
Non-Invasive Ventilation: When, Where, How to Start, and How to Stop

 ,
, 
Abstract
1. Introduction
2. Methodology
3. Epidemiology
4. Indications for NIV According to Recent Guidelines
5. NIV Weaning: Initiation Criteria and Monitoring Guidelines
- Effective cough and minimal secretions
- Stability of the primary issue that necessitated intubation
- Absence of acute infection
- Hemodynamic stability: heart rate ≤ 140 bpm, systolic BP 90–160 mmHg, with minimal or no vasopressors
- Adequate oxygenation: SpO2 ≥ 90% on FiO2 ≤ 40%, or PaO2/FiO2 ≥150 mmHg
- PEEP ≤ 8 cmH2O
- Respiratory rate < 35 breaths/min
- Absence of significant apneic episodes
- Tidal volume ≥ 5 mL/kg
- Adequate mental status
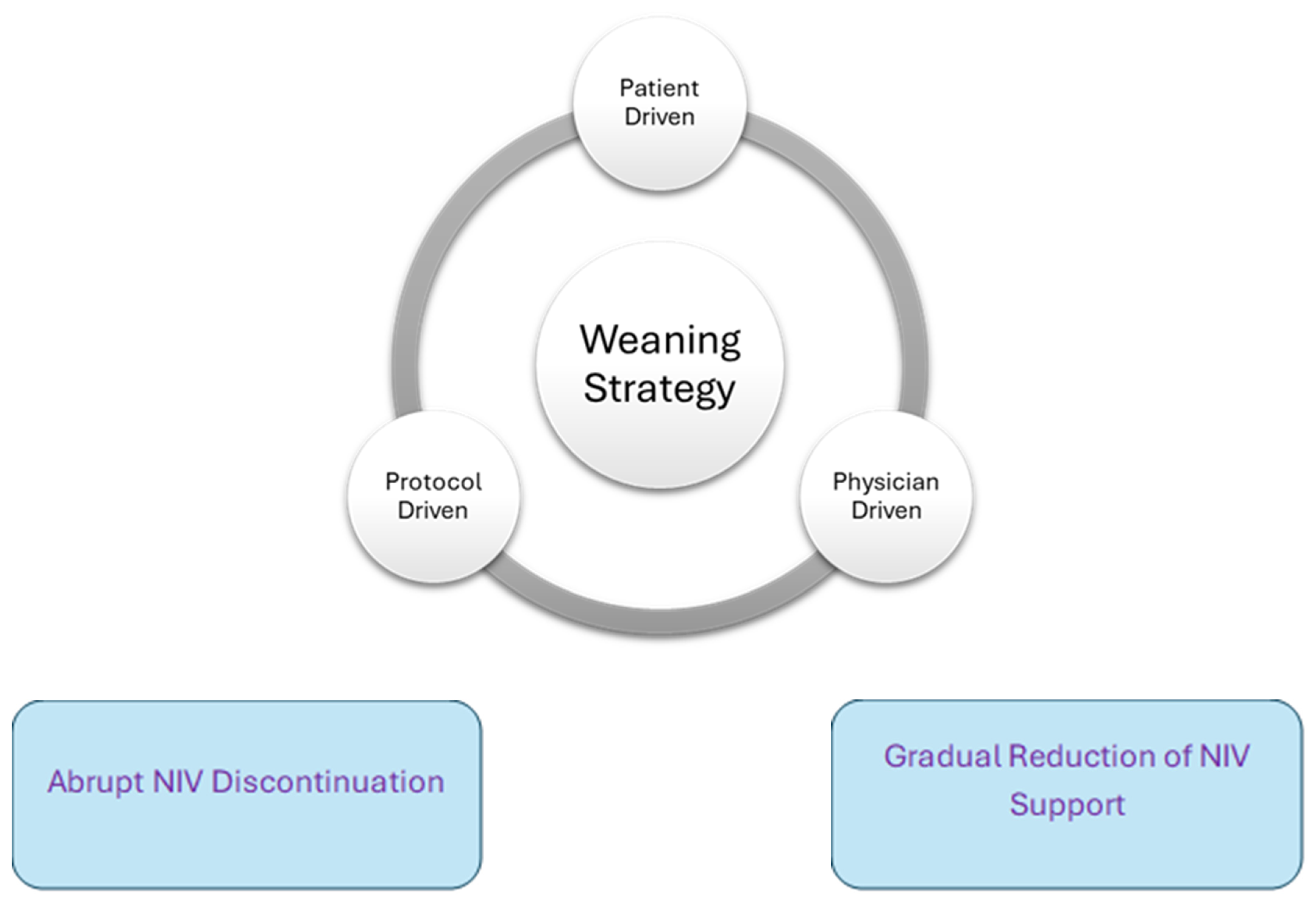
6. Weaning Strategies and Techniques for NIV
- Gradual weaning
- 2.
- Abrupt discontinuation
7. Location for Weaning
- ICU.
- 2.
- Step-down/high-dependency units (HDUs).
- 3.
- General medical floors.
8. Predictors of Successful Weaning
- H—Heart rate
- A—Acidosis (pH)
- C—Consciousness (Glasgow Coma Scale)
- O—Oxygenation (PaO2/FiO2)
- R—Respiratory rate
9. Predictors for Failure of Weaning and Need for Escalation
10. Methods of Escalation
11. Outcomes of Failure to Wean
12. Limitations
13. Future Directions
14. Conclusions
Funding
Conflicts of Interest
References
- Stewart, S.; Hua, A.; Lillis, A.; Coppel, J.; O’Shaughnessy, T.C.; Macavei, V.M. Non-invasive ventilation simulation session outcomes in healthcare professionals. Eur. Respir. J. 2016, 48 (Suppl. S60), PA3061. [Google Scholar]
- Gao, F.; Li-Hong, Y.; Hai-Rong, H.; Xian-Cang, M.; Xian-Cang, M.; Jun, L.; Ya-Jing, Z.; Li-Tao, G.; Xue, W.; Jie, Z. The effect of reintubation on ventilator-associated pneumonia and mortality among mechanically ventilated patients with intubation: A systematic review and meta-analysis. Heart Lung 2016, 45, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Chihara, Y.; Egawa, H.; Oga, T.; Tsuboi, T.; Handa, T.; Yagi, S.; Iida, T.; Yoshizawa, A.; Yamamoto, K.; Mishima, M. Predictive Factors for Reintubation following Noninvasive Ventilation in Patients with Respiratory Complications after Living Donor Liver Transplantation. PLoS ONE 2013, 8, e81417. [Google Scholar] [CrossRef] [PubMed]
- Esteban, A.; Frutos-Vivar, F.; Ferguson, N.D.; Arabi, Y.; Apezteguía, C.; González, M.; Epstein, S.K.; Hill, N.S.; Nava, S.; Soares, M.A.; et al. Noninvasive Positive-Pressure Ventilation for Respiratory Failure after Extubation. N. Engl. J. Med. 2004, 350, 2452–2460. [Google Scholar] [CrossRef]
- Hirsch, K.G.; Abella, B.S.; Amorim, E.; Bader, M.K.; Barletta, J.F.; Berg, K.; Callaway, C.W.; Friberg, H.; Gilmore, E.J.; Greer, D.M. Critical Care Management of Patients After Cardiac Arrest: A Scientific Statement from the American Heart Association and Neurocritical Care Society. Circulation 2024, 149, e168–e200. [Google Scholar] [CrossRef]
- Cîvîrjic, I.; Nerpii, A.; Stefantov, N.; Voleac, I.; Cernei, N.; Gherasim, O.; Șandru, S. Parameters predicting non-invasive ventilation failure in COVID-19 patients. Mold. J. Health Sci. 2024, 11, 3–10. [Google Scholar]
- Karagiannidis, C.; Hentschker, C.; Westhoff, M.; Weber-Carstens, S.; Janssens, U.; Kluge, S.; Pfeifer, M.; Spies, C.; Welte, T.; Rossaint, R.; et al. Observational study of changes in utilization and outcomes in mechanical ventilation in COVID-19. PLoS ONE 2022, 17, e0262315. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ouellette, D.R.; Patel, S.; Girard, T.D.; Kress, J.P.; Thille, A.W.; Brochard, L.; Mancebo, J.; Talmor, D.; Mehta, S.; Matthay, M.A.; et al. Liberation from mechanical ventilation in critically ill adults: An official American College of Chest Physicians/American Thoracic Society clinical practice guideline: Inspiratory pressure augmentation during spontaneous breathing trials, protocols minimizing sedation, and noninvasive ventilation immediately after extubation. Chest 2017, 151, 166–180. [Google Scholar]
- Ruzsics, I.; Matrai, P.; Hegyi, P.; Nemeth, D.; Tenk, J.; Csenkey, A.; Eross, B.; Varga, G.; Balasko, M.; Petervari, E.; et al. Noninvasive ventilation improves the outcome in patients with pneumonia-associated respiratory failure: Systematic review and meta-analysis. J. Infect. Public Health 2022, 15, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Demoule, A.; Chevret, S.; Carlucci, A.; Kouatchet, A.; Jaber, S.; Meziani, F.; Schmidt, M.; Schnell, D.; Clergue, C.; Aboab, J.; et al. Changing use of noninvasive ventilation in critically ill patients: Trends over 15 years in francophone countries. Intensive Care Med. 2016, 42, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.R.; Kim, H.; Gozalo, P.L.; Bunker, J.; Teno, J.M. Trends in Noninvasive and Invasive Mechanical Ventilation Among Medicare Beneficiaries at the End of Life. JAMA Intern. Med. 2021, 181, 93–102. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fortis, S.; Gao, Y.; Rewerts, K.; Sarrazin, M.V.; Kaboli, P.J. Home noninvasive ventilation use in patients hospitalized with COPD. Clin. Respir. J. 2023, 17, 811–815. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nava, S.; Hill, N. Non-invasive ventilation in acute respiratory failure. Lancet 2009, 374, 250–259. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Criner, G.J.; Gayen, S.; Zantah, M.; Dominguez Castillo, E.; Naranjo, M.; Lashari, B.; Pourshahid, S.; Gangemi, A. Clinical review of non-invasive ventilation. Eur. Respir. J. 2024, 64, 2400396. [Google Scholar] [CrossRef] [PubMed]
- Rochwerg, B.; Brochard, L.; Elliott, M.W.; Hess, D.; Hill, N.S.; Nava, S.; Navalesi, P.; Antonelli, M.; Brozek, J.L.; Conti, G.; et al. Official ERS/ATS clinical practice guidelines: Noninvasive ventilation for acute respiratory failure. Eur. Respir. J. 2017, 50, 1602426. [Google Scholar] [CrossRef]
- Lemiale, V.; Mokart, D.; Resche-Rigon, M.; Lambert, J.; Mayaux, J.; Vincent, F.; Benoit, D.; Azoulay, E.; Schlemmer, B.; Darmon, M.; et al. Effect of noninvasive ventilation vs oxygen therapy on mortality among immunocompromised patients with acute respiratory failure: A randomized clinical trial. JAMA 2015, 314, 1711–1719. [Google Scholar] [CrossRef]
- Frat, J.P.; Ragot, S.; Girault, S.; Thille, A.W.; Perbet, S.; Prat, G.; Richard, J.C.; Mercat, A.; Robert, R.; Gacouin, A.; et al. Effect of non-invasive oxygenation strategies in immunocompromised patients with severe acute respiratory failure: A post-hoc analysis of a randomized trial. Lancet Respir. Med. 2016, 4, 646–652. [Google Scholar] [CrossRef]
- Jaber, S.; Chanques, G.; Jung, B.; Sebbane, M.; Verzilli, D.; Carr, J.; Capdevila, X.; Mehta, S.; Jung, B.; Blanch, L.; et al. Postoperative noninvasive ventilation. Anesthesiology 2010, 112, 453–461. [Google Scholar] [CrossRef]
- Auriany, G.; Jallot, A.; Herve, P.; Andreu, M.; Guéret-Ricevuto, C.; Mertens, P.; Lemaire, F.; Rouby, J.J. Noninvasive ventilation reduces mortality in acute respiratory failure following lung resection. Am. J. Respir. Crit. Care Med. 2001, 164, 1231–1235. [Google Scholar] [CrossRef]
- Jaber, S.; Lescot, T.; Futier, E.; Petit, A.; Pereira, B.; Ruckly, S.; Ouanes, I.; Molinari, N.; Lucet, J.C.; Perez, P.; et al. Effect of noninvasive ventilation on tracheal reintubation among patients with hypoxemic respiratory failure following abdominal surgery: A randomized clinical trial. JAMA 2016, 315, 1345–1353. [Google Scholar] [CrossRef]
- Bolliger, C.T.; Van Eeden, S.F. Treatment of multiple rib fractures randomized controlled trial comparing ventilatory with nonventilatory management. Chest 1990, 97, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Gunduz, M.; Unlugenc, H.; Ozalevli, M.; Kiyan, E.; Ozdogan, S.; Kayhan, S.; Topuz, O.; Altintas, N.; Basoglu, O.K. A comparative study of continuous positive airway pressure (CPAP) and intermittent positive pressure ventilation (IPPV) in patients with flail chest. Emerg. Med. J. 2005, 22, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, M.; Valencia, M.; Nicolas, J.M.; Torres, A.; de la Bellacasa, J.P.; Gonzalez, G.; Carriedo, D.; Sellares, J.; Marrades, R.M.; Roca, J.; et al. Early noninvasive ventilation averts extubation failure in patients at risk: A randomized trial. Am. J. Respir. Crit. Care Med. 2006, 173, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Nava, S.; Gregoretti, C.; Fanfulla, F.; Squadrone, E.; Navarra, A.; Rampulla, C.; Rubini, F.; Marangio, E.; Vitacca, M. Noninvasive ventilation to prevent respiratory failure after extubation in high-risk patients. Crit. Care Med. 2005, 33, 2465–2470. [Google Scholar] [CrossRef]
- Blackwood, B.; Alderdice, F.; Burns, K.; Cardwell, C.R.; Lavery, G.; O’Halloran, P.; Bell, E.; O’Connor, T.; Cooper, C.; Connolly, B.; et al. Use of weaning protocols for reducing duration of mechanical ventilation in critically ill adult patients: Cochrane systematic review and meta-analysis. BMJ 2011, 342, c7237. [Google Scholar] [CrossRef]
- Boles, J.M.; Bion, J.; Connors, A.; Herridge, M.; Marsh, B.; Melot, C.; Pearl, R.; Silverman, H.; Stewart, T.; Welte, T.; et al. Weaning from mechanical ventilation. Eur. Respir. J. 2007, 29, 1033–1056. [Google Scholar] [CrossRef]
- Masip, J.; Peacock, W.F.; Price, S.; Cullen, L.; Martin-Sanchez, F.J.; Seferovic, P.; Maisel, A.S.; Miro, O.; Filippatos, G.; Vrints, C.; et al. Indications and practical approach to non-invasive ventilation in acute heart failure. Eur. Heart J. 2018, 39, 17–25. [Google Scholar] [CrossRef]
- Carron, M.; Freo, U.; BaHammam, A.S.; Navalesi, P.; Fanfulla, F.; Antonelli, M.; Navari, N.; Spadaro, S.; Esquinas, A.M.; Nava, S.; et al. Complications of non-invasive ventilation techniques: A comprehensive qualitative review of randomized trials. Br. J. Anaesth. 2013, 110, 896–914. [Google Scholar] [CrossRef]
- Ugurlua, A.O.; Ergan, B. How do I wean a patient with acute hypercapnic respiratory failure from noninvasive ventilation? Pulmonology 2023, 29, 144–150. [Google Scholar] [CrossRef]
- Schmidt, G.A.; Girard, T.D.; Kress, J.P.; Thille, A.W.; Mancebo, J.; Talmor, D.; Brochard, L.; Mehta, S.; Matthay, M.A.; Patel, S.; et al. Official executive summary of an American Thoracic Society/American College of Chest Physicians clinical practice guideline: Liberation from mechanical ventilation in critically ill adults. Am. J. Respir. Crit. Care Med. 2017, 195, 115–119. [Google Scholar] [CrossRef]
- Yi, L.J.; Tian, X.; Chen, M.; Ding, Q.; Chen, Z.; Wu, Y.; Liu, D.; Zhang, S.; Xu, X.; Huang, W.; et al. Comparative efficacy and safety of four different spontaneous breathing trials for weaning from mechanical ventilation: A systematic review and network meta-analysis. Front. Med. 2021, 8, 731196. [Google Scholar] [CrossRef]
- Faverio, P.; Stainer, A.; De Giacomi, F.; Ryu, J.H.; Della Casa, G.; Rossi, G.; Polverino, E.; Guglielmi, G.; Blasi, F. Noninvasive ventilation weaning in acute hypercapnic respiratory failure due to COPD exacerbation: A real-life observational study. Can. Respir. J. 2019, 2019, 3478968. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Tang, X.; Huang, S.; Zhan, Q.; Fan, Y.; Yuan, J.; Deng, J.; Liu, Y.; Wang, C. Protocol-directed versus physician-directed weaning from noninvasive ventilation: The impact on chronic obstructive pulmonary disease patients. J. Trauma Acute Care Surg. 2012, 72, 1271–1275. [Google Scholar] [CrossRef] [PubMed]
- Suzanne, M.; Amaddeo, A.; Pin, I.; Milési, C.; Mortamet, G. Weaning from Noninvasive Ventilation and High Flow Nasal Cannula in Bronchiolitis: A Survey of Practice. Pediatr. Pulmonol. 2020, 55, 3104–3109. [Google Scholar] [CrossRef] [PubMed]
- Munshi, L.; Mancebo, J.; Brochard, L.J. Noninvasive Respiratory Support for Adults with Acute Respiratory Failure. N. Engl. J. Med. 2022, 387, 1688–1698. [Google Scholar] [CrossRef]
- Lun, C.T.; Chan, V.L.; Leung, W.S.; Lam, W.K.; Chan, C.K.; Ng, L.W.; Chow, M.P.; Tsang, K.Y. A pilot randomized study comparing two methods of non-invasive ventilation withdrawal after acute respiratory failure in chronic obstructive pulmonary disease. Respirology 2013, 18, 814–819. [Google Scholar] [CrossRef]
- Sellares, J.; Ferrer, M.; Anton, A.; Almirall, J.; Blanch, L.; Balcells, E.; Ballester, E.; Roca, J.; Hernández, G.; Masclans, J.R.; et al. Discontinuing noninvasive ventilation in severe chronic obstructive pulmonary disease exacerbations: A randomized controlled trial. Eur. Respir. J. 2017, 50, 1601448. [Google Scholar] [CrossRef]
- Ergan, B.; Nasiłowski, J.; Winck, J.C. How Should We Monitor Patients with Acute Respiratory Failure Treated with Noninvasive Ventilation? Eur. Respir. Rev. 2018, 27, 170101. [Google Scholar] [CrossRef]
- Monti, G.; Cabrini, L.; Kotani, Y.; Cabrini, S.; Bonatti, G.; Donati, A.; Zangrillo, A.; Cecconi, M.; Latronico, N.; Landoni, G.; et al. Early noninvasive ventilation in general wards for acute respiratory failure: An international, multicenter, open-label, randomized trial. Br. J. Anaesth. 2025, 134, 382–391. [Google Scholar] [CrossRef]
- Yu, J.; Lee, M.R.; Chen, C.T.; Lin, Y.T.; How, C.K. Predictors of Successful Weaning from Noninvasive Ventilation in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Single-Center Retrospective Cohort Study. Lung 2021, 199, 457–466. [Google Scholar] [CrossRef]
- Kheir, M.; Dong, V.; Roselli, V.; Mina, B. The role of ultrasound in predicting non-invasive ventilation outcomes: A systematic review. Front. Med. 2023, 31, 1233518. [Google Scholar] [CrossRef]
- Li, S.; Chen, Z.; Yan, W. Application of bedside ultrasound in predicting the outcome of weaning from mechanical ventilation in elderly patients. BMC Pulm. Med. 2021, 21, 217. [Google Scholar] [CrossRef]
- Schaeffer, B.Z.; Fazio, S.A.; Stocking, J.C.; Adams, J.Y.; Liu, A.; Black, H.B.; Harper, R.W.; Cortes-Puch, I.; Albertson, T.E.; Kuhn, B.T. Using the ROX Index to Predict Treatment Outcome for High-Flow Nasal Cannula and/or Noninvasive Ventilation in Patients with COPD Exacerbations. Respir. Care 2024, 69, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, A.; Lopez, A.; Carrillo, L.; Caldeira, V.; Guia, M.; Alonso, N.; Renedo, A.; Quintana, M.E.; Sanchez, J.M.; Esquinas, A. Validity of a clinical scale in predicting the failure of non-invasive ventilation in hypoxemic patients. J. Crit. Care 2020, 60, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Wang, S.; Liu, P.; Han, X.; Tian, Y.; Gao, F.; Zhou, J.; Mou, J.; Qin, Q.; Yu, J.; et al. Early prediction of noninvasive ventilation failure in COPD patients: Derivation, internal validation, and external validation of a simple risk score. Ann. Intensive Care 2019, 9, 108. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, S.; Gupta, N.; Adhikari, S.D.; Todur, P.; Maddani, S.S.; Rao, S. Utility of the One-time HACOR Score as a Predictor of Weaning Failure from Mechanical Ventilation: A Prospective Observational Study. Indian J. Crit. Care Med. 2022, 26, 900–905. [Google Scholar] [CrossRef]
- Ferreyro, B.L.; Dianti, J.; Munshi, L. Defining Failure of Noninvasive Ventilation for Acute Respiratory Distress Syndrome: Have We Succeeded? Ann. Am. Thorac. Soc. 2022, 19, 167–169. [Google Scholar] [CrossRef]
- Scala, R.; Pisani, L. Noninvasive ventilation in acute respiratory failure: Which recipe for success. Eur. Respir. Rev. 2018, 27, 180029. [Google Scholar] [CrossRef]
- Nishikimi, M.; Nishida, K.; Shindo, Y.; Taito, S.; Kashiwagi, K.; Otani, T.; Hagiwara, E.; Naito, H.; Takeda, R.; Nishimura, M.; et al. Failure of non-invasive respiratory support after 6 hours from initiation is associated with ICU mortality. PLoS ONE 2021, 16, e0251030. [Google Scholar] [CrossRef]
- Corrêa, T.D.; Sanches, P.R.; de Morais, L.C.; Silva, E.; Vieira, S.R.; Ornellas, D.S.; Silva, U.V.; Figueiredo, R.C.; Moreira, L.F.; Amaral, J.B.; et al. Performance of noninvasive ventilation in acute respiratory failure in critically ill patients: A prospective, observational, cohort study. BMC Pulm. Med. 2015, 15, 144. [Google Scholar] [CrossRef]
- Antonelli, M.; Conti, G.; Moro, M.L.; Esquinas, A.; Gonzalez-Diaz, G.; Confalonieri, M.; Pelaia, P.; Principi, T.; Gregoretti, C.; Beltrame, F.; et al. Predictors of failure of noninvasive positive pressure ventilation in patients with acute hypoxemic respiratory failure: A multi-center study. Intensive Care Med. 2001, 27, 1718–1728. [Google Scholar] [CrossRef]
- Mina, B.; Newton, A.; Hadda, V. Noninvasive Ventilation in Treatment of Respiratory Failure-Related COVID-19 Infection: Review of Literature. Can. Respir. J. 2022, 2022, 9914081. [Google Scholar] [CrossRef]
- Murad, A.; Li, P.Z.; Dial, S.; Shahin, J. The role of noninvasive positive pressure ventilation in community-acquired pneumonia. J. Crit. Care 2015, 30, 49–54. [Google Scholar] [CrossRef]
- Carron, M.; Freo, U.; Zorzi, M.; Ori, C. Predictors of failure of noninvasive ventilation in patients with severe community-acquired pneumonia. J. Crit. Care 2010, 540, e9–e14. [Google Scholar] [CrossRef] [PubMed]
- Leela-Amornsin, S.; Triganjananun, C.; Yuksen, C.; Jenpanitpong, C.; Watcharakitpaisan, S. Clinical Prediction Score for Successful Weaning from Noninvasive Positive Pressure Ventilation (NIPPV) in Emergency Department; a Retrospective Cohort Study. Arch. Acad. Emerg. Med. 2022, 10, e79. [Google Scholar] [CrossRef] [PubMed]
- Hund, E.F.; Fogel, W.; Krieger, D.; DeGeorgia, M.; Hacke, W. Critical illness polyneuropathy: Clinical findings and outcomes of a frequent cause of neuromuscular weaning failure. Crit. Care Med. 1996, 24, 1328–1333. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Frazer-Green, L.; Amin, R.; Wolfe, L.; Faulkner, G.; Casey, K.; Sharma, G.; Selim, B.; Zielinski, D.; Aboussouan, L.S.; et al. Respiratory Management of Patients with Neuromuscular Weakness: An American College of Chest Physicians Clinical Practice Guideline and Expert Panel Report. Chest 2023, 164, 394–413. [Google Scholar] [CrossRef]
- Burns, K.E.; Meade, M.O.; Premji, A.; Adhikari, N.K. Noninvasive ventilation as a weaning strategy for mechanical ventilation in adults with respiratory failure: A Cochrane systematic review. CMAJ 2014, 186, E112–E122. [Google Scholar] [CrossRef]
- Burns, K.E.A.; Stevenson, J.; Laird, M.; Adhikari, N.K.J.; Li, Y.; Lu, C.; He, X.; Wang, W.; Liang, Z.; Chen, L.; et al. Non-invasive ventilation versus invasive weaning in critically ill adults: A systematic review and meta-analysis. Thorax 2022, 77, 752–761. [Google Scholar] [CrossRef]
- Meeder, A.M.; Tijan, D.H.T.; van Zentan, A.R.H. Noninvasive and invasive positive pressure ventilation for acute respiratory failure in critically ill patients: A comparative cohort study. J. Thorac. Dis. 2016, 8, 813–825. [Google Scholar] [CrossRef]
- Vignon, P. Cardiopulmonary interactions during ventilator weaning. Front. Physiol. 2023, 14, 1275100. [Google Scholar] [CrossRef]
- Hryciw, B.N.; Hryciw, N.; Alexander, T.; Wong, J.; Zhang, M.; Gajic, O.; Kannan, S.; Chanques, G.; Jaber, S.; Dres, M.; et al. Predictors of noninvasive ventilation failure in the post-extubation period: A systematic review and meta-analysis. Crit. Care Med. 2023, 51, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Metkus, T.S.; Miller, P.E.; Stephen, R.S.; Kagiyama, N.; Doshi, A.; Sato, K.; Croft, L.B.; Kato, T.; Rali, A.S.; Venkateshvaran, A.; et al. Incidence, predictors, and outcomes of failure of noninvasive ventilation in acute heart failure hospitalization. Respir. Care 2020, 65, 1527–1533. [Google Scholar] [CrossRef]
- Zhang, Z.; Jun, D. Nosocomial pneumonia in non-invasive ventilation patients: Incidence characteristics outcomes. J. Hosp. Infect. 2015, 91, 153–157. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Indication | Recommendation for Use of NIV Based on ERS/ATS Guidelines | Strength of Recommendation |
|---|---|---|
| Moderate-to-severe COPD causing respiratory acidosis | Bilevel NIV for patients with ARF leading to acute or acute-on-chronic respiratory acidosis (pH ≤ 7.35) due to COPD exacerbation | Strong recommendation, high certainty of evidence |
| Trial of bilevel NIV in patients considered to require endotracheal intubation and mechanical ventilation, unless the patient is immediately deteriorating | Strong recommendation, moderate certainty of evidence Strongest recommendation is in patients with pH 7.25–7.35 | |
| ARF from acute cardiogenic pulmonary edema | Either bilevel NIV or CPAP for patients with ARF due to cardiogenic pulmonary edema | Strong recommendation, moderate certainty of evidence |
| ARF in immunocompromised patients | Early NIV for immunocompromised patients with ARF | Conditional recommendation, moderate certainty of evidence |
| Post-operative ARF | Use of NIV for patients with post-operative ARF | Conditional recommendation, moderate certainty of evidence |
| ARF from chest trauma | Use of NIV for chest trauma patients with ARF | Conditional recommendation, moderate certainty of evidence |
| ARF in palliative care | Offering NIV to dyspneic patients for palliation in the setting of terminal cancer or other terminal conditions | Conditional recommendation, moderate certainty of evidence |
| Aid in weaning from mechanical ventilation in hypercapnic patients | NIV can be used to facilitate weaning from mechanical ventilation in patients with hypercapnic respiratory failure | Conditional recommendation, moderate certainty of evidence |
| Prevention post-extubation respiratory failure | Non-high-risk patients: NIV should not be used to prevent post-extubation respiratory failure | Conditional recommendation, very low certainty of evidence |
| High-risk patients: NIV should not be used to prevent post-extubation respiratory failure | Conditional recommendation, low certainty of evidence | |
| Treatment of post-extubation respiratory failure | NIV should not be used in the treatment of patients with established post-extubation respiratory failure | Conditional recommendation, low certainty of evidence |
| ARF in acute asthma | Unable to offer a recommendation | |
| ARF in pandemic viral illness | Unable to offer a recommendation | |
| Aid in weaning from mechanical ventilation in hypoxic patients | Unable to offer a recommendation |
|
|
|
| Weaning Eligibility Criteria: Patients were considered for weaning when the following criteria were met during NIV:
|
| Initial Assessment: Once criteria were met:
|
Weaning Protocol:
|
Weaning Failure Criteria Were Defined As:
|
| PaO2/FiO2 ratio greater than 200 at one hour after NIV initiation |
| Respiratory rate < 20–22 breath/min without signs of distress |
| Tidal volumes less than 9 mL/kg of predicted body weight at one hour after initiation of NIV |
| pH > 7.33 |
| PaCO2 normalization to baseline |
| Glascow Coma Scale score of over 13 |
| Rapid Shallow Beathing Index (RSBI) threshold of less than 67.4 breaths/min/L |
| LUS scores less than 18 |
| Higher diaphragm thickness fraction (DTF) |
| ROX Index > 4.88 after 2 h |
| HACOR Score < 5 |
| Immediate failure (within minutes to <1 h): | Often due to secretion retention, hypercapnic encephalopathy, patient intolerance, agitation, or NIV asynchrony. |
| Early failure (1–48 h): | Typically caused by persistent gas exchange abnormalities, worsening acute illness, or unrelieved respiratory distress. |
| Late failure (>48 h) | Occurs after an initial improvement, often linked to sleep disruption and serious comorbidities. |
| Category | Risk Factor |
|---|---|
| Respiratory Parameters |
|
| Timing of Failure |
|
| Technical Issues |
|
| Patient Tolerance |
|
| Underlying Conditions |
|
| Hemodynamic Instability |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zimnoch, M.; Eldeiry, D.; Aruleba, O.; Schwartz, J.; Avaricio, M.; Ishikawa, O.; Mina, B.; Esquinas, A. Non-Invasive Ventilation: When, Where, How to Start, and How to Stop. J. Clin. Med. 2025, 14, 5033. https://doi.org/10.3390/jcm14145033
Zimnoch M, Eldeiry D, Aruleba O, Schwartz J, Avaricio M, Ishikawa O, Mina B, Esquinas A. Non-Invasive Ventilation: When, Where, How to Start, and How to Stop. Journal of Clinical Medicine. 2025; 14(14):5033. https://doi.org/10.3390/jcm14145033
Chicago/Turabian StyleZimnoch, Mary, David Eldeiry, Oluwabunmi Aruleba, Jacob Schwartz, Michael Avaricio, Oki Ishikawa, Bushra Mina, and Antonio Esquinas. 2025. "Non-Invasive Ventilation: When, Where, How to Start, and How to Stop" Journal of Clinical Medicine 14, no. 14: 5033. https://doi.org/10.3390/jcm14145033
APA StyleZimnoch, M., Eldeiry, D., Aruleba, O., Schwartz, J., Avaricio, M., Ishikawa, O., Mina, B., & Esquinas, A. (2025). Non-Invasive Ventilation: When, Where, How to Start, and How to Stop. Journal of Clinical Medicine, 14(14), 5033. https://doi.org/10.3390/jcm14145033