
Effect of Complex Venous Outflow Drainage Reconstruction on Postoperative Graft Function in Right-Lobe Living Donor Liver Transplantation

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Type, Duration, and Location of Study
2.2. Preoperative Evaluation
2.3. Surgical Procedures
2.4. Intraoperative Hemodynamic Monitoring
2.5. Definition of Groups and Parameters
2.6. Study Protocol and Ethics Committee Approval
2.7. Statistical Analysis
3. Results
3.1. General Assessment of Recipients’ Features
3.2. Comparison of CORM and Non-CORM Groups
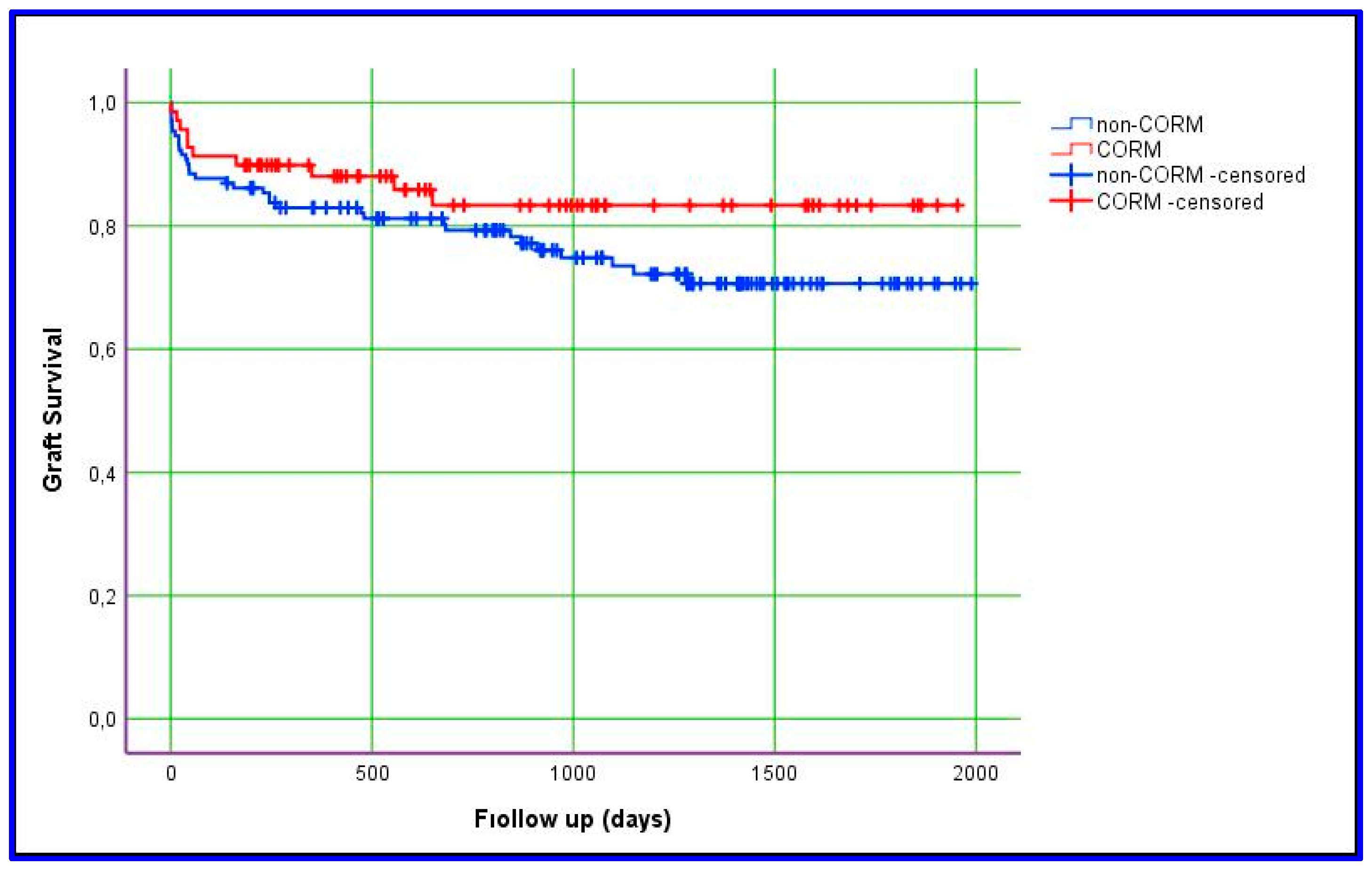
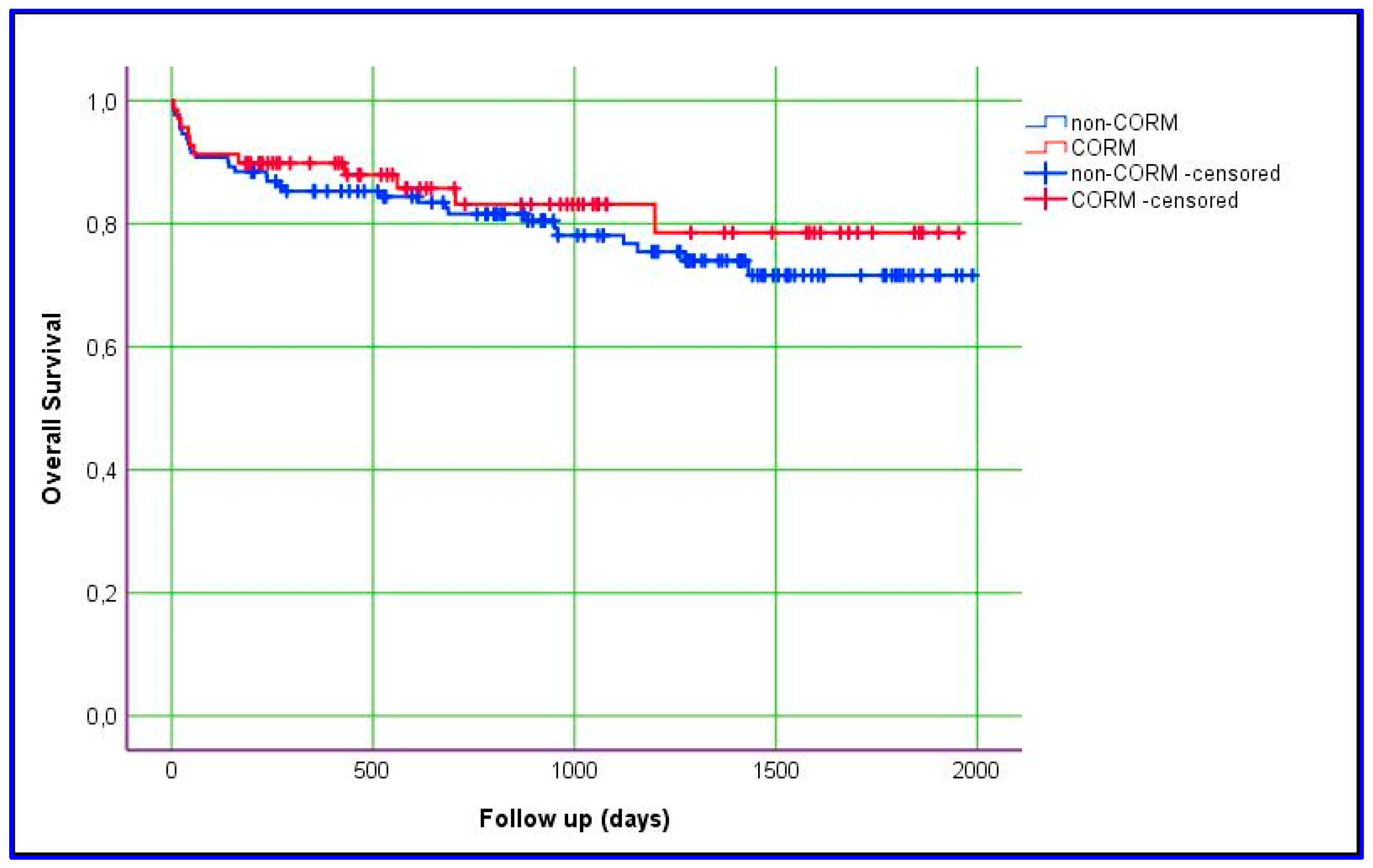
3.3. Comparison of CORM and Non-CORM Groups Based on Survival
3.4. Comparison of CORM and Non-CORM Groups Based on Postoperative Early Complications
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Starzl, T.; Groth, C.; Brettschneider, L.; Penn, I.; Fulginiti, V.; Moon, J.; Blanchard, H.; Martin, A., Jr.; Porter, K. Orthotopic homotransplantation of the human liver. Ann. Surg. 1968, 168, 392–415. [Google Scholar] [CrossRef]
- Akbulut, S.; Yilmaz, S. Liver transplantation in Turkey: Historical review and future perspectives. Transplant. Rev. 2015, 29, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Ikegami, T.; Onda, S.; Furukawa, K.; Haruki, K.; Shirai, Y.; Gocho, T. Small-for-size graft, small-for-size syndrome and inflow modulation in living donor liver transplantation. J. Hepatobiliary Pancreat. Sci. 2020, 27, 799–809. [Google Scholar] [CrossRef]
- de Villa, V.; Chen, C.; Chen, Y.; Wang, C.; Lin, C.; Cheng, Y.; Huang, T.; Jawan, B.; Eng, H. Right lobe living donor liver transplantation-addressing the middle hepatic vein controversy. Ann. Surg. 2003, 238, 275–282. [Google Scholar] [CrossRef]
- Lo, C.M. The middle hepatic vein controversy: Art and science. Liver Transpl. 2018, 24, 870–871. [Google Scholar] [CrossRef]
- Thorat, A.; Jeng, L.; Yang, H.; Li, P.; Li, M.; Yeh, C.; Chen, T.; Hsu, S.; Poon, K. Outflow reconstruction for right liver allograft with multiple hepatic veins: “V-plasty” of hepatic veins to form a common outflow channel versus 2 or more hepatic vein-to-inferior vena cava anastomoses in limited retrohepatic space. Liver Transpl. 2016, 22, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.A.; Soin, A.S. Complex Reconstruction of Right-Lobe Grafts on the Bench: Portal Vein, Anterior Sector Hepatic Veins, Inferior Hepatic Veins and Multiple Bile Ducts. J. Clin. Exp. Hepatol. 2025, 15, 102411. [Google Scholar] [CrossRef] [PubMed]
- Koc, S.; Akbulut, S.; Soyer, V.; Yilmaz, M.; Barut, B.; Kutlu, R.; Yilmaz, S. Hepatic Venous Outflow Obstruction After Living-Donor Liver Transplant: Single Center Experience. Exp. Clin. Transplant. 2021, 19, 832–841. [Google Scholar] [CrossRef]
- Chen, P.; Wang, W.; Yan, L.; Wen, T.; Li, B.; Zhao, J. Reconstructing middle hepatic vein tributaries in right-lobe living donor liver transplantation. Dig. Surg. 2014, 31, 210–218. [Google Scholar] [CrossRef]
- Lee, S.G. A complete treatment of adult living donor liver transplantation: A review of surgical technique and current challenges to expand indication of patients. Am. J. Transplant. 2015, 15, 17–38. [Google Scholar] [CrossRef]
- Sugawara, Y.; Makuuchi, M.; Sano, K.; Imamura, H.; Kaneko, J.; Ohkubo, T.; Matsui, Y.; Kokudo, N. Vein reconstruction in modified right liver graft for living donor liver transplantation. Ann. Surg. 2003, 237, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Jeng, L.; Thorat, A.; Yang, H.; Li, P. Venous outflow reconstruction in living donor liver transplantation: Dealing with venous anomalies. World J. Transplant. 2015, 5, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Namgoong, J.; Hwang, S.; Kim, K.; Park, G.; Kim, K.; Oh, S.; Cho, H.; Kwon, H.; Kwon, Y. Unification venoplasty of the outflow hepatic vein for laparoscopically harvested left liver grafts in pediatric living donor liver transplantation. Korean J. Transplant. 2020, 34, 293–301. [Google Scholar] [CrossRef]
- Aktas, S.; Alkara, U.; Sevmis, M.; Kilercik, H.; Yıldız, H.; Sevmis, S. Analysis of Hepatic Arterial Reconstruction Technique Using Surgical Loupes for Living-Donor Liver Transplantation: Results From a Single Center. Transplant. Proc. 2021, 53, 2929–2933. [Google Scholar] [CrossRef]
- Kilercik, H.; Akbulut, S.; Aktas, S.; Alkara, U.; Sevmis, S. Effect of Hemodynamic Monitoring Systems on Short-Term Outcomes after Living Donor Liver Transplantation. Medicina 2024, 60, 1142. [Google Scholar] [CrossRef]
- Vandenbroucke, J.; von Elm, E.; Altman, D.; Gøtzsche, P.; Mulrow, C.; Pocock, S.; Poole, C.; Schlesselman, J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- Jadlowiec, C.C.; Taner, T. Liver transplantation: Current status and challenges. World J. Gastroenterol. 2016, 22, 4438–4445. [Google Scholar] [CrossRef]
- Yagi, S.; Singhal, A.; Jung, D.H.; Hashimoto, K. Living-donor liver transplantation: Right versus left. Int. J. Surg. 2020, 82s, 128–133. [Google Scholar] [CrossRef]
- Lee, S.H.; Na, G.H.; Choi, H.J.; Kim, D.G.; You, Y.K. Impact of the Reconstruction Material on the Patency of Middle Hepatic Vein in Living Donor Liver Transplantation Using the Right Liver. Transplant. Proc. 2019, 51, 2745–2749. [Google Scholar] [CrossRef]
- Balci, D.; Kirimker, E.O. Hepatic vein in living donor liver transplantation. Hepatobiliary Pancreat. Dis. Int. 2020, 19, 318–323. [Google Scholar] [CrossRef]
- Dulundu, E. Outflow Reconstruction Techniques in Living Donor Liver Transplantation. Surg. Gastroenterol. Oncol. 2021, 26, 74–80. [Google Scholar] [CrossRef]
- Taha, A.M.I.; Abdalla, A.M.; Hassan, R.A.; Elkhateb, A.I.; Ali, A.M. Outflow Reconstruction in Right Lobe Living Donor Liver Transplant: Middle Hepatic Vein Reconstruction Versus Separate Tributaries to Inferior Vena Cava Anastomosis. Exp. Clin. Transplant. 2023, 21, 245–250. [Google Scholar] [CrossRef]
- Neumann, J.O.; Thorn, M.; Fischer, L.; Schöbinger, M.; Heimann, T.; Radeleff, B.; Schmidt, J.; Meinzer, H.P.; Büchler, M.W.; Schemmer, P. Branching patterns and drainage territories of the middle hepatic vein in computer-simulated right living-donor hepatectomies. Am. J. Transplant. 2006, 6, 1407–1415. [Google Scholar] [CrossRef]
- Ogiso, S.; Okuno, M.; Shindoh, J.; Sakamoto, Y.; Mizuno, T.; Araki, K.; Goumard, C.; Nomi, T.; Ishii, T.; Uemoto, S.; et al. Conceptual framework of middle hepatic vein anatomy as a roadmap for safe right hepatectomy. HPB 2019, 21, 43–50. [Google Scholar] [CrossRef]
- Guo, H.; Wang, K.; Chen, K.; Liu, Z.; Al-Ameri, A.; Shen, Y.; Xu, X.; Zheng, S. Middle hepatic vein reconstruction in adult right lobe living donor liver transplantation improves recipient survival. Hepatobiliary Pancreat. Dis. Int. 2019, 18, 125–131. [Google Scholar] [CrossRef]
- Woo, H.Y.; Hong, S.K.; Cho, J.H.; Lee, J.M.; Choi, Y.; Yi, N.J.; Lee, K.W.; Suh, K.S. Complications of polytetrafluoroethylene graft use in middle hepatic vein reconstruction in living donor liver transplantation: A retrospective, single-centre, long-term, real-world experience. Transpl. Int. 2021, 34, 455–464. [Google Scholar] [CrossRef]
- Arikan, T.; Mammadov, E.; Emek, E.; Bozkurt, B.; Inan Gurcan, N.; Yazici, P.; Sahin, T.; Serin, A.; Aydin, U.; Tokat, Y. Utility of Polyethylene Terephthalate (Dacron) Vascular Grafts for Venous Outflow Reconstruction in Living-Donor Liver Transplantations. Transplant. Proc. 2019, 51, 2442–2445. [Google Scholar] [CrossRef]
- Jothimani, D.; Devarajan, V.; Kumar, S.; Sampath, S.; Rela, M. Polytetrafluoroethylene Infection-related Sepsis in Liver Transplant Recipients. J. Clin. Infect. Dis. Soc. 2023, 1, 290–293. [Google Scholar] [CrossRef]
- Ha, T.Y.; Hwang, S.; Jung, D.H.; Ahn, C.S.; Kim, K.H.; Moon, D.B.; Song, G.W.; Park, G.C.; Park, H.W.; Park, Y.H.; et al. Complications analysis of polytetrafluoroethylene grafts used for middle hepatic vein reconstruction in living-donor liver transplantation. Transplant. Proc. 2014, 46, 845–849. [Google Scholar] [CrossRef]
- Koc, C.; Akbulut, S.; Ozdemir, F.; Kose, A.; Isik, B.; Yologlu, S.; Yilmaz, S. Analysis of Risk Factors Affecting the Development of Infection in Artificial Vascular Grafts Used for Reconstruction of Middle Hepatic Vein Tributaries in Living Donor Liver Transplantation. Transplantation 2019, 103, 1871–1876. [Google Scholar] [CrossRef]
- Li, Z.; Rammohan, A.; Gunasekaran, V.; Hong, S.; Chen, I.C.; Kim, J.; Hervera Marquez, K.A.; Hsu, S.C.; Kirimker, E.O.; Akamatsu, N.; et al. Novel Benchmark for Adult-to-Adult Living-donor Liver Transplantation: Integrating Eastern and Western Experiences. Ann. Surg. 2023, 278, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Goja, S.; Yadav, S.K.; Roy, R.; Soin, A.S. A retrospective comparative study of venous vs nonringed expanded polytetrafluoroethylene extension grafts for anterior sector outflow reconstruction in right lobe living donor liver transplantation. Clin. Transplant. 2018, 32, e13344. [Google Scholar] [CrossRef] [PubMed]
- Marubashi, S.; Dono, K.; Nagano, H.; Asaoka, T.; Hama, N.; Kobayashi, S.; Miyamoto, A.; Takeda, Y.; Umeshita, K.; Monden, M. Postoperative hyperbilirubinemia and graft outcome in living donor liver transplantation. Liver Transpl. 2007, 13, 1538–1544. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Features | Result |
|---|---|
| Age (years) | 53 (52–56) |
| Gender (male/female (%)) | 132/67 (66.3/33.7) |
| Child score (A/B/C (%)) | 23/135/41 (11.6/67.8/20.6) |
| HCC (n (%)) | 43 (21.6) |
| BMI (kg/m2) | 26.8 (26–28) |
| MELD score | 14 (14–16) |
| Ejection fraction (%) | 65 (65–70) |
| PAP (mmHg) | 30 (30–35) |
| HB | 10.6 (10–11.3) |
| PLT | 81 (73–91) |
| Creatinine | 0.78 (0.74–0.83) |
| Na | 137 (137–138) |
| Albumin | 3.2 (3.1–3.3) |
| AST | 52 (49–59) |
| ALT | 35 (32–40) |
| Total bilirubin | 1.8 (1.6–2.1) |
| Direct bilirubin | 0.9 (0.9–1.2) |
| PT | 16.1 (15.7–16.7) |
| INR | 1.4 (1.3–1.4) |
| Fibrinogen | 124 (124–132) |
| AT-III | 54 (50–57) |
| Protein S | 66 (65–70) |
| Protein C | 45 (42–49) |
| Intraop PRBCs | 2 (2–3) |
| Intraop FFPs | 2 (2–3) |
| Intraop crystalloids (mL) | 5500 (5350–6000) |
| Intraop urine output (mL) | 2200 (2000–2400) |
| Anhepatic phase (min) | 56 (53–60) |
| CIT (min) | 41 (40–44) |
| WIT (min) | 40 (39–42) |
| Graft volume (gr) | 876 (846–905) |
| GRWR | 1.2 (1.2–1.4) |
| Operation time (hour) | 6 (6–7) |
| PVT (n (%)) | 33 (16.6) |
| HRS (n (%)) | 37 (18.6) |
| Ascites (n (%)) | 175 (87.9) |
| Total bilirubin (POD30) | 0.7 (0.6–0.8) |
| Hospital stay (days) | 14 (13–15) |
| ICU stay (days) | 1 (1–2) |
| Re-exploration (n (%)) | 32 (16.1) |
| 30-day mortality (n (%)) | 10 (5.0) |
| 365-day mortality (n (%)) | 25 (12.6) |
| Follow-up (days) | 920 (860–1024) |
| Reconstruction Features | Anastomosis Design | Number of Patients |
|---|---|---|
| RHV+ V5 and V8, RHV+ V5 (n = 2) and RHV + V8 (n = 2) | RHV to RHV, V5 and V8 via Y-shape PTFE graft to IVC | 30 |
| RHV to RHV, V5 and V8 via separate PTFE grafts to IVC | 5 | |
| RHV+ (V5 or V8) + RIHV | RHV to RHV, IRHV to IVC, V5 via PTFE graft to IVC | 17 |
| RHV+ RIHVs (n = 2) | RHV to RHV, each IRHV separate distal anastomosis to IVC | 2 |
| RHV+ V5 + RIHVs (n = 2) | RHV to RHV, each IRHV separately to IVC, V5 via PTFE graft to IVC | 5 |
| RHV+ V5+ V8 + RIHV | RHV to RHV, IRHV to IVC, V5 and V8 via separate PTFE grafts to IVC | 4 |
| RHV to RHV, IRHV to IVC, V5 and V8 via Y-shape PTFE graft to IVC | 4 | |
| RHV+ V5+ V8 + RIHVs (n = 2) | RHV to RHV, each IRHV separately to IVC, V5 and V8 via Y-shape PTFE graft to IVC | 1 |
| RHV+ V5 (n = 2) + V8 + RIHV | RHV to RHV, IRHV to IVC, 2 V5 via Y-shape PTFE graft to IVC and V8 via PTFE to IVC | 1 |
| Features | CORM (n = 69) | Non-CORM (n = 130) | p |
|---|---|---|---|
| Gender (%) | 0.144 | ||
| Male | 41 (59.4) | 92 (70.8) | |
| Female | 28 (40.6) | 38 (29.2) | |
| ABO matching (%) | 0.277 | ||
| Identical | 48 (69.6) | 101 (77.7) | |
| Compatible | 21 (30.4) | 29 (22.3) | |
| Age | 30 (28–34) | 33 (32–35) | 0.279 |
| BMI | 23.7 (22.6–25) | 25 (24.6–25.8) | 0.011 |
| HB | 14.5 (13.9–15.0) | 15.1 (14.9–15.4) | 0.013 |
| PLT | 252 (238–266) | 252 (244–275) | 0.992 |
| Creatinine | 0.8 (0.8–0.9) | 0.8 (0.8–0.9) | 0.123 |
| Na | 140 (140–141) | 140 (140–141) | 0.982 |
| Albumin | 4.8 (4.8–5.0) | 4.7 (4.7–4.8) | 0.168 |
| AST | 18 (17–20) | 19 (19–20) | 0.071 |
| ALT | 16 (15–20) | 18 (17–21) | 0.092 |
| Total bilirubin | 0.4 (0.4–0.5) | 0.5 (0.5–0.6) | 0.893 |
| Direct bilirubin | 0.2 (0.2–0.3) | 0.2 (0.2–0.3) | 0.585 |
| Cholesterol (total) | 158 (153–167) | 164 (157–170) | 0.348 |
| Triglycerides | 81 (76–90) | 96 (85–106) | 0.179 |
| PT | 12 (11.8–12.2) | 11.7 (11.6–12) | 0.083 |
| INR | 1.0 (1.0–1.1) | 1.0 (1.0–1.1) | 0.052 |
| Protein C | 100 (97–108) | 102 (98–108) | 0.511 |
| Protein S | 88 (84–91) | 89 (86–92) | 0.412 |
| Features | CORM (n = 69) | Non-CORM (n = 130) | p |
|---|---|---|---|
| Age | 51 (49–56) | 54 (53–57) | 0.510 |
| Gender | 0.235 | ||
| Male | 42 (60.9) | 90 (69.2) | |
| Female | 27 (39.1) | 40 (30.8) | |
| Child score | 0.670 | ||
| A | 9 (13) | 14 (11) | |
| B | 44 (64) | 91 (70) | |
| C | 16 (23) | 25 (19) | |
| Underlying diseases | 0.336 | ||
| HBV | 13 (18.8) | 39 (30) | |
| HCV | 1 (1.4) | 6 (4.6) | |
| Alcohol | 7 (10.1) | 11 (8.5) | |
| MASLD | 19 (27.5) | 21 (16.2) | |
| Cryptogenic | 12 (17.4) | 20 (15.4) | |
| Autoimmune | 5 (7.2) | 12 (9.2) | |
| Others | 12 (17.4) | 21 (16.2) | |
| HCC | 9 (13) | 34 (26) | 0.050 |
| BMI | 28 (26- 29) | 26 (25–27) | 0.089 |
| MELD score | 16 (14–18) | 14 (14–17) | 0.336 |
| Ejection fraction (%) | 65 (65–70) | 65 (65–70) | 0.636 |
| PAP (mmHg) | 30 (30–35) | 30 (30–35) | 0.266 |
| HB | 11 (10–12) | 10.6 (10–11.5) | 0.688 |
| PLT | 83 (72–101) | 79 (68–91) | 0.688 |
| Creatinine | 0.71 (0.63–0.81) | 0.78 (0.75–0.85) | 0.127 |
| Na | 137 (137–139) | 137 (137–138) | 0.402 |
| Albumin | 3.2 (2.9–3.4) | 3.2 (3.1–3.4) | 0.905 |
| AST | 52 (42–63) | 51 (46–59) | 0.780 |
| ALT | 33 (29–46) | 36 (31–40) | 0.863 |
| Total bilirubin | 1.9 (1.4–2.5) | 1.7 (1.5–2.2) | 0.736 |
| Direct bilirubin | 0.9 (0.7–1.3) | 0.9 (0.8–1.3) | 0.453 |
| PT | 16.2 (15.5–17.7) | 16.1 (15.5–16.7) | 0.350 |
| INR | 1.4 (1.3–1.5) | 1.4 (1.3–1.4) | 0.292 |
| Fibrinogen | 124 (124–134) | 124 (124–132) | 0.168 |
| AT-III | 48 (44–57) | 54.5 (50–59) | 0.176 |
| Protein S | 66 (63–72) | 66.5 (65–72) | 0.970 |
| Protein C | 44 (39–52) | 45 (41–49) | 0.941 |
| PVT | 10 (11.4) | 23 (21.6) | 0.706 |
| HRS | 11 (15.9) | 25 (19.2) | 0.704 |
| Ascites | 61 (88) | 114 (88) | 1.000 |
| Features | CORM (n = 69) | Non-CORM (n = 130) | p |
|---|---|---|---|
| Intraop PRBCs | 2 (2–3) | 2 (2–3) | 0.330 |
| Intraop FFPs | 1 (1–2) | 2 (2–3) | 0.011 |
| Intraop crystalloids (mL) | 5500 (5500–6000) | 5650 (5000–6000) | 0.659 |
| Intraop urine output (mL) | 2250 (1800–2500) | 2000 (2000–2300) | 0.559 |
| Anhepatic phase (min) | 63 (59–70) | 51 (47–57) | <0.001 |
| CIT (min) | 46 (42–50) | 38 (35–42) | <0.001 |
| WIT (min) | 48 (43–50) | 33 (30–37) | <0.001 |
| Graft volume (gr) | 833 (800–887) | 898 (855–935) | 0.022 |
| GRWR | 1.1 (1.1–1.2) | 1.2 (1.2–1.4) | 0.004 |
| Operation time (hours) | 6 (6–7) | 6 (6–7) | 0.343 |
| Features | CORM (n = 69) | Non-CORM (n = 130) | p |
|---|---|---|---|
| Total bilirubin (POD30) | 0.66 (0.45–1) | 0.74 (0.42–1.3) | 0.483 |
| Hospital stay | 15 (15–18) | 14 (13–17) | 0.426 |
| Re-exploration | 13 (19) | 19 (15) | 0.569 |
| ICU stay (day) | 1 (1–2) | 1 (1–2) | 0.304 |
| 30-day mortality | 3 (4) | 7 (5) | 1.000 |
| 365-day mortality | 7 (10.1) | 18 (14.0) | 0.586 |
| Follow-up (days) | 644 (520–982) | 959 (871–1256) | 0.074 |
| Graft loss | 0.716 | ||
| Primary non-function | 2 | 4 | |
| Hepatic artery thrombosis | 0 | 2 |
| Features | CORM (n = 69) | Non-CORM (n = 130) | p |
|---|---|---|---|
| Overall survival | 0.461 | ||
| 1 year | 89.9% | 85.3% | |
| 3 years | 831% | 80.5% | |
| 5 years | 78.5% | 71.6% | |
| Graft survival | 0.167 | ||
| 1 year | 88.1% | 82.9% | |
| 3 years | 83.3% | 80.2% | |
| 5 years | 83.3% | 70.6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kilercik, H.; Akbulut, S.; Elsarawy, A.; Aktas, S.; Alkara, U.; Sevmis, S. Effect of Complex Venous Outflow Drainage Reconstruction on Postoperative Graft Function in Right-Lobe Living Donor Liver Transplantation. J. Clin. Med. 2025, 14, 2005. https://doi.org/10.3390/jcm14062005
Kilercik H, Akbulut S, Elsarawy A, Aktas S, Alkara U, Sevmis S. Effect of Complex Venous Outflow Drainage Reconstruction on Postoperative Graft Function in Right-Lobe Living Donor Liver Transplantation. Journal of Clinical Medicine. 2025; 14(6):2005. https://doi.org/10.3390/jcm14062005
Chicago/Turabian StyleKilercik, Hakan, Sami Akbulut, Ahmed Elsarawy, Sema Aktas, Utku Alkara, and Sinasi Sevmis. 2025. "Effect of Complex Venous Outflow Drainage Reconstruction on Postoperative Graft Function in Right-Lobe Living Donor Liver Transplantation" Journal of Clinical Medicine 14, no. 6: 2005. https://doi.org/10.3390/jcm14062005
APA StyleKilercik, H., Akbulut, S., Elsarawy, A., Aktas, S., Alkara, U., & Sevmis, S. (2025). Effect of Complex Venous Outflow Drainage Reconstruction on Postoperative Graft Function in Right-Lobe Living Donor Liver Transplantation. Journal of Clinical Medicine, 14(6), 2005. https://doi.org/10.3390/jcm14062005