Effect of Intrasilicone Bevacizumab Injection in Diabetic Tractional Retinal Detachment Surgery: A Retrospective Case-Control Study


Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Surgical Technique and Postoperative Managements
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics and Clinical Characteristics
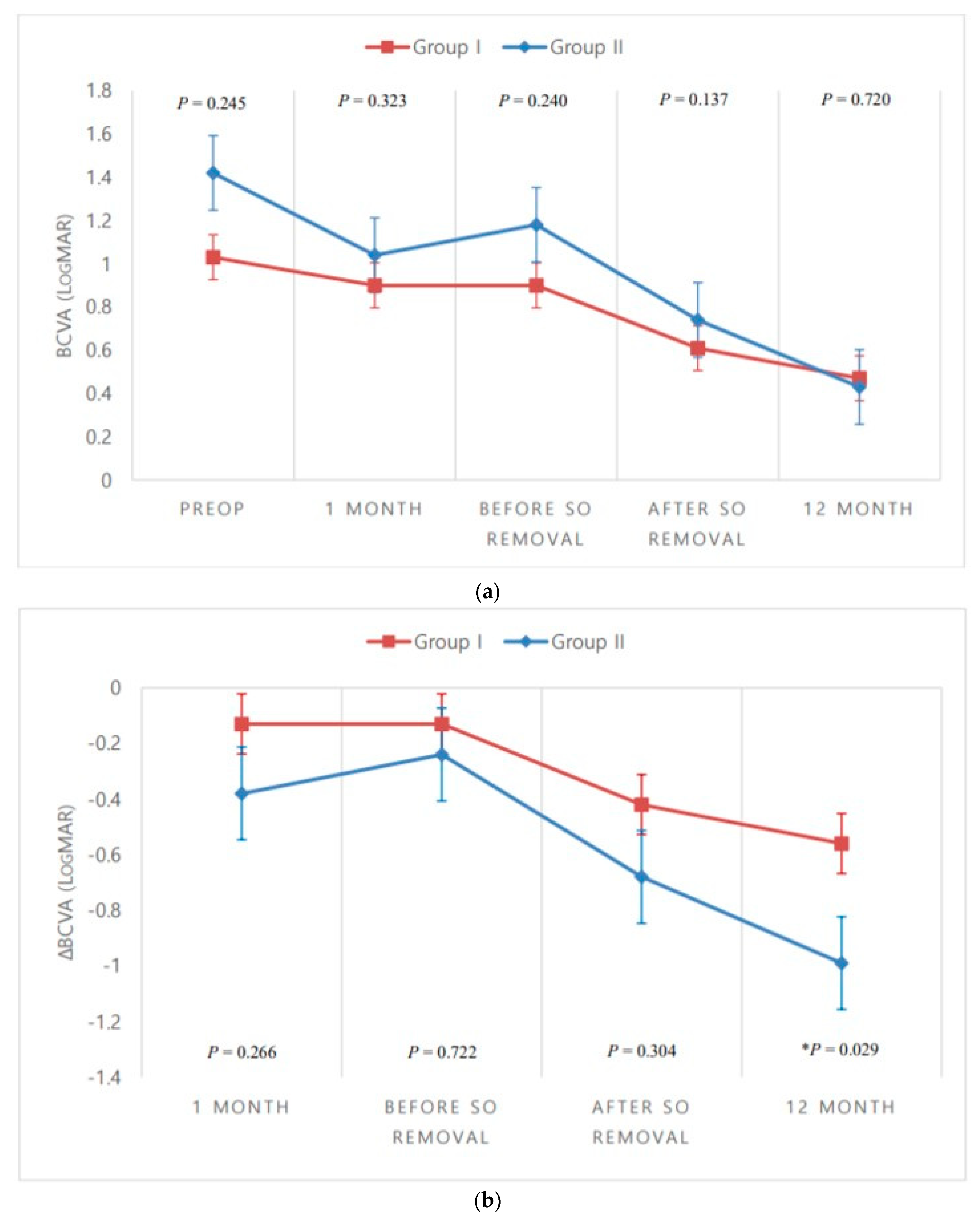
3.2. Visual Outcomes
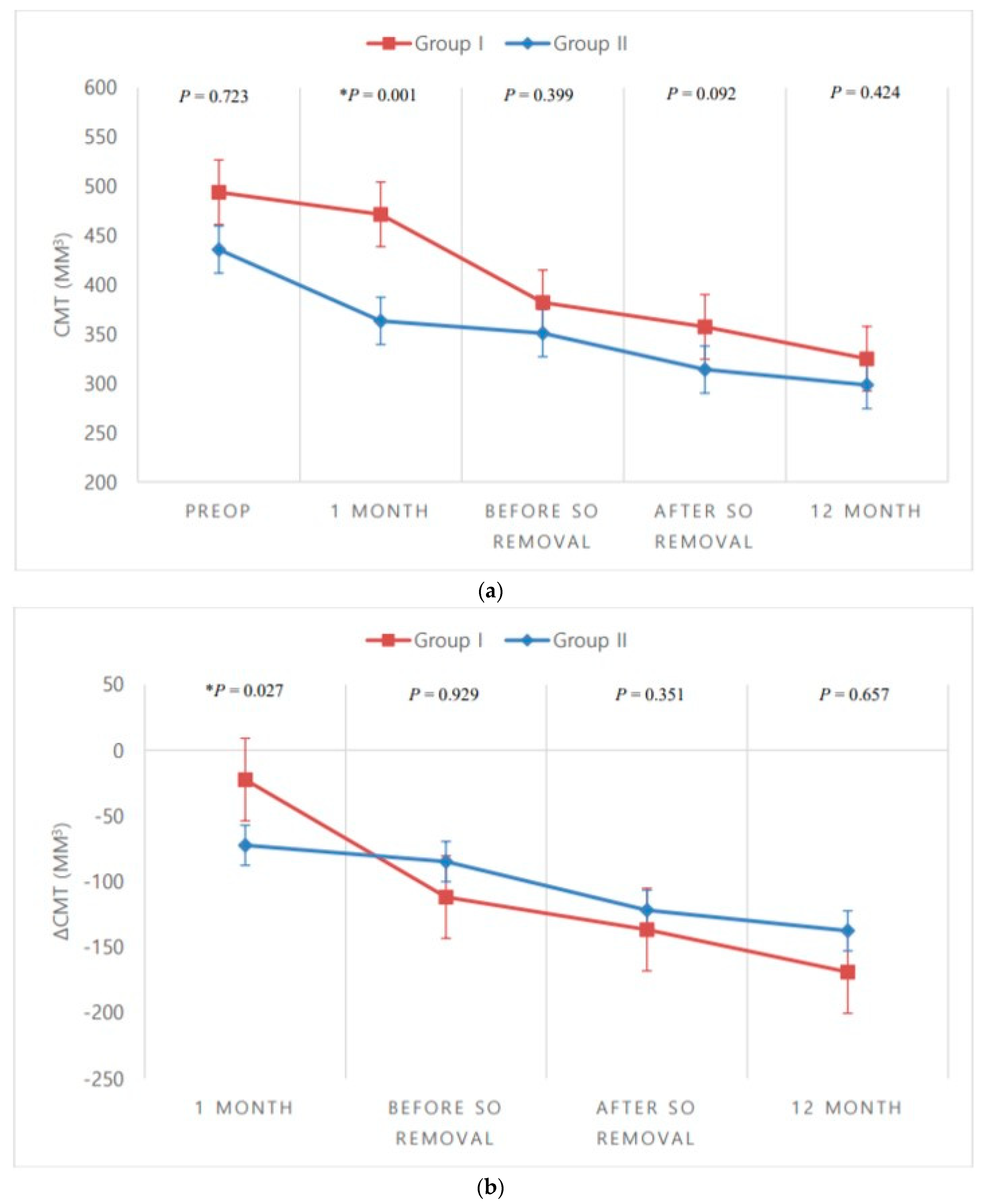
3.3. Anatomic Outcomes
3.4. Postoperative Complications and Other Outcomes
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Fong, D.S.; Ferris, F.L., III; Davis, M.D.; Chew, E.Y. Causes of severe visual loss in the early treatment diabetic retinopathy study: ETDRS report no. 24. Early Treatment Diabetic Retinopathy Study Research Group. Am. J. Ophthalmol. 1999, 127, 137–141. [Google Scholar] [CrossRef]
- Stewart, M.W.; Browning, D.J.; Landers, M.B. Current management of diabetic tractional retinal detachments. Indian J. Ophthalmol. 2018, 66, 1751–1762. [Google Scholar] [CrossRef]
- Abu El-Asrar, A.M.; Al-Bishi, S.M.; Kangave, D. Outcome of temporary silicone oil tamponade in complex rhegmatogenous retinal detachment. Eur. J. Ophthalmol. 2003, 13, 474–481. [Google Scholar] [CrossRef]
- Scott, I.U.; Flynn, H.W., Jr.; Murray, T.G.; Smiddy, W.E.; Davis, J.L.; Feuer, W.J. Outcomes of complex retinal detachment repair using 1000- vs 5000-centistoke silicone oil. Arch. Ophthalmol. 2005, 123, 473–478. [Google Scholar] [CrossRef]
- Castellarin, A.; Grigorian, R.; Bhagat, N.; Del Priore, L.; Zarbin, M.A. Vitrectomy with silicone oil infusion in severe diabetic retinopathy. Br. J. Ophthalmol. 2003, 87, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Yeh, P.T.; Yang, C.M.; Lin, Y.C.; Chen, M.S.; Yang, C.H. Bevacizumab pretreatment in vitrectomy with silicone oil for severe diabetic retinopathy. Retina 2009, 29, 768–774. [Google Scholar] [CrossRef]
- Ferrara, N. Vascular endothelial growth factor: Basic science and clinical progress. Endocr. Rev. 2004, 25, 581–611. [Google Scholar] [CrossRef]
- Hegazy, H.M.; Kivilcim, M.; Peyman, G.A.; Unal, M.H.; Liang, C.; Molinari, L.C.; Kazi, A.A. Evaluation of toxicity of intravitreal ceftazidime, vancomycin, and ganciclovir in a silicone oil-filled eye. Retina 1999, 19, 553–557. [Google Scholar] [CrossRef]
- Grzybowski, A.; Told, R.; Sacu, S.; Bandello, F.; Moisseiev, E.; Loewenstein, A.; Schmidt-Erfurth, U. 2018 update on intravitreal injections: Euretina Expert Consensus Recommendations. Ophthalmologica 2018, 239, 181–193. [Google Scholar] [CrossRef]
- Ahmadieh, H.; Feghhi, M.; Tabatabaei, H.; Shoeibi, N.; Ramezani, M.; Mohebbi, M.R. Triamcinolone acetonide in silicone-filled eyes as adjunctive treatment for proliferative vitreoretinopathy: A randomized clinical trial. Ophthalmology 2008, 115, 1938–1943. [Google Scholar] [CrossRef]
- Chhablani, J.; Narayanan, R. Anti-VEGF therapy in a silicone oil-filled myopic eye with choroidal neovascularisation. BMJ Case Rep. 2015, bcr2014208663. [Google Scholar] [CrossRef] [PubMed]
- Falavarjani, K.G.; Modarres, M.; Nazari, H. Therapeutic effect of bevacizumab injected into the silicone oil in eyes with neovascular glaucoma after vitrectomy for advanced diabetic retinopathy. Eye 2010, 24, 717–719. [Google Scholar] [CrossRef] [PubMed]
- Salman, A.G. Intrasilicone bevacizumab injection for iris neovascularization after vitrectomy for proliferative diabetic retinopathy. Ophthalmic Res. 2013, 49, 20–24. [Google Scholar] [CrossRef]
- Alishiri, A.; Naderi, M.; Jadidi, K.; Mosavi, S.A. Efficacy of simultaneous usage of bevacizumab and silicone oil injection after vitrectomy in diabetic tractional retinal detachment. Razavi Int. J. Med. 2017, e43217. [Google Scholar] [CrossRef]
- Rashad, M.A.; Mohamed, A.A.A.; Ahmed, A.I. Value of optical coherence tomography in the detection of macular pathology before the removal of silicone oil. Clin. Ophthalmol. 2016, 10, 121–135. [Google Scholar] [CrossRef]
- Iyer, S.S.R.; Regan, K.A.; Burnham, J.M.; Chen, C.J. Surgical management of diabetic tractional retinal detachments. Surv. Ophthalmol. 2019, 64, 780–809. [Google Scholar] [CrossRef]
- Aiello, L.P.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E.; et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef]
- Chen, E.; Park, C.H. Use of intravitreal bevacizumab as a preoperative adjunct for tractional retinal detachment repair in severe proliferative diabetic retinopathy. Retina 2006, 26, 699–700. [Google Scholar] [CrossRef]
- Rizzo, S.; Genovesi-Ebert, F.; Di Bartolo, E.; Vento, A.; Miniaci, S.; Williams, G. Injection of intravitreal bevacizumab (Avastin) as a preoperative adjunct before vitrectomy surgery in the treatment of severe proliferative diabetic retinopathy (PDR). Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 837–842. [Google Scholar] [CrossRef]
- Yeoh, J.; Williams, C.; Allen, P.; Buttery, R.; Chiu, D.; Clark, B.; Essex, R.; McCombe, M.; Qureshi, S.; Campbell, W.G. Avastin as an adjunct to vitrectomy in the management of severe proliferative diabetic retinopathy: A prospective case series. Clin. Exp. Ophthalmol. 2008, 36, 449–454. [Google Scholar] [CrossRef]
- Hattori, T.; Shimada, H.; Nakashizuka, H.; Mizutani, Y.; Mori, R.; Yuzawa, M. Dose of intravitreal bevacizumab (Avastin) used as preoperative adjunct therapy for proliferative diabetic retinopathy. Retina 2010, 30, 761–764. [Google Scholar] [CrossRef] [PubMed]
- Ahmadieh, H.; Shoeibi, N.; Entezari, M.; Monshizadeh, R. Intravitreal bevacizumab for prevention of early postvitrectomy hemorrhage in diabetic patients: A randomized clinical trial. Ophthalmology 2009, 116, 1943–1948. [Google Scholar] [CrossRef] [PubMed]
- Lo, W.R.; Kim, S.J.; Aaberg, T.M., Sr.; Bergstrom, C.; Srivastava, S.; Yan, J.; Martin, D.F.; Hubbard, G.B., III. Visual outcomes and incidence of recurrent vitreous hemorrhage after vitrectomy in diabetic eyes pretreated with bevacizumab (Avastin). Retina 2009, 29, 926–931. [Google Scholar] [CrossRef]
- Da R Lucena, D.; Ribeiro, J.A.S.; Costa, R.A.; Barbosa, J.C.; Scott, I.U.; de Figueirido-Pontes, L.L.; Jorge, R. Intraoperative bleeding during vitrectomy for diabetic tractional retinal detachment with versus without preoperative intravitreal bevacizumab (IBeTra study). Br. J. Ophthalmol. 2009, 93, 688–691. [Google Scholar] [CrossRef]
- Oshima, Y.; Shima, C.; Wakabayashi, T.; Kusaka, S.; Shiraga, F.; Masahito, O.; Tano, Y. Microincision vitrectomy surgery and intravitreal bevacizumab as a surgical adjunct to treat diabetic traction retinal detachment. Ophthalmology 2009, 116, 927–938. [Google Scholar] [CrossRef]
- di Lauro, R.; De Ruggiero, P.; di Lauro, R.; di Lauro, M.T.; Romano, M.R. Intravitreal bevacizumab for surgical treatment of severe proliferative diabetic retinopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2010, 248, 785–791. [Google Scholar] [CrossRef]
- Simo, R.; Carrasco, E.; Garcia-Ramirez, M.; Hernandez, C. Angiogenic and antiangiogenic factors in proliferative diabetic retinopathy. Curr. Diabetes. Rev. 2006, 2, 71–98. [Google Scholar] [CrossRef]
- Funatsu, H.; Yamashita, H.; Ikeda, T.; Mimura, T.; Eguchi, S.; Hori, S. Vitreous levels of interleukin-6 and vascular endothelial growth factor are related to diabetic macular edema. Ophthalmology 2003, 110, 1690–1696. [Google Scholar] [CrossRef]
- Gorenjak, V.; Vance, D.R.; Petrelis, A.M.; Stathopoulou, M.G.; Dadé, S.; Shamieh, S.E.; Helena, M.; Masson, C.; Lamont, J.; Fitzgerald, P.; et al. Peripheral blood mononuclear cells extracts VEGF protein levels and VEGF mRNA: Associations with inflammatory molecules in a healthy population. PLoS ONE 2019, 14, e0220902. [Google Scholar] [CrossRef]
- Park, D.H.; Shin, J.P.; Kim, S.Y. Intravitreal injection of bevacizumab and triamcinolone acetonide at the end of vitrectomy for diabetic vitreous hemorrhage: A comparative study. Graefes Arch. Clin. Exp. Ophthalmol. 2010, 248, 641–650. [Google Scholar] [CrossRef]
- Cheema, R.A.; Mushtaq, J.; Al-Khars, W.; Al-Askar, E.; Cheema, M.A. Role of intravitreal bevacizumab (Avastin) injected at the end of diabetic vitrectomy in preventing postoperative recurrent vitreous hemorrhage. Retina 2010, 30, 1646–1650. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Woo, S.J.; Chung, H.; Park, K.H. The effect of adjunctive intravitreal bevacizumab for preventing postvitrectomy hemorrhage in proliferative diabetic retinopathy. Ophthalmology 2011, 118, 2218–2226. [Google Scholar] [CrossRef] [PubMed]
- Byon, I.S.; Lee, J.E.; Oum, B.S. Intravitreal injection of triamcinolone acetonide in vitrectomy with silicone oil placement. J. Korean Ophthalmol. Soc. 2006, 47, 1298–1305. [Google Scholar]
- Esenulku, C.M.; Gunay, M. Location of a dexamethasone implant at the macula after intravitreal injection in a silicone oil-filled eye. Case Rep. Ophthalmol. Med. 2006, 5107652. [Google Scholar] [CrossRef]
- Kroll, P.; Rodrigues, E.B.; Hoerle, S. Pathogenesis and classification of proliferative diabetic vitreoretinopathy. Ophthalmologica 2007, 221, 78–94. [Google Scholar] [CrossRef]
- Sato, K.; Tsuboi, K.; Nakashima, H.; Emi, K. Characteristics of cases with postoperative vitreous hemorrhage after 25-gauge vitrectomy for repair of proliferative diabetic retinopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 665–671. [Google Scholar] [CrossRef]
- Moradian, S.; Ahmadieh, H.; Malihi, M.; Soheilian, M.; Dehghan, M.H.; Azarmina, M. Intravitreal bevacizumab in active progressive proliferative diabetic retinopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 1699–1705. [Google Scholar] [CrossRef]
- Arevalo, J.F.; Maia, M.; Flynn, H.W., Jr.; Saravia, M.; Avery, R.L.; Wu, L.; Eid Farah, M.; Pieramici, D.J.; Berrocal, M.H.; Sanchez, J.G. Tractional retinal detachment following intravitreal bevacizumab (Avastin®) in patients with severe proliferative diabetic retinopathy. Br. J. Ophthalmol. 2008, 92, 213–216. [Google Scholar] [CrossRef]
- Pearson, R.V.; McLeod, D.; Gregor, Z.J. Removal of silicone oil following diabetic vitrectomy. Br. J. Ophthalmol. 1993, 77, 204–207. [Google Scholar] [CrossRef]
- Barca, F.; Caporossi, T.; Rizzo, S. Silicone oil: Different physical properties and clinical applications. BioMed Res. Int. 2014, 502143. [Google Scholar] [CrossRef]
- Yorston, D.; Wickham, L.; Benson, S.; Bunce, C.; Sheard, R.; Charteris, D. Predictive clinical features and outcomes of vitrectomy for proliferative diabetic retinopathy. Br. J. Ophthalmol. 2008, 92, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; You, Y.; Du, W.; Zhao, C.; Li, J.; Mao, J.; Chen, H.; Cheng, L. Ocular pharmacokinetics of bevacizumab in vitrectomized eyes with silicone oil tamponade. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5221–5226. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group I (n = 26) | Group II (n = 20) | p-Value | |
|---|---|---|---|
| Age (years) | 54.77 ± 4.97 | 54.60 ± 9.19 | 0.283 1 |
| Sex (n, %) | |||
| Male | 14 (53.8%) | 12 (60.0%) | 0.454 2 |
| Female | 12 (46.2%) | 8 (40.0%) | |
| Laterality (n, %) | |||
| Right | 6 (23.1%) | 4 (20.0%) | 0.547 2 |
| Left | 20 (76.9%) | 16 (80.0%) | |
| HTN (n, %) | 8 (30.8%) | 4 (20.0%) | 0.316 2 |
| Duration of DM (years) | 7.60 ± 6.02 | 5.80 ± 7.90 | 0.074 1 |
| Preop hemoglobin A1C (%) | 8.17 ± 0.91 | 9.56 ± 2.61 | 0.022 1 |
| PRP (n, %) | 14 (53.8%) | 8 (40.0%) | 0.263 2 |
| Preop IOP (mmHg) | 15.25 ± 3.34 | 17.19 ± 6.41 | 0.739 1 |
| Preop BCVA (logMAR [Snellen]) | 1.03 ± 0.69 [20/214] | 1.42 ± 1.03 [20/526] | 0.245 1 |
| Preop CMT (μm) | 493.92 ± 219.63 | 435.80 ± 125.22 | 0.723 1 |
| Preop IVB injections (n) | 1.40 ± 0.82 | 1.08 ± 0.27 | 0.172 1 |
| Postop hemoglobin A1C (%) | 7.89 ± 1.76 | 6.94 ± 0.33 | 0.328 1 |
| Combine cataract surgery (n, %) | 16 (61.5%) | 16 (80.0%) | 0.153 2 |
| SO volume (cc) | 4.22 ± 0.31 | 4.46 ± 0.60 | 0.368 1 |
| Duration of SO (months) | 4.46 ± 2.70 | 4.00 ± 1.72 | 0.500 1 |
| Group I 1 (n = 26) | Group II 1 (n = 20) | p-Value 2 | |
|---|---|---|---|
| BCVA (logMAR [Snellen]) | |||
| Preop | 1.03 ± 0.69 [20/214] | 1.42 ± 1.03 [20/526] | 0.245 |
| POD 1 month | 0.90 ± 0.67 [20/159] | 1.04 ± 0.61 [20/219] | 0.323 |
| Before SO removal | 0.90 ± 0.46 [20/159] | 1.18 ± 0.66 [20/303] | 0.240 |
| 1 month after SO removal | 0.61 ± 0.46 * [20/81] | 0.74 ± 0.46 * [20/110] | 0.137 |
| POD 12 month | 0.47 ± 0.51 * [20/59] | 0.43 ± 0.52 * [20/54] | 0.720 |
| ΔBCVA (logMAR) | |||
| POD 1 month | −0.13 ± 0.77 | −0.38 ± 0.88 | 0.266 |
| Before SO removal | −0.13 ± 0.66 | −0.24 ± 0.76 | 0.722 |
| After SO removal | −0.42 ± 0.72 | −0.68 ± 0.77 | 0.304 |
| POD 12 month | −0.56 ± 0.80 | −0.99 ± 0.73 | 0.029 |
| CMT (μm) | |||
| Preop | 493.92 ± 219.63 | 435.80 ± 125.22 | 0.723 |
| POD 1 month | 471.54 ± 120.14 | 363.40 ± 59.57 * | 0.001 |
| Before SO removal | 382.08 ± 73.63 | 351.00 ± 41.17 * | 0.399 |
| 1 month after SO removal | 357.31 ± 84.21 * | 314.00 ± 38.53 * | 0.092 |
| POD 12 month | 325.00 ± 77.71 * | 298.30 ± 29.58 * | 0.424 |
| ΔCMT (μm) | |||
| POD 1 month | −22.39 ± 203.99 | −72.40 ± 139.35 | 0.027 |
| Before SO removal | −111.85 ± 202.61 | −84.80 ± 139.98 | 0.929 |
| After SO removal | −136.62 ± 243.70 | −121.80 ± 135.81 | 0.351 |
| POD 12 month | −168.92 ± 239.76 | −137.50 ± 132.67 | 0.657 |
| Group I (n = 26) | Group II (n = 20) | p-Value | |
|---|---|---|---|
| Postop complication | 3 (11.5%) | 2 (10.0%) | 0.627 1 |
| IOP increase | 0 | 2 | |
| Vitreous hemorrhage | 1 | 0 | |
| Fibrovascular membrane proliferation | 2 | 0 | |
| 12-month Postop hemoglobin A1c (%) | 7.89 ± 1.76 | 6.94 ± 0.33 | 0.328 2 |
| IVB injections after SO removal (n, %) | 6 (23.1%) | 0 (0.0%) | 0.025 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, S.K.; Lee, M.-W.; Lee, Y.-H. Effect of Intrasilicone Bevacizumab Injection in Diabetic Tractional Retinal Detachment Surgery: A Retrospective Case-Control Study. J. Clin. Med. 2020, 9, 3114. https://doi.org/10.3390/jcm9103114
Baek SK, Lee M-W, Lee Y-H. Effect of Intrasilicone Bevacizumab Injection in Diabetic Tractional Retinal Detachment Surgery: A Retrospective Case-Control Study. Journal of Clinical Medicine. 2020; 9(10):3114. https://doi.org/10.3390/jcm9103114
Chicago/Turabian StyleBaek, Seung Kook, Min-Woo Lee, and Young-Hoon Lee. 2020. "Effect of Intrasilicone Bevacizumab Injection in Diabetic Tractional Retinal Detachment Surgery: A Retrospective Case-Control Study" Journal of Clinical Medicine 9, no. 10: 3114. https://doi.org/10.3390/jcm9103114
APA StyleBaek, S. K., Lee, M.-W., & Lee, Y.-H. (2020). Effect of Intrasilicone Bevacizumab Injection in Diabetic Tractional Retinal Detachment Surgery: A Retrospective Case-Control Study. Journal of Clinical Medicine, 9(10), 3114. https://doi.org/10.3390/jcm9103114