Herbal Medicines (Danggui Liuhuang Decoctions) for Management of Menopausal Symptoms: A Systematic Review of Randomized Controlled Trials




Abstract
1. Introduction
2. Methods
2.1. Study Registration and Protocol Information
2.2. Data Source
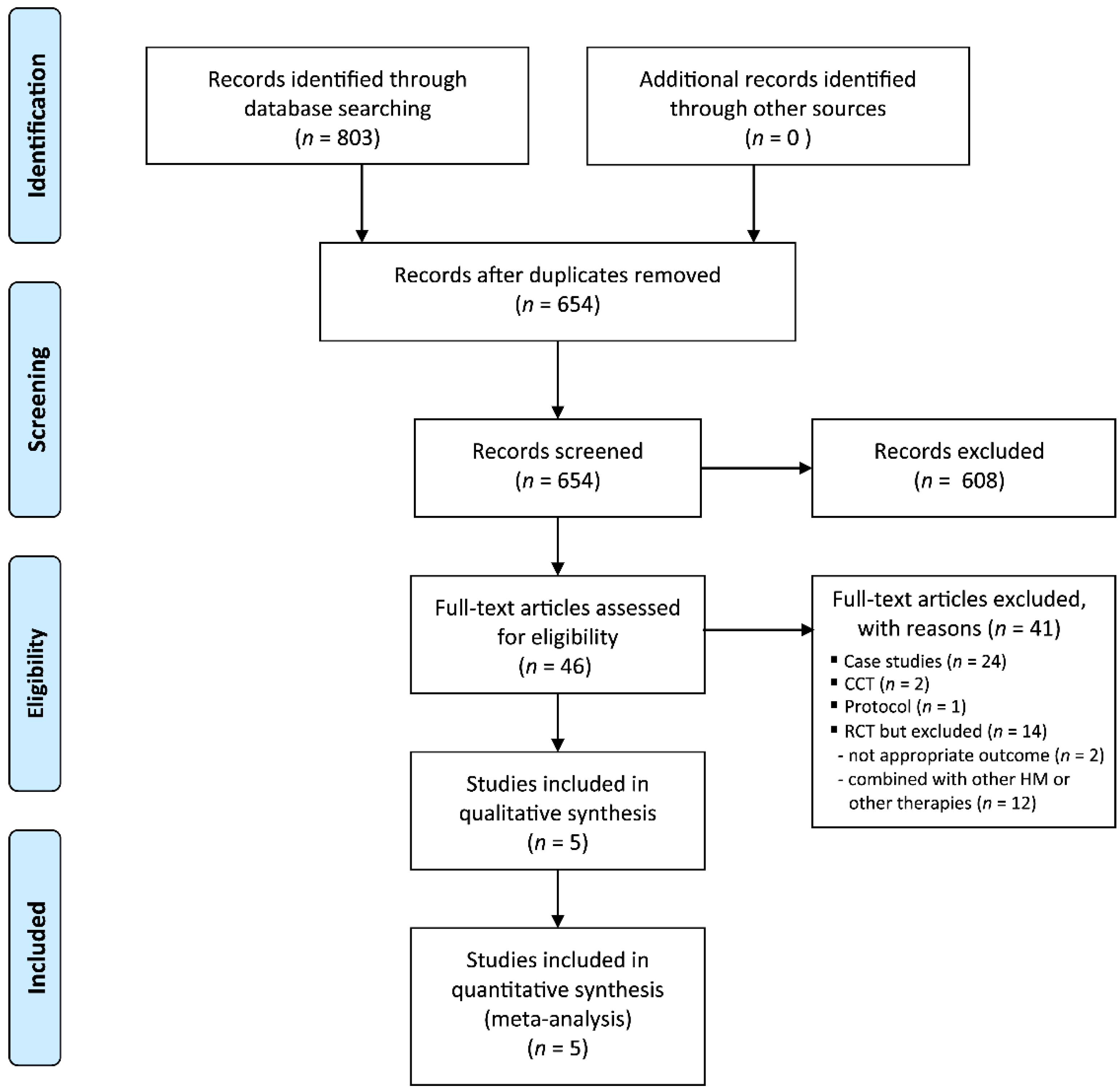
2.3. Study Selection
2.3.1. Types of Studies
2.3.2. Types of Participants
2.3.3. Types of Interventions
2.3.4. Types of Outcome Measurements
Primary Outcomes
Secondary Outcomes
2.4. Data Extraction and Risk of Bias Assessment
2.4.1. Data Extraction
2.4.2. Risk of Bias
2.4.3. Certainty of Evidence
2.5. Data Analysis
3. Results
3.1. Description of the Included Trials
3.2. Risk of Bias
3.3. Outcome Measurements
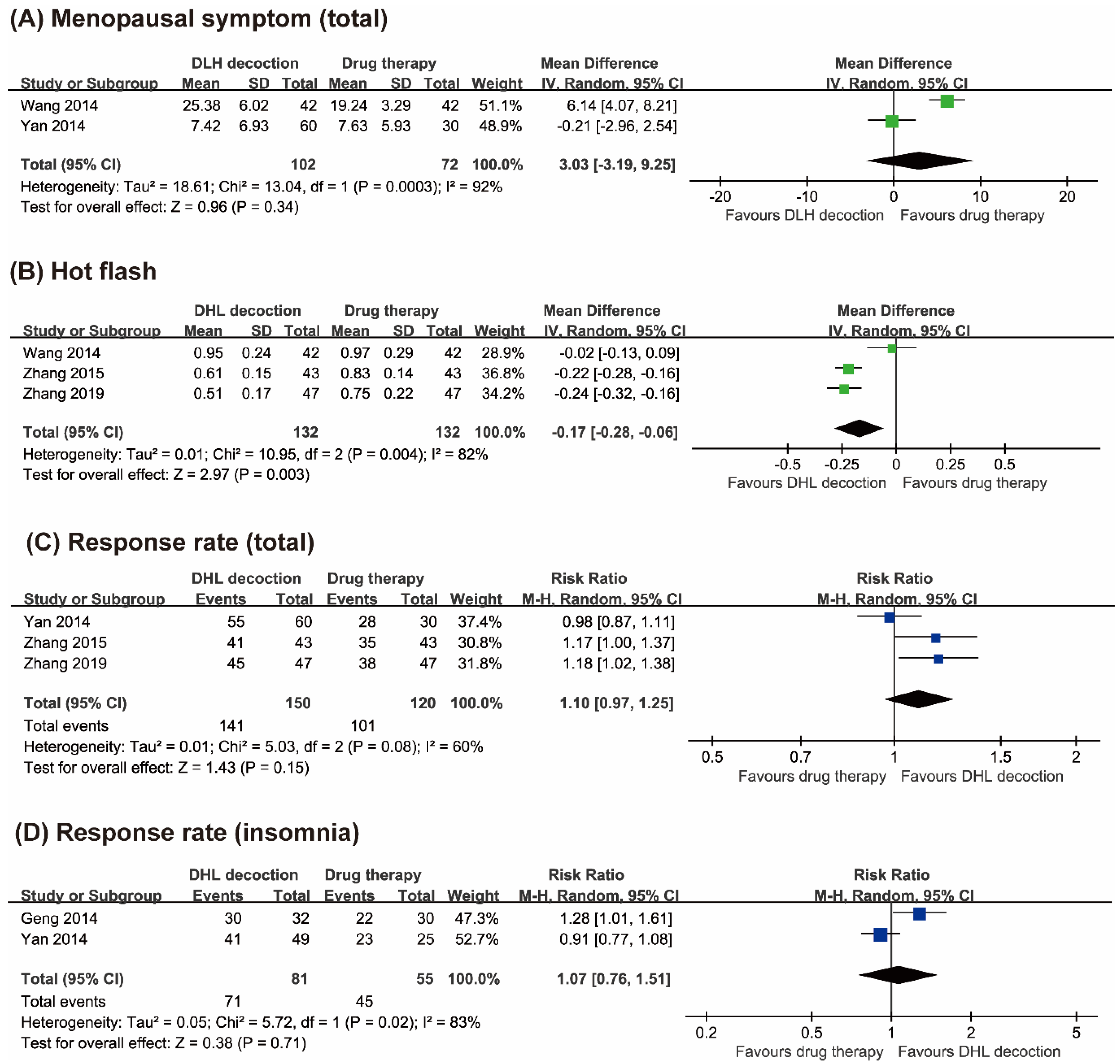
3.3.1. Menopausal Symptoms
3.3.2. Response Rate
3.3.3. Adverse Events
4. Discussion
4.1. Summary of the Main Results
4.2. Overall Completeness and Applicability of the Evidence
4.3. Cernatinty of the Evidence
4.4. Potential Biases in the Review Process
4.5. Agreements and Disagreements with Other Studies or Reviews
4.6. Implications for Practice
4.7. Implications for Research
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Deborah, G. Managment of menopausal symptoms. N. Engl. J. Med. 2006, 355, 2338–2347. [Google Scholar]
- Takahashi, T.A.; Johnson, K.M. Menopause. Med Clin. North Am. 2015, 99, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Rosano, G.M.C.; Vitale, C.; Marazzi, G.; Volterrani, M. Menopause and cardiovascular disease: The evidence. Climacteric 2007, 10, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Sciomer, S.; De Carlo, C.; Moscucci, F.; Maffei, S. Age at menopause: A fundamental data of interest to acquire in female patients’ anamnesis. Int. J. Cardiol. 2016, 215, 358–359. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Group on Hormonal Factors in Breast Cancer Type and timing of menopausal hormone therapy and breast cancer risk: Individual participant meta-analysis of the worldwide epidemiological evidence. Lancet 2019, 394, 1159–1168. [CrossRef]
- Hartley, L.; Eisinga, A.; Main, C.; Figuls, M.R.I.; Cosp, X.B.; Sánchez, R.G.; Knight, B. Hormone therapy for preventing cardiovascular disease in post-menopausal women. Cochrane Database Syst. Rev. 2015, CD002229. [Google Scholar] [CrossRef]
- Chlebowski, R.T.; Anderson, G.L. Menopausal hormone therapy and breast cancer mortality: Clinical implications. Ther. Adv. Drug Saf. 2015, 6, 45–56. [Google Scholar] [CrossRef]
- Posadzki, P.; Ernst, E. Prevalence of CAM use by UK climacteric women: A systematic review of surveys. Climacteric 2012, 16, 3–7. [Google Scholar] [CrossRef]
- Posadzki, P.; Lee, M.S.; Moon, T.; Choi, T.; Park, T.; Ernst, E. Prevalence of complementary and alternative medicine (CAM) use by menopausal women: A systematic review of surveys. Maturitas 2013, 75, 34–43. [Google Scholar] [CrossRef]
- Li, M.; Hung, A.; Lenon, G.B.; Yang, A.W.H. Chinese herbal formulae for the treatment of menopausal hot flushes: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0222383. [Google Scholar] [CrossRef]
- Wang, J.; Liu, J.; Ni, X.; Nie, G.; Zeng, Y.; Cao, X.; Li, X.; Wang, X. Adjuvant Therapy of Oral Chinese Herbal Medicine for Menopausal Depression: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2018, 2018, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lou, X.-T.; Shi, Y.-H.; Tong, Q.; Zheng, G.-Q. Erxian decoction, a Chinese herbal formula, for menopausal syndrome: An updated systematic review. J. Ethnopharmacol. 2019, 234, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Tao, J.; Song, H.; Chen, A.; Yang, H.; Zuo, M.; Li, H. Chinese herbal medicine Kuntai capsule for treatment of menopausal syndrome: A systematic review of randomized clinical trials. Complement. Ther. Med. 2016, 29, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Liew, Y.; Liu, Z.L. Chinese herbal medicine for menopausal symptoms. Cochrane Database Syst. Rev. 2016, 3, CD009023. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.Q.; Zheng, L.; Quan, Y.H. Research progress of new application of old medicine on modified dangguiliuhuang decoction. J. Hubei Univ. Chin. Med. 2015, 17, 105–108. [Google Scholar]
- Cao, H.; Tuo, L.; Tuo, Y.; Xia, Z.; Fu, R.; Liu, Y.; Quan, Y.; Liu, J.; Yu, Z.; Xiang, M. Immune and Metabolic Regulation Mechanism of Dangguiliuhuang Decoction against Insulin Resistance and Hepatic Steatosis. Front. Pharmacol. 2017, 8, 445. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Cao, H.; Ji, Y.; Pei, Y.; Yu, Z.; Quan, Y.; Xiang, M. Interaction of dendritic cells and T lymphocytes for the therapeutic effect of Dangguiliuhuang decoction to autoimmune diabetes. Sci. Rep. 2015, 5, 13982. [Google Scholar] [CrossRef]
- Jun, J.H.; Lee, H.W.; Zhang, J.; Yang, F.; Lee, M.S. Herbal medicine (Danggui Liuhuang decoction) for managing menopausal symptoms. Medicine 2018, 97, e9735. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2010; Available online: http://www.cochrane-handbook.org (accessed on 5 February 2013).
- Guyatt, G.H.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Zhang, Y. Clinical observation on 47 cases of perimenopausal syndrome treated with danggui liuhuang decoction and estradiol valerate. Chin. J. Ethnomed. Ethnopharm. 2019, 28, 101–103. [Google Scholar]
- Wang, S.F.; Xu, J.Y.; Shi, Z.R. Analysis on the clinical effect and safety of remifemin combined with traditional chieses medicine for the treatment of perimenopause syndrome. Chin. J. Birth Health Hered. 2014, 22, 110–114. [Google Scholar]
- Yan, C.; Wang, H.; Liu, P.; Cao, Y.F.; Wei, Z.H.; Li, P. Clinical study on danggui liuhuang decoction in the treatment of climacteric syndromes. J. Sichuan TCM 2014, 32, 95–97. [Google Scholar]
- Zhang, D.H. Modified danggui liuhuang decoction and routine hormone replacement therapy effect in the treatment of perimenopausal syndrome. Chin. J. Gerontol. 2015, 35, 2484–2486. [Google Scholar]
- Geng, J.; Yu, Q. A clinical observation on danggui liuhuang decoction for 32 cases of menopausal insomnia. J. TCM 2014, 55, 1581–1583. [Google Scholar]
- Currie, H.; Hamoda, H.; Fenton, B.W. Menopause. BMJ Best Practice 2020. Available online: https://bestpractice.bmj.com/topics/en-gb/194 (accessed on 20 May 2020).
- Schulz, K.F.; Altman, U.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Sample Size Conditions (Age) | Intervention Group (Regimen) | Control Group (Regimen) | Main Outcomes | Intergroup Differences | Adverse Event | Composition of Herbal Medicine |
|---|---|---|---|---|---|---|---|
| Zhang (2019) [21] | 94 women who experienced menopausal symptoms (A:50.62; B:50.38) | (A) DLH decoction (2 times daily for 4 weeks, n = 47) | (B) Drug therapy (Progynova, 2 mg, once daily for 4 weeks, n = 47) | (1) Menopausal symptoms (KI) (2) Response rate | (1) Total: n.r.; hot flash: MD, −0.24 [−0.32, −0.16], p < 0.001; insomnia: n.r. (2) Total: RR, 1.18 [1.02, 1.38], p = 0.03 | n.r. | Angelicae Gigantis Radix 6 g, Astragali Radix 12 g, Coptidis Rhizoma 6 g, Rehmanniae Radix Crudus 12 g, Rehmanniae Radix Preparata 18 g, Phellodendri Cortex 9 g, Scutellariae Radix 9 g |
| Wang (2014) [22] | 168 * women who experienced menopausal symptoms (A: 47.6; B: 48.6) | (A) Modified DLH decoction (2 times daily for 12 weeks, n = 42) | (B) Drug therapy (Climen, 1 tablet, once daily for 12 weeks, n = 42) (C) TCM patent prescription (n = 42) † (D) A plus C (n = 42) † | Menopausal symptoms (KI) | Total: MD, 6.14 [4.07, 8.21], p < 0.001; hot flush, MD, −0.02 [−0.13, 0.09], NS.; insomnia: n.r. | Stomachache (A:1, B:3); breast pain (A:11, B: 29); gastrointestinal reaction (B:4); vaginal bleeding (A:2, B:4) | Angelicae Gigantis Radix 15 g, Astragali Radix 30 g, Coptidis Rhizoma 10 g, Rehmanniae Radix Crudus 20 g, Rehmanniae Radix Preparata 20 g, Phellodendri Cortex 15 g, Scutellariae Radix 15 g Hot flushes and sweating (Fossilia Ossis Mastodi 15 g, Ostreae Testa 15 g, Schisandrae Fructus 10 g); Insomnia (Bupleuri Radix 10 g, Zizyphi Semen 20 g); Headaches (Gastrodiae Rhizoma 6 g, Uncariae Ramulus cum Uncus 6 g); Excessive menstrual blood volume (Ecliptae Herba 15 g, Sanguisorbae Radix Carbonisatum 10 g); Emotional disturbance (Tritici Levis Semen 30 g, Glycyrrhizae Radix Preparata 10 g, Zizyphi Fructus 15 g) |
| Yan (2014) [23] | 90 women who experienced menopausal symptoms (n.r.) | (A) Modified DLH decoction (3 times daily or 3 weeks, n = 60) | (B) Drug therapy (Tibolone, 1 tablet, 2.5 mg, once daily for 3 weeks, n = 30) | (1) Menopausal symptoms (KI) (2) Response rate | (1) Total: MD, −0.21 [−2.96, 2.54], NS.; hot flash: n.r.; insomnia: n.r. (2) Total: RR, 0.98 [0.87, 1.11], NS | n.r. | Angelicae Gigantis Radix 5 g, Astragali Radix 30 g, Coptidis Rhizoma 10 g, Rehmanniae Radix Crudus 20 g, Rehmanniae Radix Preparata 20 g, Phellodendri Cortex 15 g, Scutellariae Radix 15 g, Polygoni Multiflori Caulis 60 g, Zizyphi Semen 20 g |
| Zhang (2015) [24] | 86 women who experienced menopausal symptoms (A: 49.3; B: 48.7) | (A) Modified DLH decoction (2 times daily for 12 weeks, n = 43) | (B) Drug therapy (Tibolone tablets, 2.5 mg, once daily for 12 weeks, n = 43) | (1) Menopausal symptoms (KI) (2) Response rate | (1) Total: n.r.; hot flash: MD, −0.22 [−0.28, −0.16], p < 0.001; insomnia: n.r. (2) Total: RR, 1.17 [1.00, 1.37], p < 0.05 | Breast pain (B:2); vaginal bleeding (B:2) | Angelicae Gigantis Radix 10 g, Astragali Radix 20 g, Coptidis Rhizoma 3 g, Rehmanniae Radix Crudus 10 g, Rehmanniae Radix Preparata 20 g, Phellodendri Cortex 6 g, Scutellariae Radix 10 g, Nelumbinis Plumula 10 g, Uncariae Ramulus cum Uncus 15 g |
| Geng (2014) [25] | 62 women who experienced menopausal symptoms (insomnia) (A: 50.0; B: 49.5) | (A) Modified DLH decoction (2 times daily for 4 weeks, n = 32) | (B) Drug therapy (Estazolam tablets, 1 mg or 3 mg to 4 mg with severe symptoms once daily for 4 weeks, n = 30) | Response rate | RR, 1.28 [1.01, 1.61] based on insomnia score | Dizziness (B:7); daytime sleepiness (B:3); fatigue (B:11) | Angelicae Gigantis Radix 15 g, Astragali Radix 30 g, Coptidis Rhizoma 10 g, Rehmanniae Radix Crudus 12 g, Rehmanniae Radix Preparata 10 g, Phellodendri Cortex 12 g, Scutellariae Radix 12 g, Hot flushes and sweating (Lycii Radicis Cortex 15 g); Insomnia (Gardeniae Fructus 9 g, Lophatheri Herba 12 g); Headaches (Chrysanthemi Flos 9 g, Mori Folium 12 g); Emotional disturbance (Lilii Bulbus 15 g); Sweating (Tritici Levis Semen 30 g) |
| DLH Decoction Compared to Conventional Drug Therapies for Menopausal Symptoms | |||||
|---|---|---|---|---|---|
| Patient or Population: Menopausal Symptoms Setting: community/ outpatients Intervention: DLH Decoction Comparison: Conventional Drug Therapies | |||||
| Outcomes | No. of Participants (Studies) Follow-up | Certainty of the Evidence (GRADE) | Relative Effect (95% CI) | Anticipated Absolute Effects* | |
| Risk with Conventional Drug Therapies | Risk Difference with DLH Decoction | ||||
| Menopausal symptoms Kupperman index (follow up: range 3 weeks to 12 weeks) | 174 (2 RCTs) | ⨁◯◯◯ VERY LOW a,b,c,d | - | MD 3.03 higher (3.19 lower to 9.25 higher) | |
| Hot flashes (follow up: range 3 weeks to 12 weeks) | 264 (3 RCTs) | ⨁⨁◯◯ LOW a,d | - | MD 0.17 lower (0.28 lower to 0.06 lower) | |
| Response rate (follow up: range 3 weeks to 12 weeks) | 270 (3 RCTs) | ⨁◯◯◯ VERY LOW a,b,d | RR 1.10 (1.07 to 1.25) | 842 per 1000 | 84 more per 1000 (59 more to 210 more) |
| Response rate (insomnia) (follow up: range 3 weeks to 12 weeks) | 136 (2 RCTs) | ⨁◯◯◯ VERY LOW a,b,d | RR 1.07 (0.76 to 1.51) | 818 per 1000 | 57 more per 1000 (196 fewer to 417 more) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jun, J.H.; Lee, H.W.; Zhang, J.; Yang, F.; Lee, M.S. Herbal Medicines (Danggui Liuhuang Decoctions) for Management of Menopausal Symptoms: A Systematic Review of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 1778. https://doi.org/10.3390/jcm9061778
Jun JH, Lee HW, Zhang J, Yang F, Lee MS. Herbal Medicines (Danggui Liuhuang Decoctions) for Management of Menopausal Symptoms: A Systematic Review of Randomized Controlled Trials. Journal of Clinical Medicine. 2020; 9(6):1778. https://doi.org/10.3390/jcm9061778
Chicago/Turabian StyleJun, Ji Hee, Hye Won Lee, Junhua Zhang, Fengwen Yang, and Myeong Soo Lee. 2020. "Herbal Medicines (Danggui Liuhuang Decoctions) for Management of Menopausal Symptoms: A Systematic Review of Randomized Controlled Trials" Journal of Clinical Medicine 9, no. 6: 1778. https://doi.org/10.3390/jcm9061778
APA StyleJun, J. H., Lee, H. W., Zhang, J., Yang, F., & Lee, M. S. (2020). Herbal Medicines (Danggui Liuhuang Decoctions) for Management of Menopausal Symptoms: A Systematic Review of Randomized Controlled Trials. Journal of Clinical Medicine, 9(6), 1778. https://doi.org/10.3390/jcm9061778