
Exploring Coronavirus Disease 2019 Risk Factors: A Text Network Analysis Approach


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Analysis
- (1)
- Keyword Extraction and Cleaning
- Keywords were extracted from the titles, abstracts, and keywords of the selected articles using Python 3.9, Natural Language Toolkit (NLTK) 3.6.7, and Text Rank algorithm.
- Standardization was applied to account for variations in capitalization, pluralization, abbreviations, and special characters.
- Synonyms were consolidated into single representative terms, ensuring consistency across the dataset.
- (2)
- Keyword Analysis and Visualization
- Key keywords were analyzed using term frequency analysis and Term Frequency-Inverse Document Frequency (TF-IDF) with Python’s Sklearn module (Scikit-learn 0.24.2).
- Results were visualized using Gephi 0.9.2, a widely used open-source tool for network analysis.
- (3)
- Clustering and Network Classification
- Clusters were identified using modularity-based algorithms and PageRank centrality measures in Gephi.
- Nodes with low similarity were filtered to improve clustering accuracy.
- The Jaccard similarity coefficient threshold was set at 0.065 to exclude weak associations. The threshold (0.065) was determined based on both heuristic analysis and empirical validation. Following prior research [11], network visualization was used to assess optimal threshold selection. Additionally, multiple threshold values (0.05, 0.06, 0.07) were tested to balance network density and meaningful keyword relationships. The threshold of 0.065 was selected as it minimized noise while retaining key associations.
- (4)
- Temporal Trend Analysis
- Temporal trends were analyzed by computing monthly similarity indices based on frequency matrices and Jaccard coefficients.
- Cut-off points were determined by identifying peaks and troughs in similarity trends using statistical methods, including moving averages and Z-scores, to ensure objective detection.
- Four distinct time intervals were identified, highlighting emerging keywords in each period.
3. Results
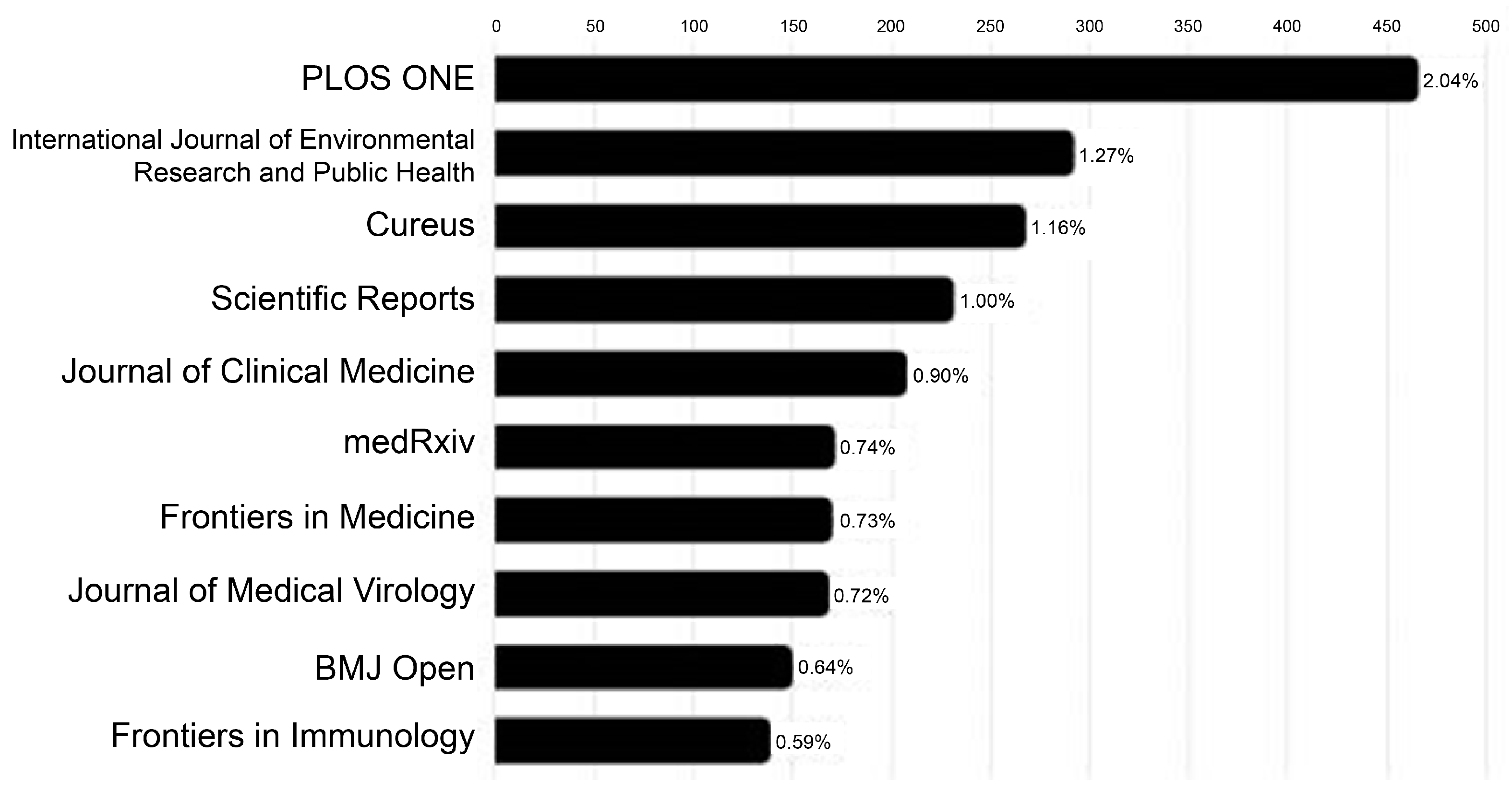
3.1. Characteristics of Severe COVID-19 Risk Factor Studies and Key Keywords
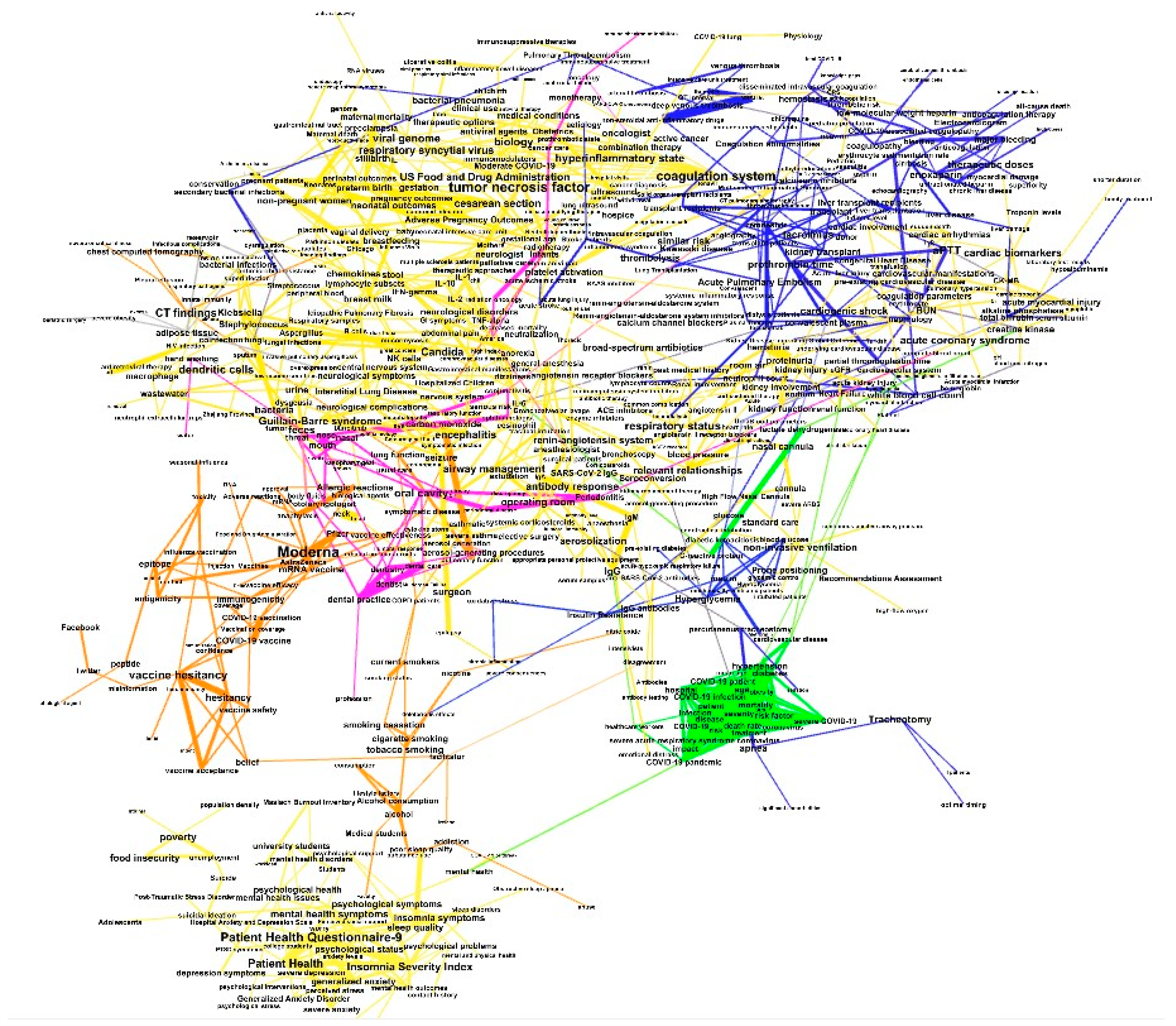
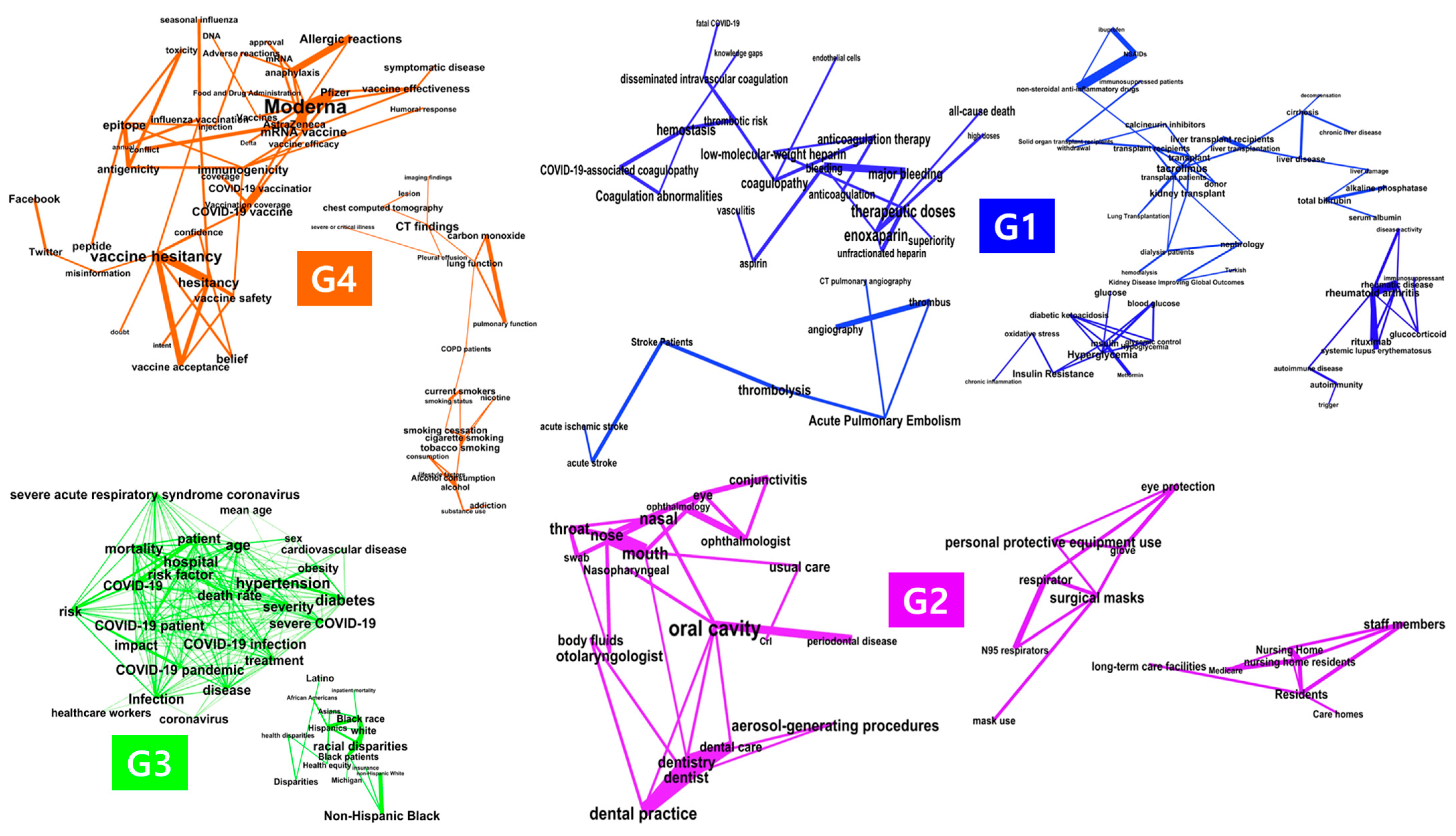
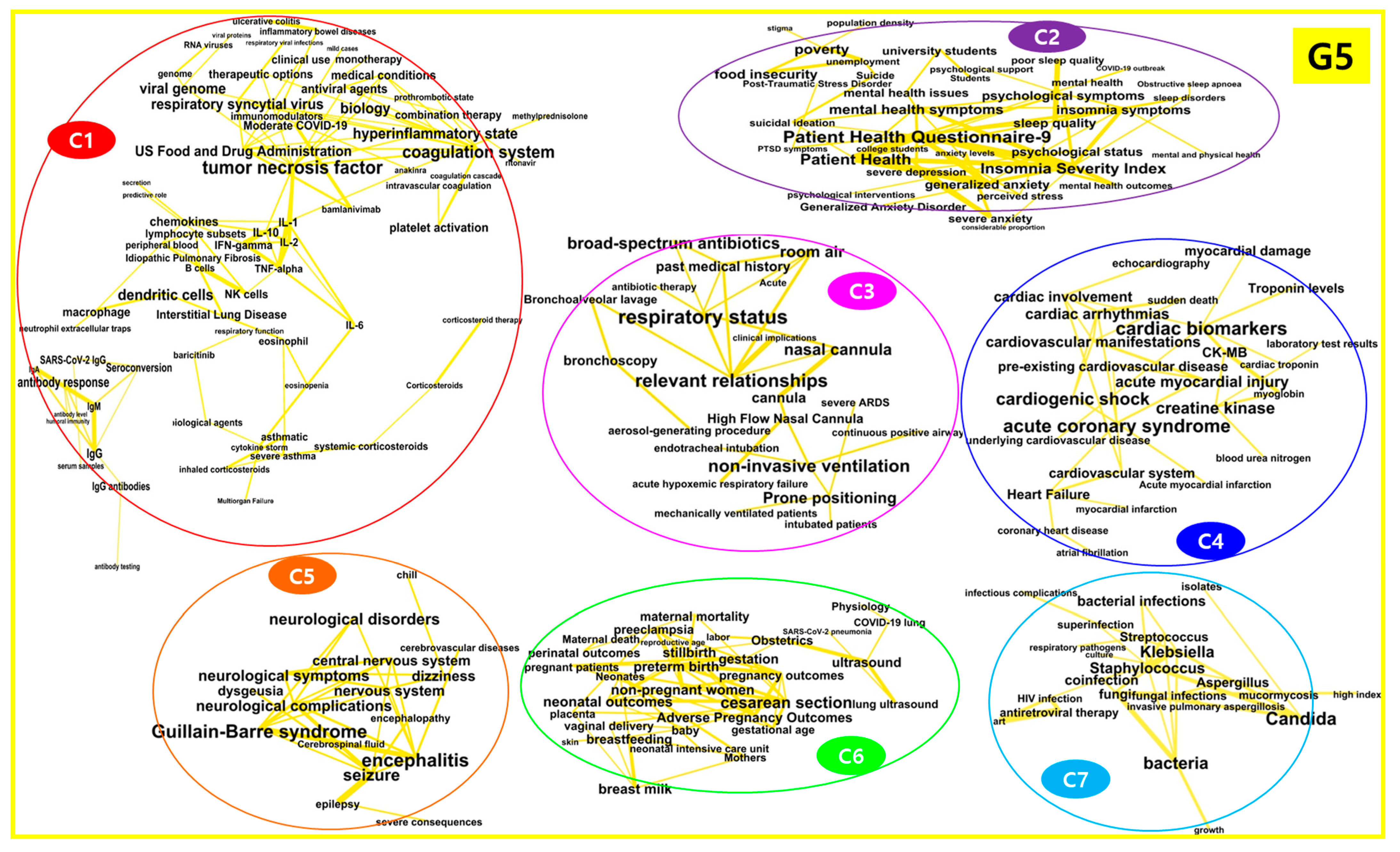
3.2. Network Analysis of Keywords
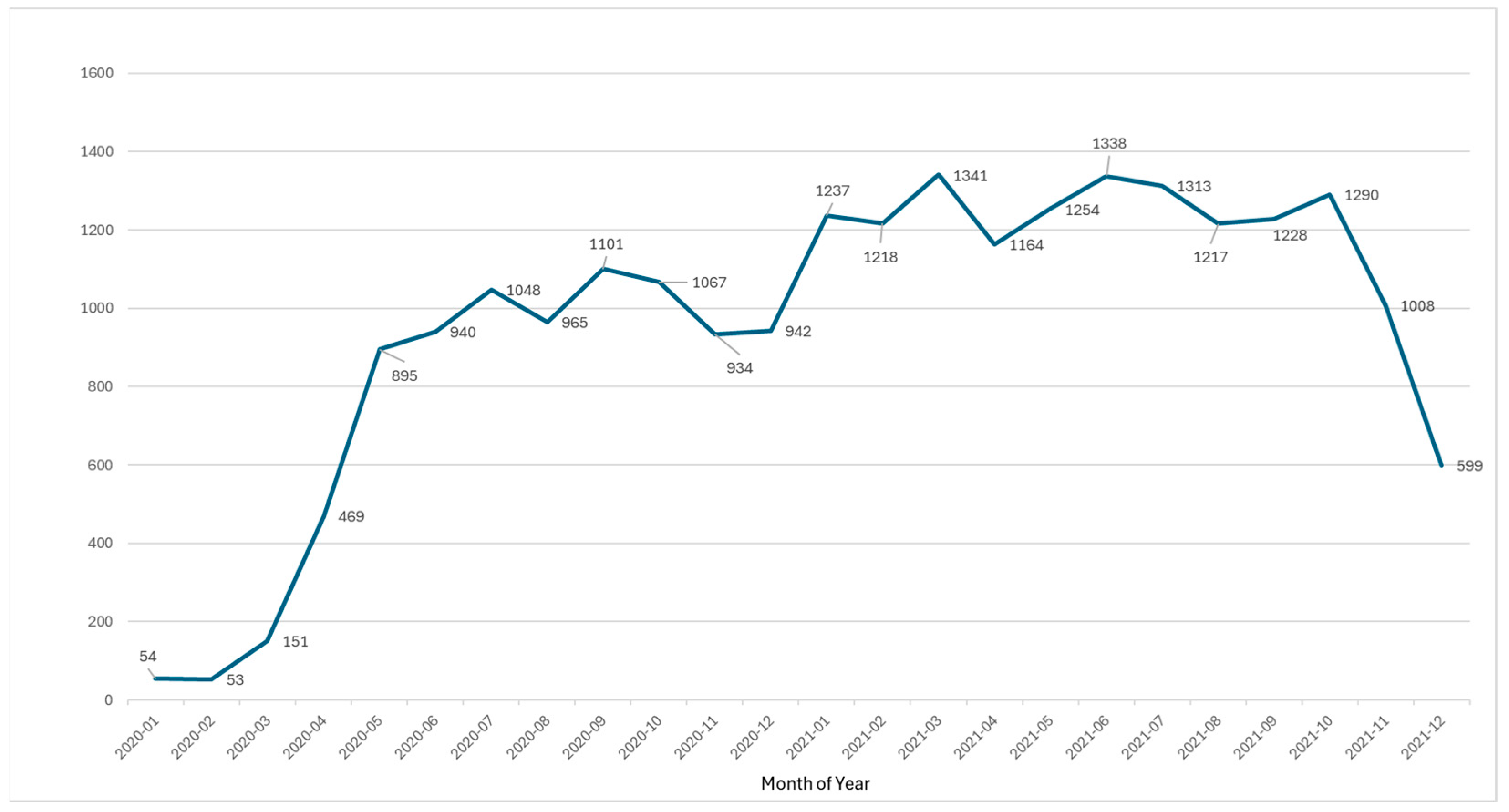
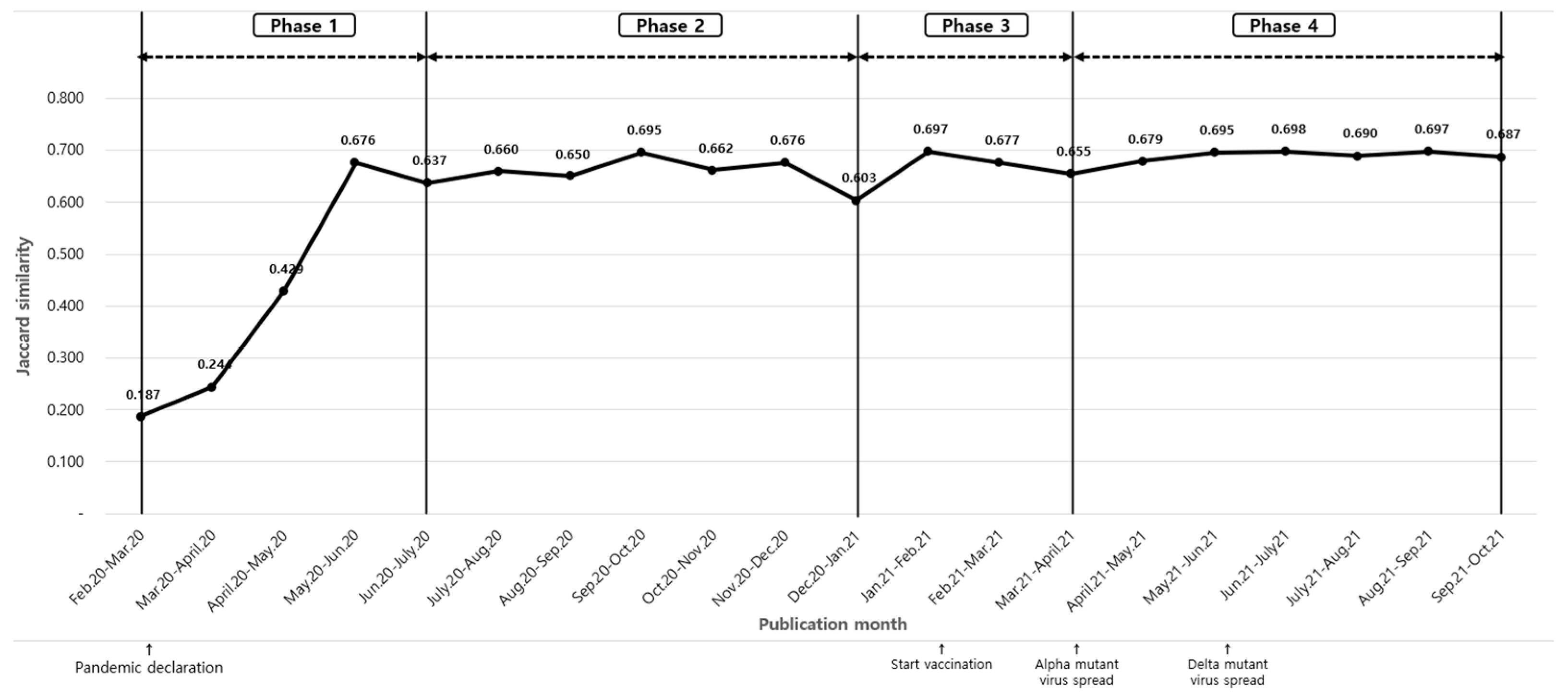
3.3. Temporal Trends of Severe COVID-19 Risk Factor Studies
4. Discussion
4.1. Principal Findings
4.2. Network and Cluster Analysis
4.3. Inter-Cluster Relationships
4.4. Temporal Trends
4.5. Strengths and Limitations
4.6. Implications and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CK-MB | Creatine Kinase-MB |
| COPD | Chronic Obstructive Pulmonary Disease |
| COVID-19 | Coronavirus Disease 2019 |
| IgG | Immunoglobulin G |
| IgM | Immunoglobulin M |
| IL-6 | Interleukin-6 |
| NIV | Non-Invasive Ventilation |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| TF-IDF | Term Frequency–Inverse Document Frequency |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Query Detailed | Number of Literature |
|---|---|---|
| PubMed | ((COVID-19 OR SARS-CoV-2 OR 2019-nCoV OR 2019-Novel Coronavirus OR COVID OR COVID-2019 OR coronavirus-disease-2019 OR severe-acute-respiratory-syndrome-coronavirus-2 [Title/Abstract]) AND (risk[Title/Abstract] OR risk factor[Title/Abstract] OR predict[Title/Abstract]) AND (severe[Title/Abstract] OR critical[Title/Abstract] OR ICU care[Title/Abstract] OR mechanical ventilation[Title/Abstract] OR intensive care unit[Title/Abstract] OR severity[Title/Abstract] OR respiratory failure[Title/Abstract] OR fatal[Title/Abstract])) | 17,674 |
| CINAHL | (COVID-19 OR SARS-CoV-2 OR 2019-nCoV OR 2019-Novel Coronavirus OR COVID OR COVID-2019 OR coronavirus disease-2019 OR severe-acute-respiratory-syndrome-coronavirus-2) AND (risk OR risk factor OR predict) AND (severe OR critical OR ICU care OR mechanical ventilation OR intensive care unit OR severity OR respiratory failure OR fatal) | 4367 |
| EMBASE | ‘coronavirus disease 2019′:ab,ti AND (‘risk factor’:ab,ti OR risk:ab,ti) AND (‘disease severity’:ab,ti OR ‘intensive care’:ab,ti OR ‘intensive care unit’:ab,ti OR ‘artificial ventilation’:ab,ti OR ‘respiratory failure’:ab,ti OR fatality:ab,ti) | 1886 |
| WoS | (COVID-19 OR SARS-CoV-2 OR 2019-nCoV OR 2019-Novel Coronavirus OR COVID OR COVID-2019 OR coronavirus disease-2019 OR severe-acute-respiratory-syndrome-coronavirus-2) AND (risk OR risk factor OR predict) AND (severe OR critical OR ICU care OR mechanical ventilation OR intensive care unit OR severity OR respiratory failure OR fatal) | 18,973 |
| Rank | Keyword | Frequency | PageRank Centrality | Rank | Keyword | Frequency | PageRank Centrality |
|---|---|---|---|---|---|---|---|
| 1 | Age | 3224 | 0.001136 | 26 | Multiorgan failure | 234 | 0.000272 |
| 2 | Treatment | 2934 | 0.000911 | 27 | Asymptomatic | 229 | 0.000576 |
| 3 | Diabetes | 1504 | 0.001191 | 28 | Vitamin D | 214 | 0.000961 |
| 4 | Hypertension | 1230 | 0.001232 | 29 | Virus transmission | 189 | 0.000343 |
| 5 | Obesity | 1045 | 0.000732 | 30 | Anticoagulation | 180 | 0.000866 |
| 6 | Healthcare workers | 960 | 0.00062 | 31 | Mild cases | 165 | 0.000211 |
| 7 | Sex | 941 | 0.000576 | 32 | America | 160 | 0.000569 |
| 8 | Mean age | 767 | 0.000665 | 33 | COVID-19 treatment | 152 | 0.000281 |
| 9 | C-reactive protein | 596 | 0.000865 | 34 | Convalescent plasma | 148 | 0.001066 |
| 10 | Mental health | 543 | 0.000887 | 35 | IgM | 142 | 0.001007 |
| 11 | Social distancing | 449 | 0.000203 | 36 | Platelet | 142 | 0.000565 |
| 12 | Cardiovascular disease | 428 | 0.000686 | 37 | Nasopharyngeal swab | 140 | 0.000631 |
| 13 | IgG | 428 | 0.00143 | 38 | Cardiovascular system | 134 | 0.000943 |
| 14 | IL-6 | 415 | 0.000961 | 39 | Immunosuppressant | 133 | 0.000421 |
| 15 | Cytokine storm | 398 | 0.000573 | 40 | Coronary heart disease | 132 | 0.000446 |
| 16 | COVID-19 vaccine | 360 | 0.001217 | 41 | Hyperglycemia | 128 | 0.001327 |
| 17 | Invasive mechanical ventilation | 355 | 0.000295 | 42 | Reverse transcription PCR | 126 | 0.000377 |
| 18 | Dyspnea | 322 | 0.000465 | 43 | Rheumatic disease | 126 | 0.000924 |
| 19 | COVID-19 transmission | 319 | 0.000403 | 44 | Non-invasive ventilation | 124 | 0.001531 |
| 20 | COVID-19 vaccination | 319 | 0.000911 | 45 | Glucocorticoid | 116 | 0.00092 |
| 21 | Lactate dehydrogenase | 285 | 0.001003 | 46 | Endotracheal intubation | 115 | 0.000567 |
| 22 | Acute kidney injury | 273 | 0.000776 | 47 | Chloroquine | 113 | 0.00066 |
| 23 | Tocilizumab | 258 | 0.000549 | 48 | Cancer care | 108 | 0.000854 |
| 24 | Remdesivir | 257 | 0.001012 | 49 | Vitamin D deficiency | 108 | 0.000574 |
| 25 | Heart failure | 235 | 0.000947 | 50 | Aerosol-generating procedures | 107 | 0.001079 |
| 51 | CT scan | 107 | 0.000351 | 76 | chest CT | 84 | 0.001138 |
| 52 | preterm birth | 107 | 0.001283 | 77 | dentist | 84 | 0.001023 |
| 53 | physical activity | 104 | 0.000525 | 78 | healthy controls | 84 | 0.000648 |
| 54 | Australian | 103 | 0.000668 | 79 | myocardial infarction | 84 | 0.000427 |
| 55 | prone positioning | 102 | 0.001243 | 80 | laboratory markers | 83 | 0.000251 |
| 56 | chronic lung disease | 100 | 0.000206 | 81 | patient health questionnaire-9 | 82 | 0.002146 |
| 57 | secondary infection | 100 | 0.000857 | 82 | post-traumatic stress disorder | 82 | 0.000686 |
| 58 | RT-PCR testing | 99 | 0.00031 | 83 | radiotherapy | 82 | 0.000903 |
| 59 | females | 98 | 0.000337 | 84 | antibody response | 81 | 0.001636 |
| 60 | healthy individuals | 97 | 0.000384 | 85 | coagulopathy | 81 | 0.001146 |
| 61 | sociodemographic factors | 97 | 0.000348 | 86 | European society | 81 | 0.001098 |
| 62 | hemoglobin | 96 | 0.000811 | 87 | renal failure | 81 | 0.000399 |
| 63 | hemodialysis | 95 | 0.000422 | 88 | viral pneumonia | 81 | 0.00028 |
| 64 | white blood cell count | 95 | 0.001327 | 89 | mechanically ventilated patients | 80 | 0.000509 |
| 65 | neutrophil count | 93 | 0.001072 | 90 | pregnant patients | 80 | 0.000871 |
| 66 | multisystem inflammatory syndrome | 92 | 0.000643 | 91 | antiviral therapy | 79 | 0.000343 |
| 67 | socioeconomic status | 92 | 0.000641 | 92 | inflammatory bowel diseases | 79 | 0.000647 |
| 68 | symptomatic COVID-19 | 92 | 0.000565 | 93 | HIV infection | 78 | 0.000598 |
| 69 | corticosteroids | 90 | 0.000509 | 94 | cesarean section | 77 | 0.001697 |
| 70 | Switzerland | 88 | 0.000393 | 95 | innate immunity | 77 | 0.000648 |
| 71 | surgeon | 86 | 0.001447 | 96 | propensity score | 77 | 0.000636 |
| 72 | beneficial effect | 85 | 0.000455 | 97 | virus infection | 77 | 0.000639 |
| 73 | elective surgery | 85 | 0.00102 | 98 | endothelial cells | 76 | 0.000272 |
| 74 | receiver operating characteristic curve | 85 | 0.000768 | 99 | most common symptom | 76 | 0.000351 |
| 75 | autoimmune disease | 84 | 0.000616 | 100 | vasopressor | 76 | 0.000295 |
| 101 | white | 76 | 0.001528 | 126 | demographic information | 65 | 0.000384 |
| 102 | renin-angiotensin system | 75 | 0.00149 | 127 | Denmark | 65 | 0.000808 |
| 103 | standard care | 74 | 0.001171 | 128 | herd immunity | 65 | 0.000386 |
| 104 | lung disease | 73 | 0.000365 | 129 | immunomodulators | 65 | 0.000949 |
| 105 | SARS-CoV-2 spike protein | 73 | 0.00097 | 130 | neutrophil-to-lymphocyte ratio | 65 | 0.000509 |
| 106 | ventilatory support | 73 | 0.00032 | 131 | alcohol consumption | 64 | 0.001007 |
| 107 | chest radiography | 72 | 0.000638 | 132 | chronic liver disease | 64 | 0.000581 |
| 108 | SARS-CoV-2 pneumonia | 72 | 0.000259 | 133 | non-pharmaceutical interventions | 64 | 0.000854 |
| 109 | airway | 69 | 0.000514 | 134 | smoking status | 64 | 0.000591 |
| 110 | D-dimer level | 69 | 0.000725 | 135 | anti-SARS-CoV-2 antibodies | 63 | 0.000759 |
| 111 | thromboembolic complications | 69 | 0.000557 | 136 | atrial fibrillation | 63 | 0.00037 |
| 112 | ACE2 receptor | 68 | 0.000268 | 137 | belief | 63 | 0.001276 |
| 113 | genome | 68 | 0.00076 | 138 | California | 63 | 0.000343 |
| 114 | long-term care facilities | 68 | 0.000932 | 139 | contact tracing | 63 | 0.000564 |
| 115 | mRNA vaccine | 68 | 0.001323 | 140 | occupation | 63 | 0.001077 |
| 116 | worry | 68 | 0.000817 | 141 | oxygen support | 63 | 0.000319 |
| 117 | hematological malignancies | 67 | 0.001023 | 142 | self-isolation | 63 | 0.000349 |
| 118 | influenza vaccination | 67 | 0.000821 | 143 | transmissibility | 63 | 0.000271 |
| 119 | patient health | 67 | 0.001849 | 144 | central nervous system | 62 | 0.001034 |
| 120 | ACE-2 | 66 | 0.001213 | 145 | methylprednisolone | 62 | 0.000563 |
| 121 | Bangladesh | 66 | 0.00029 | 146 | oxidative stress | 62 | 0.000713 |
| 122 | blood pressure | 66 | 0.001118 | 147 | perceived stress | 62 | 0.000861 |
| 123 | confidence | 66 | 0.000745 | 148 | psychological symptoms | 62 | 0.001323 |
| 124 | abdominal pain | 65 | 0.000988 | 149 | relapse | 62 | 0.000413 |
| 125 | anticoagulation therapy | 65 | 0.001079 | 150 | seroconversion | 62 | 0.00123 |
| 151 | critical disease | 61 | 0.000496 | 176 | Hispanics | 59 | 0.001094 |
| 152 | dysregulation | 61 | 0.00051 | 177 | IL-1 | 59 | 0.001205 |
| 153 | IgA | 61 | 0.000667 | 178 | investigator | 59 | 0.000704 |
| 154 | insomnia severity index | 61 | 0.001768 | 179 | machine learning model | 59 | 0.000408 |
| 155 | insulin | 61 | 0.001046 | 180 | perceived risk | 59 | 0.000321 |
| 156 | mental health outcomes | 61 | 0.000682 | 181 | sequential organ failure assessment | 59 | 0.001008 |
| 157 | metabolism | 61 | 0.000494 | 182 | supplementation | 59 | 0.001031 |
| 158 | mobility | 61 | 0.001083 | 183 | acute coronary syndrome | 58 | 0.001673 |
| 159 | tobacco smoking | 61 | 0.001362 | 184 | chest pain | 58 | 0.000251 |
| 160 | anorexia | 60 | 0.001089 | 185 | conflict | 58 | 0.000566 |
| 161 | fibrosis | 60 | 0.00037 | 186 | immune function | 58 | 0.000664 |
| 162 | home quarantine | 60 | 0.00043 | 187 | preventive strategies | 58 | 0.000322 |
| 163 | hypoxemic respiratory failure | 60 | 0.000434 | 188 | prothrombin time | 58 | 0.001617 |
| 164 | lymphocytopenia | 60 | 0.000542 | 189 | rituximab | 58 | 0.001095 |
| 165 | males | 60 | 0.00028 | 190 | TNF-alpha | 58 | 0.00094 |
| 166 | neutralizing antibodies | 60 | 0.000465 | 191 | travel | 58 | 0.000554 |
| 167 | nosocomial transmission | 60 | 0.000269 | 192 | water | 58 | 0.000605 |
| 168 | rheumatoid arthritis | 60 | 0.001324 | 193 | alcohol | 57 | 0.001026 |
| 169 | vaccines | 60 | 0.000779 | 194 | bacteria | 57 | 0.001565 |
| 170 | zinc | 60 | 0.001032 | 195 | black race | 57 | 0.001431 |
| 171 | aerosolization | 59 | 0.001502 | 196 | immune dysregulation | 57 | 0.000511 |
| 172 | bed | 59 | 0.0005 | 197 | kidney transplant | 57 | 0.001297 |
| 173 | Delta | 59 | 0.00024 | 198 | lesion | 57 | 0.00084 |
| 174 | feeling | 59 | 0.000414 | 199 | positive test results | 57 | 0.000272 |
| 175 | healthcare resources | 59 | 0.000209 | 200 | social determinants | 57 | 0.000525 |
| Phase | Month | Similarity |
|---|---|---|
| 1 | 2020.02.∼2020.03. | 0.187 |
| 2020.03.∼2020.04. | 0.244 | |
| 2020.04.∼2020.05. | 0.429 | |
| 2020.05.∼2020.06. | 0.676 | |
| 2020.06.∼2020.07. | 0.637 | |
| 2 | 2020.07.∼2020.08. | 0.660 |
| 2020.08.∼2020.09. | 0.650 | |
| 2020.09.∼2020.10. | 0.695 | |
| 2020.10.∼2020.11. | 0.662 | |
| 2020.11.∼2020.12. | 0.676 | |
| 2020.12.∼2021.01. | 0.603 | |
| 3 | 2021.01.∼2021.02. | 0.697 |
| 2021.02.∼2021.03. | 0.677 | |
| 2021.03.∼2021.04. | 0.655 | |
| 4 | 2021.04.∼2021.05. | 0.679 |
| 2021.05.∼2021.06. | 0.695 | |
| 2021.06.∼2021.07. | 0.698 | |
| 2021.07.∼2021.08. | 0.690 | |
| 2021.08.∼2021.09. | 0.697 | |
| 2021.09.∼2021.10. | 0.687 |
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 12 February 2022).
- Centers for Disease Control and Prevention. COVID-19 Overview and Infection Prevention and Control Priorities in Non-U.S. Healthcare Settings. Available online: https://archive.cdc.gov/www_cdc_gov/coronavirus/2019-ncov/hcp/non-us-settings/overview/index.html (accessed on 12 February 2022).
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef]
- Eysenbach, G. How to fight an infodemic: The four pillars of infodemic management. J. Med. Internet Res. 2020, 22, e21820. [Google Scholar] [CrossRef]
- Lodhwal, V.; Choudhary, G. Survey Paper: Automatic Title Generation for Text with RNN and Pre-trained Transformer Language Model. Int. J. Res. Appl. Sci. Eng. Technol. 2023, 11, 2117–2124. [Google Scholar] [CrossRef]
- Dritsas, E.; Trigka, M. Exploring the intersection of machine learning and big data: A survey. Mach. Learn. Knowl. Extr. 2025, 7, 13. [Google Scholar] [CrossRef]
- Park, S.; Park, J. Identifying the knowledge structure and trends of outreach in public health care: A text network analysis and topic modeling. Int. J. Environ. Res. Public Health 2021, 18, 9309. [Google Scholar] [CrossRef]
- Kim, H.J.; Bae, S.H.; Park, J.H. Research trends on cancer-related cognitive impairment in patients with non-central nervous system cancer: Text network analysis and topic modeling. J. Korean Acad. Fundam. Nurs. 2023, 30, 313–324. [Google Scholar] [CrossRef]
- Lee, S.S. Analytical Study on the Relationship between Centralities of Research Networks and Research Performances. J. Korean Libr. Inf. Sci. Soc. 2013, 44, 405–428. [Google Scholar] [CrossRef]
- Zhang, H.; Wu, Y.; He, Y.; Liu, X.; Liu, M.; Tang, Y.; Xu, S.; Wang, M.; Wang, W.; Liang, G.; et al. Age-related risk factors and complications of patients with COVID-19: A population-based retrospective study. Front. Med. 2022, 8, 757459. [Google Scholar] [CrossRef]
- Du, Y.; Zhou, N.; Zha, W.; Lv, Y. Hypertension is a clinically important risk factor for critical illness and mortality in COVID-19: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 745–755. [Google Scholar] [CrossRef]
- Fan, X.; Han, J.; Zhao, E.; Fang, J.; Wang, D.; Cheng, Y.; Shi, Y.; Wang, Z.; Yao, Z.; Lu, P.; et al. The effects of obesity and metabolic abnormalities on severe COVID-19-related outcomes after vaccination: A population-based study. Cell Metab. 2023, 35, 585–600.e5. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhou, K.; Misra-Hebert, A.; Bena, J. Impact of metabolic syndrome on severity of COVID-19 illness. Metab. Syndr. Relat. Disord. 2022, 20, 191–249. [Google Scholar] [CrossRef]
- Ramirez, G.A.; Bozzolo, E.P.; Gobbi, A.; Castelli, E.; Centurioni, C.; Di Meo, M.; Della Torre, E.; Di Scala, F.; Morgillo, A.; Marinosci, A.; et al. Outcomes of noninvasive ventilation as the ceiling of treatment in patients with COVID-19. Panminerva Med. 2022, 64, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Castro, R.A.; Frishman, W.H. Thrombotic complications of COVID-19 infection: A review. Cardiol. Rev. 2021, 29, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Impact of personal protective equipment use on health care workers’ physical health during the COVID-19 pandemic: A systematic review and meta-analysis. Am. J. Infect. Control 2021, 49, 1305–1315. [Google Scholar] [CrossRef]
- Mackey, K.; Ayers, C.K.; Kondo, K.K.; Saha, S.; Advani, S.M.; Young, S.; Spencer, H.; Rusek, M.; Anderson, J.; Veazie, S.; et al. Racial and ethnic disparities in COVID-19-related infections, hospitalizations, and deaths: A systematic review. Ann. Intern. Med. 2021, 174, 362–373. [Google Scholar] [CrossRef]
- Schoch-Spana, M.; Brunson, E.K.; Long, R.; Ruth, A.; Ravi, S.J.; Trotochaud, M.; Borio, L.; Brewer, J.; Buccina, J.; Connell, N.; et al. The public’s role in COVID-19 vaccination: Human-centered recommendations to enhance pandemic vaccine awareness, access, and acceptance in the United States. Vaccine 2021, 39, 6004–6012. [Google Scholar] [CrossRef]
- Mohammed, I.; Nauman, A.; Paul, P.; Ganesan, S.; Chen, K.-H.; Jalil, S.M.S.; Jaouni, S.H.; Kawas, H.; Khan, W.A.; Vattoth, A.L.; et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: A systematic review. Hum. Vaccin. Immunother. 2022, 18, 2027160. [Google Scholar] [CrossRef]
- Chodkiewicz, J.; Talarowska, M.; Miniszewska, J.; Nawrocka, N.; Bilinski, P. Alcohol consumption reported during the COVID-19 pandemic: The initial stage. Int. J. Environ. Res. Public Health 2020, 17, 4677. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Han, H.; Liu, F.; Lv, Z.; Wu, K.; Liu, Y.; Feng, Y.; Zhu, C. Positive rate of RT-PCR detection of SARS-CoV-2 infection in 4880 cases from one hospital in Wuhan, China, from Jan to Feb 2020. Clin. Chim. Acta 2020, 505, 172–175. [Google Scholar] [CrossRef]
- Zhong, R.; Chen, L.; Zhang, Q.; Li, B.; Qiu, Y.; Wang, W.; Tan, D.; Zou, Y. Which factors—Smoking, drinking alcohol, betel quid chewing, or underlying diseases—Are more likely to influence the severity of COVID-19? Front. Physiol. 2021, 11, 623498. [Google Scholar] [CrossRef]
- Zhang, L.; Zhao, W.; Sun, B.; Huang, Y.; Glänzel, W. How scientific research reacts to international public health emergencies: A global analysis of response patterns. Scientometrics 2020, 124, 747–773. [Google Scholar] [CrossRef]
- Thomeer, M.B.; Moody, M.D.; Yahirun, J. Racial and ethnic disparities in mental health and mental health care during the COVID-19 pandemic. J. Racial Ethn. Health Disparities 2023, 10, 961–976. [Google Scholar] [CrossRef]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long covid—Mechanisms, risk factors, and management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]

| Rank | Keyword | Frequency | PageRank Centrality | Rank | Frequency | Frequency | Page Rank Centrality |
|---|---|---|---|---|---|---|---|
| 1 | Age | 3224 | 0.001136 | 26 | Multiorgan failure | 234 | 0.000272 |
| 2 | Treatment | 2934 | 0.000911 | 27 | Asymptomatic | 229 | 0.000576 |
| 3 | Diabetes | 1504 | 0.001191 | 28 | Vitamin D | 214 | 0.000961 |
| 4 | Hypertension | 1230 | 0.001232 | 29 | Virus transmission | 189 | 0.000343 |
| 5 | Obesity | 1045 | 0.000732 | 30 | Anticoagulation | 180 | 0.000866 |
| 6 | Healthcare workers | 960 | 0.00062 | 31 | Mild cases | 165 | 0.000211 |
| 7 | Sex | 941 | 0.000576 | 32 | America | 160 | 0.000569 |
| 8 | Mean age | 767 | 0.000665 | 33 | COVID-19 treatment | 152 | 0.000281 |
| 9 | C-reactive protein | 596 | 0.000865 | 34 | Convalescent plasma | 148 | 0.001066 |
| 10 | Mental health | 543 | 0.000887 | 35 | IgM | 142 | 0.001007 |
| 11 | Social distancing | 449 | 0.000203 | 36 | Platelet | 142 | 0.000565 |
| 12 | Cardiovascular disease | 428 | 0.000686 | 37 | Nasopharyngeal swab | 140 | 0.000631 |
| 13 | IgG | 428 | 0.00143 | 38 | Cardiovascular system | 134 | 0.000943 |
| 14 | IL-6 | 415 | 0.000961 | 39 | Immunosuppressant | 133 | 0.000421 |
| 15 | Cytokine storm | 398 | 0.000573 | 40 | Coronary heart disease | 132 | 0.000446 |
| 16 | COVID-19 vaccine | 360 | 0.001217 | 41 | Hyperglycemia | 128 | 0.001327 |
| 17 | Invasive mechanical ventilation | 355 | 0.000295 | 42 | Reverse transcription PCR | 126 | 0.000377 |
| 18 | Dyspnea | 322 | 0.000465 | 43 | Rheumatic disease | 126 | 0.000924 |
| 19 | COVID-19 transmission | 319 | 0.000403 | 44 | Non-invasive ventilation | 124 | 0.001531 |
| 20 | COVID-19 vaccination | 319 | 0.000911 | 45 | Glucocorticoid | 116 | 0.00092 |
| 21 | Lactate dehydrogenase | 285 | 0.001003 | 46 | Endotracheal intubation | 115 | 0.000567 |
| 22 | Acute kidney injury | 273 | 0.000776 | 47 | Chloroquine | 113 | 0.00066 |
| 23 | Tocilizumab | 258 | 0.000549 | 48 | Cancer care | 108 | 0.000854 |
| 24 | Remdesivir | 257 | 0.001012 | 49 | Vitamin D deficiency | 108 | 0.000574 |
| 25 | Heart failure | 235 | 0.000947 | 50 | Aerosol-generating procedures | 107 | 0.001079 |
| Group | Factors | Subtopic | Keywords |
|---|---|---|---|
| G1 | Biomedicine factors | - | thrombolysis, acute pulmonary embolism, hyperglycemia, rheumatoid arthritis, kidney transplant, hemostasis, insulin resistance, transplant, major bleeding, liver transplant recipients, coagulopathy, low-molecular-weight heparin, coagulation abnormalities, glucose, transplant recipients, COVID-19-associated coagulopathy, rheumatic disease |
| G2 | Occupational and environmental factors | - | oral cavity, surgical masks, personal protective equipment use, staff members, dental practice, mouth, nasal, residents, aerosol-generating procedures, dentist, otolaryngologist, long-term care facilities, nursing home, nursing home residents |
| G3 | Demographic factors | - | non-hispanic black, racial disparities, white, black race, Latino, hypertension, diabetes, age, hospital, mortality, COVID-19 infection, COVID-19 patient, COVID-19 pandemic, health equity, obesity, mean age, sex |
| G4 | Health behavior factors | - | Moderna, vaccine hesitancy, vaccine acceptance, tobacco smoking, mRNA vaccine, COVID-19 vaccine, allergic reactions, smoking cessation, epitope, cigarette smoking, nicotine, COPD patients, immunogenicity, current smokers, lung function, vaccine safety, alcohol, alcohol consumption |
| G5 | Complication factors | C1 (Immunologic) | tumor necrosis factor, coagulation system, hyperinflammatory state, IgG, macrophage, IL-1, IL-10, NK cells, IL-2, IL-6, B cells, cytokine storm |
| C2 (Psychiatric) | Patient Health Questionnaire-9, Insomnia Severity Index, poverty, mental health symptoms, insomnia symptoms, sleep quality, psychological symptoms, generalized anxiety, psychological status, mental health issues | ||
| C3 (Respiratory) | respiratory status, non-invasive ventilation, nasal cannula, room air, prone positioning, bronchoscopy, high-flow nasal cannula | ||
| C4 (Cardiac) | cardiac biomarkers, acute coronary syndrome, acute myocardial injury, cardiac arrhythmias, heart failure, pre-existing cardiovascular disease, CK-MB | ||
| C5 (Neurologic) | encephalitis, Guillain-Barre syndrome, seizure, neurological disorders, neurological symptoms | ||
| C6 (Gynecologic) | cesarean section, neonatal outcomes, breast milk, preterm birth, adverse pregnancy outcomes, breastfeeding, maternal mortality | ||
| C7 (Secondary Infection) | Candida, bacteria, Klebsiella, Staphylococcus, bacterial infections, coinfection |
| Keywords | Phase 1 | Phase 2 | Phase 3 | Phase 4 |
|---|---|---|---|---|
| Obesity | 91 | 320 | 170 | 464 |
| Social distancing | 67 | 144 | 62 | 176 |
| Dyspnea | 42 | 100 | 56 | 124 |
| COVID-19 transmission | 39 | 83 | 60 | 137 |
| Chloroquine | 32 | 41 | 15 | 25 |
| Emergency department | 30 | 101 | 63 | 159 |
| America | 27 | 55 | 28 | 50 |
| Radiotherapy | 26 | 24 | 11 | 21 |
| Virus transmission | 22 | 60 | 35 | 72 |
| Coronary heart disease | 22 | 34 | 25 | 51 |
| Cancer care | 21 | 39 | 16 | 32 |
| Dentist | 21 | 28 | 9 | 26 |
| Perceived stress | - | 13 | 15 | 34 |
| Psychological symptoms | - | 13 | 12 | 37 |
| Hispanics | - | 17 | 16 | 26 |
| Generalized anxiety | - | 15 | 10 | 24 |
| Psychological well-being | - | 10 | 8 | 30 |
| Health disparities | - | 15 | 11 | 13 |
| Urea | - | 15 | 9 | 14 |
| Common complication | - | 14 | 9 | 15 |
| Deep venous thrombosis | - | 13 | 10 | 11 |
| Black race | 1 | 21 | 9 | 26 |
| Critical disease | 1 | 20 | 14 | 26 |
| Second wave | 1 | 19 | 29 | 90 |
| Persistent symptoms | - | 2 | 10 | 22 |
| Long COVID | - | - | 6 | 21 |
| Nationality | - | - | 6 | 14 |
| Mucormycosis | - | 1 | 6 | 32 |
| Moderna | - | 1 | 5 | 44 |
| First lockdown | - | 1 | 5 | 21 |
| Risk and protective factors | - | 2 | 7 | 19 |
| Anaphylaxis | - | 2 | 6 | 27 |
| Blood parameters | 1 | 1 | 9 | 12 |
| Sociodemographic data | - | 2 | 8 | 10 |
| mRNA vaccine | - | 1 | 4 | 63 |
| Delta | - | 1 | 3 | 55 |
| Bamlanivimab | - | - | - | 35 |
| Vaccine effectiveness | - | 2 | 2 | 27 |
| New variants | - | - | 3 | 26 |
| Vaccination coverage | - | - | 3 | 23 |
| Vaccine acceptance | - | 1 | 3 | 19 |
| Vaccination campaign | - | 1 | 3 | 18 |
| Kidney replacement therapy | 1 | 3 | - | 17 |
| Fungal infections | 1 | 2 | 2 | 16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.-A.; Lee, S.-K. Exploring Coronavirus Disease 2019 Risk Factors: A Text Network Analysis Approach. J. Clin. Med. 2025, 14, 2084. https://doi.org/10.3390/jcm14062084
Kang M-A, Lee S-K. Exploring Coronavirus Disease 2019 Risk Factors: A Text Network Analysis Approach. Journal of Clinical Medicine. 2025; 14(6):2084. https://doi.org/10.3390/jcm14062084
Chicago/Turabian StyleKang, Min-Ah, and Soo-Kyoung Lee. 2025. "Exploring Coronavirus Disease 2019 Risk Factors: A Text Network Analysis Approach" Journal of Clinical Medicine 14, no. 6: 2084. https://doi.org/10.3390/jcm14062084
APA StyleKang, M.-A., & Lee, S.-K. (2025). Exploring Coronavirus Disease 2019 Risk Factors: A Text Network Analysis Approach. Journal of Clinical Medicine, 14(6), 2084. https://doi.org/10.3390/jcm14062084