Effects of Prevalent and Incident Atrial Fibrillation on Renal Outcome, Cardiovascular Events, and Mortality in Patients with Chronic Kidney Disease

Abstract
1. Introduction
2. Experimental Section
2.1. Data Source
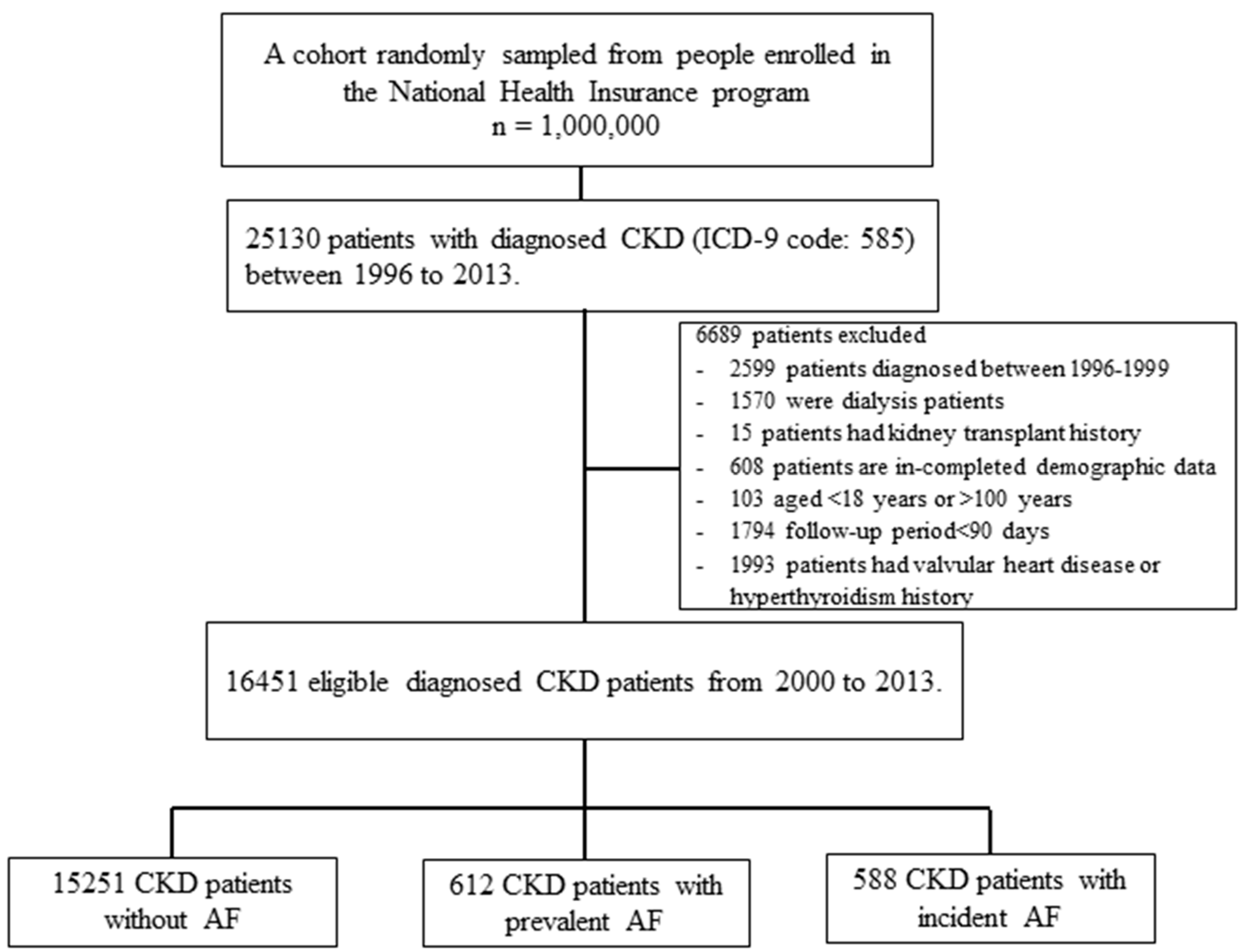
2.2. Study Cohort and Design
2.3. Study Outcomes and Relevant Confounding Variables
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Participants
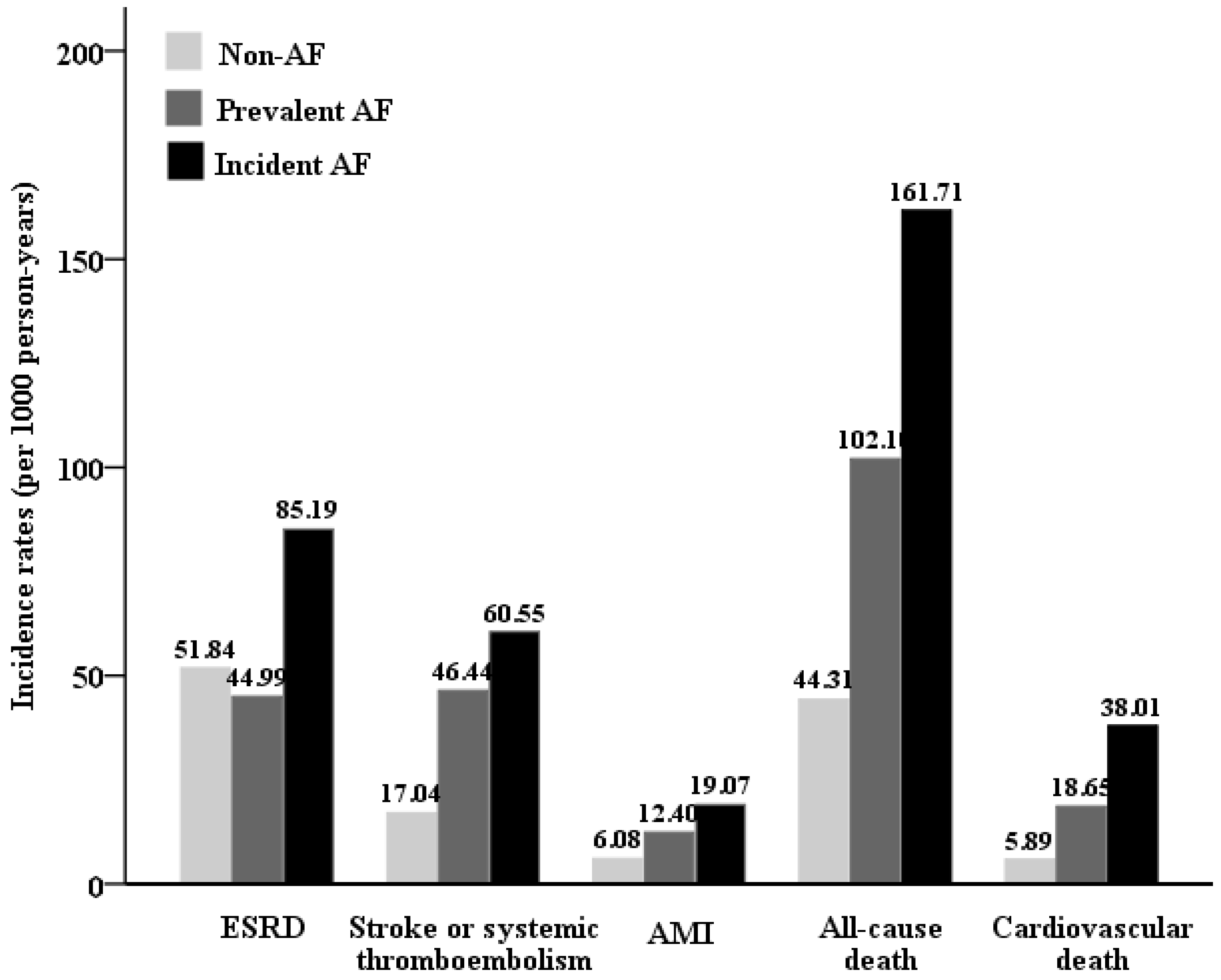
3.2. Rates of Outcome Events by AF Status
3.3. Association of AF Status with Subsequent ESRD
3.4. Association of AF Status with Subsequent All-Cause and CV Deaths
3.5. Association of AF Status with Subsequent Cardiovascular Events
3.6. Subgroup Analyses
3.7. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Fullerton, H.J. Heart disease and stroke statistics—2012 update: A report from the American Heart Association. Circulation 2012, 125, e2–e220. [Google Scholar]
- Stewart, S.; Hart, C.L.; Hole, D.J.; McMurray, J.J. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am. J. Med. 2002, 113, 359–364. [Google Scholar] [CrossRef]
- Stewart, S.; MacIntyre, K.; MacLeod, M.; Bailey, A.; Capewell, S.; McMurray, J. Trends in hospital activity, morbidity and case fatality related to atrial fibrillation in Scotland, 1986–1996. Eur. Hear J. 2001, 22, 693–701. [Google Scholar] [CrossRef]
- Lee, W.C.; Lamas, G.A.; Balu, S.; Spalding, J.; Wang, Q.; Pashos, C.L. Direct treatment cost of atrial fibrillation in the elderly American population: A Medicare perspective. J. Med. Econ. 2008, 11, 281–298. [Google Scholar] [CrossRef]
- Bansal, N.; Xie, D.; Tao, K.; Chen, J.; Deo, R.; Horwitz, E.; Hsu, C.-Y.; Kallem, R.K.; Keane, M.G.; Lora, C.M.; et al. Atrial Fibrillation and Risk of ESRD in Adults with CKD. Clin. J. Am. Soc. Nephrol. 2016, 11, 1189–1196. [Google Scholar] [CrossRef]
- Coresh, J.; Selvin, E.; Stevens, L.A.; Manzi, J.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Levey, A.S. Prevalence of Chronic Kidney Disease in the United States. JAMA 2007, 298, 2038. [Google Scholar] [CrossRef]
- Di Lullo, L.; House, A.; Gorini, A.; Santoboni, A.; Russo, D.; Ronco, C. Chronic kidney disease and cardiovascular complications. Heart Fail. Rev. 2015, 20, 259–272. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; Perrone, R.D.; Lau, J.; Eknoyan, G. National Kidney Foundation Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Ann. Intern. Med. 2003, 139, 137–147. [Google Scholar] [CrossRef]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; Parfrey, P. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Su, Y.-C.; Lee, C.-C.; Huang, Y.-S.; Hwang, S.-J. Chronic Kidney Disease Itself Is a Causal Risk Factor for Stroke beyond Traditional Cardiovascular Risk Factors: A Nationwide Cohort Study in Taiwan. PLoS ONE 2012, 7, e36332. [Google Scholar] [CrossRef]
- Alonso, A.; Lopez, F.L.; Matsushita, K.; Loehr, L.R.; Agarwal, S.K.; Chen, L.Y.; Soliman, E.Z.; Astor, B.C.; Coresh, J. Chronic Kidney Disease is Associated with the Incidence of Atrial Fibrillation: The Atherosclerosis Risk in Communities (ARIC) Study. Circulation 2011, 123, 2946–2953. [Google Scholar] [CrossRef]
- Ananthapanyasut, W.; Napan, S.; Rudolph, E.H.; Harindhanavudhi, T.; Ayash, H.; Guglielmi, K.E.; Lerma, E.V. Prevalence of atrial fibrillation and its predictors in nondialysis patients with chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2010, 5, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Baber, U.; Howard, V.J.; Halperin, J.L.; Soliman, E.Z.; Zhang, X.; McClellan, W.; Muntner, P. Association of chronic kidney disease with atrial fibrillation among adults in the United States: Reasons for Geographic and Racial Differences in Stroke (REGARDS) study. Circ. Arrhythm. Electrophysiol. 2011, 4, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-Y.; Chiu, Y.-W.; Chang, J.-S.; Lin, H.-L.; Lee, C.T.-C.; Chiu, G.-F.; Kuo, M.-C.; Wu, M.-T.; Chen, H.-C.; Hwang, S.-J. Association of prescribed Chinese herbal medicine use with risk of end-stage renal disease in patients with chronic kidney disease. Kidney Int. 2015, 88, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-H.; Lee, Y.-C.; Tsai, C.-T.; Chang, S.-N.; Chung, Y.-H.; Lin, M.-S.; Lin, J.-W.; Lai, M.-S. Continuation of statin therapy and a decreased risk of atrial fibrillation/flutter in patients with and without chronic kidney disease. Atherosclerosis 2014, 232, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Weng, S.-C.; Wu, C.-L.; Kor, C.-T.; Chiu, P.-F.; Wu, M.-J.; Chang, C.-C.; Tarng, D.-C. Migraine and subsequent chronic kidney disease risk: A nationwide population-based cohort study. BMJ Open 2017, 7, e018483. [Google Scholar] [CrossRef]
- Hsu, T.-W.; Liu, J.-S.; Hung, S.-C.; Kuo, K.-L.; Chang, Y.-K.; Chen, Y.-C.; Hsu, C.-C.; Tarng, D.-C. Renoprotective Effect of Renin-Angiotensin-Aldosterone System Blockade in Patients with Predialysis Advanced Chronic Kidney Disease, Hypertension, and Anemia. JAMA Intern. Med. 2014, 174, 347. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Murray, K.T. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2014, 64, e1–e76. [Google Scholar] [CrossRef]
- McCaffrey, D.F.; Griffin, B.A.; Almirall, D.; Slaughter, M.E.; Ramchand, R.; Burgette, L.F. A Tutorial on Propensity Score Estimation for Multiple Treatments Using Generalized Boosted Models. Stat. Med. 2013, 32, 3388–3414. [Google Scholar] [CrossRef]
- Hsu, P.-K.; Kor, C.-T.; Hsieh, Y.-P. Effect of New-Onset Diabetes Mellitus on Renal Outcomes and Mortality in Patients with Chronic Kidney Disease. J. Clin. Med. 2018, 7, 550. [Google Scholar] [CrossRef]
- Olesen, J.B.; Lip, G.Y.; Kamper, A.-L.; Hommel, K.; Køber, L.; Lane, D.A.; Lindhardsen, J.; Gislason, G.H.; Torp-Pedersen, C. Stroke and Bleeding in Atrial Fibrillation with Chronic Kidney Disease. N. Engl. J. Med. 2012, 367, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Xie, D.; Sha, D.; Appel, L.J.; Deo, R.; Feldman, H.I.; He, J.; Jamerson, K.; Kusek, J.W.; Messe, S.; et al. Cardiovascular Events after New-Onset Atrial Fibrillation in Adults with CKD: Results from the Chronic Renal Insufficiency Cohort (CRIC) Study. J. Am. Soc. Nephrol. 2018, 29, 2859–2869. [Google Scholar] [CrossRef] [PubMed]
- Hillege, H.L.; Nitsch, D.; Pfeffer, M.A.; Swedberg, K.; McMurray, J.J.; Yusuf, S.; de Zeeuw, D. Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) Investigators: Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation 2006, 113, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Hillege, H.L.; van Gilst, W.H.; van Veldhuisen, D.J.; Navis, G.; Grobbee, D.E.; De Graeff, P.A.; De Zeeuw, D. CATS Randomized Trial: Accelerated decline and prognostic impact of renal function after myocardial infarction and the benefits of ACE inhibition: The CATS randomized trial. Eur. Heart J. 2003, 24, 412–420. [Google Scholar] [CrossRef]
- Watanabe, H.; Watanabe, T.; Sasaki, S.; Nagai, K.; Roden, D.M.; Aizawa, Y. Close bidirectional relationship between chronic kidney disease and atrial fibrillation: The Niigata preventive medicine study. Am. Hear J. 2009, 158, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Fan, D.; Hsu, C.Y.; Ordonez, J.D.; Marcus, G.M.; Go, A.S. Incident atrial fibrillation and risk of end-stage renal disease in adults with chronic kidney disease. Circulation 2013, 127, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Soliman, E.Z.; Safford, M.M.; Muntner, P.; Khodneva, Y.; Dawood, F.Z.; Zakai, N.A.; Thacker, E.L.; Judd, S.; Howard, V.J.; Howard, G.; et al. Atrial Fibrillation and the Risk of Myocardial Infarction. JAMA Intern. Med. 2014, 174, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Wolf, P.A.; D’Agostino, R.B.; Silbershatz, H.; Kannel, W.B.; Levy, D. Impact of atrial fibrillation on the risk of death: The Framingham Heart Study. Circulation 1998, 98, 946–952. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, W.T.; Salahuddin, T.; Broughton, S.T.; Soliman, E.Z. Atrial Fibrillation and Cardiovascular Outcomes in the Elderly. Pacing Clin. Electrophysiol. 2016, 39, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Potpara, T.S.; Polovina, M.M.; Licina, M.M.; Marinkovic, J.M.; Lip, G.Y. Predictors and prognostic implications of incident heart failure following the first diagnosis of atrial fibrillationin patients with structurally normal hearts: The Belgrade Atrial Fibrillation Study. Eur. J. Heart Fail. 2013, 15, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Odutayo, A.; Wong, C.X.; Hsiao, A.J.; Hopewell, S.; Altman, D.G.; Emdin, C.A. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: Systematic review and meta-analysis. BMJ 2016, 354, 4482. [Google Scholar] [CrossRef] [PubMed]
- Genovesi, S.; Vincenti, A.; Rossi, E.; Pogliani, D.; Acquistapace, I.; Stella, A.; Valsecchi, M.G. Atrial Fibrillation and Morbidity and Mortality in a Cohort of Long-term Hemodialysis Patients. Am. J. Kidney Dis. 2008, 51, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.J.; Ou, S.M.; Chao, P.W.; Kuo, S.C.; Lee, Y.J.; Yang, C.Y.; Chen, Y.T. Risks of death and stroke in patients undergoing hemodialysis with new-onset atrial fibrillation: A competing-risk analysis of a nationwide cohort. Circulation 2016, 133, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Fan, D.; Hsu, C.; Ordonez, J.D.; Go, A.S. Incident Atrial Fibrillation and Risk of Death in Adults With Chronic Kidney Disease. J. Am. Hear. Assoc. 2014, 3, e001303. [Google Scholar] [CrossRef] [PubMed]
- Massicotte-Azarniouch, D.; Kuwornu, J.P.; Lam, N.N.; Molnar, A.O.; McCallum, M.K.; Garg, A.X.; Carrero, J.-J.; Zimmerman, D.; Sood, M.M. Incident Atrial Fibrillation and the Risk of Congestive Heart Failure, Myocardial Infarction, End-Stage Kidney Disease, and Mortality Among Patients With a Decreased Estimated GFR. Am. J. Kidney Dis. 2018, 71, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Faul, C.; Amaral, A.P.; Oskouei, B.; Hu, M.-C.; Sloan, A.; Isakova, T.; Gutierrez, O.M.; Aguillon-Prada, R.; Lincoln, J.; Hare, J.M.; et al. FGF23 induces left ventricular hypertrophy. J. Clin. Investig. 2011, 121, 4393–4408. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-C.; Su, H.-M.; Hung, C.-C.; Chang, J.-M.; Liu, W.-C.; Tsai, J.-C.; Lin, M.-Y.; Hwang, S.-J.; Chen, H.-C. Echocardiographic Parameters are Independently Associated with Rate of Renal Function Decline and Progression to Dialysis in Patients with Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2011, 6, 2750–2758. [Google Scholar] [CrossRef] [PubMed]
- Burstein, B.; Calderone, A.; Qi, X.-Y.; Yeh, Y.-H.; Nattel, S. Atrial cardiomyocyte tachycardia alters cardiac fibroblast function: A novel consideration in atrial remodeling. Cardiovasc. Res. 2007, 76, 442–452. [Google Scholar] [CrossRef] [PubMed]
- Bukowska, A.; Lendeckel, U.; Krohn, A.; Keilhoff, G.; Have, S.T.; Neumann, K.H.; Goette, A. Atrial fibrillation down-regulates renal neutral endopeptidase expression and induces profibrotic pathways in the kidney. Europace 2008, 10, 1212–1217. [Google Scholar] [CrossRef] [PubMed][Green Version]



{kind=link}
{kind=link}
| CKD Cohort | Maximum Standardization Difference between Groups | |||||
|---|---|---|---|---|---|---|
| Non-AF | Prevalent AF | Incident AF | p-Value | Before IPW a (%) | After IPW a (%) | |
| Sample size | 15,251 | 612 | 588 | -- | -- | -- |
| Age, years | 65 ± 14 | 76 ± 10 | 72 ± 10 | <0.001 | 0.746 | 0.161 |
| Gender, Male | 9076 (59.51%) | 397 (64.87%) | 337 (57.31%) | 0.015 | 0.111 | 0.098 |
| Monthly income, NTD | 14,144.97 ± 13,893.61 | 10,331.85 ± 11,240.98 | 10,067.77 ± 10,329.03 | <0.001 | 0.340 | 0.119 |
| Geographical location | ||||||
| Northern | 6509 (42.68%) | 264 (43.14%) | 246 (41.84%) | 0.894 | 0.028 | 0.093 |
| Central | 2799 (18.35%) | 112 (18.3%) | 121 (20.58%) | 0.392 | 0.073 | 0.088 |
| Southern | 5521 (36.2%) | 207 (33.82%) | 197 (33.5%) | 0.211 | 0.073 | 0.035 |
| Eastern | 422 (2.77%) | 29 (4.74%) | 24 (4.08%) | 0.004 | 0.094 | 0.042 |
| Comorbidities | ||||||
| Coronary artery disease | 2881 (18.89%) | 254 (41.5%) | 197 (33.5%) | <0.001 | 0.559 | 0.127 |
| Chronic obstructive pulmonary disease | 1451 (9.51%) | 137 (22.39%) | 99 (16.84%) | <0.001 | 0.424 | 0.081 |
| Cancer | 1119 (7.34%) | 50 (8.17%) | 32 (5.44%) | 0.156 | 0.116 | 0.021 |
| Liver Cirrhosis | 361 (2.37%) | 16 (2.61%) | 5 (0.85%) | 0.050 | 0.117 | 0.140 |
| Dementia | 379 (2.49%) | 30 (4.9%) | 16 (2.72%) | 0.001 | 0.152 | 0.113 |
| Rheumatoid disease | 317 (2.08%) | 14 (2.29%) | 9 (1.53%) | 0.609 | 0.040 | 0.021 |
| Peptic ulcer disease | 2934 (19.24%) | 151 (24.67%) | 127 (21.6%) | 0.002 | 0.137 | 0.046 |
| CHA2DS2-VASc score | 3 ± 2 | 4 ± 2 | 3 ± 1 | <0.001 | 0.806 | 0.102 |
| 0 | 1159 (7.6%) | 8 (1.31%) | 8 (1.36%) | <0.001 | ||
| 1 | 2903 (19.03%) | 35 (5.72%) | 40 (6.8%) | <0.001 | ||
| 2 | 3674 (24.09%) | 79 (12.91%) | 124 (21.09%) | <0.001 | ||
| 3 | 3360 (22.03%) | 141 (23.04%) | 152 (25.85%) | 0.081 | ||
| 4 | 2317 (15.19%) | 140 (22.88%) | 135 (22.96%) | <0.001 | ||
| 5 | 1200 (7.87%) | 109 (17.81%) | 81 (13.78%) | <0.001 | ||
| ≥6 | 638 (4.18%) | 100 (16.34%) | 48 (8.16%) | <0.001 | ||
| Long-term medication use | ||||||
| ACEI/ARB | 6537 (42.86%) | 383 (62.58%) | 288 (48.98%) | <0.001 | 0.396 | 0.074 |
| beta-blocker | 4948 (32.44%) | 324 (52.94%) | 237 (40.31%) | <0.001 | 0.432 | 0.125 |
| Diuretics | 4192 (27.49%) | 328 (53.59%) | 233 (39.63%) | <0.001 | 0.573 | 0.083 |
| Statin | 4133 (27.1%) | 185 (30.23%) | 139 (23.64%) | 0.037 | 0.194 | 0.117 |
| NSAIDs | 2286 (14.99%) | 131 (21.41%) | 107 (18.2%) | <0.001 | 0.179 | 0.012 |
| Pentoxifylline | 1028 (6.74%) | 63 (10.29%) | 50 (8.5%) | 0.001 | 0.139 | 0.114 |
| ESA | 130 (0.85%) | 3 (0.49%) | 3 (0.51%) | 0.430 | 0.047 | 0.090 |
| Aspirin/clopidogrel | 3929 (25.76%) | 362 (59.15%) | 203 (34.52%) | <0.001 | 0.748 | 0.105 |
| Warfarin | 141 (0.92%) | 76 (12.42%) | 8 (1.36%) | <0.001 | 0.99 | 0.029 |
| Annual frequency of medical visits | 30 ± 20 | 34 ± 20 | 34 ± 22 | <0.001 | 0.218 | 0.080 |
| Outcome | Event | IR (95% CI) | Weighted Time-Dependent Cox Model | |||||
|---|---|---|---|---|---|---|---|---|
| cHR (95% CI) | p-Value | aHR (95% CI) | p-value | aHR (95% CI) | p-Value | |||
| ESRD | ||||||||
| Non-AF | 3440 | 51.84 (50.11–53.57) | 1 | 1 | 0.34 (0.32–0.36) | <0.0001 | ||
| Prevalent AF | 89 | 44.99 (35.64–54.34) | 1.29 (1.22–1.36) | <0.001 | 1.40 (1.32–1.48) | <0.001 | 0.48 (0.45–0.51) | <0.0001 |
| Incident AF | 95 | 85.19 (68.06–102.32) | 3.05 (2.88–3.23) | <0.001 | 2.91 (2.74–3.09) | <0.001 | 1 | |
| Stroke or systemic thromboembolism | ||||||||
| Non-AF | 1247 | 17.04 (16.09–17.98) | 1 | 1 | 0.61 (0.56–0.66) | <0.0001 | ||
| Prevalent AF | 89 | 46.44 (36.79–56.09) | 2.02 (1.88–2.16) | <0.001 | 1.89 (1.77–2.03) | <0.001 | 1.14 (1.05–1.25) | 0.002 |
| Incident AF | 79 | 60.55 (47.19–73.9) | 2.51 (2.33–2.72) | <0.001 | 1.67 (1.54–1.81) | <0.001 | 1 | |
| Acute myocardial infarction | ||||||||
| Non-AF | 461 | 6.08 (5.52–6.63) | 1 | 1 | 0.50 (0.44–0.57) | <0.0001 | ||
| Prevalent AF | 26 | 12.4 (7.64–17.17) | 1.34 (1.18–1.52) | <0.001 | 1.24 (1.09–1.41) | 0.001 | 0.62 (0.53–0.72) | <0.0001 |
| Incident AF | 28 | 19.07 (12.01–26.13) | 3.02 (2.67–3.41) | <0.001 | 1.99 (1.75–2.27) | <0.001 | 1 | |
| All-cause mortality | ||||||||
| Non-AF | 3399 | 44.31 (42.82–45.8) | 1 | 1 | 0.46 (0.44–0.49) | <0.0001 | ||
| Prevalent AF | 219 | 102.1 (88.58–115.62) | 1.83 (1.74–1.92) | <0.001 | 1.64 (1.56–1.72) | <0.001 | 0.76 (0.72–0.81) | <0.0001 |
| Incident AF | 251 | 161.71 (141.7–181.72) | 3.11 (2.96–3.27) | <0.001 | 2.17 (2.06–2.29) | <0.001 | 1 | |
| Cardiovascular mortality | ||||||||
| Non-AF | 452 | 5.89 (5.35–6.44) | 1 | 1 | 0.22 (0.19–0.25) | <0.0001 | ||
| Prevalent AF | 40 | 18.65 (12.87–24.43) | 3.18 (2.83–3.57) | <0.001 | 2.95 (2.62–3.32) | <0.001 | 0.64 (0.57–0.72) | <0.0001 |
| Incident AF | 59 | 38.01 (28.31–47.71) | 6.81 (6.08–7.63) | <0.001 | 4.61 (4.09–5.20) | <0.001 | 1 | |
| Subgroup | ESRD | Stroke or Systemic Thromboembolism | AMI | All-Cause Mortality | Cardiovascular Mortality | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Prevalent AF vs. Non-AF | Incident AF vs. Non-AF | Prevalent AF vs. Non-AF | Incident AF vs. Non-AF | Prevalent AF vs. Non-AF | Incident AF vs. Non-AF | Prevalent AF vs. Non-AF | Incident AF vs. Non-AF | Prevalent AF vs. Non-AF | Incident AF vs. Non-AF | |
| Age | ||||||||||
| Age < 65 | 1.48 (1.36–1.62) | 3.02 (2.75–3.31) | 1.93 (1.75–2.13) | 1.67 (1.52–1.83) | 1.68 (1.49–1.89) | 2.18 (1.97–2.42) | 1.98 (1.71–2.29) | 2.07 (1.83–2.33) | 3.27 (2.47–4.33) | 6.92 (5.01–9.56) |
| Age ≥ 65 | 1.30 (1.20–1.41) | 2.86 (2.63–3.11) | 1.88 (1.72–2.05) | 1.7 (1.53–1.89) | 1.11 (0.95–1.30) | 1.47 (1.23–1.77) | 1.78 (1.68–1.88) | 2.25 (2.12–2.40) | 2.92 (2.55–3.35) | 5.20 (4.51–5.98) |
| p for interaction | 0.029 | <0.001 | 0.104 | 0.650 | 0.037 | <0.001 | <0.001 | 0.529 | 0.436 | 0.610 |
| Gender | ||||||||||
| Female | 1.48 (1.36–1.61) | 3.27 (2.99–3.57) | 1.66 (1.45–1.89) | 2.15 (1.89–2.44) | 0.98 (0.76–1.26) | 2.20 (1.75–2.77) | 1.56 (1.44–1.70) | 2.72 (2.51–2.96) | 3.64 (3.05–4.35) | 8.28 (6.95–9.87) |
| Male | 1.27 (1.18–1.38) | 2.92 (2.68–3.17) | 2.08 (1.90–2.26) | 1.34 (1.20–1.49) | 1.43 (1.22–1.66) | 1.89 (1.61–2.21) | 1.69 (1.58–1.80) | 1.93 (1.8–2.07) | 2.70 (2.28–3.20) | 2.96 (2.47–3.55) |
| p for interaction | 0.005 | 0.119 | <0.001 | <0.001 | 0.013 | 0.012 | 0.430 | <0.001 | 0.004 | <0.001 |
| CHA2DS2-VASc Score | ||||||||||
| CHA2DS2-VASc Score ≤3 | 1.65 (1.54–1.77) | 3.37 (3.13–3.62) | 2.40 (2.18–2.64) | 2.31 (2.09–2.55) | 1.92 (1.62–2.28) | 3.52 (2.98–4.14) | 1.96 (1.83–2.10) | 2.13 (1.99–2.28) | 3.17 (2.67–3.77) | 5.78 (4.87–6.85) |
| CHA2DS2-VASc Score >3 | 1.02 (0.92–1.13) | 3.23 (2.9–3.59) | 1.54 1.38–1.72) | 2.04 (1.79–2.34) | 1.04 (0.60–1.78) | 2.34 (1.89–2.89) | 1.44 (1.33–1.56) | 3.10 (2.87–3.35) | 1.56 (1.28–1.89) | 8.41 (7.12–9.93) |
| p for interaction | <0.001 | 0.408 | <0.001 | 0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Renin-angiotensin system inhibitors use | ||||||||||
| Non-user | 1.47 (1.34–1.6) | 2.46 (2.23–2.71) | 1.99 (1.87–2.11) | 2.03 (1.9–2.18) | 1.58 (1.47–1.69) | 2.68 (2.5–2.88) | 1.68 (1.57–1.81) | 2.57 (2.39–2.77) | 4.79 (3.99–5.76) | 4.97 (4.08–6.06) |
| User | 1.44 (1.33–1.56) | 3.52 (3.24–3.81) | 1.29 (1.16–1.43) | 2.09 (1.88–2.33) | 1.18 (0.74–1.87) | 1.03 (0.54–1.98) | 1.76 (1.63–1.89) | 2.02 (1.87–2.18) | 2.07 (1.75–2.46) | 5.27 (4.51–6.16) |
| p for interaction | 0.909 | <0.001 | <0.001 | <0.001 | 0.7437 | <0.001 | 0.4018 | 0.3070 | <0.001 | 0.847 |
| Outcome | Weighted Time-Dependent Cox Model | |||||
|---|---|---|---|---|---|---|
| aHR a (95% CI) | p-Value | aHR b (95% CI) | p-Value | aHR c (95% CI) | p-Value | |
| ESRD | ||||||
| Non-AF | 1 | 1 | ||||
| Prevalent AF | 1.41 (1.33–1.49) | <0.001 | 1.44 (1.36–1.52) | <0.0001 | ||
| Incident AF | 2.85 (2.68–3.02) | <0.001 | 2.90 (2.73–3.08) | <0.0001 | ||
| Stroke | ||||||
| Non-AF | 1 | 1 | ||||
| Prevalent AF | 1.90 (1.77–2.04) | <0.001 | 1.88 (1.75–2.02) | <0.0001 | ||
| Incident AF | 1.86 (1.72–2.02) | <0.001 | 1.82 (1.67–1.97) | <0.0001 | ||
| Acute myocardial infarction | ||||||
| Non-AF | 1 | 1 | ||||
| Prevalent AF | 1.27 (1.11–1.44) | <0.001 | 1.2 (1.05–1.36) | 0.005 | ||
| Incident AF | 2.22 (1.95–2.53) | <0.001 | 2.09 (1.84–2.38) | <0.0001 | ||
| All-cause mortality | ||||||
| Non-AF | 1 | 1 | ||||
| Prevalent AF | 1.71 (1.63–1.80) | <0.001 | 1.72 (1.63–1.80) | <0.0001 | ||
| Incident AF | 2.51 (2.38–2.65) | <0.001 | 2.49 (2.36–2.62) | <0.0001 | ||
| CV mortality | ||||||
| Non-AF | 1 | 1 | ||||
| Prevalent AF | 2.88 (2.56–3.23) | <0.001 | 3.29 (2.91–3.71) | <0.0001 | ||
| Incident AF | 5.08 (4.51–5.72) | <0.001 | 4.6 2(4.10–5.21) | <0.0001 | ||
| Stroke (excluding TIA) | ||||||
| Non-AF | 1 | 1 | 1 | |||
| Prevalent AF | 2.02 (1.88–2.18) | <0.0001 | 1.82 (1.69–1.96) | <0.0001 | 2.02 (1.88–2.17) | <0.0001 |
| Incident AF | 1.87 (1.72–2.03) | <0.0001 | 1.49 (1.36–1.62) | <0.0001 | 1.66 (1.53–1.81) | <0.0001 |
| Stroke (excluding pulmonary embolism) | ||||||
| Non-AF | 1 | 1 | 1 | 1 | ||
| Prevalent AF | 2.10 (1.95–2.26) | <0.0001 | 1.87 (1.73–2.02) | 2.10 (1.95–2.26) | 2.05 (1.91–2.21) | <0.0001 |
| Incident AF | 1.95 (1.79–2.13) | <0.0001 | 1.60 (1.46–1.75) | 1.95 (1.79–2.13) | 1.78 (1.63–1.94) | <0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, H.-H.; Kor, C.-T.; Hsieh, Y.-P.; Chiu, P.-F. Effects of Prevalent and Incident Atrial Fibrillation on Renal Outcome, Cardiovascular Events, and Mortality in Patients with Chronic Kidney Disease. J. Clin. Med. 2019, 8, 1378. https://doi.org/10.3390/jcm8091378
Hsu H-H, Kor C-T, Hsieh Y-P, Chiu P-F. Effects of Prevalent and Incident Atrial Fibrillation on Renal Outcome, Cardiovascular Events, and Mortality in Patients with Chronic Kidney Disease. Journal of Clinical Medicine. 2019; 8(9):1378. https://doi.org/10.3390/jcm8091378
Chicago/Turabian StyleHsu, Hsin-Hui, Chew-Teng Kor, Yao-Peng Hsieh, and Ping-Fang Chiu. 2019. "Effects of Prevalent and Incident Atrial Fibrillation on Renal Outcome, Cardiovascular Events, and Mortality in Patients with Chronic Kidney Disease" Journal of Clinical Medicine 8, no. 9: 1378. https://doi.org/10.3390/jcm8091378
APA StyleHsu, H.-H., Kor, C.-T., Hsieh, Y.-P., & Chiu, P.-F. (2019). Effects of Prevalent and Incident Atrial Fibrillation on Renal Outcome, Cardiovascular Events, and Mortality in Patients with Chronic Kidney Disease. Journal of Clinical Medicine, 8(9), 1378. https://doi.org/10.3390/jcm8091378