A Modified Two-Step Screening Strategy for Gestational Diabetes Mellitus Based on the 2013 WHO Criteria by Combining the Glucose Challenge Test and Clinical Risk Factors

 ,
, 
 ,
, 
Abstract
1. Introduction
2. Subjects and Methods
2.1. Study Design
2.2. Study Participants
2.3. Study Assessments
2.4. Statistical Analysis
3. Results
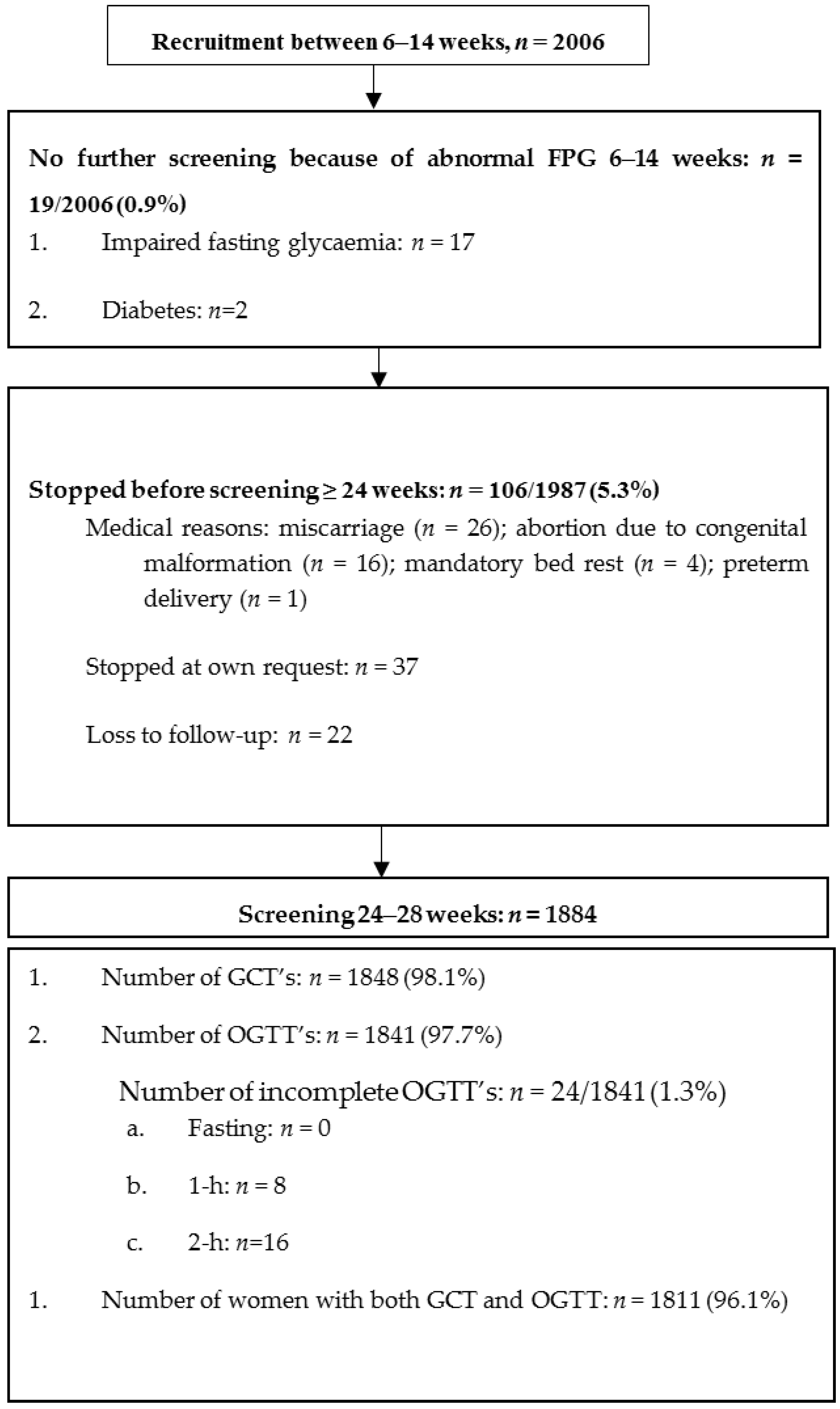
3.1. Study Participants
3.2. Characteristics of Women with GDM Who Would be Missed Using a GCT Threshold of 7.2 mmol/L
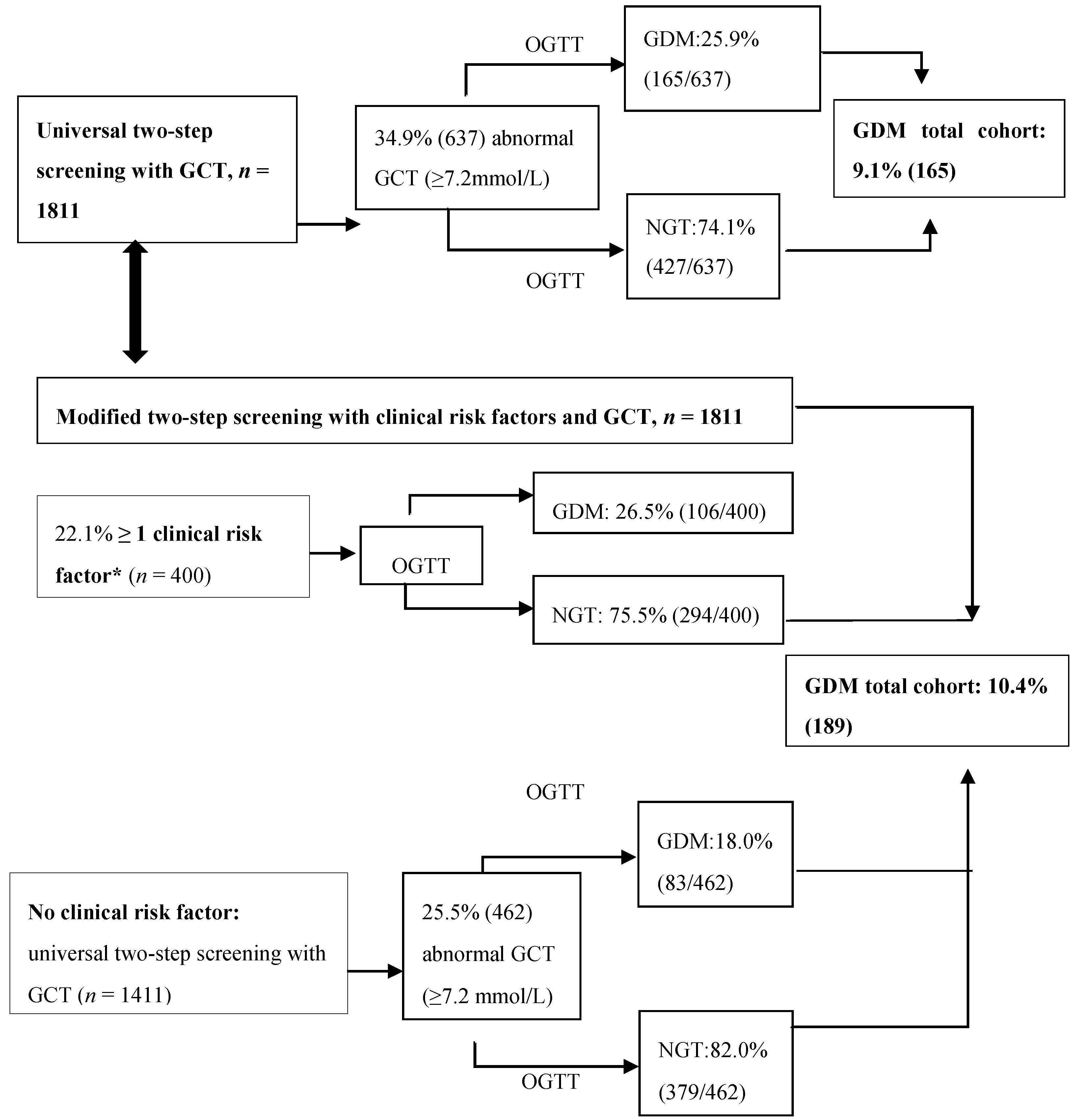
3.3. Sensitivity of Screening with the GCT Combined with Clinical Risk Factors
3.4. Differences in Biochemical Variables Across the Four Subgroups According to the GCT and OGTT Result
3.5. Tolerance and Preference of the GCT and OGTT
4. Conclusions
5. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Crowther, C.A.; Hiller, J.E.; Moss, J.R.; McPhee, A.J.; Jeffries, W.S.; Robinson, J.S.; Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial Group. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N. Engl. J. Med. 2005, 352, 2477–2486. [Google Scholar] [CrossRef] [PubMed]
- Landon, M.B.; Spong, C.Y.; Thom, E.; Carpenter, M.W.; Ramin, S.M.; Casey, B.; Wapner, R.J.; Varner, M.W.; Rouse, D.J.; Thorp, J.M., Jr.; et al. A multicenter, randomized trial of treatment for mild gestational diabetes. N. Engl. J. Med. 2009, 361, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, L.; Casas, J.P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel; Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.; Hod, M.; et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar]
- World Health Organization. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy: A world health organization guideline. Diabetes Res. Clin. Pract. 2014, 103, 341–363. [Google Scholar] [CrossRef]
- Benhalima, K.; Mathieu, C.; Damm, P.; Van Assche, A.; Devlieger, R.; Desoye, G.; Corcoy, R.; Mahmood, T.; Nizard, J.; Savona-Ventura, C.; et al. A proposal for the use of uniform diagnostic criteria for gestational diabetes in Europe: An opinion paper by the European board & college of obstetrics and gynaecology (ebcog). Diabetologia 2015, 58, 1422–1429. [Google Scholar] [PubMed]
- Ryan, E.A. Diagnosing gestational diabetes. Diabetologia 2011, 54, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Cundy, T.; Ackermann, E.; Ryan, E.A. Gestational diabetes: New criteria may triple the prevalence but effect on outcomes is unclear. BMJ 2014, 348, g1567. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of medical care in diabetes–2013. Diabetes Care 2013, 36 (Suppl. 1), S11–S66. [Google Scholar] [CrossRef] [PubMed]
- Donovan, L.E.; Savu, A.; Edwards, A.L.; Johnson, J.A.; Kaul, P. Prevalence and timing of screening and diagnostic testing for gestational diabetes mellitus: A population-based study in alberta, canada. Diabetes Care 2016, 39, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, M.M.; Punnose, J.; Dhatt, G.S. Gestational diabetes: Problems associated with the oral glucose tolerance test. Diabetes Res. Clin. Pract. 2004, 63, 73–74. [Google Scholar] [CrossRef] [PubMed]
- Donovan, L.; Hartling, L.; Muise, M.; Guthrie, A.; Vandermeer, B.; Dryden, D.M. Screening tests for gestational diabetes: A systematic review for the U.S. Preventive services task force. Ann. Intern. Med. 2013, 159, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Benhalima, K.; Van Crombrugge, P.; Moyson, C.; Verhaeghe, J.; Vandeginste, S.; Verlaenen, H.; Vercammen, C.; Maes, T.; Dufraimont, E.; De Block, C.; et al. The sensitivity and specificity of the glucose challenge test in a universal two-step screening strategy for gestational diabetes mellitus using the 2013 world health organization criteria. Diabetes Care 2018, 41, e111–e112. [Google Scholar] [CrossRef] [PubMed]
- Benhalima, K.; Van Crombrugge, P.; Verhaeghe, J.; Vandeginste, S.; Verlaenen, H.; Vercammen, C.; Dufraimont, E.; De Block, C.; Jacquemyn, Y.; Mekahli, F.; et al. The belgian diabetes in pregnancy study (bedip-n), a multi-centric prospective cohort study on screening for diabetes in pregnancy and gestational diabetes: Methodology and design. BMC Pregnancy Childbirth 2014, 14, 226. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.E. The relative contributions of insulin resistance and beta-cell dysfunction to the pathophysiology of type 2 diabetes. Diabetologia 2003, 46, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Kirwan, J.P.; Huston-Presley, L.; Kalhan, S.C.; Catalano, P.M. Clinically useful estimates of insulin sensitivity during pregnancy: Validation studies in women with normal glucose tolerance and gestational diabetes mellitus. Diabetes Care 2001, 24, 1602–1607. [Google Scholar] [CrossRef] [PubMed]
- Retnakaran, R.; Qi, Y.; Goran, M.I.; Hamilton, J.K. Evaluation of proposed oral disposition index measures in relation to the actual disposition index. Diabet. Med. 2009, 26, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Devlieger, R.; Martens, E.; Martens, G.; Van Mol, C.; Cammu, H. Perinatale Activiteiten in Vlaanderen 2014; Vzw Studiecentrum voor Perinatale Epidemiologie (SPE): Brussel, Belgium, 2014; p. 56. [Google Scholar]
- van Leeuwen, M.; Louwerse, M.D.; Opmeer, B.C.; Limpens, J.; Serlie, M.J.; Reitsma, J.B.; Mol, B.W. Glucose challenge test for detecting gestational diabetes mellitus: A systematic review. BJOG 2012, 119, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Sievenpiper, J.L.; McDonald, S.D.; Grey, V.; Don-Wauchope, A.C. Missed follow-up opportunities using a two-step screening approach for gestational diabetes. Diabetes Res. Clin. Pract. 2012, 96, e43–e46. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. Standards of medical care in diabetes. Diabetes Care 2017, 40 (Suppl. 1), S120–S127. [Google Scholar]
- Denice, S.F.; Howard, B.; Lois, D.; Ariane, G.; Tina, K.; Erin, K.; Rema, S. 2018 clinical practice guidelines. Diabetes and pregnancy. Can. J. Diabetes 2018, 42, S255–S282. [Google Scholar]
- Goldberg, R.J.; Ye, C.; Sermer, M.; Connelly, P.W.; Hanley, A.J.; Zinman, B.; Retnakaran, R. Circadian variation in the response to the glucose challenge test in pregnancy: Implications for screening for gestational diabetes mellitus. Diabetes Care 2012, 35, 1578–1584. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Garden, F.; Jalaludin, B. Hyperglycaemia following glucose challenge test during pregnancy: When can a screening test become diagnostic? Diabetes Res. Clin. Pract. 2009, 83, 394–396. [Google Scholar] [CrossRef] [PubMed]
- McElduff, A.; Hitchman, R. Screening for gestational diabetes: The time of day is important. Med. J. Aust. 2002, 176, 136. [Google Scholar] [PubMed]
- Kramer, C.K.; Swaminathan, B.; Hanley, A.J.; Connelly, P.W.; Sermer, M.; Zinman, B.; Retnakaran, R. Each degree of glucose intolerance in pregnancy predicts distinct trajectories of beta-cell function, insulin sensitivity, and glycemia in the first 3 years postpartum. Diabetes Care 2014, 37, 3262–3269. [Google Scholar] [CrossRef] [PubMed]
- Sacks, D.A.; Hadden, D.R.; Maresh, M.; Deerochanawong, C.; Dyer, A.R.; Metzger, B.E.; Lowe, L.P.; Coustan, D.R.; Hod, M.; Oats, J.J.; et al. Frequency of gestational diabetes mellitus at collaborating centers based on iadpsg consensus panel-recommended criteria: The hyperglycemia and adverse pregnancy outcome (hapo) study. Diabetes Care 2012, 35, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Farrar, D.; Duley, L.; Dowswell, T.; Lawlor, D.A. Different strategies for diagnosing gestational diabetes to improve maternal and infant health. Cochrane Database Syst. Rev. 2017, 8, CD007122. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | GDM N = 231 | NGT N = 1610 | p-Value | |
|---|---|---|---|---|
| Mean gestational week first visit | 11.9 ± 1.8 | 11.9 ± 1.7 | 11.9 ±1.8 | 0.970 |
| Mean age (years) | 30.8 ± 4.1 | 32.0 ± 4.7 | 30.6 ± 3.9 | <0.001 |
| Mean pre-pregnancy BMI (kg/m²) Pre-pregnancy overweight Pre-pregnancy obesity | 24.1 ± 4.7 22.2 (423) 11.3 (215) | 25.8 ± 5.5 24.9 (54) 21.7 (47) | 23.8 ± 4.4 21.8 (336) 9.1 (140) | <0.001 |
| Mean BMI at first visit (kg/m²) Overweight at first visit Obesity at first visit | 24.7 ± 4.7 25.2 (502) 13.3 (265) | 26.6 ± 5.3 29.1 (67) 23.5 (54) | 24.4 ± 4.5 24.9 (398) 11.0 (176) | <0.001 |
| Waist circumference at first visit (cm) Waist ≥ 80–88 cm Waist >88 cm | 87.3 ± 11.7 35.0 (671) 39.8 (762) | 91.2 ± 13.0 30.7 (67) 50.9 (111) | 86.5 ± 10.9 36.8 (567) 37.3 (574) | <0.001 |
| Ethnic minorities | 10.7 (213) | 18.9 (43) | 8.2 (132) | <0.001 |
| Highest education: Primary school Till 15 years High school Bachelor Master | 1.2 (24) 4.6 (92) 13.9 (278) 41.8 (806) 35.5 (684) | 2.6 (6) 4.8 (11) 17.0 (36) 37.5 (81) 35.6 (77) | 0.9 (15) 4.3 (69) 12.2 (189) 43.1 (675) 36.2 (568) | 0.387 |
| Smoking before pregnancy | 29.5 (587) | 35.1 (80) | 28.4 (456) | 0.043 |
| Smoking during pregnancy | 3.8 (75) | 5.7 (13) | 3.2 (52) | 0.082 |
| First degree family history of diabetes | 13.1 (255) | 18.7 (42) | 11.8 (185) | 0.005 |
| Second degree family history of diabetes | 44.1 (717) | 48.3 (84) | 42.6 (557) | 0.166 |
| History of GDM* | 9.3 (90) | 30.2 (36) | 5.3 (40) | <0.001 |
| History of impaired glucose intolerance | 1.6 (27) | 2.9 (6) | 1.1 (15) | 0.033 |
| History of macrosomia* | 11.7 (115) | 15.8 (19) | 11.5 (88) | 0.176 |
| Systolic blood pressure first visit (mmHg) | 115.1 ± 10.7 | 116.4 ± 11.5 | 114.8 ± 10.4 | 0.047 |
| Diastolic blood pressure first visit (mmHg) | 70.6 ± 8.2 | 72.1 ± 8.8 | 70.3 ± 8.1 | 0.002 |
| Systolic hypertension first visit | 2.2 (44) | 3.0 (7) | 1.9 (30) | 0.215 |
| Diastolic hypertension first visit | 1.9 (39) | 3.5 (8) | 1.6 (26) | 0.063 |
| Systolic blood pressure at time of the OGTT (mmHg) | 113.4 ± 10.2 | 115.0 ± 11.3 | 113.1 ± 10.0 | 0.050 |
| Diastolic blood pressure at time of the OGTT (mmHg) | 67.3 ± 8.0 | 69.0 ± 8.3 | 67.0 ± 7.9 | <0.001 |
| Systolic Hypertension at time of the OGTT | 1.2 (23) | 3.1 (7) | 0.9 (15) | 0.014 |
| Diastolic Hypertension at time of the OGTT | 0.7 (13) | 1.7 (4) | 0.6 (9) | 0.068 |
| Fertility treatment | 14.6 (292) | 16.4 (38) | 14.8 (238) | 0.507 |
| PCOS | 7.1 (142) | 4.8 (11) | 7.3 (117) | 0.169 |
| Multiparity | 47.7 (956) | 51.9 (120) | 46.5 (748) | 0.120 |
| Fasting glycaemia (mmol/L) at first visit | 4.5 (4.2–4.7) | 4.7 (4.4–4.9) | 4.5 (4.4–4.7) | <0.001 |
| HbA1c (mmol/mol and %) at first visit | 31 (29–32) 5.0 (4.8–5.1) | 32 (30–34) 5.1 (4.9–5.3) | 30 (29–32) 4.9 (4.8–5.1) | <0.001 |
| Total cholesterol (mmol/L) at first visit | 4.7 (4.2–5.3) | 6.3 (5.6–7.0) | 6.3 (5.7–7.0) | 0.894 |
| HDL-cholesterol (mmol/L) at first visit | 1.8 (1.5–2.0) | 1.9 (1.6–2.2) | 1.9 (1.6–2.2) | 0.090 |
| LDL-cholesterol (mmol/L) at first visit | 2.5 (2.0–2.9) | 3.4 (2.8–4.0) | 3.4 (2.9–4.1) | 0.611 |
| Triglycerides (mmol/L) at first visit | 1.1 (0.8–1.3) | 2.0 (1.6–2.5) | 1.8 (1.4–2.3) | <0.001 |
| HOMA-IR at first visit | 9.4 (6.6–13.5) | 10.7 (7.9–16.9) | 9.1 (6.5–12.9) | <0.001 |
| HOMA-B at first visit | 922.5 (669.9–1292.1) | 930.0 (673.7–1334.0) | 918.0 (667.8–1284.0) | 0.492 |
| Mean gestational week GCT | 24.5 ± 0.9 | 24.6 ± 1.1 | 24.5 ± 0.9 | 0.439 |
| Timing of the GCT | Before 12:00 a.m.: 44.4% (811) After 12:00 a.m.: 55.6% (1016) | Before 12:00 a.m.: 48.0% (109) After 12:00 a.m.: 52.0% (118) | Before 12:00 a.m.: 43.5% (684) After 12:00 a.m.: 56.5% (888) | 0.201 |
| Hours after the last meal before the GCT | 3.6 ± 3.2 | 3.5 ± 3.1 | 3.6 ± 3.2 | 0.983 |
| Glucose value 1 h after the GCT (mmol/L) | 6.7 ± 1.5 | 8.1 ± 1.6 | 6.5 ± 1.4 | <0.001 |
| Non-fasting glucose value before the GCT (mmol/L) | 4.9 ± 0.9 | 5.4 ± 1.1 | 4.9 ± 0.9 | <0.001 |
| Mean gestational week OGTT | 26.9 ± 1.1 | 27.0 ± 1.2 | 26.9 ± 1.0 | 0.037 |
| Time between GCT and OGTT (weeks) | 2.4 ± 0.9 | 2.5 ± 1.1 | 2.3 ± 1.0 | 0.272 |
| OGTT (mmol/L): Fasting 1 h 2 h | 4.3 (4.1–4.6) 7.1 (6.0–8.3) 6.2 (5.3–7.2) | 4.7 (4.4–5.1) 9.5 (8.5–10.3) 8.6 (7.5–9.1) | 4.3 (4.1–4.5) 6.8 (5.9–7.8) 6.0 (5.1–6.9) | <0.001 <0.001 <0.001 |
| HbA1c (mmol/mol and %) at time of the OGTT | 30 (29–32) 4.9 (4.8–5.1) | 32 (30–34) 5.1 (4.9–5.3) | 30 (29–32) 4.9 (4.8–5.1) | <0.001 |
| Total cholesterol (mmol/L) at time of the OGTT | 6.3 (5.6–7.0) | 6.3 (5.6-7.0) | 6.3 (5.7–7.0) | 0.894 |
| HDL-cholesterol (mmol/L) at time of the OGTT | 1.9 (1.6–2.2) | 1.9 (1.6–2.2) | 1.9 (1.6–2.2) | 0.090 |
| LDL-cholesterol (mmol/L) at time of the OGTT | 3.4 (2.9–4.1) | 3.4 (2.8–4.0) | 3.4 (2.9–4.1) | 0.611 |
| Triglycerides (mmol/L) at time of the OGTT | 1.8 (1.5–2.3) | 2.0 (1.6–2.5) | 1.8 (1.4–2.3) | <0.001 |
| HOMA-IR at time of the OGTT | 12.4 (8.9–17.7) | 17.2 (11.5–26.5) | 11.9 (8.6–16.7) | <0.001 |
| Matsuda index at time of the OGTT | 0.5 (0.4–0.8) | 0.4 (0.3-0.5) | 0.6 (0.4-0.8) | <0.001 |
| HOMA-B at time of the OGTT | 1561.8 (1122.9–2254.9) | 1339.4 (1026.9–2073.9) | 1584.0 (1132.0–2273.4) | 0.087 |
| ISSI-2 at time of the OGTT | 0.14 (0.08–0.24) | 0.09 (0.04–0.16) | 0.14 (0.08–0.25) | <0.001 |
| Insulinogenic index/HOMA-IR at time of the OGTT | 0.31 (0.22–0.45) | 0.21 (0.16–0.29) | 0.33 (0.24–0.47) | <0.001 |
| BEDIP-N Cohort N = 2006 | Pregnant Background Population from 2014 *; N = 67,729 | |
|---|---|---|
| Mean age (years) | 30.8 ± 4.1 | 28.7 |
| ≥40 years | 2.0 | 2.7 |
| Mean BMI at first visit (kg/m²) | 24.7 ± 4.7 | 24.1 ± 4.6 |
| Overweight | 25.2 | 22.2 |
| Obesity | 13.3 | 11.2 |
| Ethnic minorities ** | 10.7 | 15.2 |
| Highest education **: Primary school Until 15 years High school Bachelor Master or PhD | 1.2 4.6 13.9 41.8 35.5 | 4.1 7.3 34.9 27.3 18.9 |
| Profession: ** Employee Laborer Self-employed No paid job (Unemployed, chronic ill or house wife) | 63.6 5.1 7.1 9.4 | 58.8 14.0 5.5 18.3 |
| Multiparity | 47.7 | 55.8 |
| Fertility treatment | 14.6 | 6.9 |
| Hypertension | 4.1 | 4.6 |
| GDM with GCT ≥ 7.2 mmol/L Group 1 N = 165 | GDM with GCT < 7.2 mmol/L Group 2 N = 63 | NGT with GCT ≥ 7.2 mmol/L Group 3 N = 472 | NGT with GCT < 7.2 mmol/L Group 4 N = 1113 | p-Value 1 vs. 4 | p-Value 2 vs. 4 | p-Value 3 vs. 4 | |
|---|---|---|---|---|---|---|---|
| Age (years) | 32.5 ± 4.7 | 31.1 ± 4.1 | 31.1 ± 3.9 | 30.4 ±3.9 | <0.001 | 0.13 | 0.004 |
| ≥ 40 years | 9.7 (16) | 0% (0) | 1.3 (6) | 1.3 (15) | <0.001 | 1.00 | 1.00 |
| BMI (Kg/m²) at first visit | 26.5 ± 5.2 | 26.8 ± 5.7 | 24.5 ± 4.5 | 24.3 ± 4.4 | <0.001 | <0.001 | 0.65 |
| Overweight at first visit Obesity at first visit | 28.7 (47) 24.8 (39) | 30.2 (19) 23.8 (15) | 24.5 (115) 12.1 (57) | 24.7 (273) 10.5 (116) | <0.001 | <0.001 | 0.84 |
| Waist circumference at first visit (cm) | 90.9 ± 12.5 | 91.9 ± 14.3 | 86.4 ±11.5 | 86.6 ± 10.6 | <0.001 | 0.006 | 0.39 |
| Waist ≥80–88 cm Waist > 88 cm | 28.8 (45) 52.6 (82) | 33.9 (20) 47.5 (28) | 38.2 (174) 34.4 (157) | 36.4 (387) 38.7 (411) | 0.004 | 0.35 | 0.28 |
| BMI (Kg/m²) at time of OGTT | 29.1 ± 5.0 | 29.3 ± 5.7 | 27.0 ± 4.4 | 26.9 ± 4.4 | <0.001 | 0.001 | 0.88 |
| Overweight at time of OGTT Obesity at time of OGTT | 37.7 (60) 37.1 (59) | 44.1 (26) 33.9 (20) | 37.1 (173) 22.1 (103) | 41.3 (444) 20.6 (222) | <0.001 | 0.004 | 0.50 |
| Ethnic minorities | 18.4 (30) | 19.3 (12) | 7.7 (36) | 8.2 (91) | 0.003 | <0.001 | 0.80 |
| Highest education: primary school Until 15 years High school Bachelor Master | 2.5 (4) 3.7 (6) 25.9 (42) 37.5 (57) 34.9 (53) | 1.6 (1) 6.4 (4) 14.5 (9) 39.3 (24) 39.3 (24) | 0.4 (2) 4.3 (20) 17.2 (79) 41.4 (190) 38.6 (177) | 1.2 (13) 4.1 (46) 16.1 (175) 44.0 (478) 35.2 (382) | 0.41 | 0.78 | 0.51 |
| History of smoking before pregnancy | 33.7 (55) | 38.7 (24) | 28.1 (132) | 28.7 (318) | 0.19 | 0.09 | 0.82 |
| Smoking during pregnancy | 6.7 (11) | 1.6 (1) | 4.3 (20) | 2.8 (31) | 0.02 | 1.00 | 0.16 |
| First degree family history of diabetes | 20.8 (32) | 12.7 (7) | 12.9 (60) | 11.3 (122) | 0.005 | 0.09 | 0.37 |
| Second degree family history of diabetes | 50.4 (64) | 44.4 (20) | 45.3 (172) | 41.7 (379) | 0.06 | 0.72 | 0.24 |
| First degree family history of GDM | 7.3 (11) | 5.4 (3) | 5.0 (22) | 3.7 (38) | 0.04 | 0.50 | 0.24 |
| History of GDM | 36.0 (32) | 13.8 (4) | 7.3 (16) | 4.6 (24) | <0.001 | 0.03 | 0.13 |
| History of impaired glucose intolerance | 3.4 (5) | 1.8 (1) | 1.7 (7) | 0.9 (8) | 0.02 | 0.40 | 0.26 |
| History of macrosomia | 20.0 (18) | 3.4 (1) | 10.9 (24) | 11.9 (63) | 0.04 | 0.23 | 0.71 |
| Systolic blood pressure first visit (mmHg) | 116.5 ± 11.7 | 116.0 ± 11.3 | 115.4 ± 10.9 | 114.6 ± 10.1 | 0.06 | 0.14 | 0.11 |
| Diastolic blood pressure first visit (mmHg) | 72.5 ± 9.0 | 71.4 ± 8.4 | 71.2 ± 8.6 | 70.0 ± 7.8 | <0.001 | 0.09 | 0.007 |
| Systolic blood pressure at time of OGTT (mmHg) | 115.1 ± 11.1 | 114.6 ± 11.8 | 113.0 ± 10.2 | 113.1 ± 10.0 | 0.08 | 0.40 | 0.84 |
| Diastolic blood pressure at time of the OGTT (mmHg) | 68.7 ± 7.9 | 69.8 ± 9.1 | 67.0 ± 8.2 | 66.9± 7.8 | 0.007 | 0.004 | 0.85 |
| Fertility treatment | 20.0 (33) | 7.9 (5) | 16.7 (79) | 13.8 (154) | 0.04 | 0.18 | 0.14 |
| PCOS | 4.8 (8) | 4.8 (3) | 8.1 (38) | 6.8 (76) | 0.33 | 0.52 | 0.37 |
| Multiparity | 54.5 (90) | 46.0 (29) | 46.4 (219) | 45.9 (510) | 0.04 | 0.98 | 0.84 |
| Fasting glycaemia (mmol/L) at first visit | 4.7 (4.4–4.9) | 4.6 (4.3–4.9) | 4.5 (4.3–4.7) | 4.5 (4.3–4.7) | <0.001 | 0.004 | 0.49 |
| HbA1c (mmol/mol and %) at first visit | 32 (30–33) 5.1 (4.9–5.2) | 31 (30–34) 5.0 (4.9–5.3) | 31 (28–32) 5.0 (4.8–5.1) | 31 (28–32) 5.0 (4.8–5.1) | <0.001 | 0.01 | 0.44 |
| Total cholesterol (mmol/L) at first visit | 4.8 (4.2–5.4) | 4.8 (4.3–5.4) | 4.8 (4.2–5.4) | 4.6 (4.1–5.2) | 0.01 | 0.12 | 0.008 |
| HDL-cholesterol (mmol/L) at first visit | 1.7 (1.5–2.0) | 1.8 (1.5–2.0) | 1.8 (1.5–2.0) | 1.7 (1.5–2.0) | 0.59 | 0.68 | 0.08 |
| LDL-cholesterol (mmol/L) at first visit | 2.4 (2.1–2.9) | 2.4 (2.1–2.9) | 2.4 (2.0–2.9) | 2.4 (2.0–2.8) | 0.10 | 0.20 | 0.43 |
| Triglycerides (mmol/L) at first visit | 1.2 (0.9–1.5) | 1.0 (0.8–1.3) | 1.0 (0.8–1.3) | 1.0 (0.8–1.2) | <0.001 | 0.04 | 0.02 |
| HOMA-IR at first visit | 10.5 (7.8–17.1) | 12.0 (8.3–14.6) | 9.2 (6.2–14.1) | 9.07 (6.5–12.7) | <0.001 | <0.001 | 0.33 |
| HOMA-B at first visit | 1354.1 (641.7–1328.4) | 969.4 (776.8–1339.6) | 936.0 (662.7–1368.0) | 912.0 (668.8–1273.3) | 0.92 | 0.17 | 0.44 |
| OGTT (mmol/L) Fasting 1 h 2 h | 4.7 (4.4–5.1) 9.7 (8.7–10.5) 8.8 (7.9–9.2) | 4.7 (4.3–5.2) 8.8 (7.8–9.9) 8.5 (6.7–9.0) | 4.3 (4.1–4.5) 7.5 (6.5–8.4) 6.5 (5.5–7.4) | 4.3 (4.1–4.5) 6.5 (5.7–7.5) 5.8 (5.0–6.6) | <0.001 <0.001 <0.001 | <0.001 <0.001 <0.001 | 0.18 <0.001 <0.001 |
| HbA1c ( mmol/mol and %) at time of the OGTT | 32 (30–34) 5.1 (4.9–5.3) | 31 (28–33) 5.0 (4.8–5.2) | 30 (28–32) 4.9(4.8–5.1) | 30 (28–32) 4.9 (4.8–5.1) | <0.001 | <0.001 | 0.13 |
| Total cholesterol (mmol/L) at time of the OGTT | 6.3 (5.6–7.0) | 6.3 (5.6–7.1) | 6.1 (5.6–7.0) | 6.3 (5.7–7.1) | 0.57 | 0.99 | 0.02 |
| HDL-cholesterol (mmol/L) at time of the OGTT | 1.9 (1.6–2.2) | 1.9 (1.6–2.2) | 1.9 (1.6–2.2) | 1.9 (1.6–2.2) | 0.08 | 0.44 | 0.44 |
| LDL-cholesterol (mmol/L) at time of the OGTT | 3.4 (2.8–4.0) | 3.5 (3.0–4.3) | 3.3 (2.8–4.0) | 3.5 (2.9–4.2) | 0.14 | 0.99 | 0.004 |
| Triglycerides (mmol/L) at time of the OGTT | 2.1 (1.6–2.7) | 2.0 (1.6–2.3) | 1.8 (1.4–2.3) | 1.8 (1.4–2.2) | <0.001 | 0.04 | 0.22 |
| HOMA-IR at time of the OGTT | 17.1 (11.8–26.1) | 17.4 (11.1–28.5) | 12.0 (8.6–17.5) | 11.9 (8.6–16.4) | <0.001 | <0.001 | 0.004 |
| Matsuda index at time of the OGTT | 0.38 (0.26–0.5) | 0.39 (0.24–0.53) | 0.54 (0.39–0.75) | 0.61 (0.44–0.82) | <0.001 | <0.001 | <0.001 |
| HOMA-B at time of the OGTT | 1315.8 (1001.2–2069.5) | 1501.2 (1048.5–2268.0) | 1592.1 (1155.3–2309.7) | 1584.0 (1125.0–2259.0) | 0.29 | 0.36 | 0.13 |
| ISSI-2 at time of the OGTT | 0.10 (0.05–0.16) | 0.09 (0.04–0.17) | 0.13 (0.07–0.23) | 0.15 (0.09–0.26) | <0.001 | 0.009 | 0.04 |
| Insulinogenic index/HOMA-IR at time of the OGTT | 0.21 (0.15–0.29) | 0.21 (0.17–0.30) | 0.31 (0.22–0.46) | 0.34 (0.24–0.48) | <0.001 | <0.001 | 0.004 |
| Risk factors | Total Number of OGTT’s needed with GCT and Risk Factors combined % (n) | Number of OGTT’s needed based on GCT % (n) | Number of OGTT’s needed based on Risk Factors % (n) | % (n) GDM | Sensitivity (95% CI), % n/N | Specificity (95% CI), % n/N | LR+ (95% CI) | LR− (95% CI) | Positive Posttest Probability | Negative Posttest Probability |
|---|---|---|---|---|---|---|---|---|---|---|
| EM background | 41.3 (749) | 31.2 (566) | 10.0 (182) | 9.8 (178) | 78.1 (72.1–83.3) 178/228 | 64.0 (61.6–66.3) 1282/1583 | 2.2 (2.0–2.4) | 0.34 (0.27–0.44) | 24.3% (20.0–28.7) | 4.8% (4.0–5.9) |
| BMI ≥ 30 kg/m² | 40.9 (741) | 30.7 (557) | 10.1 (184) | 9.7 (176) | 77.2 (71.2–82.5) 176/228 | 64.3 (61.9–66.7) 1020/1583 | 2.2 (2.0–2.4) | 0.35 (0.28–0.45) | 24.3% (20.0–28.7) | 5.0% (4.1–6.0) |
| History of GDM | 36.7 (665) | 32.5 (589) | 4.2 (76) | 9.3 (169) | 74.1 (67.9–79.7) 169/228 | 68.7 (66.4–71.0) 1089/1583 | 2.4 (2.1–2.6) | 0.38 (0.30–0.47) | 26.0% (21.4–30.7) | 5.3% (4.4–6.4) |
| Any of the 3 risk factors | 47.6 (868) | 25.5 (462) | 22.1 (400) | 10.4 (189) | 82.9 (77.4–87.5) 189/228 | 57.5 (55.0–59.9) 911/1583 | 1.9 (1.8–2.1) | 0.30 (0.22–0.40) | 22.4% (18.4–26.5) | 4.2% (3.4–5.2) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benhalima, K.; Van Crombrugge, P.; Moyson, C.; Verhaeghe, J.; Vandeginste, S.; Verlaenen, H.; Vercammen, C.; Maes, T.; Dufraimont, E.; De Block, C.; et al. A Modified Two-Step Screening Strategy for Gestational Diabetes Mellitus Based on the 2013 WHO Criteria by Combining the Glucose Challenge Test and Clinical Risk Factors. J. Clin. Med. 2018, 7, 351. https://doi.org/10.3390/jcm7100351
Benhalima K, Van Crombrugge P, Moyson C, Verhaeghe J, Vandeginste S, Verlaenen H, Vercammen C, Maes T, Dufraimont E, De Block C, et al. A Modified Two-Step Screening Strategy for Gestational Diabetes Mellitus Based on the 2013 WHO Criteria by Combining the Glucose Challenge Test and Clinical Risk Factors. Journal of Clinical Medicine. 2018; 7(10):351. https://doi.org/10.3390/jcm7100351
Chicago/Turabian StyleBenhalima, Katrien, Paul Van Crombrugge, Carolien Moyson, Johan Verhaeghe, Sofie Vandeginste, Hilde Verlaenen, Chris Vercammen, Toon Maes, Els Dufraimont, Christophe De Block, and et al. 2018. "A Modified Two-Step Screening Strategy for Gestational Diabetes Mellitus Based on the 2013 WHO Criteria by Combining the Glucose Challenge Test and Clinical Risk Factors" Journal of Clinical Medicine 7, no. 10: 351. https://doi.org/10.3390/jcm7100351
APA StyleBenhalima, K., Van Crombrugge, P., Moyson, C., Verhaeghe, J., Vandeginste, S., Verlaenen, H., Vercammen, C., Maes, T., Dufraimont, E., De Block, C., Jacquemyn, Y., Mekahli, F., De Clippel, K., Van Den Bruel, A., Loccufier, A., Laenen, A., Minschart, C., Devlieger, R., & Mathieu, C. (2018). A Modified Two-Step Screening Strategy for Gestational Diabetes Mellitus Based on the 2013 WHO Criteria by Combining the Glucose Challenge Test and Clinical Risk Factors. Journal of Clinical Medicine, 7(10), 351. https://doi.org/10.3390/jcm7100351