Presence of Chronic Obstructive Pulmonary Disease (COPD) Impair Survival in Lung Cancer Patients Receiving Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor (EGFR-TKI): A Nationwide, Population-Based Cohort Study

 , , ,
, , ,
Abstract
1. Introduction
2. Material and Methods
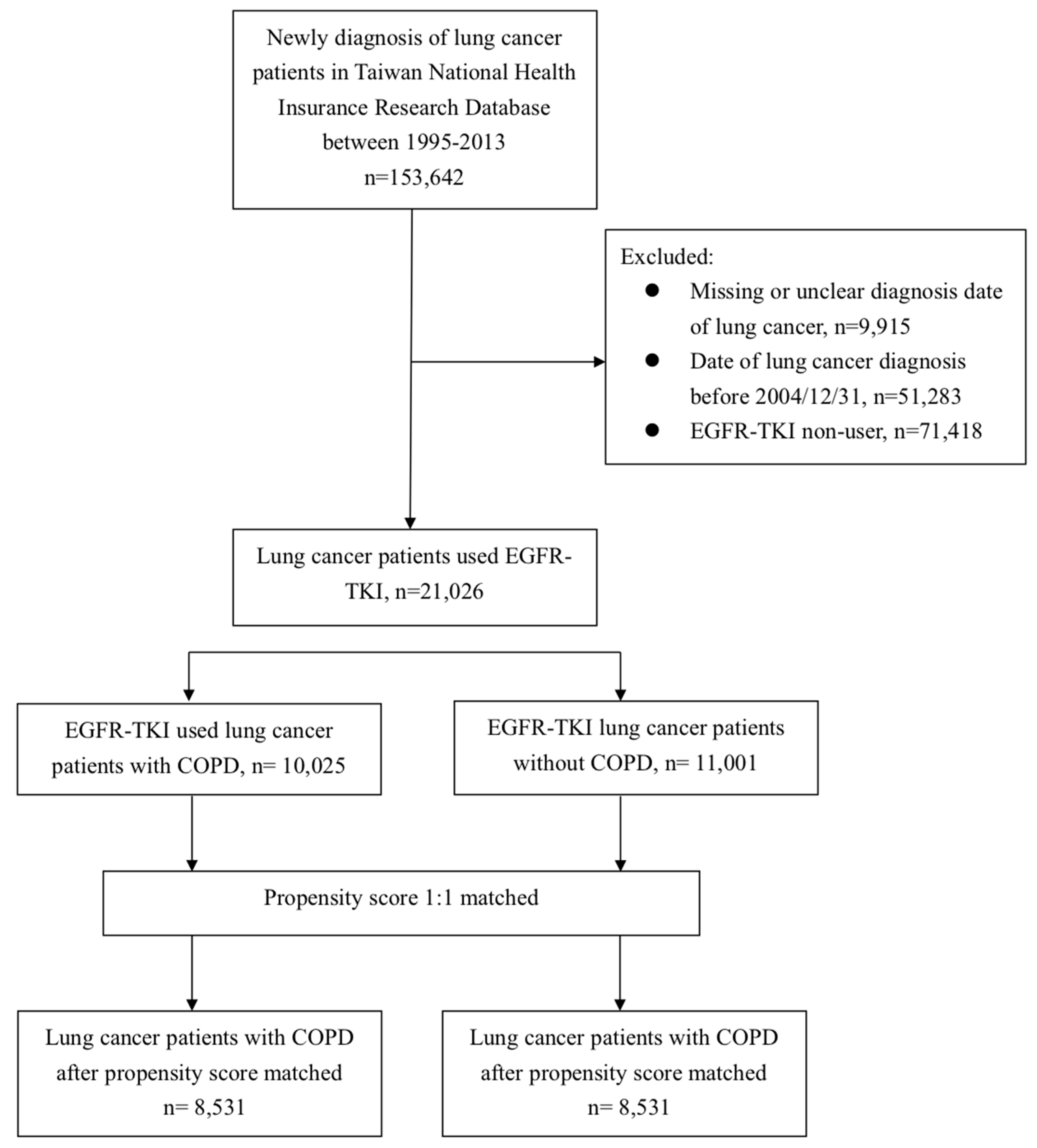
2.1. Data Source and Study Population
2.2. Study Cohort
2.3. Demographic Covariates and Comorbidities
2.4. Propensity Score Matching
2.5. Endpoints
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
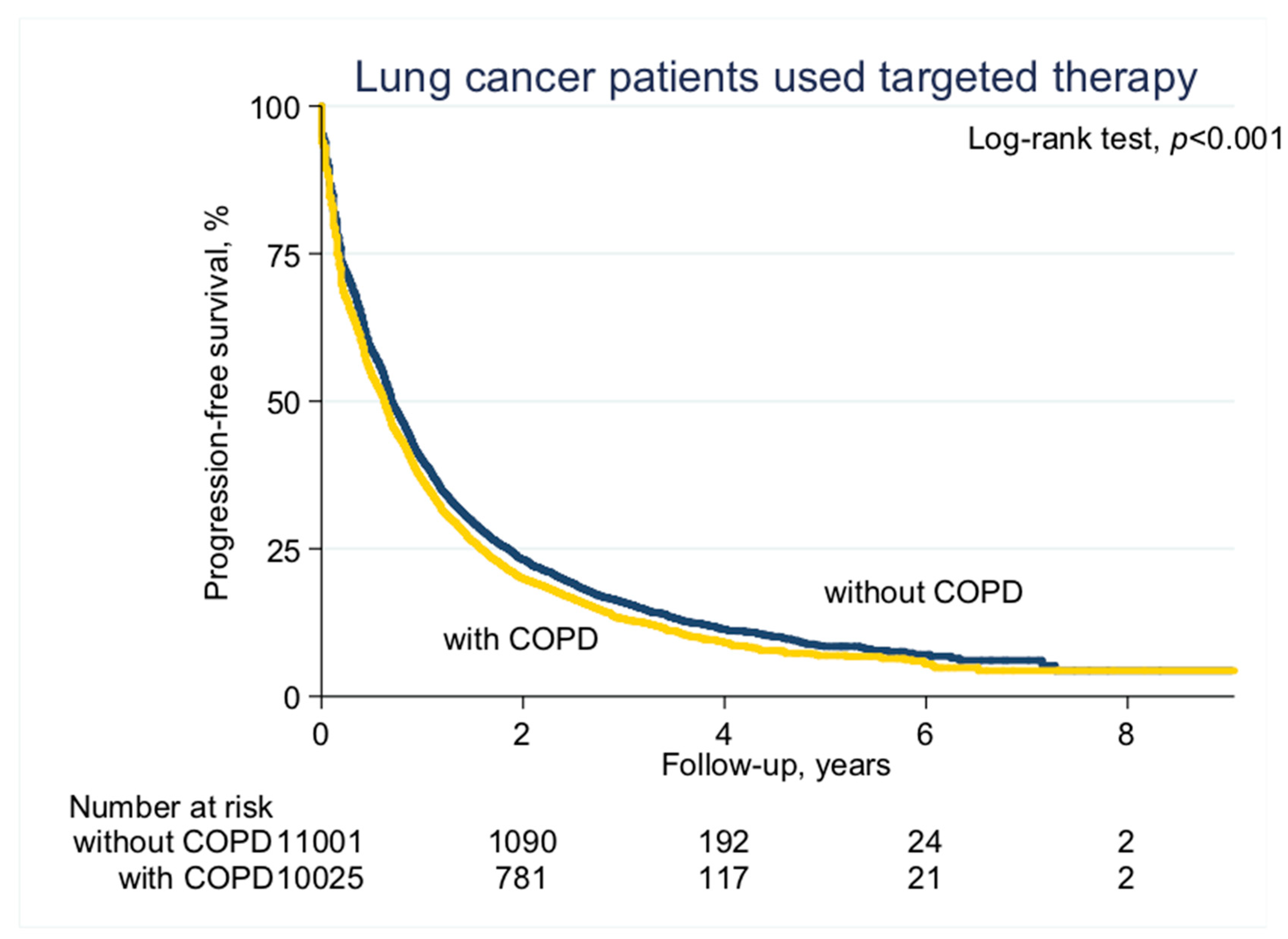
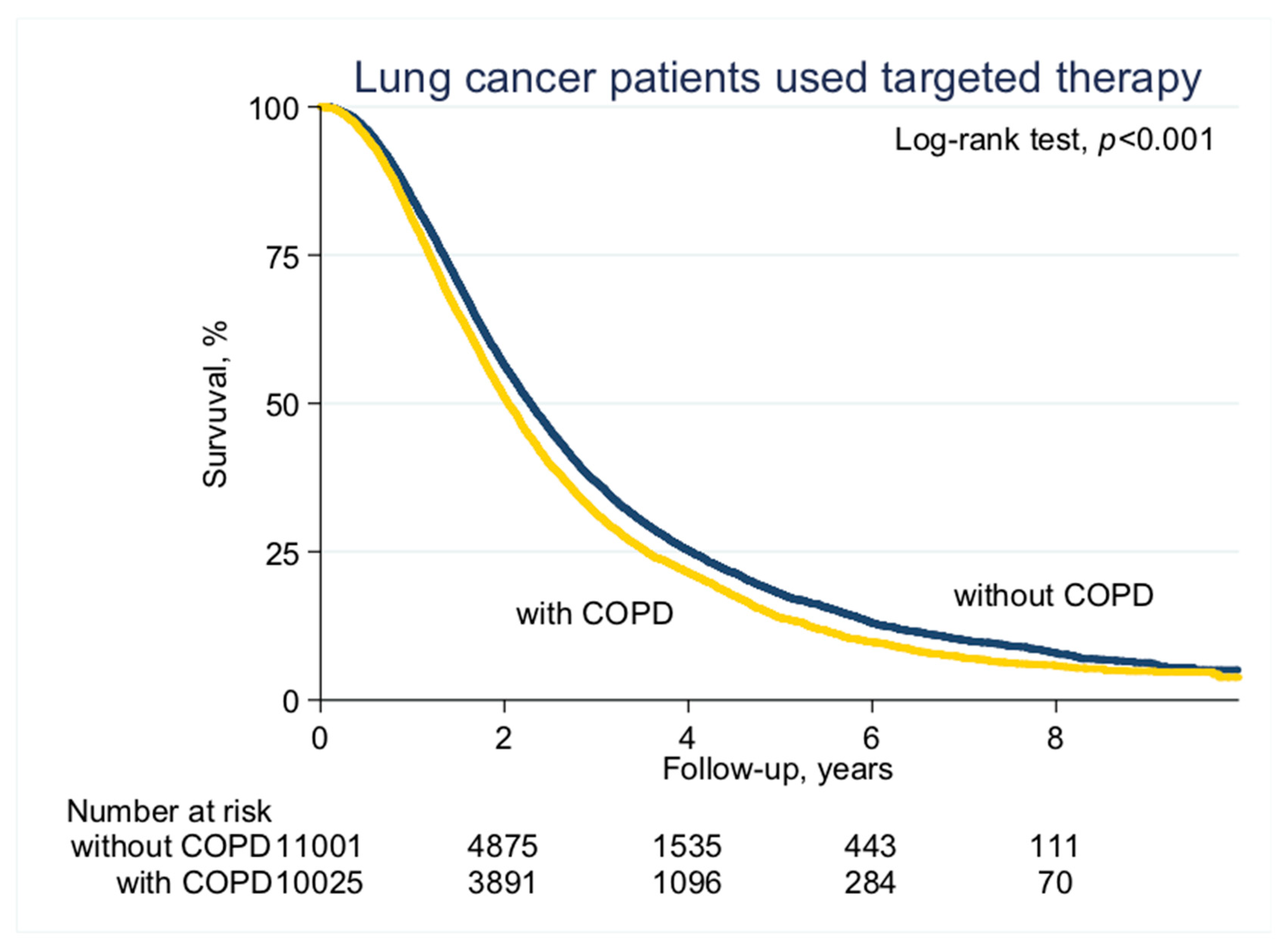
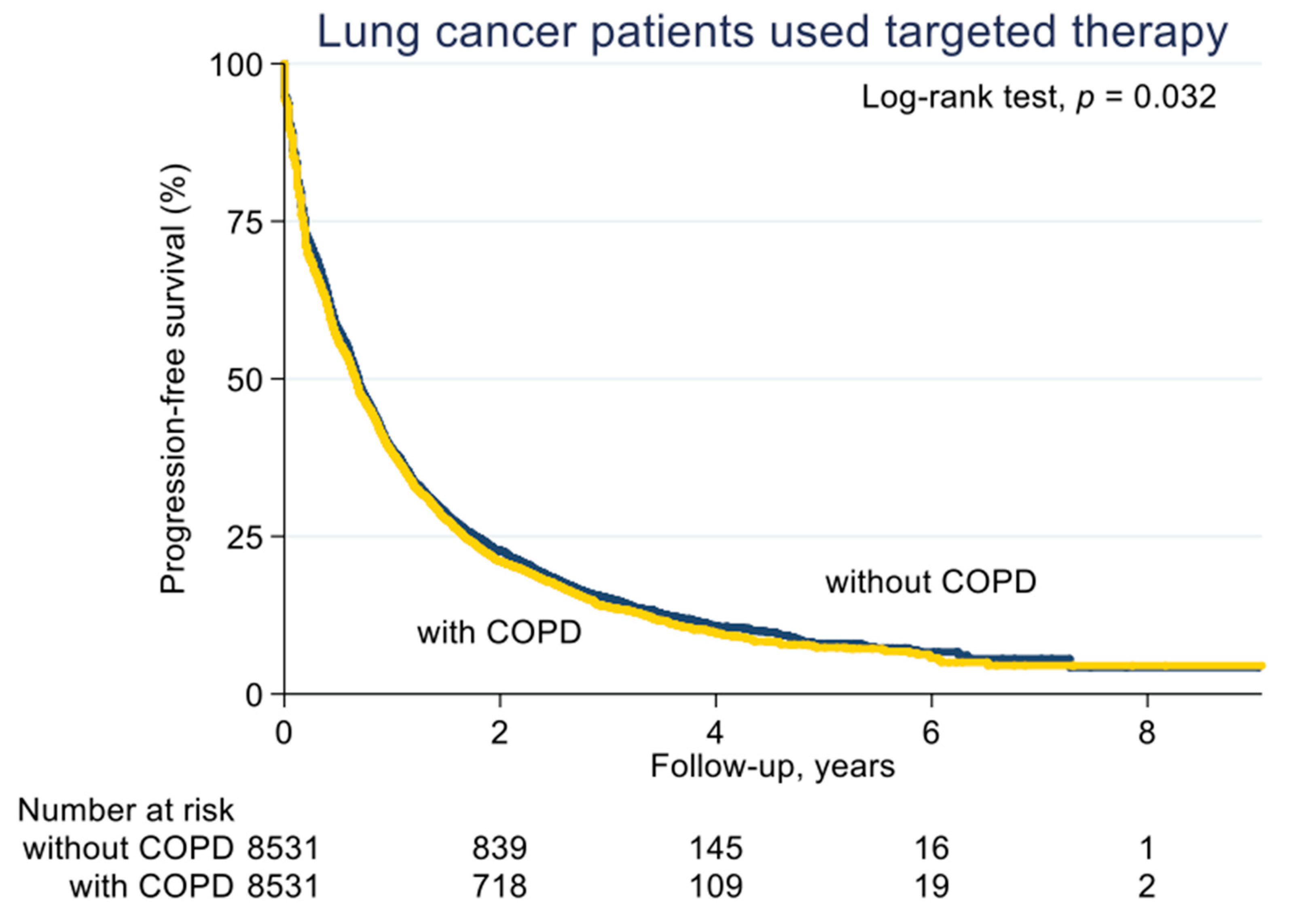
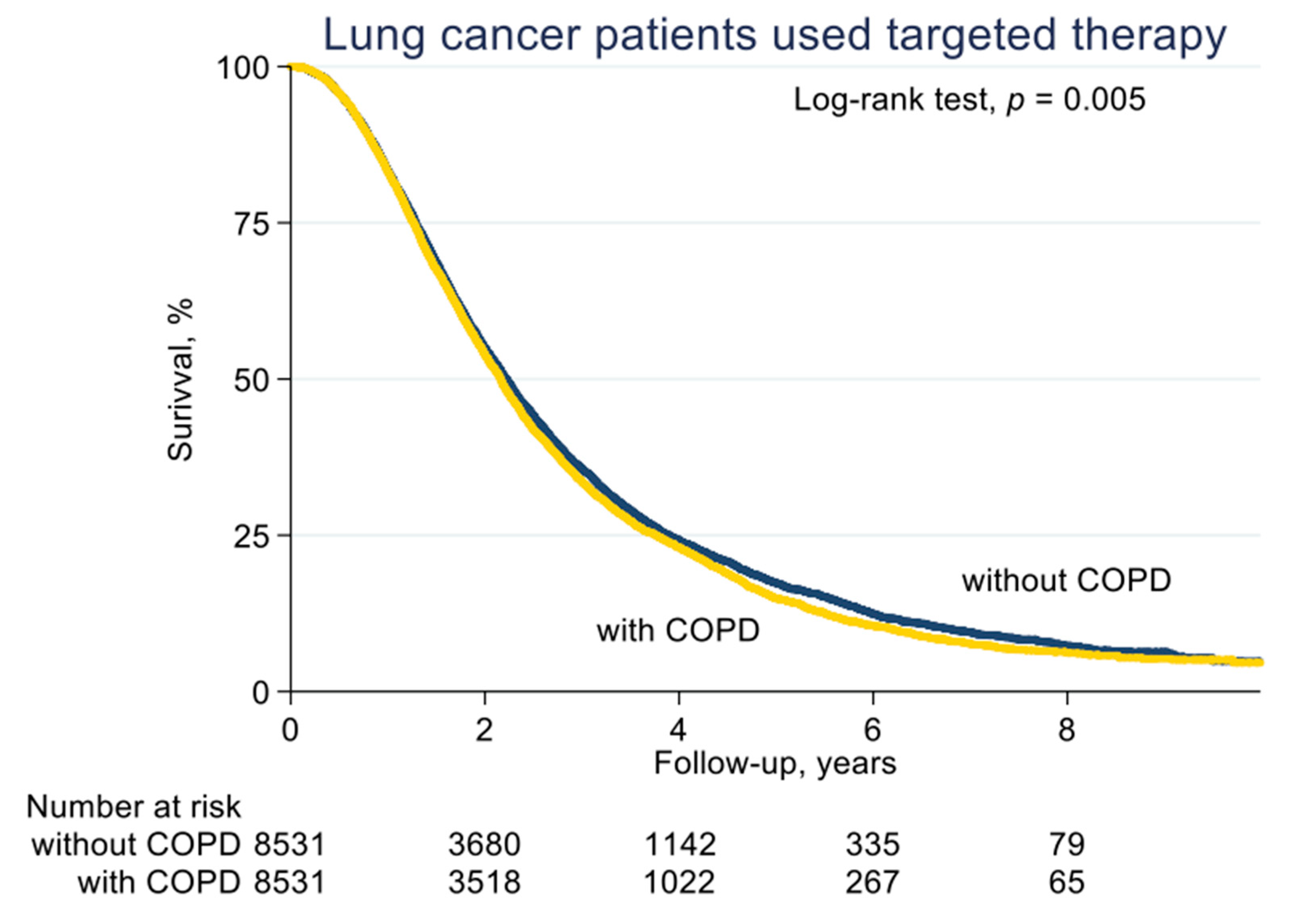
3.2. PFS and OS in COPD and non-COPD EGFR-TKI Users
3.3. Comparison of HRs of Death for All Covariates
3.4. Comparison of HRs of Progression
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegal, R.L.; Miller, K.D.; Jemal, A. Cancer Statics. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar]
- Chiang, C.J.; Lo, W.C.; Yang, Y.W.; You, S.L.; Chen, C.J.; Lai, M.S. Incidence and survival of adult cancer patients in Taiwan, 2002–2012. J. Formos. Med. Assoc. 2016, 115, 1076–1088. [Google Scholar] [CrossRef] [PubMed]
- Hanna, N.; Johnson, D.; Temin, S.; Baker, S., Jr.; Brahmer, J.; Ellis, P.M.; Giaccone, G.; Hesketh, P.J.; Jaiyesimi, I.; Leighl, N.B.; et al. Systemic therapy for stage IV non-small-cell lung cancer: American Society of Clinical Oncology Clinical Practice Guideline update. J. Clin. Oncol. 2017, 35, 3484–3515. [Google Scholar] [CrossRef] [PubMed]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin–paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.H.; Wu, Y.L.; Schuler, M.; Sebastian, M.; Popat, S.; Yamamoto, N.; Zhou, C.; Hu, C.P.; O’Byrne, K.; Feng, J.; et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): Analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol. 2015, 16, 141–151. [Google Scholar] [CrossRef]
- Lee, C.K.; Davies, L.; Wu, Y.L.; Mitsudomi, T.; Inoue, A.; Rosell, R.; Zhou, C.; Nakagawa, K.; Thongprasert, S.; Fukuoka, M.; et al. Gefitinib or Erlotinib vs. Chemotherapy for EGFR Mutation-Positive Lung Cancer: Individual Patient Data Meta-Analysis of Overall Survival. J. Natl. Cancer Inst. 2017, 109, 1883–1891. [Google Scholar] [CrossRef]
- Alexander, M.; Wolfe, R.; Ball, D.; Conron, M.; Stirling, R.G.; Solomon, B.; MacManus, M.; Officer, A.; Karnam, S.; Burbury, K.; et al. Lung cancer prognostic index: A risk score to predict overall survival after the diagnosis of non-small-cell lung cancer. Br. J. Cancer 2017, 117, 744–751. [Google Scholar] [CrossRef]
- Islam, K.M.; Jiang, X.; Anggondowati, T.; Lin, G.; Ganti, A.K. Comorbidity and Survival in Lung Cancer Patients. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1079–1085. [Google Scholar] [CrossRef]
- Young, R.P.; Hopkins, R.J.; Christmas, T.; Black, P.N.; Metcalf, P.; Gamble, G.D. COPD prevalence is increased in lung cancer, independent of age, sex and smoking history. Eur. Respir. J. 2009, 34, 380–386. [Google Scholar] [CrossRef]
- Ytterstad, E.; Moe, P.C.; Hjalmarsen, A. COPD in primary lung cancer patients: Prevalence and mortality. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 625–636. [Google Scholar] [CrossRef] [PubMed]
- Dy, S.M.; Sharkey, P.; Herbert, R.; Haddad, K.; Wu, A.W. Comorbid illnesses and health care utilization among Medicare beneficiaries with lung cancer. Crit. Rev. Oncol. Hematol. 2006, 59, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.H.; Guan, W.J.; Liu, Q.; Wang, H.Q.; Zhu, Y.N.; Chen, R.C.; Zhang, G.J. Impact of COPD and emphysema on survival of patients with lung cancer: A meta-analysis of observational studies. Respirology 2016, 21, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Omote, N.; Hashimoto, N.; Morise, M.; Sakamoto, K.; Miyazaki, S.; Ando, A.; Nakahara, Y.; Hasegawa, Y. Impact of mild to moderate COPD on feasibility and prognosis in non-small cell lung cancer patients who received chemotherapy. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 3541–3547. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Izquierdo, J.L.; Resano, P.; El Hachem, A.; Graziani, D.; Almonacid, C.; Sanchez, I.M. Impact of COPD in patients with lung cancer and advanced disease treated with chemotherapy and/or tyrosine kinase inhibitors. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 1053–1058. [Google Scholar] [CrossRef][Green Version]
- Mouronte-Roibas, C.; Leiro-Fernandez, V.; Fernandez-Villar, A.; Botana-Rial, M.; Ramos-Hernandez, C.; Ruano-Ravina, A. COPD, emphysema and the onset of lung cancer. A systematic review. Cancer Lett. 2016, 382, 240–244. [Google Scholar] [CrossRef]
- Kiri, V.A.; Soriano, J.B.; Visick, G.; Fabbri, L.M. Recent trends in lung cancer and its association with COPD: An analysis using the UK GP Research Database. Prim. Care Respir. J. 2010, 19, 57–61. [Google Scholar] [CrossRef]
- Tan, L.E.; Razak, A.M.; Lim, C.S. Association of chronic obstructive pulmonary disease and postresection lung cancer survival: A systematic review and meta-analysis. J. Investig. Med. 2017, 65, 342–352. [Google Scholar] [CrossRef]
- Parrón Collar, D.; Pazos Guerra, M.; Rodriguez, P.; Gotera, C.; Mahillo-Fenandez, I.; Peces-Barba, G.; Seijo, L.M. COPD is commonly underdiagnosed in patients with lung cancer: Results from the RECOIL study (retrospective study of COPD infradiagnosis in lung cancer). Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 1033–1038. [Google Scholar] [CrossRef]
- Sekine, Y.; Yamada, Y.; Chiyo, M.; Iwata, T.; Nakajima, T.; Yasufuku, K.; Suzuki, M.; Fujisawa, T. Association of chronic obstructive pulmonary disease and tumor recurrence in patients with stage IA lung cancer after complete resection. Ann. Thorac. Surg. 2007, 84, 946–950. [Google Scholar] [CrossRef]
- Tokumo, M.; Toyooka, S.; Kiura, K.; Shigematsu, H.; Tomii, K.; Aoe, M.; Ichimura, K.; Tsuda, T.; Yano, M.; Tsukuda, K.; et al. The relationship between epidermal growth factor receptor mutations and clinicopathologic features in Non-small cell lung cancers. Clin. Cancer Res. 2005, 11, 1167–1173. [Google Scholar] [CrossRef]
- Lim, J.U.; Yeo, C.D.; Rhee, C.K.; Kim, Y.H.; Park, C.K.; Kim, J.S.; Kim, J.W.; Lee, S.H.; Kim, S.J.; Yoon, H.K.; et al. Chronic Obstructive Pulmonary Disease-Related Non-Small-Cell Lung Cancer Exhibits a Low Prevalence of EGFR and ALK Driver Mutations. PLoS ONE 2015, 10, e0142306. [Google Scholar] [CrossRef] [PubMed]
- Takeda, K.; Yamasaki, A.; Igishi, T.; Kawasaki, Y.; Ito-Nishii, S.; Izumi, H.; Sakamoto, T.; Tonge, H.; Kodani, M.; Makino, H.; et al. Frequency of Epidermal Growth Factor Receptor Mutation in Smokers with Lung Cancer without Pulmonary Emphysema. Anticancer Res. 2017, 37, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Douillard, J.Y.; Shepherd, F.A.; Hirsh, V.; Harris, P.L.; Okimoto, R.A.; Brannigan, B.W.; Sgroi, D.C.; Muir, B.; Riemenschneider, M.J.; Iacona, R.B.; et al. Epidermal growth factor receptor mutations and gene amplification in non-small-cell lung cancer: Molecular analysis of the IDEAL/INTACT gefitinib trials. J. Clin. Oncol. 2005, 23, 8081–8092. [Google Scholar]
- Xiao, D.; Li, F.; Pan, H.; Liang, H.; Wu, K.; He, J. Integrative analysis of genomic sequencing data reveals higher prevalence of LRP1B mutations in lung adenocarcinoma patients with COPD. Sci. Rep. 2017, 7, 2121. [Google Scholar] [CrossRef] [PubMed]
- Beer, A.G.; Zenzmaier, C.; Schreinlechner, M.; Haas, J.; Dietrich, M.F.; Herz, J.; Marschang, P. Expression of a recombinant full-length LRP1B receptor in human non-small cell lung cancer cells confirms the postulated growth-suppressing function of this large LDL receptor family member. Oncotarget 2016, 7, 68721–68733. [Google Scholar] [CrossRef] [PubMed]
- Ni, S.; Hu, J.; Duan, Y.; Shi, Y.; Li, R.; Wu, H.; Qu, Y.; Li, Y. Down expression of LRP1B promotes cell migration via RhoA/Cdc42 pathway and actin cytoskeleton remodeling in renal cell cancer. Cancer Sci. 2013, 104, 817–825. [Google Scholar] [CrossRef]
- Tabouret, E.; Labussiere, M.; Alentorn, A.; Schmitt, Y.; Marie, Y.; Sanson, M. LRP1B deletion is associated with poor outcome for glioblastoma patients. J. Neurol. Sci. 2015, 358, 440–443. [Google Scholar] [CrossRef]
- De-Torres, J.P.; Sanchez-Salcedo, P.; Bastarrika, G.; Alcaide, A.B.; Pio, R.; Pajares, M.J.; Campo, A.; Berto, J.; Montuenga, L.; Del Mar Ocon, M.; et al. Telomere length, COPD and emphysema as risk factors for lung cancer. Eur. Respir. J. 2017, 49, 1601521. [Google Scholar] [CrossRef]
- Kim, E.S.; Ye, Y.; Vaporciyan, A.A.; Xing, J.; Huang, M.; Gu, J.; Roth, J.A.; Lippman, S.M.; Wu, X. Telomere length and recurrence risk after curative resection in patients with early-stage non-small-cell lung cancer: A prospective cohort study. J. Thorac. Oncol. 2015, 10, 302–308. [Google Scholar] [CrossRef]
- Thom, S.R.; Ma, M.; Bhopale, V.M.; Zhou, C.; Mao, L. Oxidative stress mediated by nitrogen at elevated pressure inhibits non-small cell lung cancer growth. Exp. Lung Res. 2017, 43, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Bozinovski, S.; Vlanhos, R.; Anthony, D.; McQualter, J.; Anderson, G.; Irving, L.; Steinfort, D. COPD and squamous cell lung cancer: Aberrant inflammation and immunity is the common link. Br. J. Pharmacol. 2016, 173, 635–648. [Google Scholar] [CrossRef] [PubMed]
- We, C.C.; Hsu, H.Y.; Liu, H.P.; Chang, J.W.; Chen, Y.T.; Hsieh, W.Y.; Hsieh, J.J.; Hsieh, M.S.; Chen, Y.R.; Huang, S.F. Reversed mutation rates of KRAS and EGFR genes in adenocarcinoma of the lung in Taiwan and their implications. Cancer 2008, 113, 3199–3208. [Google Scholar]
- Midha, A.; Dearden, S.; McCormack, R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: A systematic review and global map by ethnicity (mutMapII). Am. J. Cancer Res. 2015, 5, 2892–2911. [Google Scholar] [PubMed]
- Shi, Y.; Au, J.S.K.; Thongprasert, S.; Srinivasan, S.; Tsai, C.M.; Khoa, M.T.; Heeroma, K.; Itoh, Y.; Cornelio, G.; Yang, P.C. A Prospective, Molecular Epidemiology Study of EGFR Mutations in Asian Patients with Advanced Non–Small-Cell Lung Cancer of Adenocarcinoma Histology (PIONEER). J. Thorac. Oncol. 2014, 9, 154–162. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Propensity Score Matched | After Propensity Score Matched | |||||
|---|---|---|---|---|---|---|
| With COPD | Without COPD | p Value | With COPD | Without COPD | p Value | |
| n | 10,025 | 11,001 | 8531 | 8531 | ||
| Age (mean, SD), years | 67.6 (11.8) | 62 (12.1) | <0.001 | 65.6 (11.3) | 64.9 (11.4) | <0.001 |
| Gender | ||||||
| Male | 5167 (51.5) | 4804 (43.7) | <0.001 | 4091 (48.0) | 4030 (47.2) | 0.35 |
| Female | 4858 (48.5) | 6197 (56.3) | <0.001 | 4440 (52.0) | 4501 (52.8) | 0.35 |
| Premium level (NTD) | ||||||
| >25,000 | 3588 (35.8) | 4934 (44.9) | <0.001 | 3373 (39.5) | 3480 (40.8) | 0.09 |
| 25000–15840 | 4510 (45.0) | 4313 (39.2) | <0.001 | 3657 (42.9) | 3567 (41.8) | 0.16 |
| <15,840 | 1179 (11.8) | 1027 (9.3) | <0.001 | 883 (10.4) | 858 (10.1) | 0.53 |
| Low | 748 (7.5) | 727 (6.6) | 0.016 | 618 (7.2) | 626 (7.3) | 0.81 |
| Comorbidity | ||||||
| CHF | 662 (6.6) | 343 (3.1) | <0.001 | 304 (3.6) | 338 (4.0) | 0.17 |
| DM | 2007 (20.0) | 1835 (16.7) | <0.001 | 1677 (19.7) | 1630 (19.1) | 0.36 |
| Pneumonia | 2207 (22.0) | 1571 (14.3) | <0.001 | 1382 (16.2) | 1451 (17.0) | 0.16 |
| Sepsis | 107 (1.1) | 91 (0.8) | 0.07 | 76 (0.9) | 77 (0.9) | 0.94 |
| CCI score | 4.7 (2.7) | 4.2 (2.8) | <0.001 | 4.4 (2.6) | 4.4 (2.9) | 0.99 |
| Anti-cancer agents | ||||||
| Erlotinib | 4770 (47.6) | 4990 (45.4) | 0.001 | 4004 (46.9) | 3991 (46.8) | 0.84 |
| Gefitinib | 6071 (60.6) | 7083 (64.4) | <0.001 | 5278 (61.9) | 5302 (62.1) | 0.71 |
| Erlotinib + Gefitinib | 816 (8.1) | 1072 (9.7) | <0.001 | 751 (8.8) | 762 (8.9) | 0.77 |
| Gemcitabine | 3962 (39.5) | 4689 (42.6) | <0.001 | 3547 (41.6) | 3546 (41.6) | 0.99 |
| Docetaxel | 3321 (33.1) | 3857 (35.1) | 0.003 | 2965 (34.8) | 2947 (34.5) | 0.77 |
| Pemetrexed | 3070 (30.6) | 3864 (35.1) | <0.001 | 2843 (33.3) | 2845 (33.3) | 0.99 |
| Vinorelbine | 3894 (38.8) | 4113 (37.4) | 0.03 | 3262 (38.2) | 3219 (37.7) | 0.50 |
| Cisplatin | 1852 (18.5) | 2487 (22.6) | <0.001 | 1737 (20.4) | 1764 (20.7) | 0.61 |
| Paclitaxel | 1256 (12.5) | 1498 (13.6) | 0.019 | 1120 (13.1) | 1136 (13.3) | 0.72 |
| Carboplatin | 638 (6.4) | 609 (5.5) | 0.011 | 543 (6.4) | 519 (6.1) | 0.45 |
| Cancer treatment | ||||||
| CT + RT | 3587 (35.8) | 4626 (42.1) | <0.001 | 3335 (39.1) | 3333 (39.1) | 0.99 |
| CT | 6495 (64.8) | 7664 (69.7) | <0.001 | 5802 (68.0) | 5805 (68.0) | 0.99 |
| RT | 4754 (47.4) | 5914 (53.8) | <0.001 | 4302 (50.4) | 4352 (51.0) | 0.44 |
| Without CT or RT | 2363 (23.6) | 2049 (18.6) | <0.001 | 1762 (20.7) | 1707 (20.0) | 0.30 |
| CT regimens before EGFR-TKI | ||||||
| 0 | 3627 (36.2) | 3956 (36.0) | 0.74 | 3013 (35.3) | 3043 (35.7) | 0.63 |
| 1 | 2705 (27.0) | 2880 (26.2) | 0.19 | 2271 (26.6) | 2249 (26.4) | 0.70 |
| ≥2 | 3693 (36.8) | 4165 (37.9) | 0.13 | 3247 (38.1) | 3239 (38.0) | 0.90 |
| Concomitant drug | ||||||
| Statin | 2151 (21.5) | 1765 (16.0) | <0.001 | 1692 (19.8) | 1629 (19.1) | 0.22 |
| NSAID | 9480 (94.6) | 9964 (90.6) | <0.001 | 8000 (93.8) | 7956 (93.3) | 0.17 |
| Aspirin | 3202 (31.9) | 2332 (21.2) | <0.001 | 2304 (27.0) | 2215 (26.0) | 0.12 |
| Anti-HTN | 7265 (72.5) | 6403 (58.2) | <0.001 | 5832 (68.4) | 5690 (66.7) | 0.02 |
| Steroids | 7820 (78.0) | 8029 (73.0) | <0.001 | 6509 (76.3) | 6462 (75.7) | 0.40 |
| Propensity score | 0.6236 (0.4845) | 0.5379 (0.4986) | <0.001 | 0.4859 (0.1201) | 0.4778 (0.1266) | <0.001 |
| Crude Model | Adjusted Model a | Propensity Score Matched Adjusted Model | ||||
|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| All-cause mortality | ||||||
| COPD | 1.16 (1.12–1.20) | <0.001 | 1.05 (1.01–1.08) | 0.012 | 1.04 (1.00–1.08) | 0.033 |
| Erlotinib | 0.87 (0.84–0.90) | <0.001 | 0.56 (0.53–0.60) | <0.001 | 0.56 (0.52–0.60) | <0.001 |
| Gefitinib | 0.87 (0.84–0.90) | <0.001 | 0.55 (0.52–0.59) | <0.001 | 0.55 (0.51–0.59) | <0.001 |
| Age (mean, SD), years | 1.01 (1.01–1.01) | <0.001 | 1.01 (1.00–1.01) | <0.001 | 1.01 (1.00–1.01) | <0.001 |
| Gender | ||||||
| Male vs. Female | 1.33 (1.29–1.38) | <0.001 | 1.33 (1.29–1.38) | <0.001 | 1.32 (1.27–1.38) | <0.001 |
| Premium level (NTD) | ||||||
| >25,000 | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) | |||
| 25,000–15,840 | 1.16 (1.09–1.24) | <0.001 | 1.21 (1.12–1.30) | <0.001 | 1.17 (1.09–1.27) | <0.001 |
| <15,840 | 1.22 (1.16–1.30) | <0.001 | 1.15 (1.08–1.22) | <0.001 | 1.13 (1.05–1.21) | <0.001 |
| Low | 1.20 (1.16–1.24) | <0.001 | 1.20 (1.15–1.24) | <0.001 | 1.18 (1.13–1.23) | <0.001 |
| Comorbidity | ||||||
| CHF | 1.16 (1.08–1.26) | <0.001 | 1.10 (1.02–1.19) | 0.016 | 1.13 (1.03–1.25) | 0.013 |
| DM | 1.12 (1.07–1.17) | <0.001 | 1.15 (1.10–1.21) | <0.001 | 1.14 (1.09–1.20) | <0.001 |
| Pneumonia | 1.25 (1.19–1.30) | <0.001 | 1.19 (1.14–1.24) | <0.001 | 1.19 (1.13–1.25) | <0.001 |
| Sepsis | 1.44 (1.22–1.70) | <0.001 | 1.17 (0.99–1.38) | 0.06 | 1.24 (1.03–1.49) | 0.022 |
| CCI score | 1.05 (1.04–1.05) | <0.001 | 1.05 (1.04–1.05) | <0.001 | 1.05 (1.04–1.05) | <0.001 |
| Anti-neoplastic agents | ||||||
| Gemcitabine | 0.94 (0.91–0.97) | <0.001 | 1.01 (0.97–1.05) | 0.60 | 1.00 (0.95–1.04) | 0.99 |
| Docetaxel | 0.89 (0.86–0.92) | <0.001 | 0.98 (0.94–1.02) | 0.26 | 0.98 (0.93–1.02) | 0.31 |
| Pemetrexed | 0.69 (0.67–0.72) | <0.001 | 0.79 (0.76–0.82) | <0.001 | 0.79 (0.75–0.82) | <0.001 |
| Vinorelbine | 0.84 (0.81–0.87) | <0.001 | 0.85 (0.82–0.88) | <0.001 | 0.83 (0.80–0.86) | <0.001 |
| Cisplatin | 0.86 (0.83–0.90) | <0.001 | 0.93 (0.89–0.97) | 0.002 | 0.92 (0.87–0.97) | 0.001 |
| Paclitaxel | 0.82 (0.78–0.85) | <0.001 | 0.87 (0.83–0.92) | <0.001 | 0.89 (0.84–0.94) | <0.001 |
| Carboplatin | 0.85 (0.79–0.90) | <0.001 | 0.88 (0.82–0.94) | <0.001 | 0.88 (0.81–0.95) | 0.001 |
| Cancer treatment | ||||||
| CT | 0.79 (0.76–0.82) | < 0.001 | 0.88 (0.83–0.93) | < 0.001 | 0.90 (0.84–0.96) | 0.003 |
| RT | 0.93 (0.90–0.96) | < 0.001 | 0.96 (0.93–1.00) | 0.041 | 0.98 (0.94–1.02) | 0.23 |
| CT regimens before EGFR-TKI | ||||||
| 0 | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) | |||
| 1 | 1.04 (1.00–1.09) | 0.07 | 1.14 (1.07–1.20) | <0.001 | 1.13 (1.06–1.20) | <0.001 |
| ≥2 | 0.96 (0.92–1.00) | 0.046 | 1.17 (1.09–1.25) | <0.001 | 1.18 (1.09–1.27) | <0.001 |
| Concomitant drug | ||||||
| Statin | 0.86 (0.83–0.90) | <0.001 | 0.85 (0.81–0.90) | <0.001 | 0.85 (0.80–0.89) | <0.001 |
| NSAID | 1.18 (1.10–1.27) | <0.001 | 1.23 (1.14–1.33) | <0.001 | 1.15 (1.06–1.25) | 0.001 |
| Aspirin | 0.94 (0.91–0.98) | 0.003 | 0.86 (0.82–0.89) | <0.001 | 0.85 (0.81–0.89) | <0.001 |
| Anti-HTN | 0.92 (0.89–0.96) | <0.001 | 0.84 (0.81–0.88) | <0.001 | 0.84 (0.81–0.88) | <0.001 |
| Steroid | 1.00 (0.96–1.04) | 0.99 | 1.07 (1.02–1.12) | 0.003 | 1.07 (1.02–1.12) | 0.011 |
| Crude Model | Adjusted Model a | Propensity Score Matched Adjusted Model | ||||
|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Progression-free survival | ||||||
| COPD | 1.11 (1.08–1.15) | <0.001 | 1.05 (1.02–1.09) | 0.004 | 1.05 (1.02–1.09) | 0.006 |
| Erlotinib | 1.11 (1.08–1.15) | <0.001 | 0.36 (0.34–0.39) | <0.001 | 0.36 (0.33–0.39) | <0.001 |
| Gefitinib | 0.54 (0.52–0.56) | <0.001 | 0.28 (0.26–0.30) | <0.001 | 0.29 (0.26–0.31) | <0.001 |
| Age (mean, SD), years | 1.00 (1.00–1.00) | 0.3 | 1.00 (1.00–1.00) | 0.73 | 1.00 (1.00–1.00) | 0.09 |
| Gender | ||||||
| Male vs. Female | 1.50 (1.45–1.55) | <0.001 | 1.36 (1.31–1.41) | <0.001 | 1.35 (1.30–1.41) | <0.001 |
| Premium level (NTD) | ||||||
| >25,000 | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) | |||
| 25,000–15,840 | 1.08 (1.01–1.15) | 0.026 | 1.23 (1.15–1.32) | <0.001 | 1.22 (1.13–1.31) | <0.001 |
| <15,840 | 1.21 (1.14–1.28) | <0.001 | 1.23 (1.16–1.31) | <0.001 | 1.21 (1.14–1.30) | <0.001 |
| Low | 1.13 (1.09–1.18) | <0.001 | 1.16 (1.12–1.21) | <0.001 | 1.16 (1.11–1.21) | <0.001 |
| Comorbidity | ||||||
| CHF | 1.10 (1.02–1.18) | 0.019 | 1.12 (1.03–1.21) | 0.006 | 1.10 (1.00–1.22) | 0.05 |
| DM | 1.05 (1.01–1.10) | 0.02 | 1.11 (1.06–1.16) | <0.001 | 1.10 (1.05–1.15) | <0.001 |
| Pneumonia | 1.21 (1.16–1.26) | <0.001 | 1.15 (1.11–1.20) | <0.001 | 1.16 (1.10–1.21) | <0.001 |
| Sepsis | 1.24 (1.05–1.46) | 0.011 | 1.10 (0.93–1.30) | 0.25 | 1.15 (0.96–1.39) | 0.13 |
| CCI score | 1.02 (1.01–1.02) | <0.001 | 1.02 (1.01–1.02) | <0.001 | 1.02 (1.01–1.02) | <0.001 |
| Anti-neoplastic agents | ||||||
| Gemcitabine | 1.45 (1.40–1.49) | <0.001 | 1.24 (1.19–1.30) | <0.001 | 1.22 (1.17–1.28) | <0.001 |
| Docetaxel | 1.33 (1.29–1.38) | <0.001 | 1.09 (1.05–1.14) | <0.001 | 1.08 (1.03–1.13) | 0.001 |
| Pemetrexed | 0.99 (0.96–1.02) | 0.54 | 0.96 (0.92–1.00) | 0.032 | 0.95 (0.91–0.99) | 0.02 |
| Vinorelbine | 1.24 (1.20–1.28) | <0.001 | 1.11 (1.07–1.15) | <0.001 | 1.09 (1.05–1.14) | <0.001 |
| Cisplatin | 1.10 (1.06–1.14) | <0.001 | 0.90 (0.86–0.95) | <0.001 | 0.89 (0.84–0.94) | <0.001 |
| Paclitaxel | 1.22 (1.16–1.27) | <0.001 | 1.07 (1.02–1.12) | 0.006 | 1.08 (1.02–1.14) | 0.006 |
| Carboplatin | 1.08 (1.01–1.15) | 0.029 | 0.92 (0.86–0.99) | 0.021 | 0.92 (0.85–0.99) | 0.029 |
| Cancer treatment | ||||||
| CT | 1.43 (1.38–1.49) | <0.001 | 1.01 (0.95–1.08) | 0.74 | 1.04 (0.97–1.11) | 0.29 |
| RT | 1.13 (1.09–1.16) | <0.001 | 1.03 (0.99–1.07) | 0.11 | 1.05 (1.01–1.09) | 0.024 |
| CT regimens before EGFR-TKI | ||||||
| 0 | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) | |||
| 1 | 1.65 (1.58–1.72) | <0.001 | 1.24 (1.17–1.31) | <0.001 | 1.22 (1.15–1.30) | <0.001 |
| ≥2 | 1.93 (1.85–2.01) | <0.001 | 1.31 (1.22–1.40) | <0.001 | 1.33 (1.23–1.43) | <0.001 |
| Concomitant drug | ||||||
| Statin | 0.82 (0.79–0.86) | <0.001 | 0.86 (0.82–0.91) | <0.001 | 0.86 (0.82–0.91) | <0.001 |
| NSAID | 1.41 (1.31–1.52) | <0.001 | 1.32 (1.23–1.43) | <0.001 | 1.22 (1.12–1.33) | <0.001 |
| Aspirin | 0.91 (0.87–0.94) | <0.001 | 0.89 (0.85–0.93) | <0.001 | 0.88 (0.84–0.93) | <0.001 |
| Anti-HTN | 0.95 (0.92–0.98) | 0.004 | 0.93 (0.89–0.96) | <0.001 | 0.93 (0.89–0.97) | 0.002 |
| Steroid | 1.28 (1.23–1.33) | <0.001 | 1.06 (1.02–1.11) | 0.007 | 1.07 (1.02–1.13) | 0.006 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-C.; Rau, K.-M.; Lee, W.-C.; Hsieh, M.-C.; Liu, J.-S.; Chen, Y.-Y.; Su, H.Y.-L. Presence of Chronic Obstructive Pulmonary Disease (COPD) Impair Survival in Lung Cancer Patients Receiving Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor (EGFR-TKI): A Nationwide, Population-Based Cohort Study. J. Clin. Med. 2019, 8, 1024. https://doi.org/10.3390/jcm8071024
Wu C-C, Rau K-M, Lee W-C, Hsieh M-C, Liu J-S, Chen Y-Y, Su HY-L. Presence of Chronic Obstructive Pulmonary Disease (COPD) Impair Survival in Lung Cancer Patients Receiving Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor (EGFR-TKI): A Nationwide, Population-Based Cohort Study. Journal of Clinical Medicine. 2019; 8(7):1024. https://doi.org/10.3390/jcm8071024
Chicago/Turabian StyleWu, Chia-Che, Kun-Ming Rau, Wei-Chieh Lee, Meng-Che Hsieh, Jia-Sin Liu, Yen-Yang Chen, and Harvey Yu-Li Su. 2019. "Presence of Chronic Obstructive Pulmonary Disease (COPD) Impair Survival in Lung Cancer Patients Receiving Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor (EGFR-TKI): A Nationwide, Population-Based Cohort Study" Journal of Clinical Medicine 8, no. 7: 1024. https://doi.org/10.3390/jcm8071024
APA StyleWu, C.-C., Rau, K.-M., Lee, W.-C., Hsieh, M.-C., Liu, J.-S., Chen, Y.-Y., & Su, H. Y.-L. (2019). Presence of Chronic Obstructive Pulmonary Disease (COPD) Impair Survival in Lung Cancer Patients Receiving Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor (EGFR-TKI): A Nationwide, Population-Based Cohort Study. Journal of Clinical Medicine, 8(7), 1024. https://doi.org/10.3390/jcm8071024