
Rasch Analysis of the QuickDASH in Patients with Neck Pain

Abstract
1. Introduction
2. Materials and Methods
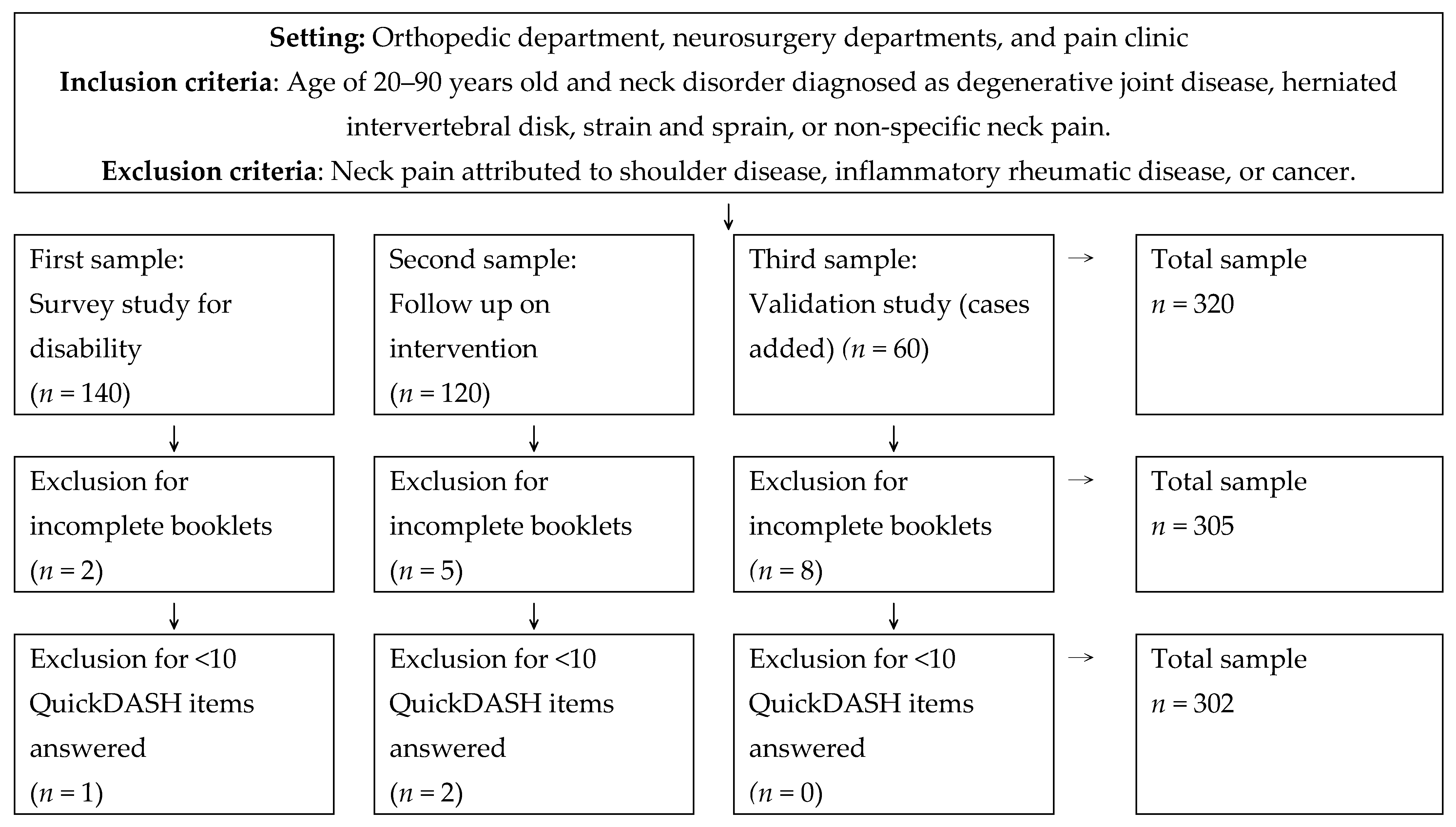
2.1. Participants
2.2. Instrument
2.3. Rasch Analysis
2.3.1. Unidimensionality
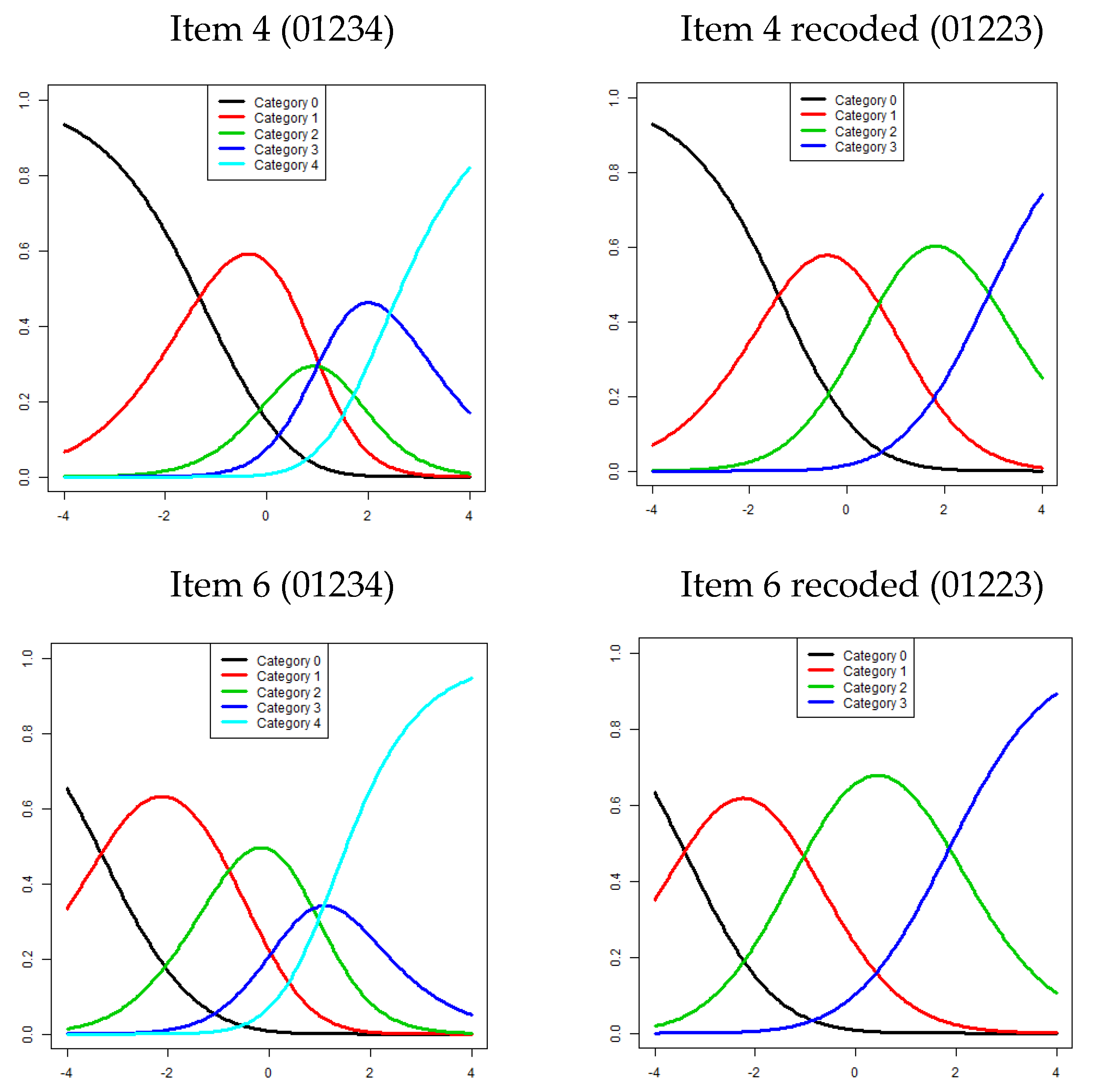
2.3.2. Category Function
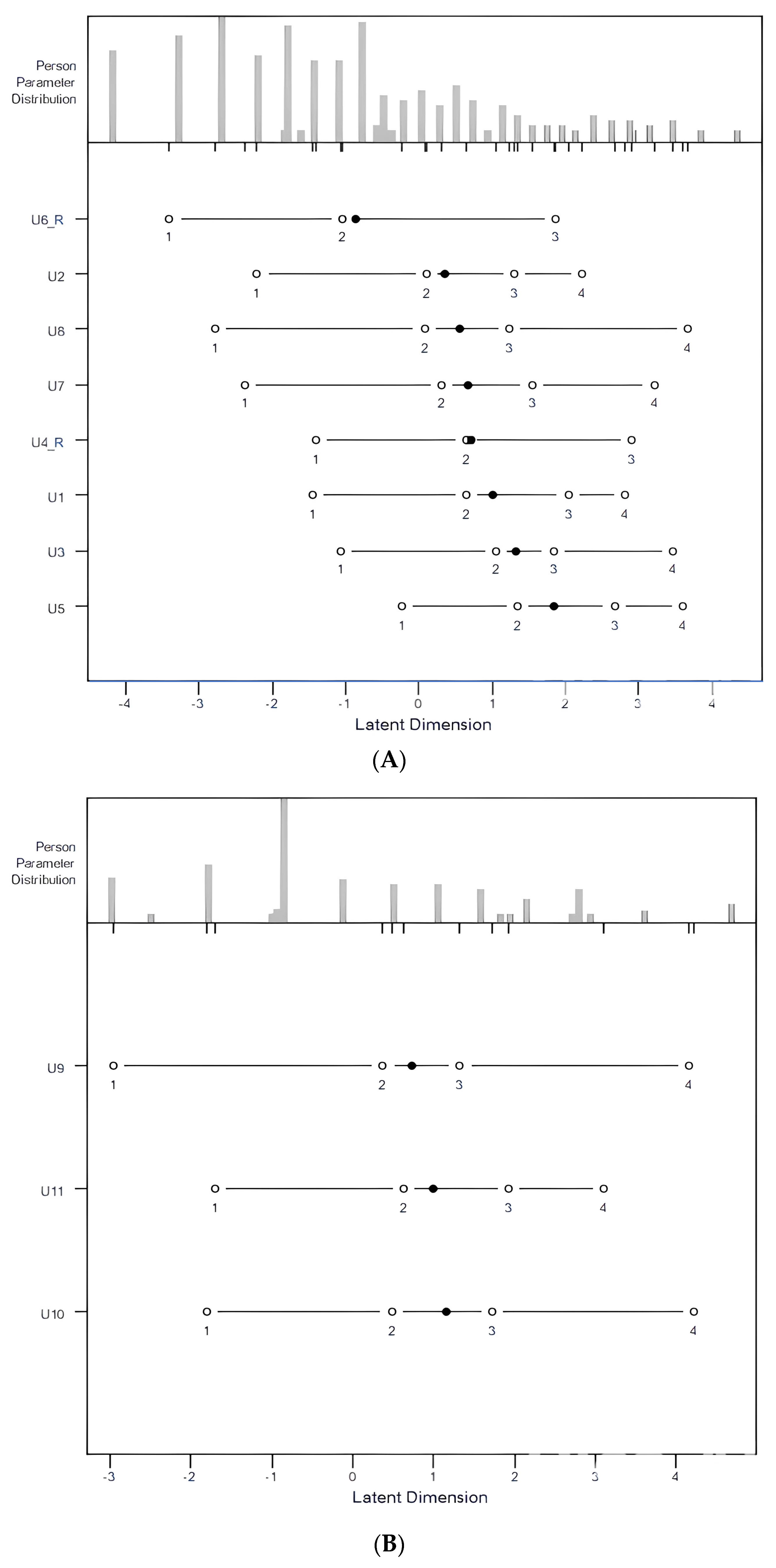
2.3.3. Item Difficulty and Targeting
2.3.4. Reliability
3. Results
3.1. Demographic Data
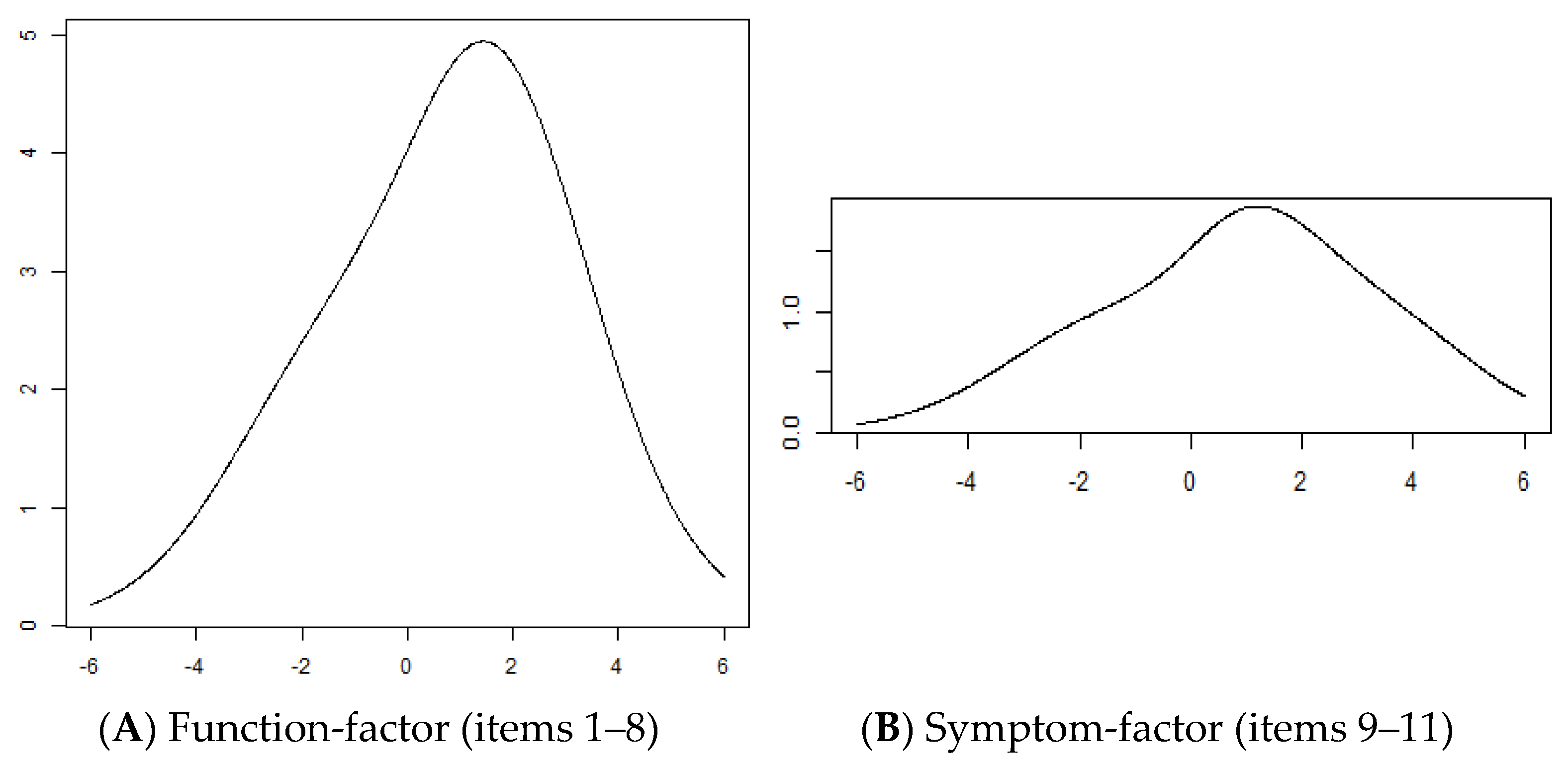
3.2. Rasch Analysis for the Function Factor
3.3. Rasch Analysis for the Symptom Factor
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| QuickDASH | Quick Disability of the Arm, Shoulder, and Hand |
| InfitMNSQ | Weighted mean square of the infit mean square |
| OutfitMNSQ | Unweighted mean square of the outfit mean square |
References
- Osborn, W.; Jull, G. Patients with non-specific neck disorders commonly report upper limb disability. Man. Ther. 2013, 18, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Wright, J.G.; Katz, J.N.; Upper Extremity Collaborative Group. Development of the QuickDASH: Comparison of three item-reduction approaches. J. Bone Jt. Surg. Am. 2005, 87, 1038–1046. [Google Scholar]
- Wiitavaara, B.; Florin, J. Content and psychometric evaluations of questionnaires for assessing physical function in people with arm-shoulder-hand disorders. A systematic review of the literature. Disabil. Rehabil. 2022, 44, 7575–7586. [Google Scholar] [CrossRef] [PubMed]
- Baylor, C.; Hula, W.; Donovan, N.J.; Doyle, P.J.; Kendall, D.; Yorkston, K. An introduction to item response theory and Rasch models for speech-language pathologists. Am. J. Speech Lang. Pathol. 2011, 20, 243–259. [Google Scholar] [CrossRef] [PubMed]
- Wright, B.D.; Linacre, J.M. Observations are always ordinal; measurements, however, must be interval. Arch. Phys. Med. Rehabil. 1989, 70, 857–860. [Google Scholar] [PubMed]
- Hsieh, C.L.; Jang, Y.; Yu, T.Y.; Wang, W.C.; Sheu, C.F.; Wang, Y.H. A Rasch analysis of the Frenchay Activities Index in patients with spinal cord injury. Spine 2007, 32, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Wright, B.D.; Masters, F. Rating Scale Analysis; Mesa Press: Chicago, IL, USA, 1982. [Google Scholar]
- Franchignoni, F.; Ferriero, G.; Giordano, A.; Sartorio, F.; Vercelli, S.; Brigatti, E. Psychometric properties of QuickDASH—A classical test theory and Rasch analysis study. Man. Ther. 2011, 16, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Jerosch-Herold, C.; Chester, R.; Shepstone, L. Rasch model analysis gives new insights into the structural validity of the QuickDASH in patients with musculoskeletal shoulder pain. J. Orthop. Sports Phys. Ther. 2017, 47, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Stirling, P.H.C.; McEachan, J.E.; Rodrigues, J.N.; Geoghegan, L.; Harrison, C.J. Modified scoring of the QuickDASH can achieve previously-unattained interval-level measurement in Dupuytren Disease and Carpal Tunnel Syndrome. Plast. Reconstr. Surg. Glob. Open 2024, 12, e5372. [Google Scholar] [CrossRef] [PubMed]
- Lue, Y.J.; Cheng, K.I.; Lin, C.L.; Chen, C.H.; Lu, Y.M. Psychometric properties of the QuickDASH in patients with neck pain. J. Clin. Med. 2025, 14, 1266. [Google Scholar] [CrossRef] [PubMed]
- Wright, B.D.; Mok, M. Rasch models overview. J. Appl. Meas. 2000, 1, 83–106. [Google Scholar] [PubMed]
- Linacre, J.M. A User’s Guide to Winsteps, Ministep Rasch-Model Computer Programs; Winsteps.com: Chicago, IL, USA, 2008. [Google Scholar]
- Decruynaere, C.; Thonnard, J.L.; Plaghki, L. How many response levels do children distinguish on faces scales for pain assessment? Eur. J. Pain 2009, 13, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Linacre, J.M. Optimizing rating scale category effectiveness. J. Appl. Meas. 2002, 3, 85–106. [Google Scholar] [PubMed]
- Lai, J.S.; Cella, D.; Dineen, K.; Bode, R.; Roenn, J.V.; Gershon, R.C.; Shevrin, D. An item bank was created to improve the measurement of cancer-related fatigue. J. Clin. Epidemiol. 2005, 58, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.M.; Wu, Y.Y.; Hsieh, C.L.; Lin, C.L.; Hwang, S.L.; Cheng, K.I.; Lue, Y.J. Measurement precision of the disability for back pain scale-by applying Rasch analysis. Health Qual. Life Outcomes 2013, 11, 119. [Google Scholar] [CrossRef] [PubMed]
- McCartney, S.; Baskerville, R.; Blagg, S.; McCartney, D. Cervical radiculopathy and cervical myelopathy: Diagnosis and management in primary care. Br. J. Gen. Pract. 2018, 68, 44–46. [Google Scholar] [CrossRef] [PubMed]
- Cuenca-Zaldívar, J.N.; Fernández-Carnero, J.; Sánchez-Romero, E.A.; Álvarez-Gonzalo, V.; Conde-Rodríguez, R.; Rodríguez-Sanz, D.; Calvo-Lobo, C. Effects of a therapeutic exercise protocol for patients with chronic non-specific back pain in primary health care: A single-group retrospective cohort study. J. Clin. Med. 2023, 12, 6478. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, A.M.; Schiphorst Preuper, H.R.; Balk, G.A.; Stewart, R.E. Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain 2014, 155, 2545–2550. [Google Scholar] [CrossRef] [PubMed]
- Linacre, J.M. Sample size and item calibration stability. Rasch Meas. Trans. 1994, 7, 328. [Google Scholar]
- Mokkink, L.B.; Prinsen, C.A.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; De Vet, H.C.; Terwee, C.B. COSMIN Study Design Checklist for Patient-Reported Outcome Measurement Instruments; COSMIN: Amsterdam, The Netherlands, 2019; pp. 1–32. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mean ± SD (Range) Percentage |
|---|---|
| Age (years) | 57.9 ± 10.4 (21–84) |
| 21–49 | 18.9% |
| 50–64 | 56.0% |
| 65–84 | 25.1% |
| Gender | |
| Male | 42.4% |
| Female | 57.6% |
| Disease duration (month) | 54.2 ± 79.8 (0.3–600) |
| Acute (<6 wk) | 7.8% |
| Subacute (6 wk–3 mo) | 12.0% |
| Chronic (>3 mo) | 80.2% |
| Education | |
| Elementary school | 23.4% |
| High school | 52.2% |
| University | 24.4% |
| Marital status | |
| Single/widowed | 16.1% |
| Married | 83.9% |
| Occupation | |
| Office worker | 23.3% |
| Laborer | 22.4% |
| Homemaker | 22.4% |
| Unemployed | 5.7% |
| Retired | 26.2% |
| Diagnosis | |
| Degenerative joint disease | 37.9% |
| Herniated intervertebral disk | 29.0% |
| Strain/sprain | 10.6% |
| Non-specific neck pain | 22.5% |
| VAS score | |
| Neck | 3.9 ± 2.9 (0–10) |
| Arm | 3.6 ± 3.0 (0–10) |
| Item | Difficulty Logit | InfitMNSQ | OutfitMNSQ | Threshold 1 | Threshold 2 | Threshold 3 | Threshold 4 |
|---|---|---|---|---|---|---|---|
| 1: Difficulty opening a jar | 1.016 | 1.124 | 1.121 | −1.447 | 0.653 | 2.038 | 2.818 |
| 2: Difficulty performing household chores | 0.359 | 0.747 | 0.757 | −2.206 | 0.108 | 1.297 | 2.237 |
| 3: Difficulty carrying a shopping bag | 1.321 | 0.774 | 0.821 | −1.061 | 1.049 | 1.836 | 3.461 |
| 4: Difficulty washing your back | 0.721 | 1.017 | 1.081 | −1.401 | 0.652 | 2.911 | NA |
| 5: Difficulty using a knife | 1.845 | 0.700 | 0.661 | −0.237 | 1.348 | 2.668 | 3.601 |
| 6: Difficulty in recreational activities | −0.858 | 0.955 | 0.934 | −3.404 | −1.035 | 1.866 | NA |
| 7: Interference with social activities | 0.671 | 0.938 | 0.893 | −2.378 | 0.307 | 1.544 | 3.211 |
| 8: Limitation in work/daily activities | 0.551 | 0.857 | 0.839 | −2.787 | 0.074 | 1.235 | 3.682 |
| Item | Difficulty Logit | Infit MNSQ | Outfit MNSQ | Threshold 1 | Threshold 2 | Threshold 3 | Threshold 4 |
|---|---|---|---|---|---|---|---|
| 1: Pain severity | 0.721 | 0.522 | 0.517 | −2.966 | 0.372 | 1.327 | 4.153 |
| 2: Tingling severity | 1.154 | 0.602 | 0.603 | −1.802 | 0.478 | 1.727 | 4.213 |
| 3: Difficulty sleeping | 0.990 | 0.863 | 0.885 | −1.700 | 0.630 | 1.926 | 3.106 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Y.-M.; Wu, Y.-Y.; Lue, Y.-J. Rasch Analysis of the QuickDASH in Patients with Neck Pain. J. Clin. Med. 2025, 14, 1870. https://doi.org/10.3390/jcm14061870
Lu Y-M, Wu Y-Y, Lue Y-J. Rasch Analysis of the QuickDASH in Patients with Neck Pain. Journal of Clinical Medicine. 2025; 14(6):1870. https://doi.org/10.3390/jcm14061870
Chicago/Turabian StyleLu, Yen-Mou, Yuh-Yih Wu, and Yi-Jing Lue. 2025. "Rasch Analysis of the QuickDASH in Patients with Neck Pain" Journal of Clinical Medicine 14, no. 6: 1870. https://doi.org/10.3390/jcm14061870
APA StyleLu, Y.-M., Wu, Y.-Y., & Lue, Y.-J. (2025). Rasch Analysis of the QuickDASH in Patients with Neck Pain. Journal of Clinical Medicine, 14(6), 1870. https://doi.org/10.3390/jcm14061870