Apparent Diffusion Coefficient Is a Novel Imaging Biomarker of Myopathic Changes in Liver Cirrhosis

 , ,
, ,
Abstract
1. Introduction
2. Methods
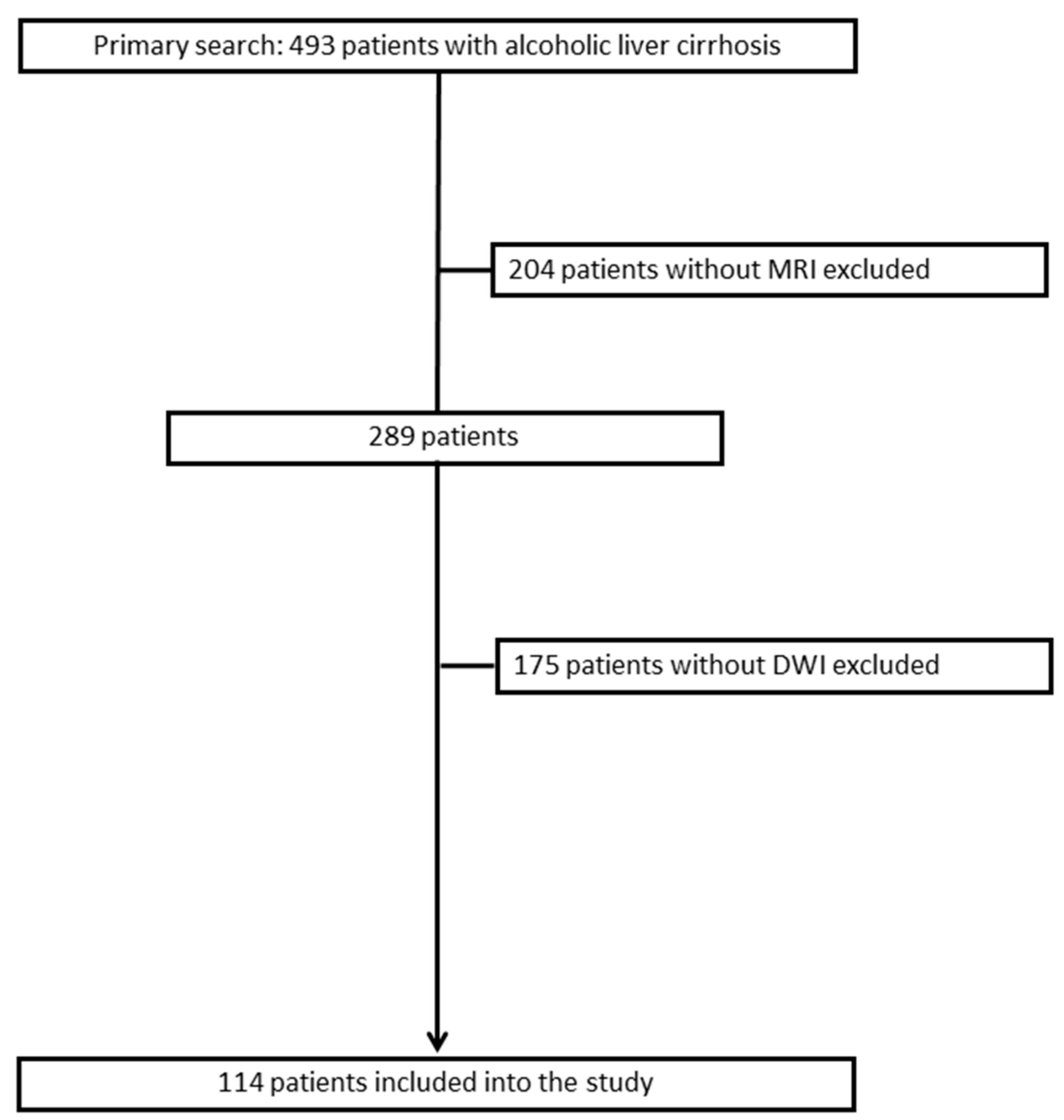
2.1. Patients
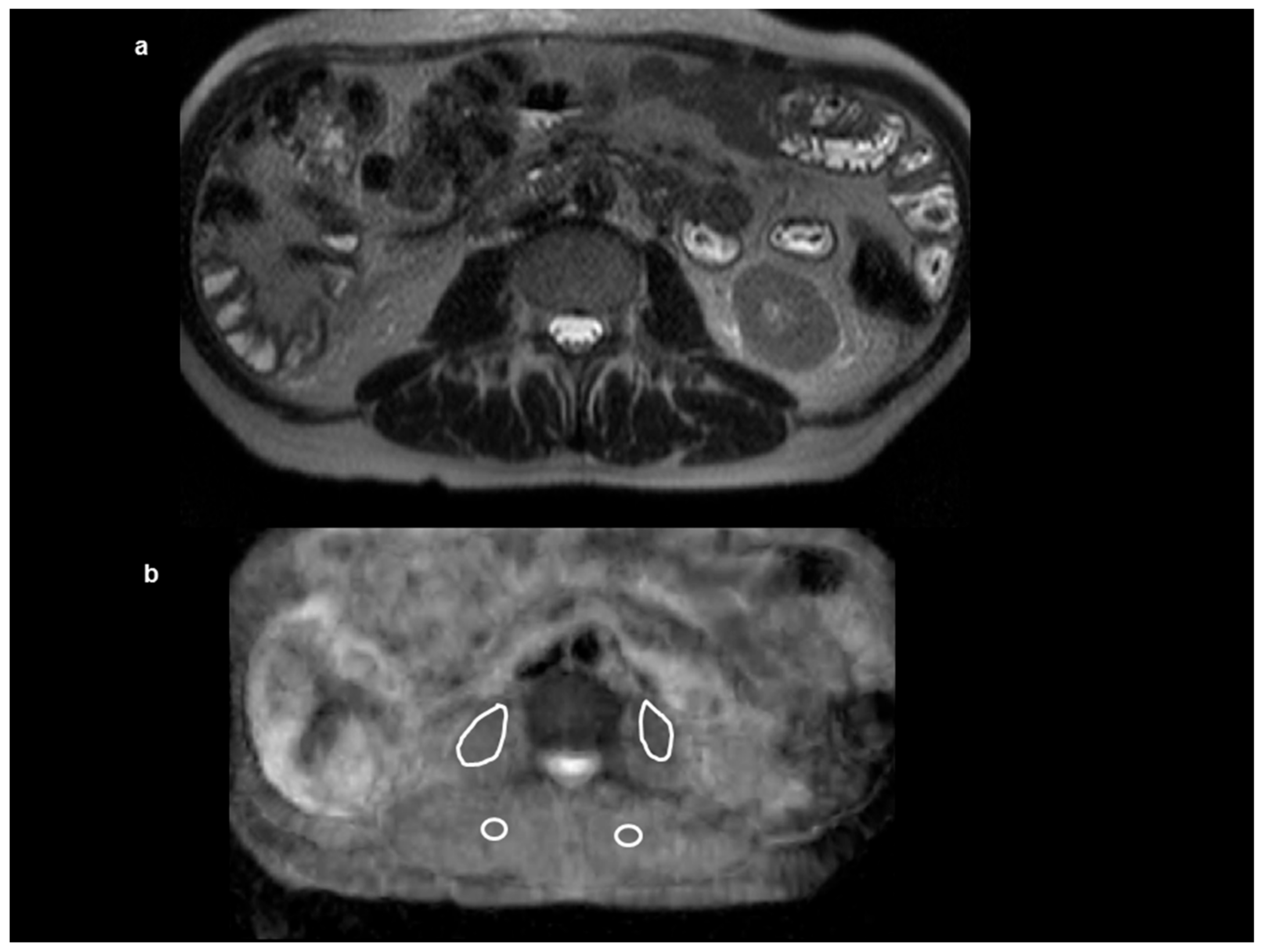
2.2. Diffusion Weighted Imaging and ADC Measurement
2.3. Statistical Analysis
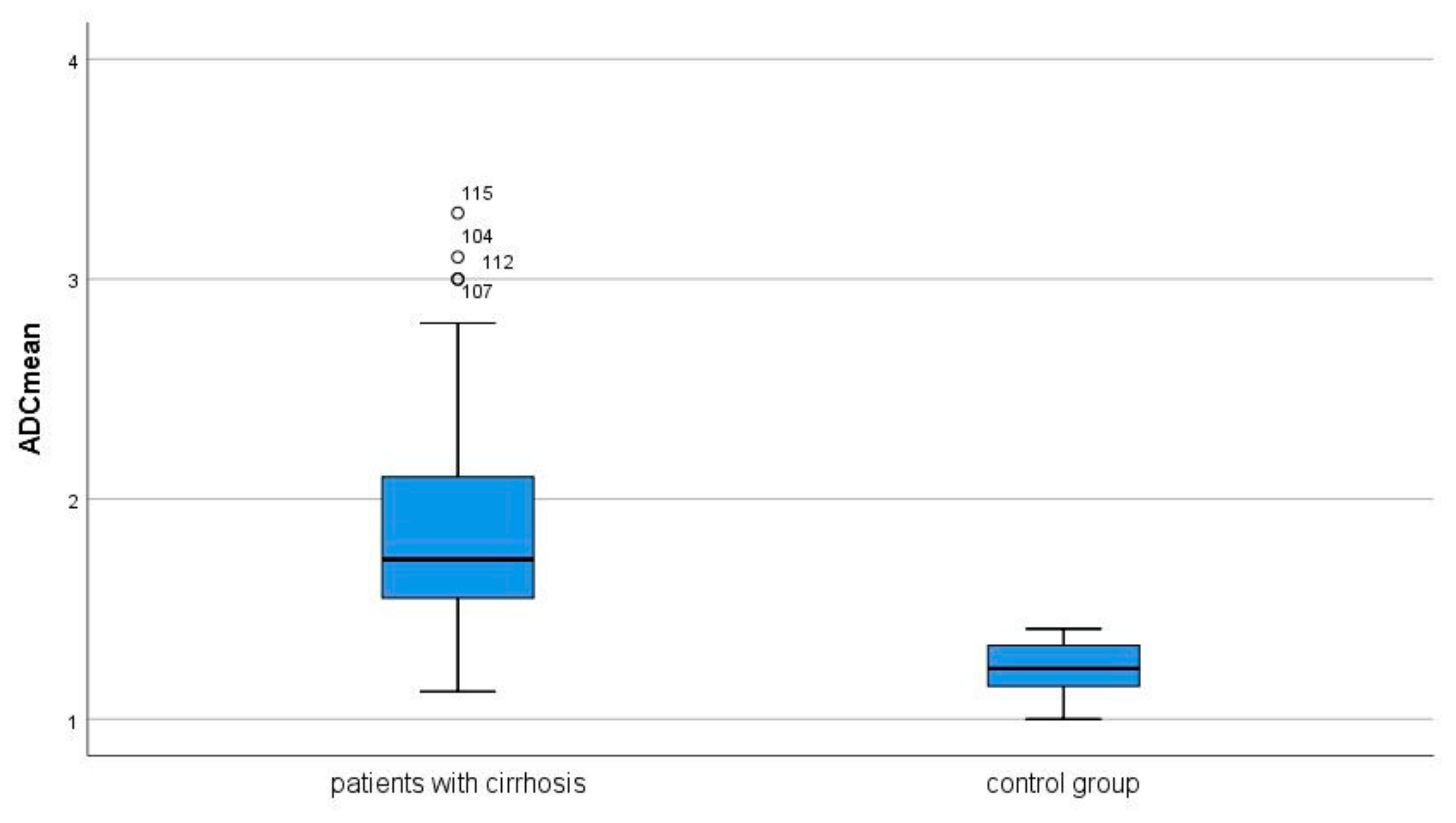
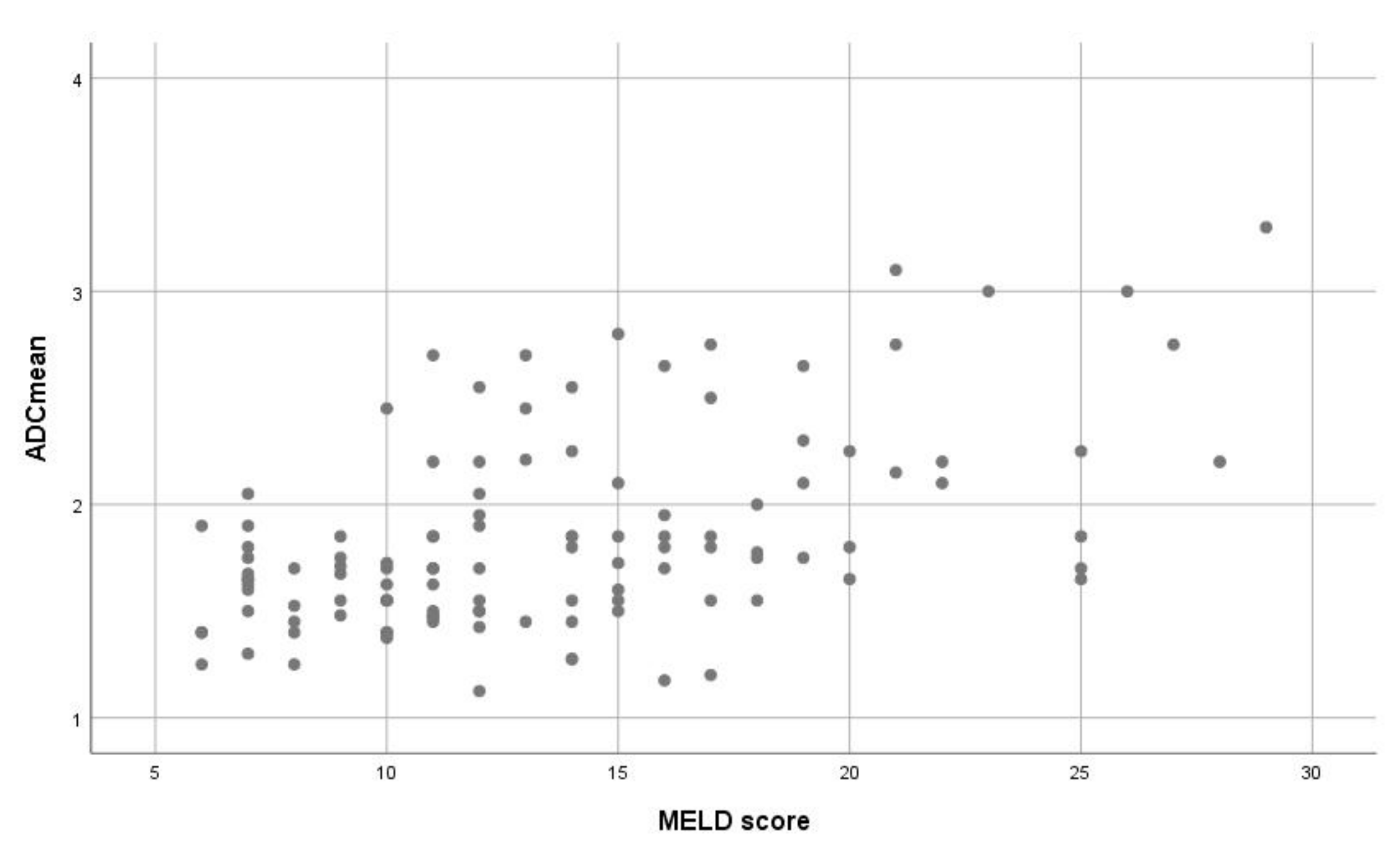
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Montano-Loza, A.J. Clinical relevance of sarcopenia in patients with cirrhosis. World J. Gastroenterol. 2014, 20, 8061–8071. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, S. Myostatin and beyond in cirrhosis: All roads lead to sarcopenia. J. Cachexia Sarcopenia Muscle 2017, 8, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Montano-Loza, A.J.; Angulo, P.; Meza-Junco, J.; Prado, C.M.; Sawyer, M.B.; Beaumont, C.; Esfandiari, N.; Ma, M.; Baracos, V.E. Sarcopenic obesity and myosteatosis are associated with higher mortality in patients with cirrhosis. J. Cachexia Sarcopenia Muscle 2016, 7, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, S.; Merli, M. Sarcopenia from mechanism to diagnosis and treatment in liver disease. J. Hepatol. 2016, 65, 1232–1244. [Google Scholar] [CrossRef] [PubMed]
- Kalafateli, M.; Mantzoukis, K.; Choi Yau, Y.; Mohammad, A.O.; Arora, S.; Rodrigues, S.; de Vos, M.; Papadimitriou, K.; Thorburn, D.; O’Beirne, J.; et al. Malnutrition and sarcopenia predict post-liver transplantation outcomes independently of the Model for End-stage Liver Disease score. J. Cachexia Sarcopenia Muscle 2017, 8, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Davuluri, G.; Silva, R.N.E.; Engelen, M.; Ten Have, G.A.M.; Prayson, R.; Deutz, N.E.P.; Dasarathy, S. Ammonia lowering reverses sarcopenia of cirrhosis by restoring skeletal muscle proteostasis. Hepatology 2017, 65, 2045–2058. [Google Scholar] [CrossRef] [PubMed]
- Davuluri, G.; Allawy, A.; Thapaliya, S.; Rennison, J.H.; Singh, D.; Kumar, A.; Sandlers, Y.; Van Wagoner, D.R.; Flask, C.A.; Hoppel, C.; et al. Hyperammonaemia-induced skeletal muscle mitochondrial dysfunction results in cataplerosis and oxidative stress. J. Physiol. 2016, 594, 7341–7360. [Google Scholar] [CrossRef] [PubMed]
- Lee, O.J.; Yoon, J.H.; Lee, E.J.; Kim, H.J.; Kim, T.H. Acute myopathy associated with liver cirrhosis. World J. Gastroenterol. 2006, 12, 2254–2258. [Google Scholar] [CrossRef] [PubMed]
- Montano-Loza, A.J.; Meza-Junco, J.; Prado, C.M.; Lieffers, J.R.; Baracos, V.E.; Bain, V.G.; Sawyer, M.B. Muscle wasting is associated with mortality in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2012, 10, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Tandon, P.; Ney, M.; Irwin, I.; Ma, M.M.; Gramlich, L.; Bain, V.G.; Esfandiari, N.; Baracos, V.; Montano-Loza, A.J.; Myers, R.P. Severe muscle depletion in patients on the liver transplant wait list: Its prevalence and independent prognostic value. Liver Transpl. 2012, 18, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Periyalwar, P.; Dasarathy, S. Malnutrition in cirrhosis: Contribution and consequences of sarcopenia on metabolic and clinical responses. Clin. Liver Dis. 2012, 16, 95–131. [Google Scholar] [CrossRef] [PubMed]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Ohnishi, S.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M.; Moriwaki, H. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition 2015, 31, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Sergi, G.; Trevisan, C.; Veronese, N.; Lucato, P.; Manzato, E. Imaging of sarcopenia. Eur. J. Radiol. 2016, 85, 1519–1524. [Google Scholar] [CrossRef] [PubMed]
- Sinelnikov, A.; Qu, C.; Fetzer, D.T.; Pelletier, J.S.; Dunn, M.A.; Tsung, A.; Furlan, A. Measurement of skeletal muscle area: Comparison of CT and MR imaging. Eur. J. Radiol. 2016, 85, 1716–1721. [Google Scholar] [CrossRef] [PubMed]
- Cespedes Feliciano, E.M.; Avrutin, E.; Caan, B.J.; Boroian, A.; Mourtzakis, M. Screening for low muscularity in colorectal cancer patients: A valid, clinic-friendly approach that predicts mortality. J. Cachexia Sarcopenia Muscle 2018. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Kang, S.H.; Kim, M.Y.; Baik, S.K. Prognostic value of sarcopenia in patients with liver cirrhosis: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186990. [Google Scholar] [CrossRef] [PubMed]
- Praktiknjo, M.; Book, M.; Luetkens, J.; Pohlmann, A.; Meyer, C.; Thomas, D.; Jansen, C.; Feist, A.; Chang, J.; Grimm, J.; et al. Fat-free muscle mass in magnetic resonance imaging predicts acute-on-chronic liver failure and survival in decompensated cirrhosis. Hepatology 2018, 67, 1014–1026. [Google Scholar] [CrossRef] [PubMed]
- Fornasa, F. Diffusion-weighted magnetic resonance imaging: What makes water run fast or slow? J. Clin. Imaging Sci. 2011, 1, 27. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Meyer, H.J.; Wienke, A. Correlation between apparent diffusion coefficient (ADC) and cellularity is different in several tumors: A meta-analysis. Oncotarget 2017, 8, 59492–59499. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Meyer, H.J.; Wienke, A. Associations between apparent diffusion coefficient (ADC) and KI 67 in different tumors: A meta-analysis. Part 1: ADCmean. Oncotarget 2017, 8, 75434–75444. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Does, M.D.; Gore, J.C. Sensitivity of MR diffusion measurements to variations in intracellular structure: Effects of nuclear size. Magn. Reson. Med. 2009, 61, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Hamerla, G.; Meyer, H.J.; Winter, K.; Schob, S.; Fiedler, E. Whole lesion histogram analysis of meningiomas derived from ADC values. Correlation with several cellularity parameters, proliferation index KI 67, nucleic content, and membrane permeability. Magn. Reson. Imaging 2018, 51, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.J.; Ziemann, O.; Kornhuber, M.; Emmer, A.; Quäschling, U.; Schob, S.; Surov, A. Apparent diffusion coefficient (ADC) does not correlate with different serological parameters in myositis and myopathy. Acta Radiol. 2018, 59, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.J.; Emmer, A.; Kornhuber, M.; Surov, A. Diffusion weighted MRI in myositis—The value of ADC histogram analysis. Br. J. Radiol. 2018, 1085, 20170900. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.J.; Emmer, A.; Kornhuber, M.; Surov, A. Associations between apparent diffusion coefficient and electromyography parameters in myositis. Brain Behav. 2018, 8, e00958. [Google Scholar] [CrossRef] [PubMed]
- Befeler, A.S.; Palmer, D.E.; Hoffman, M.; Longo, W.; Solomon, H.; Di Bisceglie, A.M. The safety of intra-abdominal surgery in patients with cirrhosis: Model for end-stage liver disease score is superior to Child-Turcotte-Pugh classification in predicting outcome. Arch. Surg. 2005, 140, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Kim, W.R. The model for end-stage liver disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, M.; Eida, S.; Sumi, M.; Nakamura, T. Apparent diffusion coefficient mapping for sinonasal diseases: Differentiation of benign and malignant lesions. AJNR Am. J. Neuroradiol. 2011, 32, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Garnov, N. Proving of a mathematical model of cell calculation based on apparent diffusion coefficient. Transl. Oncol. 2017, 10, 828–830. [Google Scholar] [CrossRef] [PubMed]
- Holl, N.; Echaniz-Laguna, A.; Bierry, G.; Mohr, M.; Loeffler, J.P.; Moser, T.; Dietemann, J.L.; Kremer, S. Diffusion-weighted MRI of denervated muscle: A clinical and experimental study. Skeletal Radiol. 2008, 37, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, X.; Guan, M.; Li, C.; Luo, L. Skeletal muscle evaluation by MRI in a rabbit model of acute ischaemia. Br. J. Radiol. 2013, 86, 20120042. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, O.; Shimao, D.; Maruyama, K.; Nielsen, M. Evaluation of exercised or cooled skeletal muscle on the basis of diffusion-weighted magnetic resonance imaging. Eur. J. Appl. Physiol. 2009, 105, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Morvan, D.; Leroy-Willig, A. Simultaneous measurements of diffusion and transverse relaxation in exercising skeletal muscle. Magn. Reson. Imaging 1995, 13, 943–948. [Google Scholar] [CrossRef]
- Kilgour, A.H.; Firth, C.; Harrison, R.; Moss, P.; Bastin, M.E.; Wardlaw, J.M.; Deary, I.J.; Starr, J.M. Seropositivity for CMV and IL-6 levels are associated with grip strength and muscle size in the elderly. Immun. Ageing 2013, 10, 33. [Google Scholar] [CrossRef] [PubMed]
- Pin, F.; Barreto, R.; Kitase, Y.; Mitra, S.; Erne, C.E.; Novinger, L.J.; Zimmers, T.A.; Couch, M.E.; Bonewald, L.F.; Bonetto, A. Growth of ovarian cancer xenografts causes loss of muscle and bone mass: A new model for the study of cancer cachexia. J. Cachexia Sarcopenia Muscle 2018. [Google Scholar] [CrossRef] [PubMed]
- Westbury, L.D.; Fuggle, N.R.; Syddall, H.E.; Duggal, N.A.; Shaw, S.C.; Maslin, K.; Dennison, E.M.; Lord, J.M.; Cooper, C. Relationships between markers of inflammation and muscle mass, strength and function: Findings from the hertfordshire cohort study. Calcif. Tissue Int. 2018, 102, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C. Inflammatory muscle diseases. N. Engl. J. Med. 2015, 372, 1734–1747. [Google Scholar] [CrossRef] [PubMed]
- Englesbe, M.J.; Patel, S.P.; He, K.; Lynch, R.J.; Schaubel, D.E.; Harbaugh, C.; Holcombe, S.A.; Wang, S.C.; Segev, D.L.; Sonnenday, C.J. Sarcopenia and mortality after liver transplantation. J. Am. Coll. Surg. 2010, 211, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, J.; Shasthry, V.; Kaal, C.R.; Anand, L.; Bhardwaj, A.; Pandit, V.; Arora, A.; Rajesh, S.; Pamecha, V.; Jain, V.; et al. Characterization of body composition and definition of sarcopenia in patients with alcoholic cirrhosis: A computed tomography based study. Liver Int. 2017, 37, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Ponrartana, S.; Andrade, K.E.; Wren, T.A.; Ramos-Platt, L.; Hu, H.H.; Bluml, S.; Gilsanz, V. Repeatability of chemical-shift-encoded water-fat MRI and diffusion-tensor imaging in lower extremity muscles in children. Am. J. Roentgenol. 2014, 202, W567–W573. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MELD Score 0–9 | MELD Score 10–19 | MELD Score > 20 |
|---|---|---|
| 1.61 ± 0.21 × 10−3 mm2 s−1 p = 0.055 vs. MELD score 10–19; p = 0.001 vs. MELD score > 20 | 1.83 ± 0.42 × 10−3 mm2 s−1 p = 0.001 vs. MELD score > 20 | 2.34 ± 0.54 × 10−3 mm2 s−1 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Surov, A.; Paul, L.; Meyer, H.J.; Schob, S.; Engelmann, C.; Wienke, A. Apparent Diffusion Coefficient Is a Novel Imaging Biomarker of Myopathic Changes in Liver Cirrhosis. J. Clin. Med. 2018, 7, 359. https://doi.org/10.3390/jcm7100359
Surov A, Paul L, Meyer HJ, Schob S, Engelmann C, Wienke A. Apparent Diffusion Coefficient Is a Novel Imaging Biomarker of Myopathic Changes in Liver Cirrhosis. Journal of Clinical Medicine. 2018; 7(10):359. https://doi.org/10.3390/jcm7100359
Chicago/Turabian StyleSurov, Alexey, Lisa Paul, Hans Jonas Meyer, Stefan Schob, Cornelius Engelmann, and Andreas Wienke. 2018. "Apparent Diffusion Coefficient Is a Novel Imaging Biomarker of Myopathic Changes in Liver Cirrhosis" Journal of Clinical Medicine 7, no. 10: 359. https://doi.org/10.3390/jcm7100359
APA StyleSurov, A., Paul, L., Meyer, H. J., Schob, S., Engelmann, C., & Wienke, A. (2018). Apparent Diffusion Coefficient Is a Novel Imaging Biomarker of Myopathic Changes in Liver Cirrhosis. Journal of Clinical Medicine, 7(10), 359. https://doi.org/10.3390/jcm7100359