

Predictive Factors for Gait Recovery in Patients Undergoing Total Hip Arthroplasty: A Propensity Score Weighting Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants/Study Subjects
2.3. Description of Experiments, Treatment, or Surgery
2.4. Variables, Outcome Measures, Data Sources, and Bias
2.5. Data Processing and Propensity Score Weighting (PSW)
2.6. Statistical Analysis
3. Results
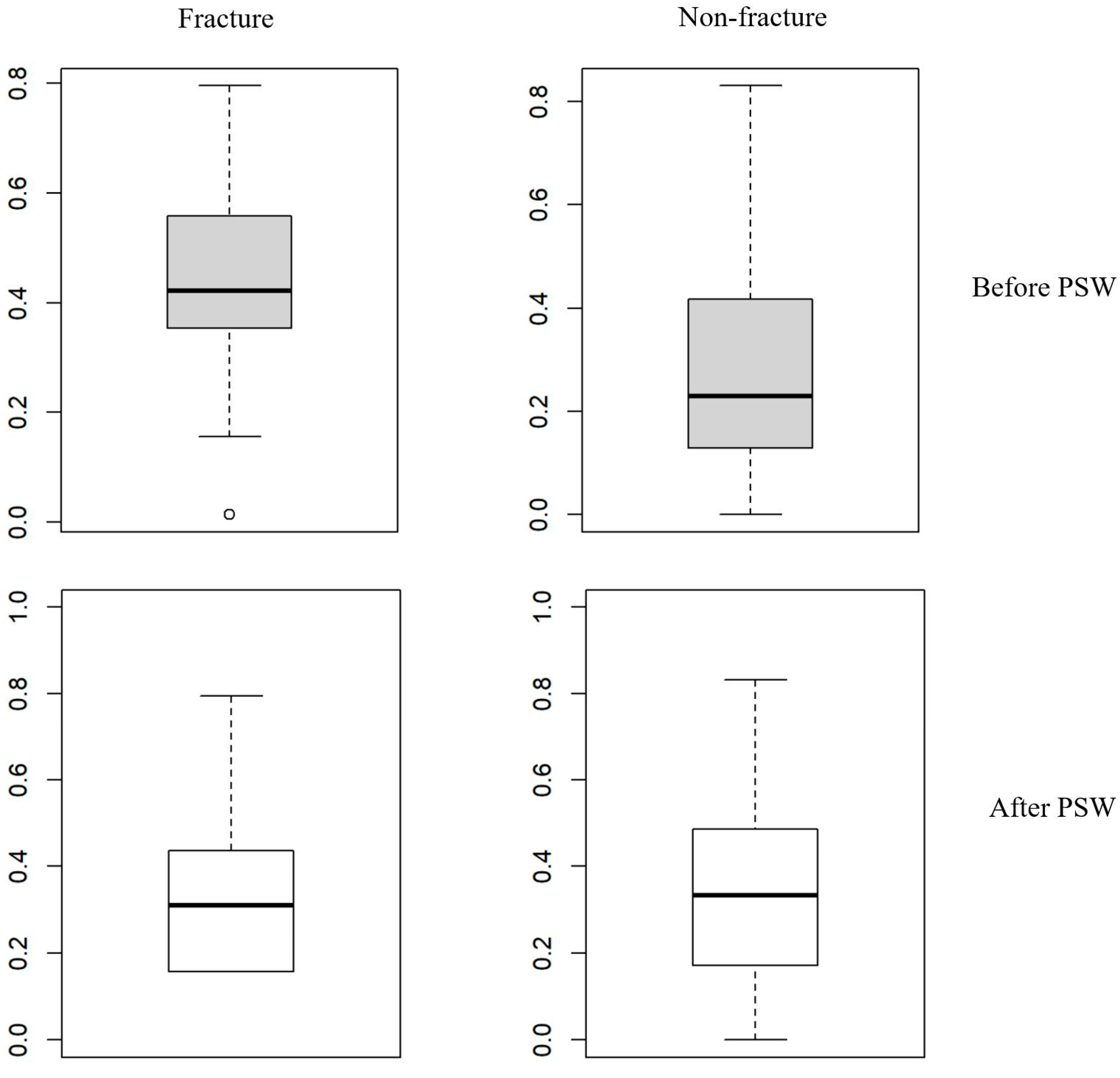
3.1. Characteristics of Participants Before and After PSW Prior to PSW
3.2. Univariate and Multivariate Logistic Regression Analysis
4. Discussion
Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pivec, R.; Johnson, A.J.; Mears, S.C.; Mont, M.A. Hip Arthroplasty. Lancet 2012, 380, 1768–1777. [Google Scholar] [CrossRef] [PubMed]
- Fontalis, A.; Epinette, J.-A.; Thaler, M.; Zagra, L.; Khanduja, V.; Haddad, F.S. Advances and Innovations in Total Hip Arthroplasty. SICOT-J. 2021, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, R.J.; Palmer, A.J.; Taylor, A.; Porter, M.L.; Malchau, H.; Glyn-Jones, S. Hip Replacement. Lancet 2018, 392, 1662–1671. [Google Scholar] [CrossRef]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of Total Joint Replacement in the United States: Future Projections to 2020–2040 Using the National Inpatient Sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef]
- Horstmann, T.; Listringhaus, R.; Haase, G.-B.; Grau, S.; Mündermann, A. Changes in Gait Patterns and Muscle Activity Following Total Hip Arthroplasty: A Six-Month Follow-Up. Clin. Biomech. 2013, 28, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Kolk, S.; Minten, M.J.; van Bon, G.E.; Rijnen, W.H.; Geurts, A.C.; Verdonschot, N.; Weerdesteyn, V. Gait and Gait-Related Activities of Daily Living after Total Hip Arthroplasty: A Systematic Review. Clin. Biomech. 2014, 29, 705–718. [Google Scholar] [CrossRef]
- Nantel, J.; Termoz, N.; Vendittoli, P.-A.; Lavigne, M.; Prince, F. Gait Patterns after Total Hip Arthroplasty and Surface Replacement Arthroplasty. Arch. Phys. Med. Rehabil. 2009, 90, 463–469. [Google Scholar] [CrossRef]
- Vissers, M.M.; Bussmann, J.B.; Verhaar, J.A.; Arends, L.R.; Furlan, A.D.; Reijman, M. Recovery of Physical Functioning after Total Hip Arthroplasty: Systematic Review and Meta-Analysis of the Literature. Phys. Ther. 2011, 91, 615–629. [Google Scholar] [CrossRef]
- Schniepp, R.; Möhwald, K.; Wuehr, M. Clinical and Automated Gait Analysis in Patients with Vestibular, Cerebellar, and Functional Gait Disorders: Perspectives and Limitations. J. Neurol. 2019, 266, 118–122. [Google Scholar] [CrossRef]
- Tanaka, R.; Shigematsu, M.; Motooka, T.; Mawatari, M.; Hotokebuchi, T. Factors Influencing the Improvement of Gait Ability after Total Hip Arthroplasty. J. Arthroplast. 2010, 25, 982–985. [Google Scholar] [CrossRef]
- Elings, J.; Hoogeboom, T.J.; van der Sluis, G.; van Meeteren, N.L. What Preoperative Patient-Related Factors Predict Inpatient Recovery of Physical Functioning and Length of Stay after Total Hip Arthroplasty? A Systematic Review. Clin. Rehabil. 2015, 29, 477–492. [Google Scholar] [CrossRef] [PubMed]
- Bandholm, T.; Wainwright, T.W.; Kehlet, H. Rehabilitation Strategies for Optimisation of Functional Recovery after Major Joint Replacement. J. Exp. Orthop. 2018, 5, 44. [Google Scholar] [CrossRef]
- Kennedy, D.M.; Hanna, S.E.; Stratford, P.W.; Wessel, J.; Gollish, J.D. Preoperative Function and Gender Predict Pattern of Functional Recovery after Hip and Knee Arthroplasty. J. Arthroplast. 2006, 21, 559–566. [Google Scholar] [CrossRef]
- Hofstede, S.N.; Gademan, M.G.; Vliet Vlieland, T.P.; Nelissen, R.G.; Marang-Van De Mheen, P.J. Preoperative Predictors for Outcomes after Total Hip Replacement in Patients with Osteoarthritis: A Systematic Review. BMC Musculoskelet. Disord. 2016, 17, 212. [Google Scholar] [CrossRef]
- Buirs, L.D.; Beers, L.W.A.H.V.; Scholtes, V.A.B.; Pastoors, T.; Sprague, S.; Poolman, R.W. Predictors of Physical Functioning after Total Hip Arthroplasty: A Systematic Review. BMJ Open 2016, 6, e010725. [Google Scholar] [CrossRef] [PubMed]
- Juan, J.; Leff, G.; Kevorken, K.; Jeanfavre, M. Hip Flexor Muscle Activation During Common Rehabilitation and Strength Exercises. J. Clin. Med. 2024, 13, 6617. [Google Scholar] [CrossRef] [PubMed]
- Rosenlund, S.; Holsgaard-Larsen, A.; Overgaard, S.; Jensen, C. The Gait Deviation Index Is Associated with Hip Muscle Strength and Patient-Reported Outcome in Patients with Severe Hip Osteoarthritis—A Cross-Sectional Study. PLoS ONE 2016, 11, e0153177. [Google Scholar] [CrossRef]
- Konnyu, K.J.; Pinto, D.; Cao, W.; Aaron, R.K.; Panagiotou, O.A.; Bhuma, M.R.; Adam, G.P.; Balk, E.M.; Thoma, L.M. Rehabilitation for Total Hip Arthroplasty: A Systematic Review. Am. J. Phys. Med. Rehabil. 2023, 102, 11–18. [Google Scholar] [CrossRef]
- dos Santos Mendes Costa, L.; de Lima, V.G.; da Silva Freires Barros, F.D.; Pereira, P.A.; Lima, R.M.A.; da Silva, A.K.A.; Tatmatsu-Rocha, J.C. Hip Arthroplasty: Effective Rehabilitation Protocols. Res. Soc. Dev. 2021, 10, e45510414370. [Google Scholar] [CrossRef]
- Bahl, J.S.; Nelson, M.J.; Taylor, M.; Solomon, L.B.; Arnold, J.B.; Thewlis, D. Biomechanical Changes and Recovery of Gait Function after Total Hip Arthroplasty for Osteoarthritis: A Systematic Review and Meta-Analysis. Osteoarthr. Cartil. 2018, 26, 847–863. [Google Scholar] [CrossRef]
- Le Manach, Y.; Collins, G.; Bhandari, M.; Bessissow, A.; Boddaert, J.; Khiami, F.; Chaudhry, H.; De Beer, J.; Riou, B.; Landais, P.; et al. Outcomes After Hip Fracture Surgery Compared With Elective Total Hip Replacement. JAMA 2015, 314, 1159–1166. [Google Scholar] [CrossRef]
- Desai, R.J.; Franklin, J.M. Alternative Approaches for Confounding Adjustment in Observational Studies Using Weighting Based on the Propensity Score: A Primer for Practitioners. BMJ 2019, 367, l5657. [Google Scholar] [CrossRef] [PubMed]
- Haukoos, J.S.; Lewis, R.J. The Propensity Score. JAMA 2015, 314, 1637–1638. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A Simulation Study of the Number of Events per Variable in Logistic Regression Analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Cifu, D.X. Braddom’s Physical Medicine and Rehabilitation, 6th ed.; Physical Agent Modalities; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Nankaku, M.; Tsuboyama, T.; Kakinoki, R.; Akiyama, H.; Nakamura, T. Prediction of Ambulation Ability Following Total Hip Arthroplasty. J. Orthop. Sci. 2011, 16, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Ross, C.; Raebel, M.A.; Shetterly, S.; Blanchette, C.; Smith, D. Use of Stabilized Inverse Propensity Scores as Weights to Directly Estimate Relative Risk and Its Confidence Intervals. Value Health 2010, 13, 273–277. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed]
- Normand, S.T.; Landrum, M.B.; Guadagnoli, E.; Ayanian, J.Z.; Ryan, T.J.; Cleary, P.D.; McNeil, B.J. Validating Recommendations for Coronary Angiography Following Acute Myocardial Infarction in the Elderly: A Matched Analysis Using Propensity Scores. J. Clin. Epidemiol. 2001, 54, 387–398. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards Best Practice When Using Inverse Probability of Treatment Weighting (IPTW) Using the Propensity Score to Estimate Causal Treatment Effects in Observational Studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Stuart, E.A. Matching Methods for Causal Inference: A Review and a Look Forward. Stat. Sci. 2010, 25, 1–21. [Google Scholar] [CrossRef]
- Shrader, M.W.; Bhowmik-Stoker, M.; Jacofsky, M.C.; Jacofsky, D.J. Gait and Stair Function in Total and Resurfacing Hip Arthroplasty: A Pilot Study. Clin. Orthop. Relat. Res. 2009, 467, 1476–1484. [Google Scholar] [CrossRef] [PubMed]
- Bergés, I.-M.; Kuo, Y.-F.; Ostir, G.V.; Granger, C.V.; Graham, J.E.; Ottenbacher, K.J. Gender and Ethnic Differences in Rehabilitation Outcomes after Hip-Replacement Surgery. Am. J. Phys. Med. Rehabil. 2008, 87, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Cherian, J.J.; Jinnah, A.H.; Robinson, K.; O’Connor, M.I.; Harwin, S.F.; Mont, M.A. Prospective, Longitudinal Evaluation of Gender Differences after Total Hip Arthroplasty. Orthopedics 2016, 39, e391–e396. [Google Scholar] [CrossRef]
- Queen, R.M.; Schmitt, D. Sex-Specific Difference in Dynamic Balance Following Total Hip Replacement. Innov. Aging 2021, 5, igab019. [Google Scholar] [CrossRef] [PubMed]
- Davidson, B.S.; Judd, D.; Dennis, D.A.; Stevens-Lapsley, J.E.; Winters, J.D.; Schenkman, M. Incorporating Neuromuscular Reeducation Techniques During Postoperative Rehabilitation Improves Functional Performance After Total Hip Arthroplasty: A Preliminary Study. J. Surg. Rehabil. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Röder, C.; Staub, L.P.; Eggli, S.; Dietrich, D.; Busato, A.; Müller, U. Influence of Preoperative Functional Status on Outcome after Total Hip Arthroplasty. JBJS 2007, 89, 11–17. [Google Scholar] [CrossRef]
- Krebs, D.E.; Robbins, C.E.; Lavine, L.; Mann, R.W. Hip Biomechanics during Gait. J. Orthop. Sports Phys. Ther. 1998, 28, 51–59. [Google Scholar] [CrossRef]
- Sato, H.; Kondo, S.; Saito, M.; Saura, R. Effects of Strengthening the Hip Flexor Muscles on Walking Ability and the Locomotive Syndrome Rank Test: An Intervention Study. J. Orthop. Sci. 2020, 25, 892–896. [Google Scholar] [CrossRef]
- Vandekerckhove, I.; Wesseling, M.; Kainz, H.; Desloovere, K.; Jonkers, I. The Effect of Hip Muscle Weakness and Femoral Bony Deformities on Gait Performance. Gait Posture 2021, 83, 280–286. [Google Scholar] [CrossRef]
- Rasch, A.; Dalén, N.; Berg, H.E. Muscle Strength, Gait, and Balance in 20 Patients with Hip Osteoarthritis Followed for 2 Years after THA. Acta Orthop. 2010, 81, 183–188. [Google Scholar] [CrossRef]
- Chevillotte, C.J.; Ali, M.H.; Trousdale, R.T.; Pagnano, M.W. Variability in Hip Range of Motion on Clinical Examination. J. Arthroplast. 2009, 24, 693–697. [Google Scholar] [CrossRef]
- Agostini, V.; Ganio, D.; Facchin, K.; Cane, L.; Carneiro, S.M.; Knaflitz, M. Gait Parameters and Muscle Activation Patterns at 3, 6 and 12 Months after Total Hip Arthroplasty. J. Arthroplast. 2014, 29, 1265–1272. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, M.L.; Lamontagne, M.; Beaulé, P.E. Lower Limb Biomechanics during Gait Do Not Return to Normal Following Total Hip Arthroplasty. Gait Posture 2010, 32, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Ewen, A.M.; Stewart, S.; Gibson, A.S.C.; Kashyap, S.N.; Caplan, N. Post-Operative Gait Analysis in Total Hip Replacement Patients—A Review of Current Literature and Meta-Analysis. Gait Posture 2012, 36, 1–6. [Google Scholar] [CrossRef]
- Yoo, J.-I.; Cha, Y.-H.; Kim, K.-J.; Kim, H.-Y.; Choy, W.-S.; Hwang, S.-C. Gait Analysis after Total Hip Arthroplasty Using Direct Anterior Approach versus Anterolateral Approach: A Systematic Review and Meta-Analysis. BMC Musculoskelet. Disord. 2019, 20, 63. [Google Scholar] [CrossRef] [PubMed]
- Hida, M.; Deguchi, Y.; Miyaguchi, K.; Nakazono, M.; Hirata, N.; Nakagawa, R.; Kitayama, A. Association between Acute Postoperative Pain and Recovery of Independent Walking Ability after Surgical Treatment of Hip Fracture. Prog. Rehabil. Med. 2018, 3, 20180012. [Google Scholar] [CrossRef]
- Brander, V.A.; Stulberg, S.D.; Adams, A.D.; Harden, R.N.; Bruehl, S.; Stanos, S.P.; Houle, T. Predicting Total Knee Replacement Pain: A Prospective, Observational Study. Clin. Orthop. Relat. Res. 2003, 416, 27–36. [Google Scholar] [CrossRef]

{kind=link}
| Before PSW | After PSW | |||||||
|---|---|---|---|---|---|---|---|---|
| Fracture | Non-Fracture | p-Value | SMD | Fracture | Non-Fracture | p-Value | SMD | |
| n | 73 | 148 | 84 | 150.5 | ||||
| Gender = M (%) | 32 (43.8) | 77 (52.0) | 0.252 | 0.165 | 50.9 (60.6) | 72.9 (48.5) | 0.356 | 0.246 |
| Age (mean (SD)) | 68.33 (8.68) | 61.73 (12.75) | <0.001 * | 0.605 | 61.95 (10.94) | 64.04 (12.26) | 0.589 | 0.18 |
| Preoperative gait ability (%) | 0.029 * | 0.518 | 0.334 | 0.472 | ||||
| Bed-ridden state | 0 (0.0) | 2 (1.4) | 0.0 (0.0) | 1.3 (0.9) | ||||
| Wheelchair mobile | 1 (1.4) | 5 (3.4) | 2.0 (2.4) | 4.2 (2.8) | ||||
| Assisted ambulation | 5 (6.8) | 5 (3.4) | 4.3 (5.1) | 9.6 (6.4) | ||||
| Independent ambulation with assistive device | 4 (5.5) | 29 (19.6) | 28.3 (33.7) | 22.1 (14.7) | ||||
| Independent ambulation without assistive device | 63 (86.3) | 107 (72.3) | 49.5 (58.9) | 113.3 (75.3) | ||||
| Duration of gait disturbance days (mean (SD)) | 52.67 (165.14) | 114.74 (386.23) | 0.19 | 0.209 | 205.40 (272.86) | 97.46 (337.69) | 0.32 | 0.352 |
| Duration of rehabilitation days (mean (SD)) | 18.79 (7.71) | 17.47 (13.60) | 0.442 | 0.12 | 16.24 (8.40) | 19.66 (20.21) | 0.375 | 0.221 |
| Interval between surgery to rehabilitation days (mean (SD)) | 6.03 (5.74) | 6.73 (4.94) | 0.348 | 0.131 | 7.45 (6.17) | 6.72 (4.92) | 0.522 | 0.131 |
| Muscle strength of operated hip | ||||||||
| Flexion > grade 3 (%) | 17 (23.3) | 59 (39.9) | 0.015 * | 0.362 | 39.5 (47.0) | 50.5 (33.5) | 0.381 | 0.278 |
| Abduction > grade 3 (%) | 18 (24.7) | 61 (41.2) | 0.016 * | 0.358 | 40.6 (48.3) | 52.5 (34.9) | 0.378 | 0.275 |
| G group (%) | 14 (19.2) | 58 (39.2) | 0.003 | 0.451 | 35.1 (41.8) | 53.0 (35.2) | 0.699 | 0.135 |
| G Group | P Group | p-Value | |
|---|---|---|---|
| n | 88.1 | 146.4 | |
| Gender = M (%) | 74.4 (84.4) | 49.5 (33.8) | <0.001 * |
| Age (mean (SD)) | 57.03 (11.52) | 67.06 (10.35) | <0.001 * |
| Preoperative ambulatory status (%) | 0.171 | ||
| Bed-ridden state | 0 (0.0) | 1.3 (0.9) | |
| Wheelchair mobile | 0.7 (0.8) | 5.5 (3.7) | |
| Assisted amulation | 0.0 (0.0) | 13.9 (9.5) | |
| Independent ambulation with assistive device | 28.4 (32.2) | 22.1 (15.1) | |
| Independent ambulation without assistive device | 59.0 (67.0) | 103.7 (70.8) | |
| Underlying disease (%) | 0.451 | ||
| Fracture | 35.1 (39.8) | 48.9 (33.4) | |
| Osteoarthritis | 23.1 (26.3) | 47.6 (32.5) | |
| Avascular necrosis | 27.7 (31.5) | 36.1 (24.6) | |
| Others | 2.1 (2.4) | 13.8 (9.4) | |
| Duration of gait disturbance days (mean (SD)) | 176.01 (259.08) | 112.14 (349.72) | 0.566 |
| Duration of rehabilitation days (mean (SD)) | 14.07 (10.26) | 21.06 (19.57) | 0.050 |
| Interval from surgery to rehabilitation days (mean (SD)) | 7.68 (4.76) | 6.56 (5.73) | 0.256 |
| Muscle strength of operated hip | |||
| Flexion > grade 3 (%) | 56.0 (63.6) | 34.0 (23.2) | <0.001 * |
| Abduction > grade 3 (%) | 56.0 (63.6) | 37.1 (25.3) | 0.001 * |
| Odds Ratio | CIL | CIH | p-Value | |
|---|---|---|---|---|
| n | ||||
| Gender, male | 1.382 | 1.225 | 1.560 | <0.001 * |
| Age, year | 0.990 | 0.985 | 0.995 | <0.001 * |
| Preoperative gait ability | ||||
| Bed-ridden state | Ref | |||
| Wheelchair mobile | 1.189 | 0.752 | 1.881 | 0.459 |
| Assisted ambulation | 1.326 | 0.867 | 2.030 | 0.195 |
| Independent ambulation with assistive device | 1.654 | 1.093 | 2.502 | 0.018 * |
| Independent ambulation without assistive device | 1.531 | 1.029 | 2.276 | 0.037 * |
| Underlying disease | ||||
| Fracture | Ref | |||
| Osteoarthritis | 1.078 | 0.946 | 1.228 | 0.262 |
| Avascular necrosis | 1.064 | 0.928 | 1.220 | 0.373 |
| Others | 0.889 | 0.735 | 1.075 | 0.225 |
| Duration of gait disturbance.days | 1.000 | 1.000 | 1.000 | 0.916 |
| Duration of rehabilitation.days | 0.999 | 0.995 | 1.002 | 0.475 |
| Interval from surgery to rehabilitation.days | 1.003 | 0.989 | 1.017 | 0.665 |
| Muscle strength of operated limb | ||||
| Flexion > grade 3 vs. ≤grade 3 | 1.516 | 1.177 | 1.953 | 0.002 * |
| Abduction > grade 3 vs. ≤grade 3 | 0.791 | 0.622 | 1.005 | 0.057 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Kim, S.Y.; Shim, S.R.; Hyun, J.K. Predictive Factors for Gait Recovery in Patients Undergoing Total Hip Arthroplasty: A Propensity Score Weighting Analysis. J. Clin. Med. 2025, 14, 1979. https://doi.org/10.3390/jcm14061979
Kim Y, Kim SY, Shim SR, Hyun JK. Predictive Factors for Gait Recovery in Patients Undergoing Total Hip Arthroplasty: A Propensity Score Weighting Analysis. Journal of Clinical Medicine. 2025; 14(6):1979. https://doi.org/10.3390/jcm14061979
Chicago/Turabian StyleKim, Yuna, Seo Young Kim, Sung Ryul Shim, and Jung Keun Hyun. 2025. "Predictive Factors for Gait Recovery in Patients Undergoing Total Hip Arthroplasty: A Propensity Score Weighting Analysis" Journal of Clinical Medicine 14, no. 6: 1979. https://doi.org/10.3390/jcm14061979
APA StyleKim, Y., Kim, S. Y., Shim, S. R., & Hyun, J. K. (2025). Predictive Factors for Gait Recovery in Patients Undergoing Total Hip Arthroplasty: A Propensity Score Weighting Analysis. Journal of Clinical Medicine, 14(6), 1979. https://doi.org/10.3390/jcm14061979