Vasculogenic Chronic Ulcer: Tissue Regeneration with an Innovative Dermal Substitute

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Dermal Substitute
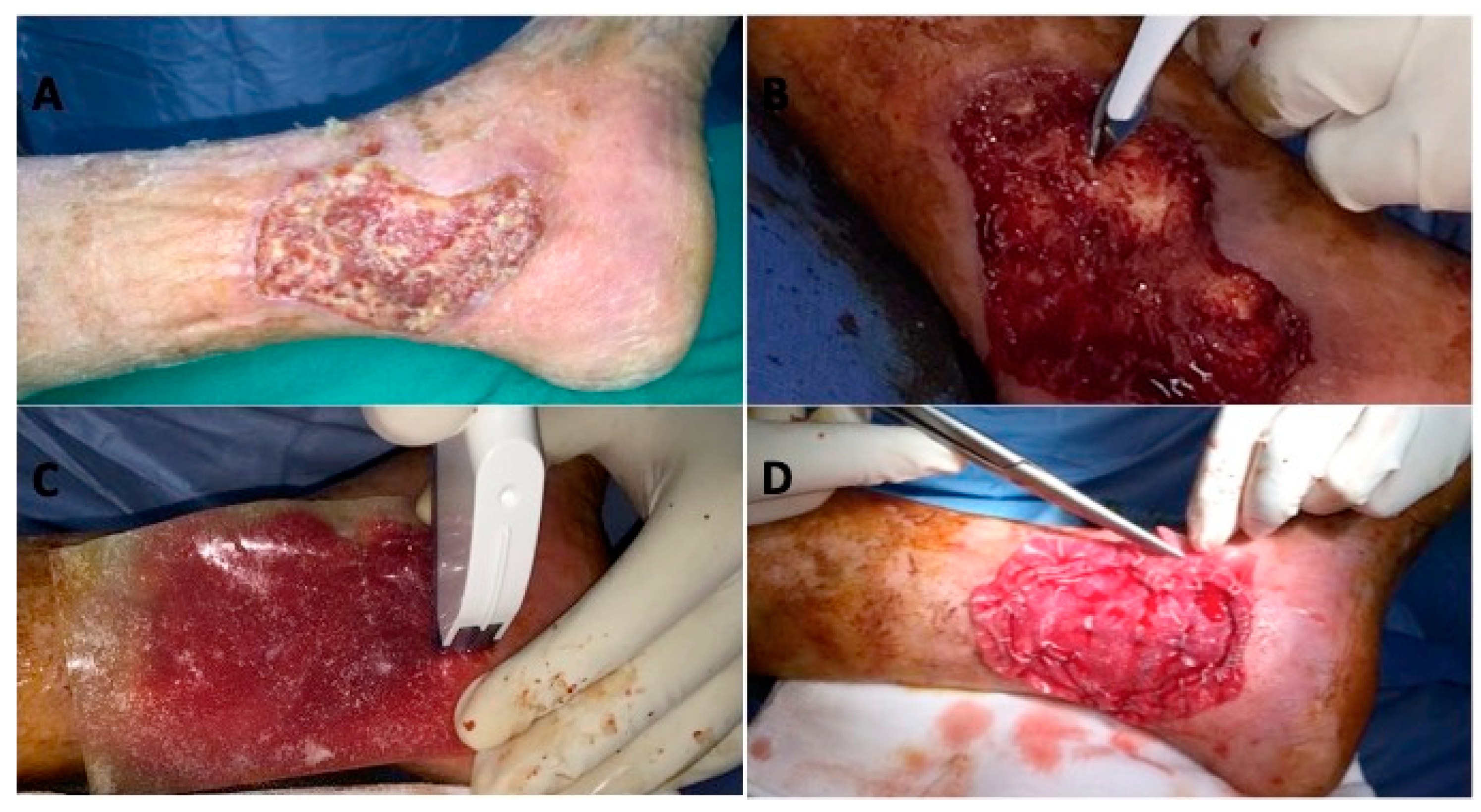
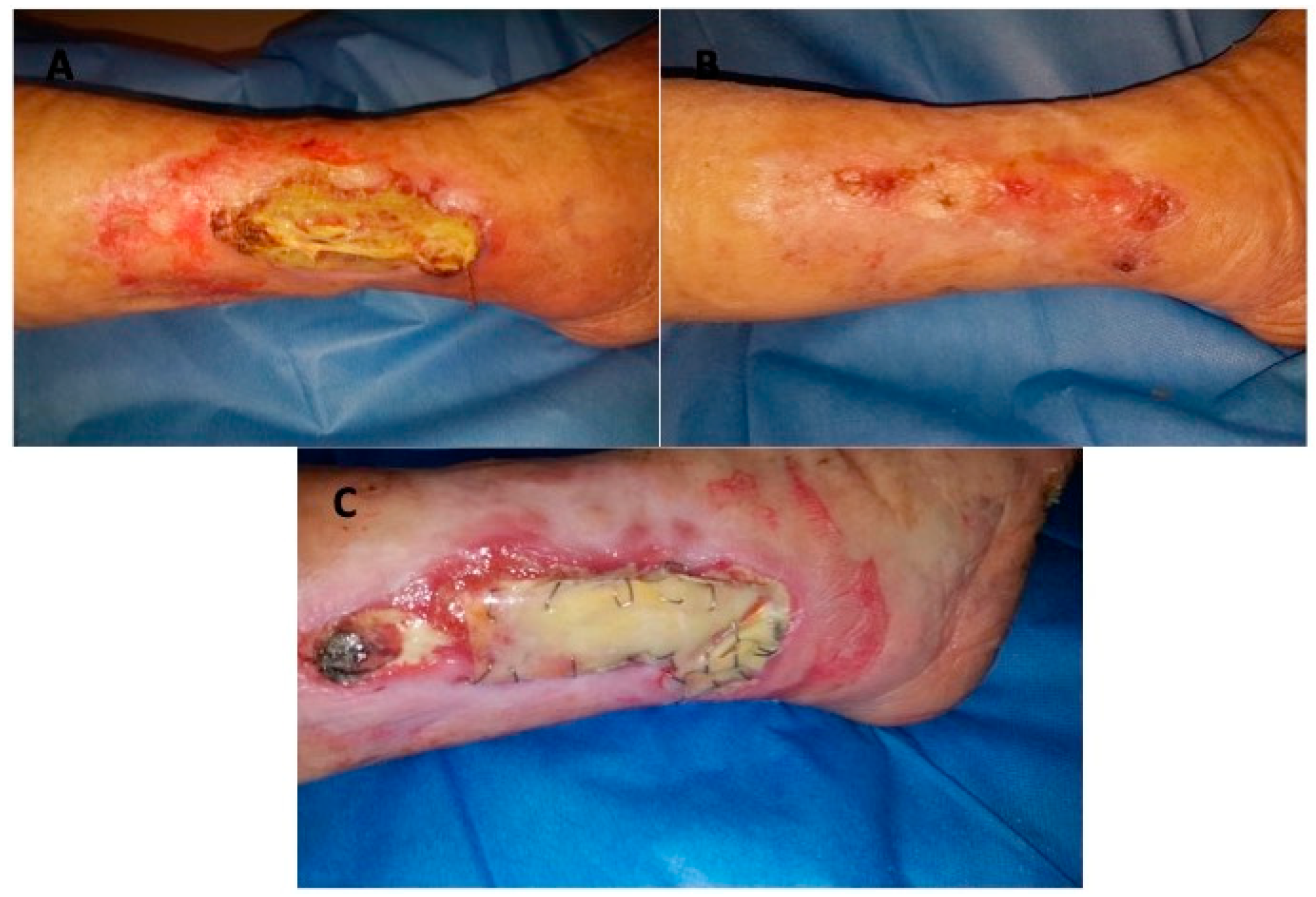
2.3. Clinical and Surgical Protocol
2.4. Clinical Criteria Evaluation During Treatment and Follow-up
2.5. Histological Evaluation
2.6. Immunohistochemical Study
2.7. Statistical Analysis
3. Results
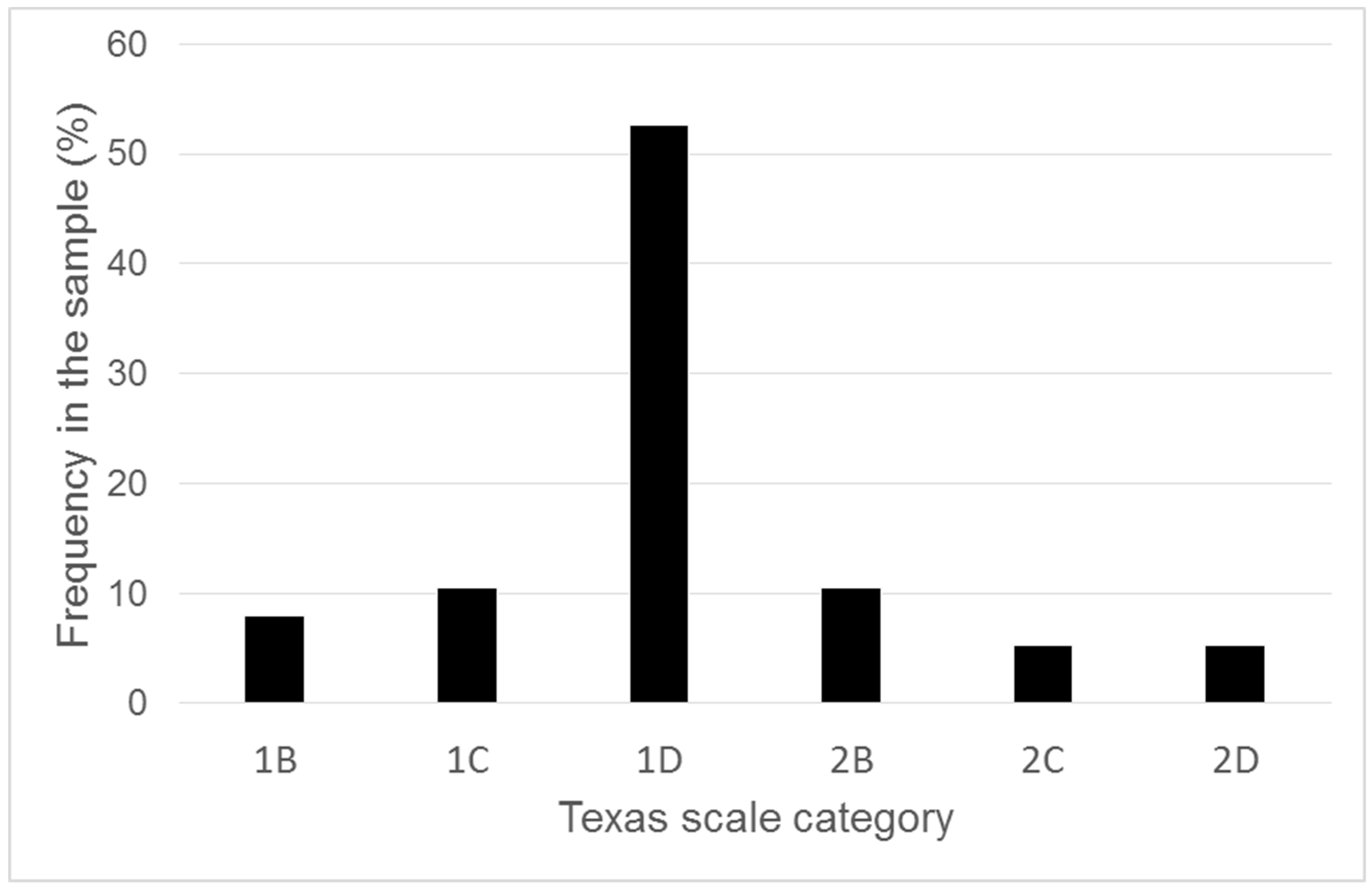
3.1. Wound Features
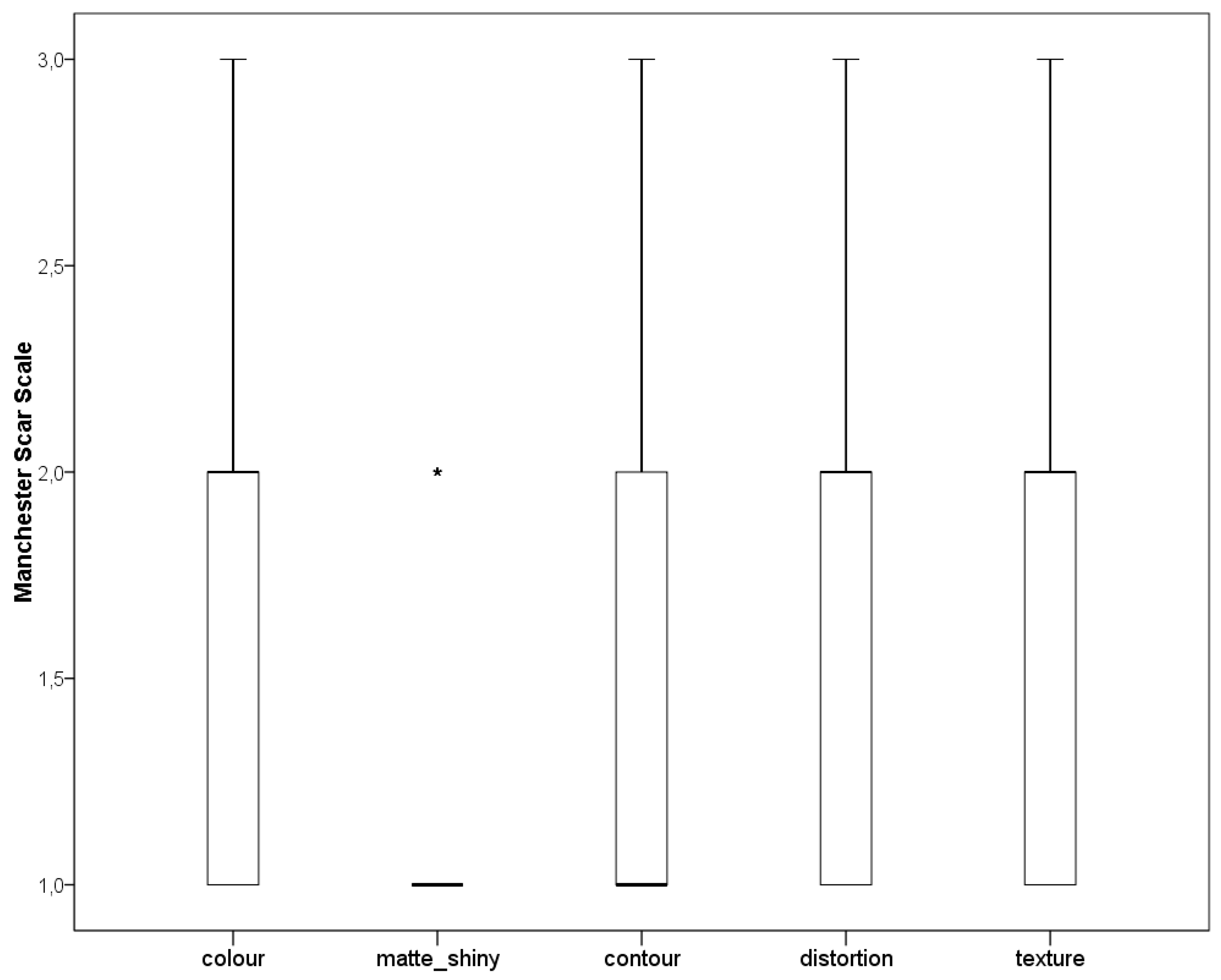
3.2. In Vivo Evaluation
3.3. In Vitro Evaluation
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| Dermal Substitute | DS |
| Dermal epidermal graft | DEG |
| Venous Leg Ulcer | VLU |
| Visual Analogical Scale | VAS |
| Manchester Scar Scale | MSS |
| Anemia | A |
| Dyslipidemia | DLP |
| Diabetes Mellitus | DM |
| Hemodialysis | HD |
| Liver Failure | LF |
| Hypertension | HPT |
| Heart Failure | HF |
| Respiratory Failure | RF |
| Kidney Failure | KF |
| Vascular Insufficiency | VI |
| Diabetic Neuropathy | DN |
| Obesity | OB |
| Diabetic Retinopathy | DR |
| Glycosaminoglycans | GAG |
| Percutaneous transluminal angioplasty | PTA |
| Critical limb ischemia | CLI |
References
- O’Donnell, T.F., Jr.; Passman, M.A.; Marston, W.A.; Ennis, W.J.; Dalsing, M.; Kistner, R.L.; Lurie, F.; Henke, P.K.; Gloviczki, M.L.; Eklöf, B.G.; et al. Management of venous leg ulcers: Clinical practice guidelines of the Society for Vascular Surgery® and the American Venous Forum. J. Vasc. Surg. 2014, 60, 3S–59S. [Google Scholar] [CrossRef]
- Hellström, A.; Nilsson, C.; Nilsson, A.; Fagerström, C. Leg ulcers in older people: A national study addressing variation in diagnosis, pain and sleep disturbance. BMC Geriatr. 2016, 16, 25. [Google Scholar] [CrossRef]
- McDaniel, H.B.; Marston, W.A.; Farber, M.A.; Mendes, R.R.; Owens, L.V.; Young, M.L.; Daniel, P.F.; Keagy, B.A. Recurrence of chronic venous ulcers on the basis of clinical, etiologic, anatomic, and pathophysiologic criteria and air plethysmography. J. Vasc. Surg. 2002, 35, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Agale, S.V. Chronic leg ulcers: Epidemiology, aetiopathogenesis, and management. Ulcers 2013, 2013, 1–9. [Google Scholar] [CrossRef]
- Abbade, L.P.; Lastória, S. Venous ulcer: Epidemiology, physiopathology, diagnosis and treatment. Int. J. Dermatol. 2005, 44, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Grey, J.E.; Harding, K.G.; Enoch, S. Venous and arterial leg ulcers. BMJ 2006, 332, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Perrin, M.; Lugli, M.; Maleti, O. Management of mixed arterial and venous lower leg ulcers. Phlebolymphology 2013, 20, 133. [Google Scholar]
- Ghauri, A.S.; Nyamekye, I.; Grabs, A.J.; Farndon, J.R.; Poskitt, K.R. The diagnosis and management of mixed arterial/venous leg ulcers in community-based clinics. Eur. J. Vasc. Endovasc. Surg. 1998, 16, 350–355. [Google Scholar] [CrossRef]
- Vowden, P. Leg ulcers: Assessment and management. Indep. Nurse 2010, 11, 30–33. [Google Scholar] [CrossRef]
- Afonso, A.; Barroso, P.; Marques, G.; Gonçalves, A.; Gonzalez, A.; Duarte, N.; Ferreira, M.J. Chronic leg ulcer-experience with 50 patients. Angiol. Cir. Vasc. 2013, 9, 148–153. [Google Scholar] [CrossRef]
- Parker, C.N.; Finlayson, K.J.; Shuter, P.; Edwards, H.E. Risk factors for delayed healing in venous leg ulcers: A review of the literature. Int. J. Clin. 2015, 69, 967–977. [Google Scholar] [CrossRef]
- Soldevilla, J.; Torra, J.E.; Verdu, J.; Rueda, J.; Martinez, F.; Roche, E. Epidemiology of chronic wounds in Spain: Results of the first national studies on pressure and leg ulcer prevalence. Wounds 2006, 18, 213–226. [Google Scholar]
- Okazaki, J.; Matsuda, D.; Tanaka, K.; Ishida, M.; Kuma, S.; Morisaki, K.; Furuyama, T.; Maehara, Y. Analysis of wound healing time and wound-free period as outcomes after surgical and endovascular revascularization for critical lower limb ischemia. J. Vasc. Surg. 2017, 67, 817–825. [Google Scholar] [CrossRef]
- Graves, N.; Zheng, H. The prevalence and incidence of chronic wounds: A literature review. Wound Pract. Res. 2014, 22, 14–19. [Google Scholar]
- Persoon, A.; Heinen, M.M.; van der Vleuten, C.J.; de Rooij, M.J.; van de Kerkhof, P.C.; van Achterberg, T. Leg ulcers: A review of their impact on daily life. J. Clin. Nurs. 2004, 13, 341–354. [Google Scholar] [CrossRef]
- O’Rourke, D.; Orchard, M.T.; Dyck, D.; Gross, P.; Guzman, R.; Junaid, A.; Koulack, J.; Thomson, L.; Zettler, N. Winnipeg Regional Health Authority. In Regional Wound Care Clinical Practice Guidelines: Venous, Arterial, and Mixed Lower Leg Ulcers; Winnipeg Regional Health Authority: Winnipeg, MB, Canada, 2016. [Google Scholar]
- O’Meara, S.; Cullum, N.; Nelson, E.A.; Dumville, J.C. Compression for venous leg ulcers. Cochrane Database Syst. Rev. 2012, 11, CD000265. [Google Scholar] [CrossRef]
- O’Meara, S.; Martyn-St James, M. Foam dressings for venous leg ulcers. Cochrane Database Syst. Rev. 2013, 5, CD009907. [Google Scholar] [CrossRef]
- Wlaschek, M.; Scharffetter-Kochanek, K. Oxidative stress in chronic venous leg ulcers. Wound Repair Regen. 2005, 13, 452–461. [Google Scholar] [CrossRef]
- Loots, M.A.; Lamme, E.N.; Zeegelaar, J.; Mekkes, J.R.; Bos, J.D.; Middelkoop, E. Differences in cellular infiltrate and extracellular matrix of chronic diabetic and venous ulcers versus acute wounds. J. Investig. Dermatol. 1998, 111, 850–857. [Google Scholar] [CrossRef]
- Schultz, G.S.; Wysocki, A. Interactions between extracellular matrix and growth factors in wound healing. Wound Repair Regen. 2009, 17, 153–162. [Google Scholar] [CrossRef]
- Cervelli, V.; Lucarini, L.; Spallone, D.; Palla, L.; Colicchia, G.M.; Gentile, P.; De Angelis, B. Use of platelet-rich plasma and hyaluronic acid in the loss of substance with bone exposure. Adv. Skin Wound Care 2011, 24, 176–181. [Google Scholar] [CrossRef]
- Baum, C.L.; Arpey, C.J. Normal cutaneous wound healing: Clinical correlation with cellular and molecular events. Dermatol. Surg. 2005, 31, 674–686. [Google Scholar] [CrossRef]
- Schultz, G.S.; Ladwig, G.; Wysocki, A. Extracellular matrix: Review of its roles in acute and chronic wounds. World Wide Wounds 2005, 2005, 1–18. [Google Scholar]
- Ågren, M.S.; Werthén, M. The extracellular matrix in wound healing: A closer look at therapeutics for chronic wounds. Int. J. Low Extrem. Wounds 2007, 6, 82–97. [Google Scholar] [CrossRef]
- Consensus, I. Acellular Matrices for the Treatment of Wounds and Expert Working Group Review; Wounds International: London, UK, 2010. [Google Scholar]
- Snyder, D.L.; Sullivan, N.; Schoelles, K.M. Skin Substitutes for Treating Chronic Wounds; Agency for Healthcare Research and Quality: Washington, DC, USA, 2012.
- Hughes, O.B.; Rakosi, A.; Macquhae, F.; Herskovitz, I.; Fox, J.D.; Kirsner, R.S. A review of cellular and acellular matrix products: Indications, techniques, and outcomes. Plast. Reconstr. Surg. 2016, 138 (Suppl. 3), 138S–147S. [Google Scholar] [CrossRef]
- Nataraj, C.; Ritter, G.; Dumas, S.; Helfer, B.S.; Brunelle, J.; Sander, T.W. Extracellular wound matrices: Novel stabilisation and sterilisation method for collagen-based biologic wound dressings. Wounds 2007, 19, 148–156. [Google Scholar]
- Mostow, E.N.; Haraway, G.D.; Dalsing, M.; Hodde, J.P.; King, D. Effectiveness of an extracellular matrix graft (OASIS Wound Matrix) in the treatment of chronic leg ulcers: A randomized clinical trial. J. Vasc. Surg. 2005, 41, 837. [Google Scholar] [CrossRef]
- Winters, C.L.; Brigido, S.A.; Liden, B.A.; Simmons, M.; Hartman, J.F.; Wright, M.L. A multicenter study involving the use of a human acellular dermal regenerative tissue matrix for the treatment of diabetic lower extremity wounds. Adv. Skin Wound Care 2008, 21, 375. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, B.; Orlandi, F.; D’Autilio, F.L.M.; Scioli, M.G.; Orlandi, A.; Cervelli, V.; Gentile, P. Long-term follow-up comparison of two different bi-layer dermal substitutes in tissue regeneration: Clinical outcomes and histological findings. Int. Wound J. 2018. [Google Scholar] [CrossRef]
- Schuklenk, U.; Ashcroft, R. International research ethics. Bioethics 2000, 14, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Kotlyar, A.A.; Vered, Z.; Goldberg, I.; Chouraqui, P.; Nas, D.; Fridman, E.; Chen-Levy, Z.; Fytlovich, S.; Sangiorgi, G.; Spagnoli, L.G.; et al. Insulin-like growth factor I and II pre serve myocardial structure in postinfarct swine. Heart 2001, 86, 693. [Google Scholar] [CrossRef]
- Cervelli, V.; Gentile, P.; De Angelis, B.; Calabrese, C.; Di Stefani, A.; Scioli, M.G.; Curcio, B.C.; Felici, M.; Orlandi, A. Application of enhanced stromal vascular fraction and fat grafting mixed with PRP in post-traumatic lower extremity ulcers. Stem Cell Res. 2011, 6, 103. [Google Scholar] [CrossRef]
- Matera, M.G.; Calzetta, L.; Passeri, D.; Facciolo, F.; Rendina, E.A.; Page, C.; Cazzola, M.; Orlandi, A. Epithelium integrity is crucial for the relaxant activity of brain natriuretic peptide in human isolated bronchi. Br. J. Pharmacol. 2011, 163, 1740–1754. [Google Scholar] [CrossRef]
- Scioli, M.G.; Stasi, M.A.; Passeri, D.; Doldo, E.; Costanza, G.; Camerini, R.; Fociani, P.; Arcuri, G.; Lombardo, K.; Pace, S.; et al. Propionyl-L-carnitine is efficacious in ulcerative colitis through its action on the immune function and microvasculature. Clin. Transl. Gastroenterol. 2014, 20, 5. [Google Scholar] [CrossRef]
- Greaves, N.S.; Iqbal, S.A.; Baguneid, M.; Bayat, A. The role of skin substitutes in the management of chronic cutaneous wounds. Wound Repair Regen. 2013, 21, 194. [Google Scholar] [CrossRef]
- Shiraki, T.; Iida, O.; Takahara, M.; Soga, Y.; Mii, S.; Okazaki, J.; Kuma, S.; Yamaoka, T.; Kamoi, D.; Shintani, Y.; et al. Comparison of Clinical Outcomes after Surgical and Endovascular Revascularization in Haemodialysis Patients with Critical Limb Ischemia. J. Atheroscler. Thromb. 2017, 2017, 35915. [Google Scholar]
- Robinson, W.P.; Loretz, L.; Hanesian, C.; Flahive, J.; Bostrom, J.; Lunig, N.; Schanzer, A.; Messina, L. Society for Vascular Surgery Wound, Ischemia, foot Infection (WIfI) score correlates with the intensity of multimodal limb treatment and patient-centered outcomes in patients with threatened limbs managed in a limb preservation center. J. Vasc. Surg. 2017, 66, 488–498. [Google Scholar] [CrossRef]
- Reed, G.W.; Salehi, N.; Giglou, P.R.; Kafa, R.; Malik, U.; Maier, M.; Shishehbor, M.H. Time to Wound Healing and Major Adverse Limb Events in Patients with Critical Limb Ischemia Treated with Endovascular Revascularization. Ann. Vasc. Surg. 2016, 36, 190–198. [Google Scholar] [CrossRef]
- Reed, G.W.; Raeisi-Giglou, P.; Kafa, R.; Malik, U.; Salehi, N.; Shishehbor, M.H. Hospital Readmissions Following Endovascular Therapy for Critical Limb Ischemia: Associations with Wound Healing, Major Adverse Limb Events, and Mortality. J. Am. Heart Assoc. 2016, 5, e003168. [Google Scholar] [CrossRef]
- Nicoli, F.; Balzani, A.; Lazzeri, D.; Gentile, P.; Chilgar, R.M.; Di Pasquali, C.; Nicoli, M.; Bocchini, I.; Agovino, A.; Cervelli, V. Severe hidradenitis suppurativa treatment using platelet-rich plasma gel and Hyalomatrix. Int Wound J. 2015, 12, 338–343. [Google Scholar] [CrossRef]
- Gentile, P.; Colicchia, G.M.; Nicoli, F.; Cervelli, G.; Curcio, C.B.; Brinci, L.; Cervelli, V. Complex abdominal wall repair using a porcine dermal matrix. Surg Innov. 2013, 20, NP12-5. [Google Scholar] [CrossRef]
- Tchero, H.; Herlin, C.; Bekara, F.; Pauline Kangambega, P.; Fluieraru, S.; Teot, L. Failure rates of artificial dermis products in treatment of diabetic foot ulcer: A systematic review and network meta-analysis. Wound Rep. Reg. 2017, 25, 691–696. [Google Scholar] [CrossRef]
- Rehfeldt, F.; Engler, A.J.; Eckhardt, A.; Ahmed, F.; Discher, D.E. Cell responses to the mechanochemical microenvironment—Implications for regenerative medicine and drug delivery. Adv. Drug Deliv. Rev. 2007, 59, 1329. [Google Scholar] [CrossRef]
- Engler, A.J.; Sen, S.; Sweeney, H.L.; Discher, D.E. Matrix elasticity directs stem cell lineage specification. Cell 2006, 126, 677. [Google Scholar] [CrossRef]
- Sridharan, R.; Cameron, A.R.; Kelly, D.J.; Kearney, C.J.; O’Brien, F.J. Biomaterial based modulation of macrophage polarization: A review and suggested design principles. Mater. Today 2015, 18, 313–325. [Google Scholar] [CrossRef]
- Spiller, K.L.; Anfang, R.R.; Spiller, K.J.; Ng, J.; Nakazawa, K.R.; Daulton, J.W.; Vunjak-Novakovic, G. The role of macrophage phenotype in vascularization of tissue engineering scaffolds. Biomaterials 2014, 35, 4477–4488. [Google Scholar] [CrossRef]
- Agrawal, H.; Tholpady, S.S.; Capito, A.E.; Drake, D.B.; Katz, A.J. Macrophage phenotypes correspond with remodeling outcomes of various acellular dermal matrices. Open J. Regen. Med. 2012, 1, 51–59. [Google Scholar] [CrossRef]
- Sindrilaru, A.; Scharffetter-Kochanek, K. Disclosure of the Culprits: Macrophages-Versatile Regulators of Wound Healing. Adv. Wound Care 2013, 2, 357–368. [Google Scholar] [CrossRef]
- Sindrilaru, A.; Peters, T.; Wieschalka, S.; Baican, C.; Baican, A.; Peter, H.; Hainzl, A.; Schatz, S.; Qi, Y.; Schlecht, A.; et al. An unrestrained proinflammatory M1 macrophage population induced by iron impairs wound healing in humans and mice. J. Clin. Investig. 2011, 1, 985–997. [Google Scholar] [CrossRef]
- Romanelli, M.; Dini, V.; Bertone, M.S. Randomized comparison of OASIS wound matrix versus moist wound dressing in the treatment of difficult-to-heal wounds of mixed arterial/venous etiology. Adv. Skin Wound Care 2010, 23, 34–38. [Google Scholar] [CrossRef]
- Shores, J.T.; Gabriel, A.; Gupta, S. Skin substitutes and alternatives: A review. Adv. Skin Wound Care 2007, 20, 493. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Age | Gender | Texas | Ø Ulcer T0 (cm) | Comorbidity |
|---|---|---|---|---|---|
| 1 | 24 | M | 1B | 5 × 4 | DM, HPT, DR |
| 2 | 39 | F | 1B | 8 × 4 | VI |
| 3 | 45 | M | 1D | 11 × 4 | HPT, DLP |
| 4 | 82 | M | 1C | 5 × 3 | HPT, HF, HFTUS, VI, P |
| 5 | 77 | M | 1D | 9 × 4 | HPT, HF, DM, DLP, DR |
| 6 | 38 | F | 1D | 5 × 3 | VI |
| 7 | 59 | M | 1D | 3 × 2 | VI |
| 8 | 61 | M | 1D | 4 × 8 | DM, DLP, DR |
| 9 | 54 | M | 1D | 2 × 2 | DM, HPT, HF, VI, DLP, OB |
| 10 | 67 | M | 1B | 4 × 3 | DM, DLP, HF, KFC, DR |
| 11 | 72 | M | 1D | 5 × 10 | HF, KFC, DLP, VI, HPT |
| 12 | 74 | F | 1C | 7 × 5 | HF, KFC, DLP, HPT |
| 13 | 75 | F | 1C | 2 × 2 | DLP, DM |
| 14 | 38 | F | 1C | 5 × 2 | KFC, HPT |
| 15 | 33 | F | 1D | 12 × 4 | DM, KFC, HF, A, VI, HPT, DR |
| 16 | 77 | M | 1D | 7 × 5 | HF, VI, HPT |
| 17 | 60 | F | 1D | 15 × 5 | DM, HF, HPT, DR |
| 18 | 41 | F | 1D | 8 × 2 | DM, HF, HPT, DR |
| 19 | 66 | M | 1D | 6 × 4 | HF, VI |
| 20 | 81 | F | 1D | 8 × 5 | VI, HF |
| 21 | 40 | M | 1D | 3 × 2 | KFC, HF, DM, A, HPT |
| 22 | 69 | F | 1D | 8 × 5 | VI |
| 23 | 54 | M | 1D | 5 × 3 | DM, VI, |
| 24 | 72 | F | 2D | 6 × 8 | DM, HPT, HF, VI |
| 25 | 44 | F | 1D | 9 × 5 | VI |
| 26 | 67 | M | 2C | 3 × 6 | DM, HPT, DLP |
| 27 | 78 | M | 1D | 3 × 8 | DM, HPT, KFC, DR |
| 28 | 63 | M | 1D | 7 × 8 | DM, HPT, DLP, DR |
| 29 | 93 | F | 1D | 5 × 6 | DM 1, KFC, DR, A, DN |
| 30 | 87 | M | 2B | 10 × 8 | DM, HPT, DLP, KFC, HF |
| 31 | 33 | M | 2C | 7 × 5 | DM, HPT, HF, VI, KFC, DLP, DR |
| 32 | 80 | F | 2D | 15 × 12 | HF, DM, DR, HPT, KFC, VI |
| 33 | 71 | M | 2B | 6 × 6 | VI, OB |
| 34 | 83 | F | 2B | 7 × 8 | DM, HPT, KFC, HF, DLP |
| 35 | 70 | M | 2B | 2 × 3 | VI, A, HF |
| NEVELIA® | |
|---|---|
| Description | NEVELIA bi-layer matrix is a sterile matrix consisting of a type I, purified, stabilized, bovine origin collagen to promote dermal regeneration becoming a vascularised tissue that is histologically very close to the normal dermis and a polyester reinforced silicone layer acting as a pseudo-epidermis. The extraction procedure and the freeze-drying process allow the structure of the collagen into a matrix with optimal hydrophily, pore structure and pore size (20–125 μm). Collagen shows a native 3D open cells structure and absence of Glycosaminoglycans (GAG) to improve cells attachments. NEVELIA® can be used in combination with a thin split thickness skin graft to recreate skin resembling normal skin in terms of function and appearance. |
| Procedure | 1 Wound excision: NEVELIA® bi-layer matrix must be applied to clean wounds freshly excised under standard operating conditions after excision of all the dead tissue on and around the graft zone. 2 Implantation of NEVELIA® bi-layer matrix: The matrix must be placed in the excised wound precisely to allow an airtight edge-to-edge joint between the healthy skin and the matrix and reduce the risk of bacterial infection. The matrix can be attached with surgical staples or sutures 3 Plantation of thin split thickness skin graft: The silicone layer is removed after 28 days and, at the same time, the thin split thickness skin graft will be applied (ensure that no hematoma, fluid build-up or infection is present). The staples or sutures must remain in place until the thin split thickness skin graft takes place (about three weeks). |
| Indication for use | NEVELIA® is indicated for dermal regeneration in individuals with skin loss, particularly in the following fields: Burns surgery (third and deep second degree burns), Reconstructive plastic surgery, Traumatology, Chronic Ulcers (including leg ulcers and diabetic foot). It is particularly useful for patients who are unable to supply sufficient donor skin for an autograft at the time of excision or to accelerate the healing in high-risk patients. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Angelis, B.; Orlandi, F.; Morais D’Autilio, M.F.L.; Di Segni, C.; Scioli, M.G.; Orlandi, A.; Cervelli, V.; Gentile, P. Vasculogenic Chronic Ulcer: Tissue Regeneration with an Innovative Dermal Substitute. J. Clin. Med. 2019, 8, 525. https://doi.org/10.3390/jcm8040525
De Angelis B, Orlandi F, Morais D’Autilio MFL, Di Segni C, Scioli MG, Orlandi A, Cervelli V, Gentile P. Vasculogenic Chronic Ulcer: Tissue Regeneration with an Innovative Dermal Substitute. Journal of Clinical Medicine. 2019; 8(4):525. https://doi.org/10.3390/jcm8040525
Chicago/Turabian StyleDe Angelis, Barbara, Fabrizio Orlandi, Margarida Fernandes Lopes Morais D’Autilio, Chiara Di Segni, Maria Giovanna Scioli, Augusto Orlandi, Valerio Cervelli, and Pietro Gentile. 2019. "Vasculogenic Chronic Ulcer: Tissue Regeneration with an Innovative Dermal Substitute" Journal of Clinical Medicine 8, no. 4: 525. https://doi.org/10.3390/jcm8040525
APA StyleDe Angelis, B., Orlandi, F., Morais D’Autilio, M. F. L., Di Segni, C., Scioli, M. G., Orlandi, A., Cervelli, V., & Gentile, P. (2019). Vasculogenic Chronic Ulcer: Tissue Regeneration with an Innovative Dermal Substitute. Journal of Clinical Medicine, 8(4), 525. https://doi.org/10.3390/jcm8040525