The Impact of COVID-19 on Gastrointestinal Motility Testing in Asia and Europe

 , , ,
, , ,  , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Survey Using Questionnaires Established for Centres in Asian Countries
2.2. Analysis of the Relationship between the Reduced Rate of Gastrointestinal Motility and Function Tests
2.3. Statistical Analysis
3. Results
3.1. Impact of the Build-Up and Peak Period of the COVID-19 Pandemic in Asian and European Countries
3.1.1. Characteristics of Participating Centres
3.1.2. Impact on Oesophageal Manometry
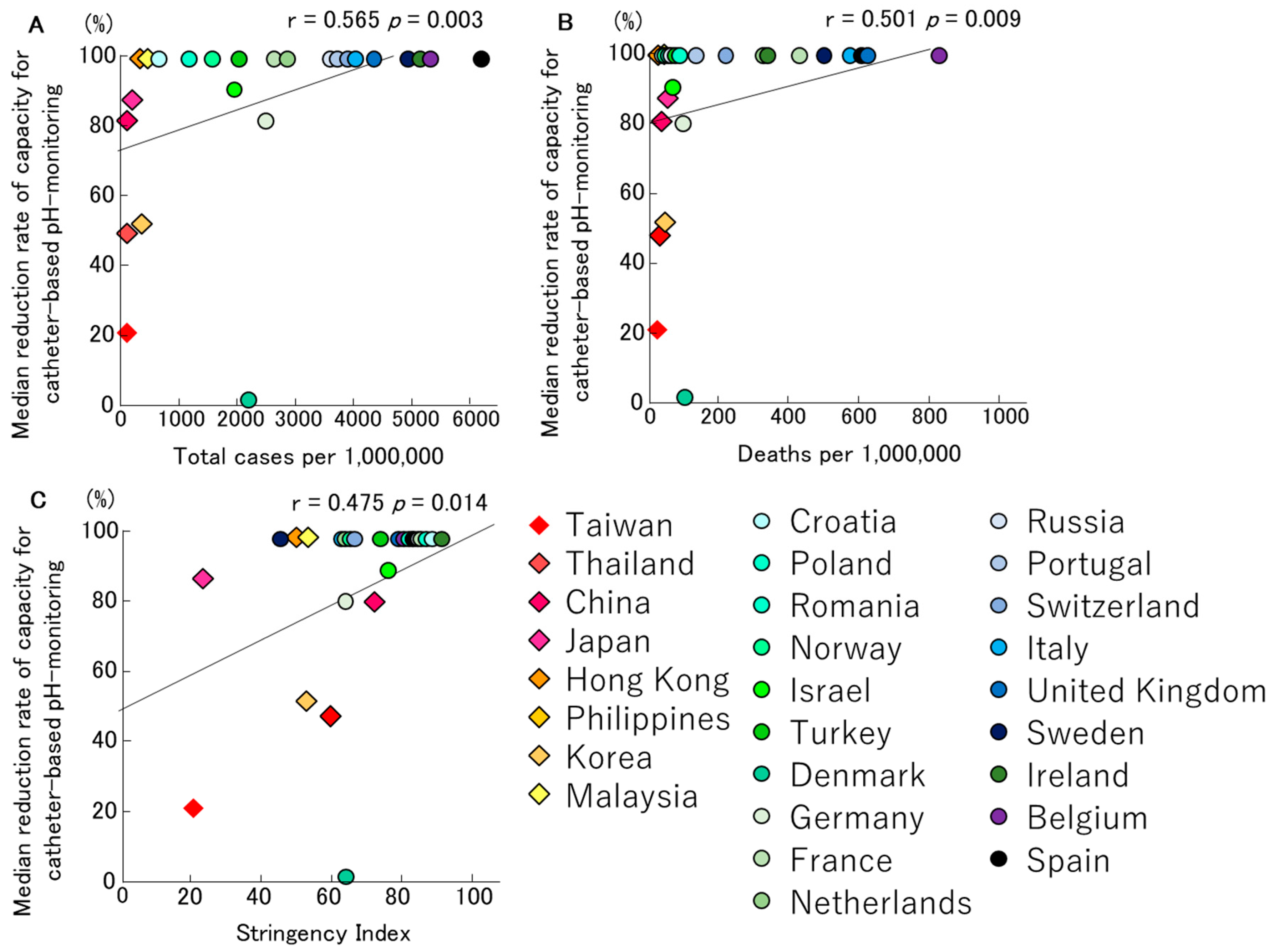
3.1.3. Impact on Catheter-Based pH Monitoring
3.1.4. Impact on Wireless pH Testing (Bravo®)
3.1.5. Impact on Anorectal Manometry
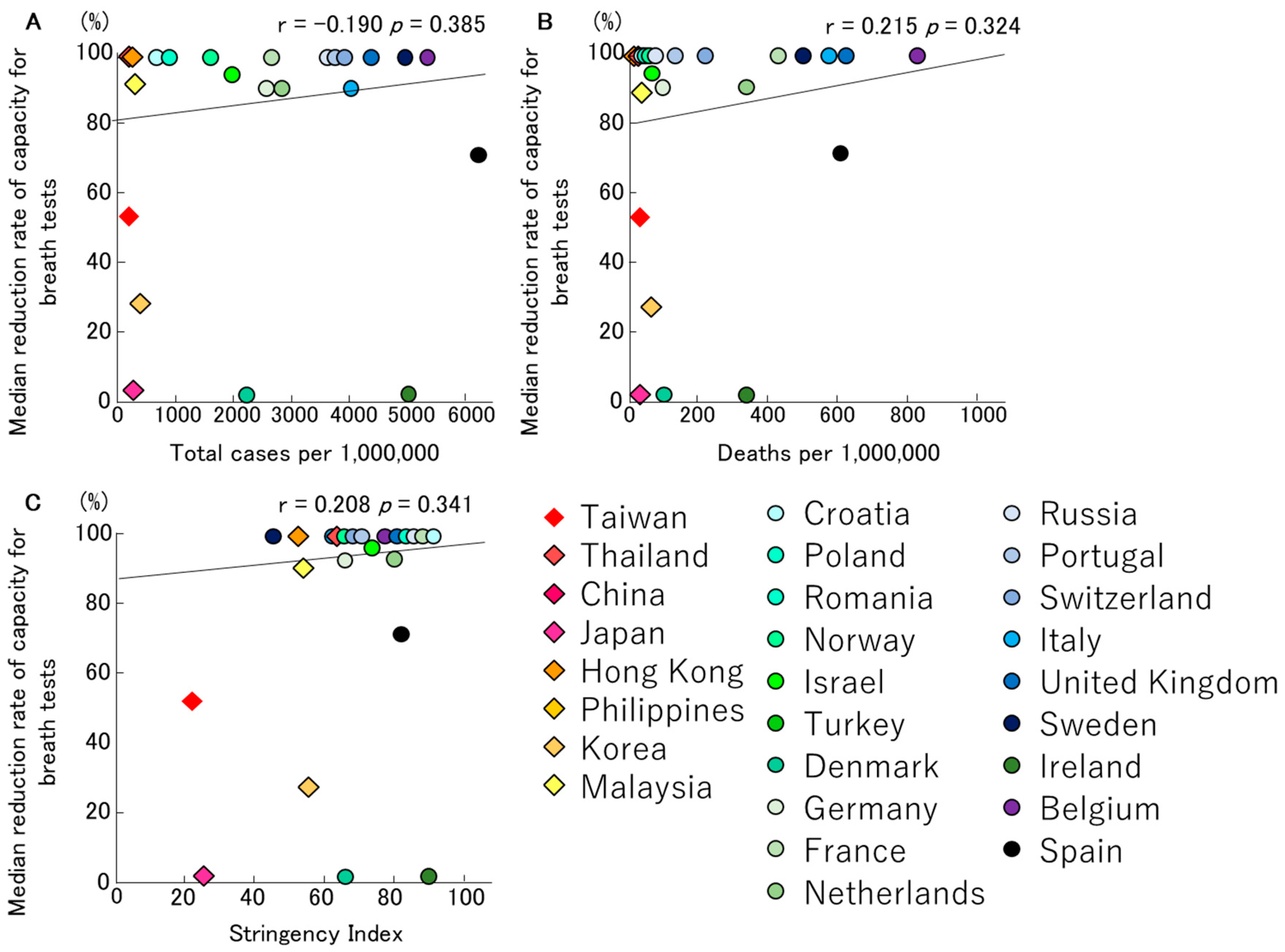
3.1.6. Impact on Breath Tests
3.2. Planned Use of Personal Protective Equipment for Motility and Function Testing during the Early Recovery Phase of the COVID-19 Pandemic
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Suzuki, H.; Matsuzaki, J.; Taniguchi, K.; Shimizu, T.; Yamane, T.; Kanai, T. Gender difference of gastric emptying in healthy volunteers and patients with functional dyspepsia. Digestion 2017, 95, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Carbone, F.; Van den Houte, K.; Clevers, E.; Andrews, C.N.; Papathanasopoulos, A.; Holvoet, L.; Tack, J. Prucalopride in gastroparesis: A randomized placebo-controlled crossover study. Am. J. Gastroenterol. 2019, 114, 1265–1274. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, A.; Boecxstaens, V.; Andrews, C.N.; Attwood, S.E.; Berrisford, R.; Bisschops, R.; Corsetti, M. How to select patients for antireflux surgery? The ICARUS guidelines (international consensus regarding preoperative examinations and clinical characteristics assessment to select adult patients for antireflux surgery). Gut 2019, 68, 1928–1941. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.D.; Gray, K.D.; Panjwani, S.; Finnerty, B.; Ciecerega, T.; Afaneh, C.; Zarnegar, R. Impact of procedural multimedia instructions for pH BRAVO testing on patient comprehension: A prospective randomized study. Dis. Esophagus 2020, 33, doz068. [Google Scholar] [CrossRef] [PubMed]
- Bredenoord, A.J.; Hebbard, G.S. Technical aspects of clinical high-resolution manometry studies. Neurogastroenterol. Motil. 2012, 24, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Du, G. COVID-19 may transmit through aerosol. Ir. J. Med. Sci. 2020, 1971, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Tack, J.; Schol, J.; Geeraerts, A.; Huang, I.H.; Mori, H.; Scarpellini, E.; Jandee, S. A survey on the impact of the COVID-19 pandemic on motility and functional investigations in Europe and considerations for recommencing activities in the early recovery phase. Neurogastroenterol. Motil. 2020, 32, e13926. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Wang, L.; Cauchemez, S.; Xu, X.; Wang, X.; Cowling, B.J.; Meyers, L.A. Risk for transportation of coronavirus disease from Wuhan to other cities in China. Emerg. Infect. Dis. 2020, 26, 1049. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Ariumi, Y.; Nishida, N.; Yamamoto, R.; Bauer, G.; Gojobori, T.; Mizokami, M. SARS-CoV-2 infections and COVID-19 mortalities strongly correlate with ACE1 I/D genotype. Gene 2020, 758, 144944. [Google Scholar] [CrossRef] [PubMed]
- Tack, J.; Vanuytsel, T.; Serra, J.; Accarino, A.; Stanghellini, V.; Barbara, G.; Drewes, A. European Society for Neurogastroenterology and Motility (ESNM) recommendations for conducting gastrointestinal motility and function testing in the recovery phase of the COVID-19 pandemic. Neurogastroenterol. Motil. 2020, 32, e13930. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, I.; De Greef, T.; Haesendonck, N.; Tack, J. Esophageal motility in children with suspected gastroesophageal reflux disease. J. Pediatric Gastroenterol. Nutr. 2010, 50, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Rohof, W.O.; Salvador, R.; Annese, V.; des Varannes, S.B.; Chaussade, S.; Costantini, M.; Busch, O.R. Outcomes of treatment for achalasia depend on manometric subtype. Gastroenterology 2013, 144, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Masaoka, T.; Kameyama, H.; Yamane, T.; Yamamoto, Y.; Takeuchi, H.; Suzuki, H.; Kanai, T. Pathophysiology of Potassium-competitive Acid Blocker–refractory Gastroesophageal Reflux and the Potential of Potassium-competitive Acid Blocker Test. J. Neurogastroenterol. Motil. 2018, 24, 577. [Google Scholar] [CrossRef] [PubMed]
- Cura Pales, C.G.; An, S.; Cruz, J.P.; Kim, K.; Kim, Y. Postoperative bowel function after anal sphincter-preserving rectal cancer surgery: Risks factors, diagnostic modalities, and management. Ann. Coloproctol. 2019, 35, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Verelst, F.; Kuylen, E.J.; Beutels, P. Indications for healthcare surge capacity in European countries facing an exponential increase in COVID19 cases. medRxiv 2020. [Google Scholar] [CrossRef]
- Sabat, I.; Neuman-Böhme, S.; Varghese, N.E.; Barros, P.P.; Brouwer, W.; van Exel, J.; Stargardt, T. United but Divided: Policy Responses and People’s Perceptions in the EU during the COVID-19 Outbreak; Health Policy: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Siah, K.T.; Rahman, M.M.; Ong, A.M.; Soh, A.Y.; Lee, Y.Y.; Xiao, Y.; Patcharatrakul, T. The Practice of Gastrointestinal Motility Laboratory During COVID-19 Pandemic: Position Statements of the Asian Neurogastroenterology and Motility Association (ANMA-GML-COVID-19 Position Statements). J. Neurogastroenterol. Motil. 2020, 26, 299. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Oesophageal Manometry | Catheter-Based pH-Monitoring | Bravo® pH-Capsule | Anal Manometry | Breath Tests | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Protection Mechanism | AS (n = 49) | EU (n = 30) | p-Value | AS (n = 50) | EU (n = 31) | p-Value | AS (n = 12) | EU (n = 13) | p-Value | AS (n = 25) | EU (n = 29) | p-Value | AS (n = 35) | EU (n = 22) | p-Value |
| None | 2% | 0% | 1.000 | 2% | 0% | 1.000 | 8% | 0% | 0.48 | 4% | 0% | 0.463 | 20% | 0% | 0.025 |
| Negative pressure room | 2% | 3% | 1.000 | 2% | 3% | 1.000 | 0% | 8% | 1.000 | 0% | 3% | 1.000 | 3% | 0% | 1.000 |
| Surgical mask | 82% | 27% | 0.000 | 80% | 26% | 0.000 | 83% | 15% | 1.000 | 88% | 55% | 0.015 | 69% | 32% | 0.013 |
| FFP2-mask | 14% | 73% | 0.000 | 14% | 71% | 0.000 | 17% | 77% | 0.005 | 4% | 55% | 0.000 | 9% | 50% | 0.001 |
| FFP3-mask | 4% | 20% | 0.048 | 4% | 23% | 0.024 | 8% | 23% | 0.593 | 4% | 10% | 0.615 | 3% | 23% | 0.028 |
| Goggles | 43% | 43% | 1.000 | 42% | 45% | 0.821 | 42% | 31% | 0.688 | 36% | 34% | 1.000 | 31% | 45% | 0.398 |
| Face shield | 63% | 80% | 0.137 | 62% | 81% | 0.089 | 83% | 77% | 1.000 | 48% | 52% | 0.79 | 49% | 68% | 0.178 |
| Hairnet | 45% | 77% | 0.010 | 44% | 81% | 0.001 | 36% | 66% | 0.055 | 63% | 64% | 0.062 | |||
| Water-resistant gown | 58% | 77% | 0.411 | 64% | 65% | 1.000 | 49% | 55% | 0.787 | ||||||
| Non-water-resistant gown | 63% | 73% | 0.461 | 62% | 74% | 0.334 | 83% | 85% | 0.593 | 12% | 28% | 0.191 | 91% | 23% | 0.239 |
| Long sleeved gloves | 16% | 23% | 0.557 | 16% | 23% | 0.559 | 8% | 15% | 1.000 | 8% | 21% | 0.262 | 94% | 0% | 0.281 |
| Standard gloves | 10% | 23% | 0.195 | 10% | 23% | 0.197 | 8% | 23% | 0.593 | 52% | 83% | 0.431 | 26% | 82% | 0.747 |
| Overshoe covers | 90% | 77% | 0.195 | 88% | 81% | 0.521 | 25% | 69% | 1.000 | 0% | 3% | 1.000 | 0% | 0% | 1.000 |
| Screening Procedure | Oesophageal Manometry | Catheter-Based pH-Monitoring | Bravo® pH-Capsule | Anal Manometry | Breath Tests | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AS (n = 50) | EU (n = 30) | p-Value | AS (n = 49) | EU (n = 31) | p-Value | AS (n = 14) | EU (n = 13) | p-Value | AS (n = 24) | EU (n = 29) | p-Value | AS (n = 35) | EU (n = 22) | p-Value | |
| None | 10% | 0% | 0.151 | 8% | 0% | 0.154 | 7% | 0% | 1.000 | 4% | 0% | 0.452 | 14% | 0% | 0.145 |
| Anamnestic risk assessment | 68% | 93% | 0.011 | 71% | 94% | 0.021 | 79% | 92% | 0.595 | 71% | 90% | 0.156 | 66% | 100% | 0.002 |
| Temperature check | 84% | 83% | 1.000 | 82% | 84% | 1.000 | 86% | 77% | 0.648 | 88% | 83% | 0.715 | 74% | 82% | 0.746 |
| Nasopharyngeal PCR-swab | 24% | 50% | 0.027 | 20% | 48% | 0.013 | 29% | 46% | 0.440 | 25% | 38% | 0.383 | 20% | 36% | 0.221 |
| CT-scan | 2% | 3% | 0.612 | 4% | 3% | 1.000 | 7% | 0% | 1.000 | 0% | 3% | 1.000 | 0% | 5% | 0.386 |
| Serology test | 0% | 7% | 0.137 | 0% | 10% | 0.055 | 0% | 8% | 0.481 | 0% | 7% | 0.494 | 0% | 9% | 0.144 |
| Saturation O2 | 0% | 3% | 0.375 | 0% | 3% | 0.388 | 0% | 0% | 1.000 | 0% | 3% | 1.000 | 0% | 5% | 0.386 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, H.; Schol, J.; Geeraerts, A.; Huang, I.-H.; Jandee, S.; Gonlachanvit, S.; Tseng, P.-H.; Lu, C.-L.; Kamiya, T.; Kim, N.; et al. The Impact of COVID-19 on Gastrointestinal Motility Testing in Asia and Europe. J. Clin. Med. 2020, 9, 3189. https://doi.org/10.3390/jcm9103189
Mori H, Schol J, Geeraerts A, Huang I-H, Jandee S, Gonlachanvit S, Tseng P-H, Lu C-L, Kamiya T, Kim N, et al. The Impact of COVID-19 on Gastrointestinal Motility Testing in Asia and Europe. Journal of Clinical Medicine. 2020; 9(10):3189. https://doi.org/10.3390/jcm9103189
Chicago/Turabian StyleMori, Hideki, Jolien Schol, Annelies Geeraerts, I-Hsuan Huang, Sawangpong Jandee, Sutep Gonlachanvit, Ping-Huei Tseng, Ching-Liang Lu, Takeshi Kamiya, Nayoung Kim, and et al. 2020. "The Impact of COVID-19 on Gastrointestinal Motility Testing in Asia and Europe" Journal of Clinical Medicine 9, no. 10: 3189. https://doi.org/10.3390/jcm9103189
APA StyleMori, H., Schol, J., Geeraerts, A., Huang, I.-H., Jandee, S., Gonlachanvit, S., Tseng, P.-H., Lu, C.-L., Kamiya, T., Kim, N., Lee, Y. Y., Kuribayashi, S., Tack, J., & Suzuki, H. (2020). The Impact of COVID-19 on Gastrointestinal Motility Testing in Asia and Europe. Journal of Clinical Medicine, 9(10), 3189. https://doi.org/10.3390/jcm9103189