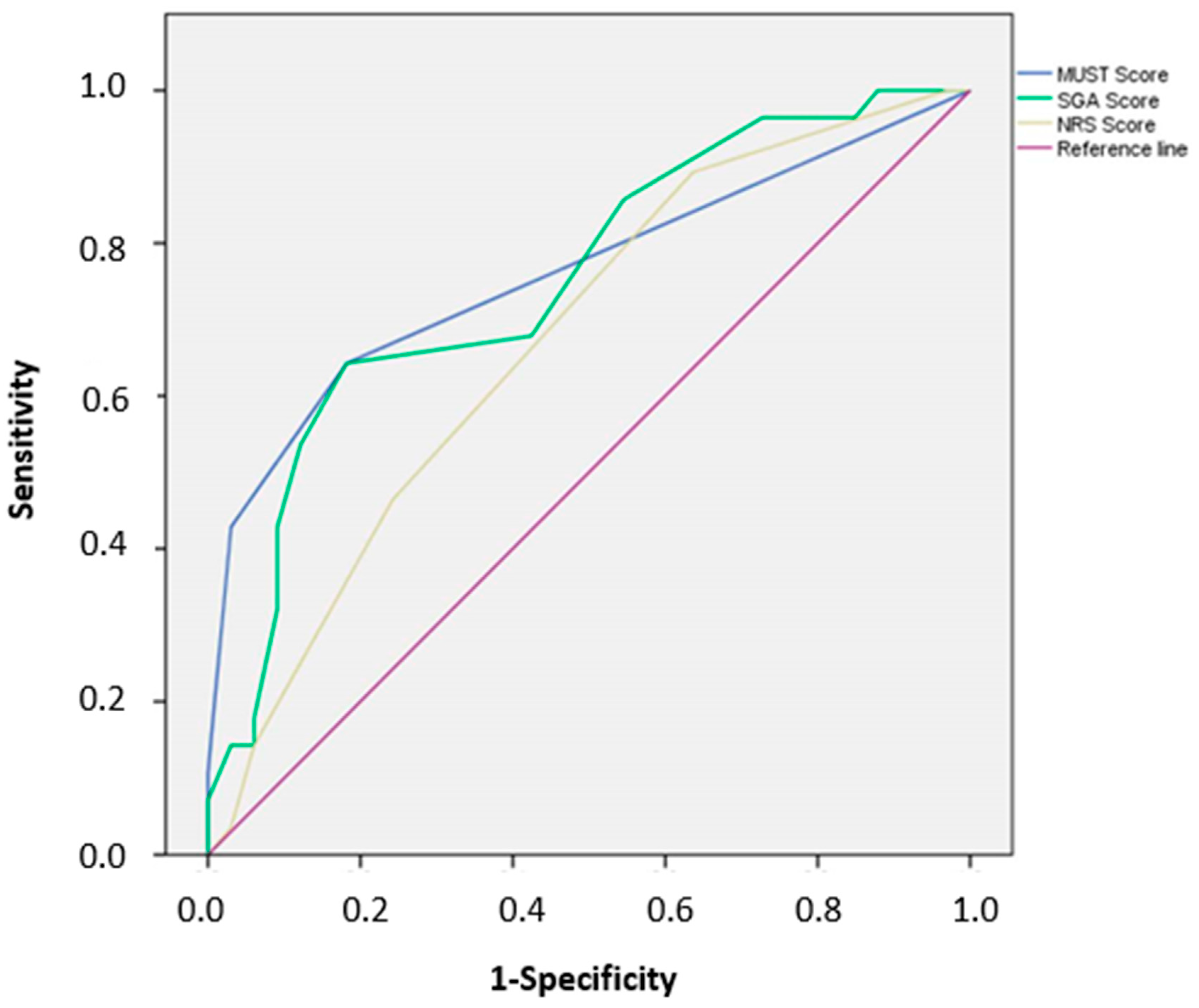
3.2. Rapidity, Sensitivity, Specificity, Accuracy, and Diagnostic Value of Nutritional Screening Tools
3.3. Malnutrition and Sarcopenia
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wittenberg, R.; Sharpin, L.; McCormick, B.; Hurst, J. The ageing society and emergency hospital admissions. Health Policy 2017, 121, 923–928. [Google Scholar] [CrossRef]
- Lim, S.L.; Ong, K.C.; Chan, Y.H.; Loke, W.C.; Ferguson, M.; Daniels, L. Malnutrition and its impact on cost of hospitalization, length of stay, readmission and 3-year mortality. Clin. Nutr. 2012, 31, 345–350. [Google Scholar] [CrossRef]
- Ruiz, A.J.; Buitrago, G.; Rodriguez, N.; Gomez, G.; Sulo, S.; Gomez, C.; Partridge, J.; Misas, J.; Dennis, R.; Alba, M.J.; et al. Clinical and economic outcomes associated with malnutrition in hospitalized patients. Clin. Nutr. 2019, 38, 1310–1316. [Google Scholar] [CrossRef]
- Bellanti, F.; Buglio, A.L.; De Stasio, E.; di Bello, G.; Tamborra, R.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Vendemiale, G. An open-label, single-center pilot study to test the effects of an amino acid mixture in older patients admitted to internal medicine wards. Nutrition 2020, 69, 110588. [Google Scholar] [CrossRef]
- Beaudart, C.; Sanchez-Rodriguez, D.; Locquet, M.; Reginster, J.Y.; Lengele, L.; Bruyere, O. Malnutrition as a Strong Predictor of the Onset of Sarcopenia. Nutrients 2019, 11, 2883. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Zhang, L.; Wang, H.; Hao, Q.; Dong, B.; Yang, M. Malnutrition-sarcopenia syndrome predicts mortality in hospitalized older patients. Sci. Rep. 2017, 7, 3171. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Hoogendijk, E.O.; Visvanathan, R.; Wright, O.R.L. Malnutrition Screening and Assessment in Hospitalised Older People: A Review. J. Nutr. Health Aging 2019, 23, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef]
- Power, L.; Mullally, D.; Gibney, E.R.; Clarke, M.; Visser, M.; Volkert, D.; Bardon, L.; de van der Schueren, M.A.E.; Corish, C.A. A review of the validity of malnutrition screening tools used in older adults in community and healthcare settings—A MaNuEL study. Clin. Nutr. ESPEN 2018, 24, 1–13. [Google Scholar] [CrossRef]
- Campbell, S.E.; Avenell, A.; Walker, A.E. Assessment of nutritional status in hospital in-patients. QJM 2002, 95, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Frank, M.; Sivagnanaratnam, A.; Bernstein, J. Nutritional assessment in elderly care: A MUST! BMJ Qual. Improv. Rep. 2015, 4, u204810.w2031. [Google Scholar] [CrossRef]
- Guigoz, Y. The Mini Nutritional Assessment (MNA) review of the literature--What does it tell us? J. Nutr. Health Aging 2006, 10, 466–485. [Google Scholar] [PubMed]
- Cereda, E. Mini nutritional assessment. Curr. Opin. Clin. Nutr. Metab Care 2012, 15, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Ghazi, L.; Fereshtehnejad, S.M.; Abbasi, F.S.; Sadeghi, M.; Shahidi, G.A.; Lokk, J. Mini Nutritional Assessment (MNA) is Rather a Reliable and Valid Instrument to Assess Nutritional Status in Iranian Healthy Adults and Elderly with a Chronic Disease. Ecol. Food Nutr. 2015, 54, 342–357. [Google Scholar] [CrossRef]
- Vellas, B.; Villars, H.; Abellan, G.; Soto, M.E.; Rolland, Y.; Guigoz, Y.; Morley, J.E.; Chumlea, W.; Salva, A.; Rubenstein, L.Z.; et al. Overview of the MNA--Its history and challenges. J. Nutr. Health Aging 2006, 10, 456–463. [Google Scholar] [PubMed]
- Juby, A.G.; Mager, D.R. A review of nutrition screening tools used to assess the malnutrition-sarcopenia syndrome (MSS) in the older adult. Clin. Nutr. ESPEN 2019, 32, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Buglio, A.L.; Bellanti, F.; Capurso, C.; Paglia, A.; Vendemiale, G. Adherence to Mediterranean Diet, Malnutrition, Length of Stay and Mortality in Elderly Patients Hospitalized in Internal Medicine Wards. Nutrients 2019, 11, 790. [Google Scholar] [CrossRef]
- Scafoglieri, A.; Clarys, J.P.; Bauer, J.M.; Verlaan, S.; Van, M.L.; Vantieghem, S.; Cederholm, T.; Sieber, C.C.; Mets, T.; Bautmans, I. Predicting appendicular lean and fat mass with bioelectrical impedance analysis in older adults with physical function decline—The PROVIDE study. Clin. Nutr. 2017, 36, 869–875. [Google Scholar] [CrossRef]
- Elia, M. Screening for Malnutrition: A Multidisciplinary Responsibility. Development and Use of the Malnutrition Universal Screening Tool (‘MUST’) for Adults; BAPEN: Redditch, UK, 2003. [Google Scholar]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? JPEN J. Parenter. Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Kossovsky, M.P.; Karsegard, V.L.; Pichard, C. Comparison of tools for nutritional assessment and screening at hospital admission: A population study. Clin. Nutr. 2006, 25, 409–417. [Google Scholar] [CrossRef]
- Ye, X.J.; Ji, Y.B.; Ma, B.W.; Huang, D.D.; Chen, W.Z.; Pan, Z.Y.; Shen, X.; Zhuang, C.L.; Yu, Z. Comparison of three common nutritional screening tools with the new European Society for Clinical Nutrition and Metabolism (ESPEN) criteria for malnutrition among patients with geriatric gastrointestinal cancer: A prospective study in China. BMJ Open 2018, 8, e019750. [Google Scholar] [CrossRef]
- Allard, J.P.; Keller, H.; Gramlich, L.; Jeejeebhoy, K.N.; Laporte, M.; Duerksen, D.R. GLIM criteria has fair sensitivity and specificity for diagnosing malnutrition when using SGA as comparator. Clin. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, M.; Atilla, F.D.; Sahin, F.; Saydam, G. The effect of malnutrition on mortality in hospitalized patients with hematologic malignancy. Supportive Care Cancer 2020, 28, 1441–1448. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Iwai, K.; Namikawa, N.; Matsuda, S.; Wakano, C.; Heya, H.; Yamanaka, M. The relationship between existing nutritional indicators and Global Leadership Initiative on Malnutrition (GLIM) criteria: A one-institution cross-sectional analysis. Clin. Nutr. 2020. [Google Scholar] [CrossRef]
- Rattanachaiwong, S.; Zribi, B.; Kagan, I.; Theilla, M.; Heching, M.; Singer, P. Comparison of nutritional screening and diagnostic tools in diagnosis of severe malnutrition in critically ill patients. Clin. Nutr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.M.; Kaiser, M.J.; Sieber, C.C. Evaluation of nutritional status in older persons: Nutritional screening and assessment. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 8–13. [Google Scholar] [CrossRef]
- Reber, E.; Gomes, F.; Vasiloglou, M.F.; Schuetz, P.; Stanga, Z. Nutritional Risk Screening and Assessment. J. Clin. Med. 2019, 8, 1065. [Google Scholar] [CrossRef]
- Weekes, C.E.; Elia, M.; Emery, P.W. The development, validation and reliability of a nutrition screening tool based on the recommendations of the British Association for Parenteral and Enteral Nutrition (BAPEN). Clin. Nutr. 2004, 23, 1104–1112. [Google Scholar]
- Diekmann, R.; Winning, K.; Uter, W.; Kaiser, M.J.; Sieber, C.C.; Volkert, D.; Bauer, J.M. Screening for malnutrition among nursing home residents—A comparative analysis of the mini nutritional assessment, the nutritional risk screening, and the malnutrition universal screening tool. J. Nutr. Health Aging 2013, 17, 326–331. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | No Malnutrition n = 82 (54%) | Malnutrition n = 70 (46%) | p |
|---|---|---|---|
| Age (years) | 77.8 ± 7.8 | 78.7 ± 7.3 | 0.4664 |
| Genre M/F (n, %) | 47/35 (57/43) | 40/30 (57/43) | 0.9827 |
| Education (n, %) | |||
| None | 0 (0) | 0 (0) | 0.8812 |
| Primary School | 45 (55) | 40 (57) | |
| Secondary School | 17 (21) | 17 (24) | |
| High School | 17 (21) | 10 (14) | |
| University | 3 (3) | 3 (5) | |
| Co-morbidities > 3 (n, %) | 37 (45) | 32 (46) | 0.9417 |
| MMSE score | 21.4 ± 6.6 | 19.9 ± 5.8 | 0.1420 |
| Weight (kg) | 76.7 ± 14.2 | 71.8 ± 16.0 | 0.0473 |
| Height (m) | 1.63 ± 0.1 | 1.62 ± 0.08 | 0.5021 |
| BMI (kg/m2) | 28.9 ± 5.9 | 27.4 ± 5.5 | 0.1091 |
| Arm circumference (cm) | 28.6 ± 4.0 | 27.2 ± 4.4 | 0.0417 |
| Waist circumference (cm) | 104.2 ± 10.7 | 99.7 ± 13.0 | 0.0206 |
| Hip circumference (cm) | 100.6 ± 10.5 | 99.2 ± 11.6 | 0.4159 |
| Waist-to-Hip ratio | 1.04 ± 0.11 | 1.00 ± 0.08 | 0.0126 |
| Tricipital skinfold thickness (cm) | 13.2 ± 4.7 | 12.6 ± 5.4 | 0.4651 |
| Bicipital skinfold thickness (cm) | 11.5 ± 4.6 | 9.8 ± 5.7 | 0.0437 |
| Subscapular skinfold thickness (cm) | 16.5 ± 6.2 | 14.0 ± 5.2 | 0.0085 |
| Supra-iliac skinfold thickness (cm) | 18.4 ± 7.0 | 13.7 ± 5.2 | <0.0001 |
| Total proteins (g/dL) | 6.4 ± 0.6 | 6.0 ± 0.8 | 0.0006 |
| Albumin (g/dL) | 3.3 ± 0.5 | 3.1 ± 0.6 | 0.0265 |
| Total Cholesterol (mg/dL) | 147 ± 36 | 116 ± 52 | <0.0001 |
| Lymphocytes (n × 103/mm3) | 1.9 ± 2.5 | 2.6 ± 3.9 | 0.1837 |
| Hemoglobin (g/dL) | 11.8 ± 2.9 | 9.6 ± 1.9 | <0.0001 |
| Iron (mg/dL) | 53.4 ± 32.7 | 47.3 ± 36.0 | 0.0839 |
| Parameter | No Malnutrition n = 82 (54%) | Malnutrition n = 70 (46%) | p |
|---|---|---|---|
| Body Cell Mass (kg) | 18.8 ± 6.6 | 10.4 ± 9.2 | <0.0001 |
| Total Body Water (L) | 37.5 ± 5.5 | 41.2 ± 9.4 | 0.003 |
| Extracellular water (L) | 22.4 ± 3.9 | 28.9 ± 10.1 | <0.0001 |
| Fat-Free Mass (%) | 63.2 ± 9.4 | 58.2 ± 11.4 | 0.0035 |
| Fat Mass (%) | 36.8 ± 9.4 | 41.8 ± 11.4 | 0.0035 |
| Skeletal Muscle Index | 8.2 ± 1.3 | 7.3 ± 1.9 | 0.0007 |
| Appendicular Skeletal Muscle Mass (kg) | 19.4 ± 3.7 | 16.5 ± 4.4 | <0.0001 |
| Appendicular Skeletal Muscle Mass (kg/m2) | 7.32 ± 2.6 | 6.30 ± 2.0 | 0.0083 |
| MUST | SGA | NRS-2002 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| GLIM | Low Risk | Medium/High Risk | Total | Well Nourished | Moderately/Severely Malnourished | Total | Low Risk | Medium/High Risk | Total |
| Well nourished | 67 | 15 | 82 | 12 | 70 | 82 | 62 | 20 | 82 |
| Malnutrition | 25 | 45 | 70 | 3 | 67 | 70 | 37 | 33 | 70 |
| Total | 92 | 60 | 152 | 15 | 137 | 152 | 99 | 53 | 152 |
| % | 95% CI | % | 95% CI | % | 95% CI | ||||
| Sensitivity | 64.3 | 51.9–75.4 | 95.7 | 88.0–99.1 | 47.1 | 35.1–59.4 | |||
| Specificity | 81.7 | 71.6–89.3 | 14.6 | 7.8–24.1 | 75.6 | 64.9–84.4 | |||
| Positive predictive value | 75.0 | 62.1–85.3 | 48.9 | 40.3–57.6 | 62.3 | 47.9–75.2 | |||
| Negative predictive value | 72.8 | 62.5 81.6 | 80.0 | 51.9–95.7 | 62.6 | 52.3–72.1 | |||
| Accuracy | 73.7 | 66.7–80.7 | 52.0 | 44.1–59.9 | 62.5 | 54.8–70.2 | |||
| к | 0.89 | 0.53 | 0.62 | ||||||
| Tool | Outcome | No Sarcopenia n (%) | Sarcopenia n (%) | OR (95% CI) | p |
|---|---|---|---|---|---|
| GLIM | No malnutrition | 50 (61.0) | 32 (39.0) | 1 | |
| Malnutrition | 25 (35.7) | 45 (64.3) | 2.7 (1.4–4.9) | 0.0029 | |
| MUST | Low risk | 60 (65.2) | 32 (34.8) | 1 | |
| Medium risk | 8 (34.8) | 15 (65.2) | 0.6 (0.3–1.2) | 0.459 | |
| High risk | 7 (18.9) | 30 (81.1) | 2.5 (1.3–3.6) | 0.0068 | |
| SGA | Well nourished | 9 (60.0) | 6 (40.0) | 1 | |
| Moderately malnourished | 44 (51.8) | 41 (48.2) | 1.4 (0.3–4.1) | 0.516 | |
| Severely malnourished | 22 (42.3) | 30 (57.7) | 2.7 (0.2–9.4) | 0.414 | |
| NRS-2002 | Low risk | 53 (53.5) | 46 (46.5) | 1 | |
| Medium risk | 12 (57.1) | 9 (42.9) | 0.1 (0.0–1.1) | 0.059 | |
| High risk | 16 (47.0) | 18 (53.0) | 1.2 (0.2–5.8) | 0.835 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellanti, F.; Lo Buglio, A.; Quiete, S.; Pellegrino, G.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Vendemiale, G. Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients. J. Clin. Med. 2020, 9, 1898. https://doi.org/10.3390/jcm9061898
Bellanti F, Lo Buglio A, Quiete S, Pellegrino G, Dobrakowski M, Kasperczyk A, Kasperczyk S, Vendemiale G. Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients. Journal of Clinical Medicine. 2020; 9(6):1898. https://doi.org/10.3390/jcm9061898
Chicago/Turabian StyleBellanti, Francesco, Aurelio Lo Buglio, Stefano Quiete, Giuseppe Pellegrino, Michał Dobrakowski, Aleksandra Kasperczyk, Sławomir Kasperczyk, and Gianluigi Vendemiale. 2020. "Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients" Journal of Clinical Medicine 9, no. 6: 1898. https://doi.org/10.3390/jcm9061898
APA StyleBellanti, F., Lo Buglio, A., Quiete, S., Pellegrino, G., Dobrakowski, M., Kasperczyk, A., Kasperczyk, S., & Vendemiale, G. (2020). Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients. Journal of Clinical Medicine, 9(6), 1898. https://doi.org/10.3390/jcm9061898