1. Introduction
Verrucae (plantar warts) are a notorious source of frustration for both practitioners and patients alike, as no single treatment is completely effective in all patients. Despite a plethora of medical literature on this subject, high quality evidence for the efficacy of almost all treatments is non-existent [
1,
2]. A review by Lipke [
3] also stated that although evidenced based reviews with guidelines have been published, they do not cover treatments that have yet to be subjected to blinded randomized, controlled clinical trials. Moreover, Lipke asserted that lack of robust evidence of a therapy, which has not been subjected to such rigorous scientific testing, does not mean that it is not worth knowing about nor worthy of use in practice, particularly when a specific treatment has been utilised and reported, albeit anecdotally, with a reasonably high clinical success rate. This article is a patient-centred, review of clinical practice of one such verrucae treatment, which was first described by Falknor [
4] in 1969, the method of which he termed “needling”.
Verrucae are benign tumours, caused by infection of epidermal keratinocytes by the double stranded DNA Human Papilloma Virus (HPV). There are currently more than 100 known types of HPV and these determine the anatomical distribution and morphology of the lesion [
5]. The most common warts on the hands and feet are the subtypes 1, 2 and 4 [
6].
Infection of the keratinocyte at the basal layer of the epidermis is established through abrasions of the skin surface. Here, the virus remains latent in the cell from 1 to 8 months [
7]. As the epidermal cells differentiate and migrate to the surface, the virus is triggered to undergo replication and maturation until it is shed in the exfoliation of the epidermis. The process of virus replication produces proliferation of prickle cells which alters the character of the epidermis, resulting in the visible warty appearance of the verrucae.
In most viral infections, the viral proteins within a cell cause damage to the host cell and stimulate production of cytotoxic T cells, which then seek out and destroy the targeted infected cells. However, unlike many viruses, HPV prevents cell lysis as infection spreads through the shedding of infected epithelial cells from the surface of the skin. In other words, there is no (or indeed limited) release of viral proteins to the circulating dentritic cells, and therefore, no (or inadequate) antigen presentation to the immune system. Furthermore, HPV proteins also encode specific functions to inhibit immune responses by inducing specific anti-inflammatory mechanisms by activating T suppressor cells. Frazer [
8] explains that “such inhibition would be expected to reduce specific antiviral defence mechanisms and also effective presentation of antigen to the host immune system”.
The absence, or reduction, of a cellular response may explain why verrucae treatments are not uniformly successful and treatment can be difficult even in immune-competent individuals. Most treatments work by destroying affected tissues, by either a cytotoxic or physically ablative mode of action. However, tissue damage alone may not be enough to produce the relevant cytokines to destroy latent virus in adjacent cells [
9], thus recurrence and further treatment is often required after apparent resolution [
10]. Verrucae persist, evading host immune surveillance, but sometimes disappear with inflammation [
11]. Sterling
et al. [
6] stated that despite the lack of antigens, HPV does sometimes induce an immune response and spontaneous regression is often seen, although warts are less likely to resolve in adults and in immuno-suppressed patients. Therefore, research into efficacy of verrucae treatment for children must take into account the incidence of a higher rate of spontaneous regression [
12].
Frazer’s work concluded that induction of cell-mediated immunity to early proteins of HPV may prove useful as a therapeutic approach to HPV infection [
8]. This is in agreement with Tyring [
13] who also stated; “The ideal way to combat HPV infection would be to improve the immune response to the virus so it is specific and directed against early viral proteins.” One way of achieving this would be by better presentation of viral antigens to the immune system. Recent research on successful treatments has been aiming toward creating an enhanced systemic immune response to eradicate the virus [
7]. This enhancement is required as although HPV does induce a localised immune response, it is not effective enough to trigger a systemic response because any expression of viral proteins are limited to superficial epithelial cells, thus there is a reduced presentation of these to the immune system.
The work of Parton and Sommerville [
14] asserted that resolution of a single plantar verruca in children aged 4–14 years could be successfully achieved by lightly debriding the lesion to produce capillary bleeding and then abraded with fine glass paper. Chapman [
15] expanded upon this work in 1998 and hypothesised that it should be possible to demonstrate a “whole body response” in patients with several verrucae in that the treatment of just one verruca will lead to the resolution of the untreated verrucae. Twenty-one patients participated in Chapman’s clinical trial with a wider age group range (aged 6–36 years) than that of Parton and Sommerville, who claimed an optimistic 94% of cases cleared within two weeks after one treatment. Chapman reported 43% success rate in participants aged 6–13 years. His conclusion concurred with Stirling’s observation; that treatment is more likely to be successful in patients under 14 years old.
The ideal verrucae treatment should result in resolution of all or a great percentage of warts, be painless, need only one or a part of a lesion treated, create no scarring and offer HPV immunity for a lifetime.
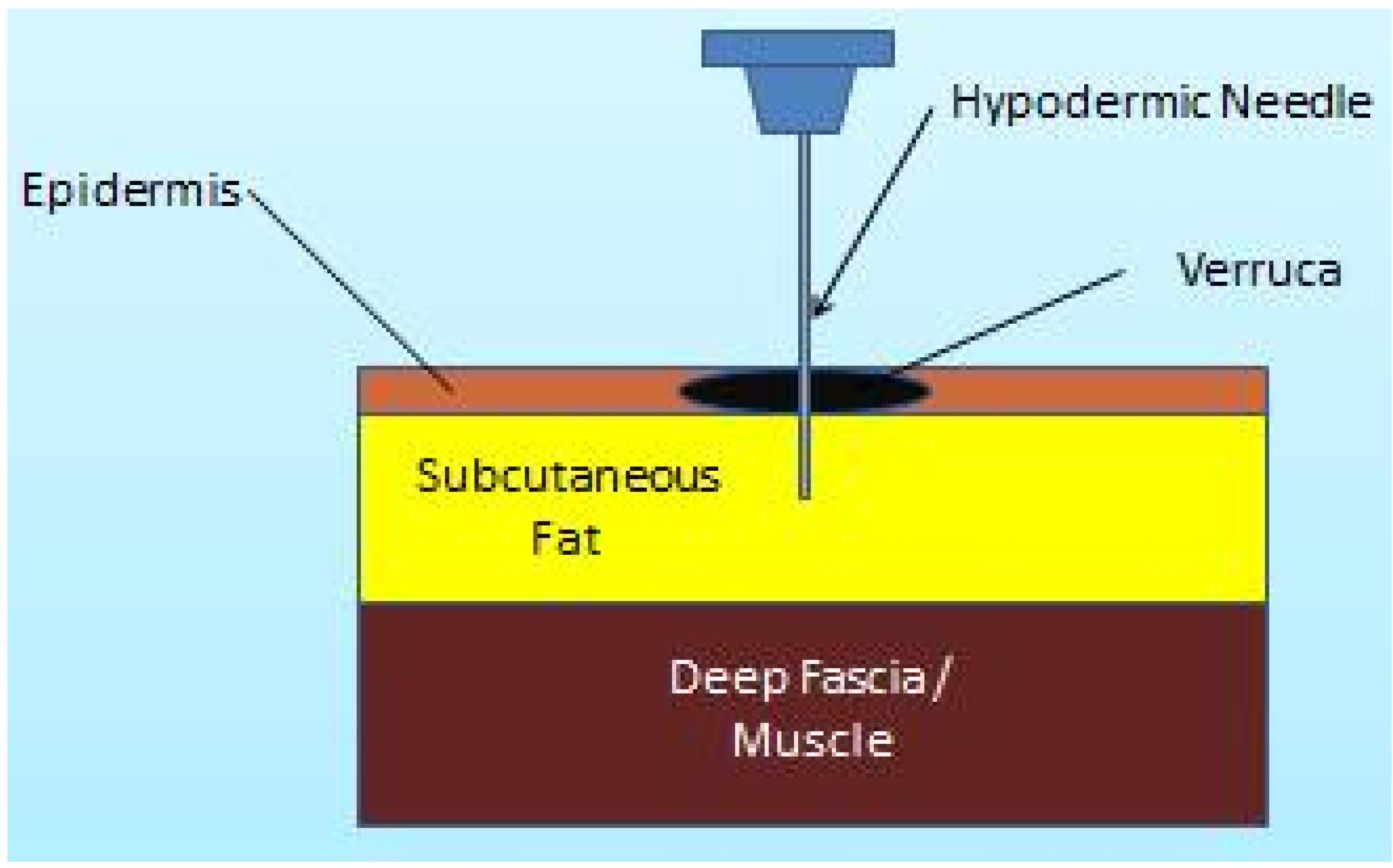
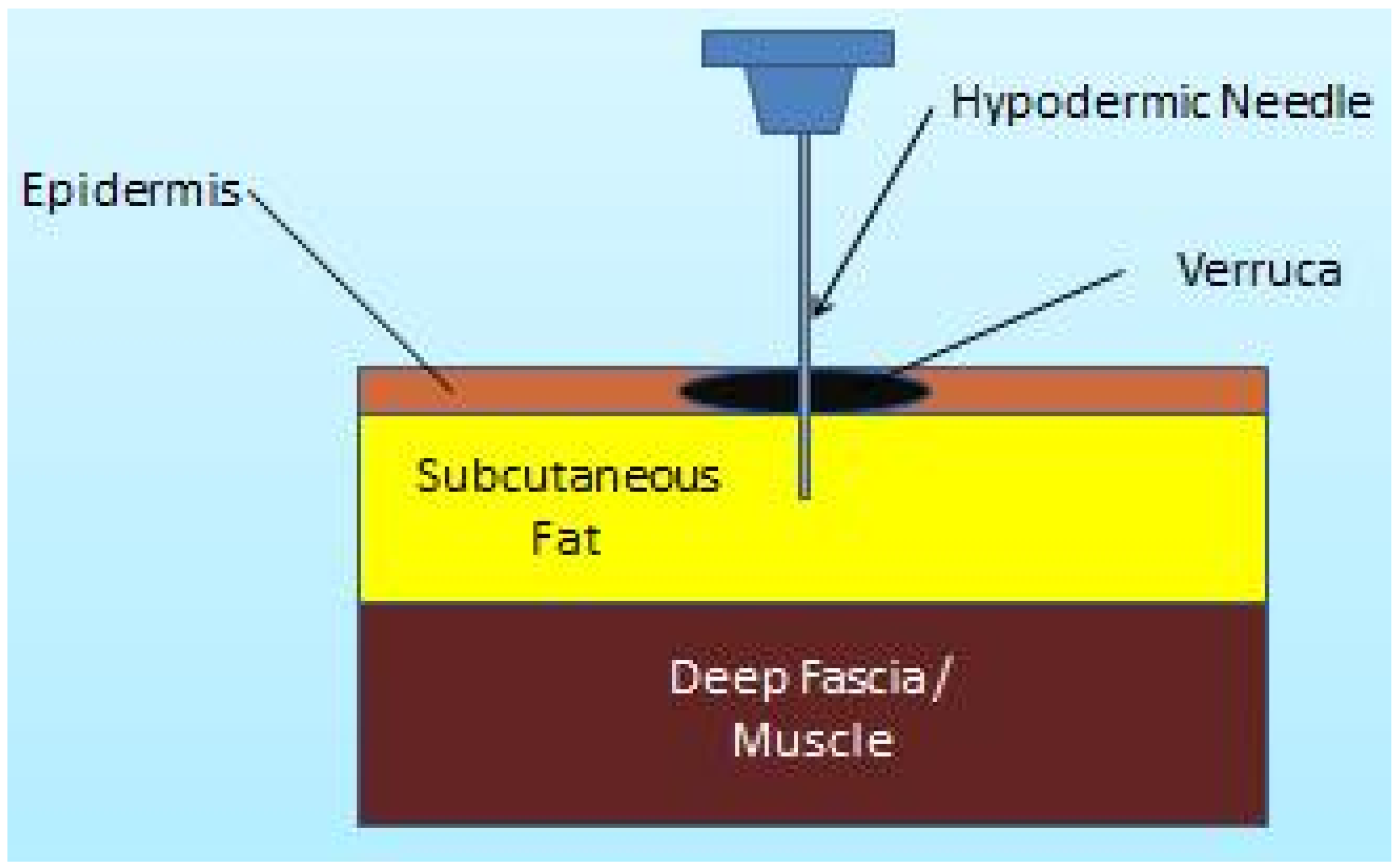
Falknor [
4] first explained a direct needling procedure as a form of physical trauma without the use of chemicals (notwithstanding the use of local anaesthesia). The method he outlined comprised of anaesthetising the verruca, then thrusting in a needle “in dart fashion, so as to penetrate the full depth of the verruca and exiting through the base of the capsule into the fat”. He claimed only two recurrences of 126 lesions treated with this technique. Subsequent published research using this method has been sparse. Skilton and Mehar [
16] published a case series of 14 patients with painful verrucae who were treated with the needling technique. They claimed resolution in 50% (7 out of the 14) had complete resolution at 8-week review. This paper retrospectively analyses 46 cases of verruca treated using Falknor’s needling method in a single private podiatry practice. The authors present a retrospective review of 46 cases (34 female, 12 male) treated within a private practice in Hampshire, UK using Falknor’s method.
3. Results and Discussion
A total of 46 patients (13 male, 33 female) underwent a standardised needling procedure. The mean age of the cohort was 41.8 years ± SD 12.65 (range 17–66 years). The average patient reported duration of the warts was 5.7 years ± SD 4.15 (range 1–20 years). The locations of all the treated lesions are given in
Table 1. A total of 45 patients were available for review at eight weeks post-operatively with one patient lost to follow up.
Table 1.
Location of primary (treated) lesions.
Table 1.
Location of primary (treated) lesions.
| Location | Numbers |
|---|
| Digits (plantar or apical aspect) | 16 |
| Plantar Metatarsal Area | 20 |
| Plantar Heel | 7 |
| Base (Proximal end) of Metatarsal Area | 3 |
Of 45 patients, 69% (21 female and 10 male) demonstrated a complete resolution of verrucae (10 patients with single lesions, 8 with mosaic and 13 with multiple types). There was no significant difference in the cure rates between males and females (
p = 0.463).
Table 2 profiles previous treatments of the resolved and unresolved lesions. Of the 45 patients, 7 (2 single lesions, 2 mosaic lesions and 3 multiple lesions) opted for a second needling treatment as the initial treatment did not fully rid all lesions.
Table 2.
Previous treatment profile of resolved (R) and unresolved (U) lesions (n = 45).
Table 2.
Previous treatment profile of resolved (R) and unresolved (U) lesions (n = 45).
| | Salicylic Acid | Cryotherapy | Salicylic Acid & Cryotherapy Combined | Natural and Homeopathic remedies | No previous treatments | Total |
|---|
| U | R | U | R | U | R | U | R | U | R | |
|---|
| Number | 7 | 12 | 1 | 1 | 3 | 7 | 0 | 2 | 3 | 9 | 45 |
| Percentage % | 16 | 27 | 2.2 | 2.2 | 6.7 | 15 | 0 | 4.4 | 6.7 | 20 | 100 |
Lesions from 14 patients (31%) failed to resolve. There was no difference in the mean duration of resolved versus unresolved lesions (mean duration unresolved 7.67 years ± SD 13.26 versus mean resolved 6.68 years ± SD 4.41 (p = 0.7571). Three of the patients with unresolved lesions (7%) reported significant reduction of verrucae size and subsequent pain, signifying a clinical improvement. All treated patients reported their pain level after needling as either “none” (n = 29 [64%]) or “mild” (n = 16 [36%]) describing mild symptoms such as “bruising” or “slight discomfort”. No post-operative infection or scarring was evident on examination or reported by patients post-operatively.
Discussion
This paper represents the largest case series published to date using Falknor’s method since his original paper was published in 1969. The selection of patients from an adult population with a broad age range (17–66 years) has reduced the possibility of spontaneous regression often observed in child population based studies of this kind. The resolution rate following a maximum of two treatments (69%) indicates a good response when compared to other modalities. Using a similar approach of exposing wart virus to the immune system, Nischal
et al. [
17] auto-implanted debrided wart tissue from sufferers’ feet and implanted into the sub-cutis of the patients forearm or thigh. Analysis of the 27 subjects demonstrated a similar 74% clearance of lesions within three months.
The observed positive clinical outcomes, in this current review, suggest that the hypothesis; provocation of a cell-mediated response as the cause of verrucae regression, is a viable premise. Needling just one lesion often produced a “cascade” effect, whereby the remaining untreated lesions also resolved in a number of patients. Thus, it can be suggested that introducing already HPV infected keratinocytes into the subcutaneous layer appears to facilitate a desired immune response in some patients.
Currently the practice of needling verrucae is not extensively practiced. This may be due to many factors, including lack of published research, preference to utilise traditional and established treatments, (such as salicylic acid and cryotherapy) or simply because many practitioners require update in anaesthesic skills for ankle block infiltration.
Although the short review period of eight weeks post-operatively, potentially does not rule out completely the possibility of reinfection or recurrence, longer term follow up is required. The authors acknowledge that this is small case series and cannot imply effectiveness and any placebo action inherent cannot be fully determined. However, a larger scale investigation, with objective measures using a control intervention, over a longer period of time would provide a more detailed picture of efficacy and long term immunity of the needling technique.



{kind=link}
{kind=link}
{kind=link}