
Environmental Temperature, Other Climatic Variables, and Cardiometabolic Profile in Acute Myocardial Infarction

 ,
,  , , ,
, , , 

Abstract
1. Introduction
2. Materials and Methods
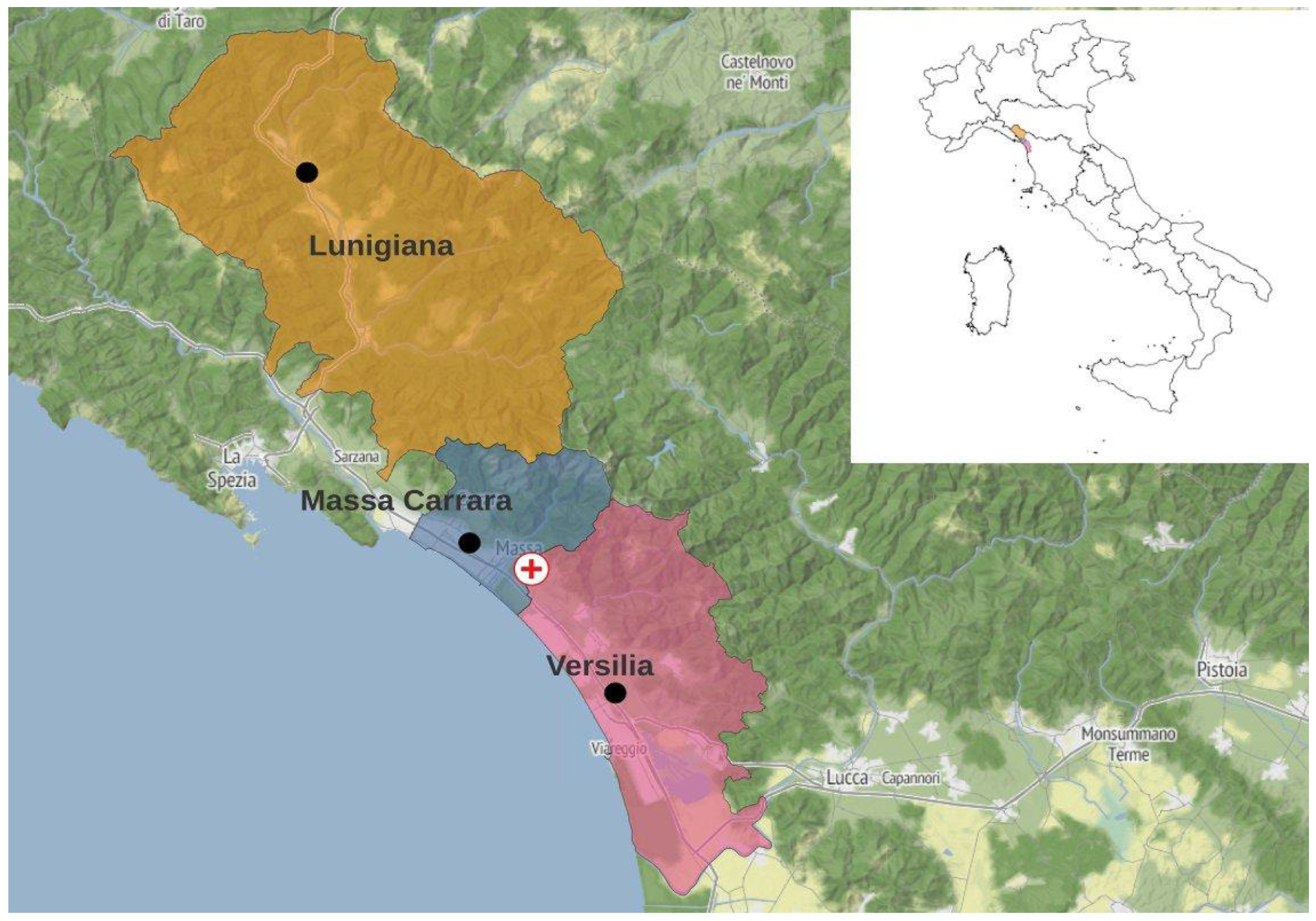
2.1. Geographical Characteristics
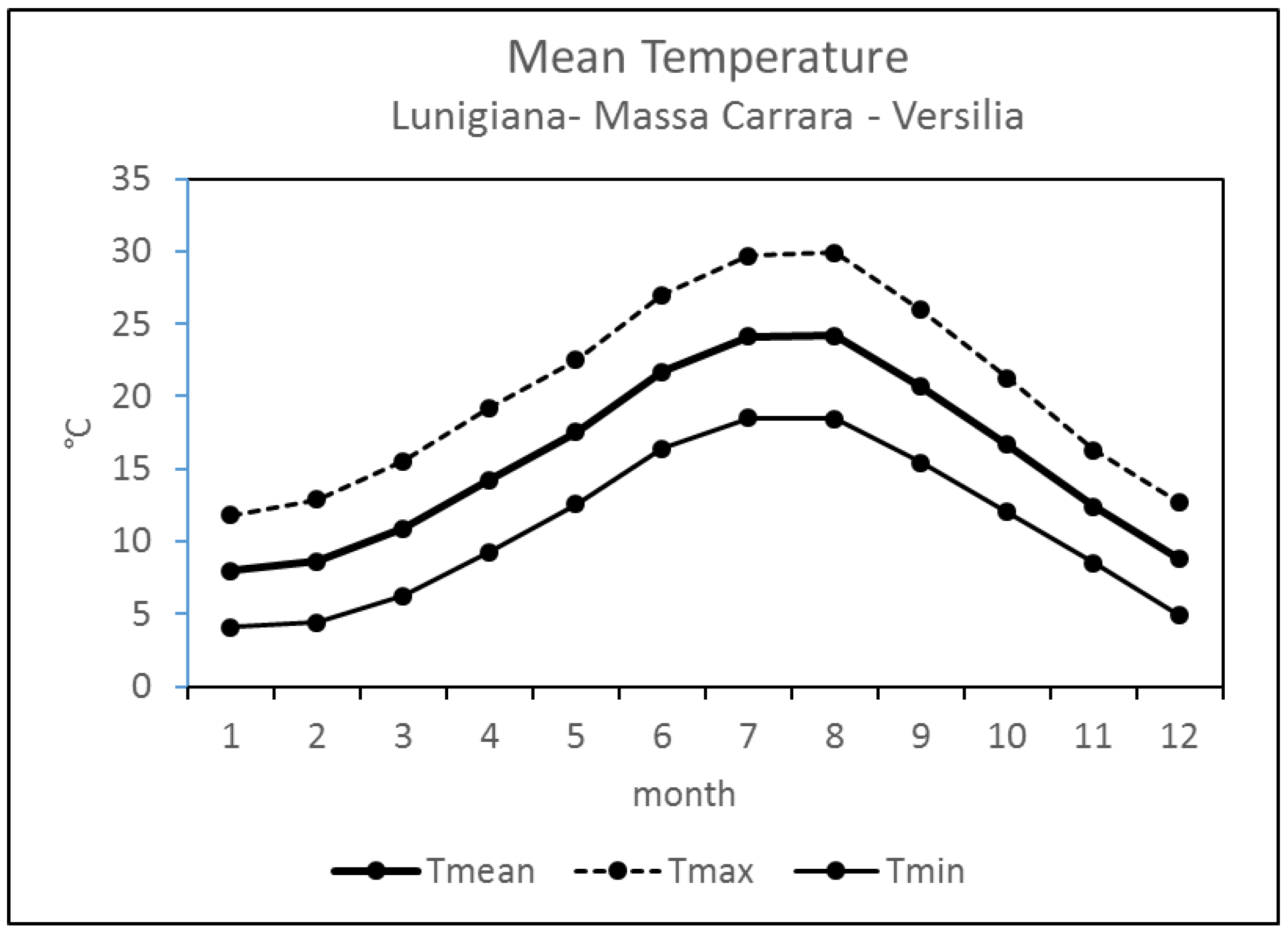
2.2. Meteorological Data
2.2.1. Approach 1—Classification of Annual Warm and Cold Periods
2.2.2. Approach 2—Classification of the Warm and Cold Extreme Days of the Two Periods
2.2.3. Approach 3—Classification of the Warm and Cold Extreme Days for Each Month of the Two Periods
2.3. Study Population Characteristics
2.4. Statistical Analysis
3. Results
3.1. Meteorological Variables
3.1.1. Approach 1—Classification of Annual Warm and Cold Periods
3.1.2. Approach 2—Calculation of 25° and 75° Percentiles for the Warm and Cold Periods (2007–2018)—Classification of the Warm and Cold Extreme Days of the Two Warm and Cold Periods
- -
- Days with meteorological parameters above the 75° percentile. For air temperature, days warmer (warm period) or less cold (cold period) than normal;
- -
- Days with meteorological parameters between the 75° and 25° percentile; days without extremes;
- -
- Days with meteorological parameters lower than the 25° percentile; days less warm (warm period) or colder (cold period) than normal. In Supplementary Tables S1–S6, the seasonal percentiles calculated for warm and cold periods are shown.
3.1.3. Approach 3—Calculation of 25° and 75° Percentiles for the Single Month of the Warm and Cold Period (2007–2018)—Classification of the Warm and Cold Extreme Days for Each Month of the Two Warm and Cold Periods
3.2. Impact of Meteorological Variables on STEMI Patient Characteristics
3.2.1. Characteristics of STEMI Patients in the Overall Population and after Stratification According to the Classification of Annual Warm (May–October) and Cold (November–April) Periods (Approach 1)
3.2.2. Characteristics of STEMI Patients Stratified According to the Warm and Cold Extreme Days of the Warm and Cold Periods (Approach 2)
Cold Period Extremes
Warm Period Extremes
3.2.3. Characteristics of STEMI Patients Stratified According to the Classification of the Warm and Cold Extreme Days for Each Month of the Two Warm and Cold Periods (Approach 3)
Monthly Extremes of the Cold Period
Monthly Extremes of the Warm Period
3.3. Characteristics of STEMI Patients Stratified According to the Heat Index (>32.4 °C)
3.4. Months with 7 Days or More with Light Circulation
3.5. Logistic Regression Analysis
4. Discussion
5. Study Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhaskaran, K.; Hajat, S.; Haines, A.; Herrett, E.; Wilkinson, P.; Smeeth, L. Effects of ambient temperature on the incidence of myocardial infarction. Heart 2009, 95, 1760–1769. [Google Scholar] [CrossRef] [PubMed]
- Wolf, K.; Schneider, A.; Breitner, S.; von Klot, S.; Meisinger, C.; Cyrys, J.; Hymer, H.; Wichmann, H.-E.; Peters, A. Air Temperature and the Occurrence of Myocardial Infarction in Augsburg, Germany. Circulation 2009, 120, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, J.; Freire, E.; Almendra, R.; Silva, G.L.; Santana, P. The impact of winter cold weather on acute myocardial infarctions in Portugal. Environ. Pollut. 2013, 183, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, Q.; Ge, Y.; Du, X.; Wang, H. Growing prevalence of heat over cold extremes with overall milder extremes and multiple successive events. Commun. Earth Environ. 2022, 3, 73. [Google Scholar] [CrossRef]
- Ebi, K.L.; Vanos, J.; Baldwin, J.W.; Bell, J.E.; Hondula, D.M.; Errett, N.A.; Hayes, K.; Reid, C.E.; Saha, S.; Spector, J.; et al. Extreme Weather and Climate Change: Population Health and Health System Implications. Annu. Rev. Public Health 2021, 42, 293–315. [Google Scholar] [CrossRef] [PubMed]
- Gebhard, C.; Gebhard, C.E.; Stähli, B.E.; Maafi, F.; Bertrand, M.J.; Wildi, K.; Fortier, A.; Galvan Onandia, Z.; Toma, A.; Zhang, Z.W.; et al. Weather and risk of ST-elevation myocardial infarction revisited: Impact on young women. PLoS ONE 2018, 13, e0195602. [Google Scholar] [CrossRef] [PubMed]
- Thornton, P.E.; Running, S.W.; White, M.A. Generating surfaces of daily meteorological variables over large regions of complex terrain. J. Hydrol. 1997, 190, 214–251. [Google Scholar] [CrossRef]
- Rothfusz, L.P. The Heat Index “Equation” (or, More Than you Ever Wanted to Know about Heat Index). NWS Southern Region Tech. Attachment SR-9023, 2p. 1990. Available online: https://www.weather.gov/media/ffc/ta_htindx.PDF (accessed on 1 April 2024).
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [PubMed]
- Harold, J. Hoxie, Seasonal incidence of coronary occlusion in a mild climate: A study based upon autopsy material. Am. Heart J. 1940, 19, 475–477. [Google Scholar]
- Heyer, H.E.; Teng, H.C.; Barris, W. The increased frequency of acute myocardial infarction during summer months in a warm climate; a study of 1386 cases from Dallas, Texas. Am. Heart J. 1953, 45, 741–748. [Google Scholar] [CrossRef]
- Chu, M.L.; Shih, C.Y.; Hsieh, T.C.; Chen, H.L.; Lee, C.W.; Hsieh, J.C. Acute Myocardial Infarction Hospitalizations between Cold and Hot Seasons in an Island across Tropical and Subtropical Climate Zones-A Population-Based Study. Int. J. Environ. Res. Public Health 2019, 16, 2769. [Google Scholar] [CrossRef] [PubMed]
- Claeys, M.J.; Coenen, S.; Colpaert, C.; Bilcke, J.; Beutels, P.; Wouters, K.; Legrand, V.; Van Damme, P.; Vrints, C. Environmental triggers of acute myocardial infarction: Results of a nationwide multiple-factorial population study. Acta Cardiol. 2015, 70, 693–701. [Google Scholar] [CrossRef]
- Ikäheimo, T.M. Cardiovascular diseases, cold exposure and exercise. Temperature 2018, 5, 123–146. [Google Scholar] [CrossRef]
- Liu, C.; Yavar, Z.; Sun, Q.; Klemcke, H.G.; Calderon, M.L.; Crimmins, S.L.; Ryan, K.L.; Xiang, L.; Hinojosa-Laborde, C.; Valtonen, R.I.P.; et al. Cardiovascular response to thermoregulatory challenges. Am. J. Physiol. Circ. Physiol. 2015, 309, H1793–H1812. [Google Scholar] [CrossRef]
- Price, R.H.M.; Graham, C.; Ramalingam, S. Association between viral seasonality and meteorological factors. Sci. Rep. 2019, 9, 929. [Google Scholar] [CrossRef] [PubMed]
- Rouzbahani, M.; Azimivghar, J.; Moghadam, R.H.; Montazeri, N.; Janjani, P.; Rai, A.; Rad, E.J.; Naderipour, A.; Salehi, N. Acute myocardial infarction: Circadian, daily, monthly and seasonal patterns of occurrence in diabetics. J. Diabetes Metab. Disord. 2021, 20, 765–770. [Google Scholar] [CrossRef]
- Tien, K.-J.; Yang, C.-Y.; Weng, S.-F.; Liu, S.-Y.; Hsieh, M.-C.; Chou, C.-W. The impact of ambient temperature on HbA1c in Taiwanese type 2 diabetic patients: The most vulnerable subgroup. J. Formos. Med. Assoc. 2015, 115, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhou, Y.; Williams, G.; Jaakkola, J.; Ou, C.; Chen, S.; Yao, T.; Qin, T.; Wu, S.; Guo, Y. Seasonality and temperature effects on fasting plasma glucose: A population-based longitudinal study in China. Diabetes Metab. 2016, 42, 267–275. [Google Scholar] [CrossRef]
- Goggins, W.B.; Chan, E.Y.; Yang, C.-Y. Weather, pollution, and acute myocardial infarction in Hong Kong and Taiwan. Int. J. Cardiol. 2013, 168, 243–249. [Google Scholar] [CrossRef]
- Ma, X.; Yan, H.; Zhang, H.; Wang, M.; Zhang, Q.; Zhou, X. Progress in the seasonal variations of blood lipids: A mini-review. Lipids Health Dis. 2020, 19, 108. [Google Scholar] [CrossRef]
- Zhou, X.; Lin, H.; Zhang, S.; Ren, J.; Wang, Z.; Zhang, Y.; Wang, M.; Zhang, Q. Effects of climatic factors on plasma lipid levels: A 5-year longitudinal study in a large Chinese population. J. Clin. Lipidol. 2016, 10, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Ockene, I.S.; Chiriboga, D.E.; Stanek, E.J., 3rd; Harmatz, M.G.; Nicolosi, R.; Saperia, G.; Well, A.D.; Freedson, P.; Merriam, P.A.; Reed, G.; et al. Seasonal variation in serum cholesterol levels: Treatment implications and possible mechanisms. Arch. Intern. Med. 2004, 164, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Donahoo, W.T.; Jensen, D.R.; Shepard, T.Y.; Eckel, R.H. Seasonal Variation in Lipoprotein Lipase and Plasma Lipids in Physically Active, Normal Weight Humans*. J. Clin. Endocrinol. Metab. 2000, 85, 3065–3068. [Google Scholar] [CrossRef] [PubMed]
- Skutecki, R.; Cymes, I.; Dragańska, E.; Glińska-Lewczuk, K.; Buciński, A.; Drozdowski, M.; Romaszko, J. Are the Levels of Lipid Parameters Associated with Biometeorological Conditions? Int. J. Environ. Res. Public Health 2019, 16, 4636. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Alavez, M.; Tabarean, I.V.; Osborn, O.; Mitsukawa, K.; Schaefer, J.; Dubins, J.; Holmberg, K.H.; Klein, I.; Klaus, J.; Gomez, L.F.; et al. Insulin Causes Hyperthermia by Direct Inhibition of Warm-Sensitive Neurons. Diabetes 2009, 59, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, S.; Maffei, S.; Prontera, C.; Battaglia, D.; Vassalle, C. Preanalytical, analytical (DiaSorin LIAISON) and clinical variables potentially affecting the 25-OH Vitamin D estimation. Clin. Biochem. 2012, 45, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Tucker, L.A. Serum, Dietary, and Supplemental Vitamin D Levels and Insulin Resistance in 6294 Randomly Selected, Non-Diabetic, U.S. Adults. Nutrients 2022, 14, 1844. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Ye, J.; Guo, G.; Lan, Z.; Li, X.; Pan, Z.; Rao, X.; Zheng, Z.; Luo, F.; Lin, L.; et al. Vitamin D Status Is Negatively Correlated with Insulin Resistance in Chinese Type 2 Diabetes. Int. J. Endocrinol. 2016, 2016, 1794894. [Google Scholar] [CrossRef]
- Szymczak-Pajor, I.; Śliwińska, A. Analysis of Association between Vitamin D Deficiency and Insulin Resistance. Nutrients 2019, 11, 794. [Google Scholar] [CrossRef]
- Krisnamurti, D.G.B.; Louis, M.; Poerwaningsih, E.H.; Tarigan, T.J.E.; Soetikno, V.; Wibowo, H.; Nugroho, C.M.H. Vitamin D supplementation alleviates insulin resistance in prediabetic rats by modifying IRS-1 and PPARγ/NF-κB expressions. Front. Endocrinol. 2023, 14, 1089298. [Google Scholar] [CrossRef]
- Surdu, A.M.; Pînzariu, O.; Ciobanu, D.-M.; Negru, A.-G.; Căinap, S.-S.; Lazea, C.; Iacob, D.; Săraci, G.; Tirinescu, D.; Borda, I.M.; et al. Vitamin D and Its Role in the Lipid Metabolism and the Development of Atherosclerosis. Biomedicines 2021, 9, 172. [Google Scholar] [CrossRef] [PubMed]
- Pingitore, A.; Mastorci, F.; Berti, S.; Sabatino, L.; Palmieri, C.; Iervasi, G.; Vassalle, C. Hypovitaminosis D and Low T3 Syndrome: A Link for Therapeutic Challenges in Patients with Acute Myocardial Infarction. J. Clin. Med. 2021, 10, 5267. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, C.; Hanisch, M.; Heinsohn, J.B.; Dostal, V.; Jehn, M.; Liebers, U.; Pankow, W.; Donaldson, G.C.; Witt, C. Increased vulnerability of COPD patient groups to urban climate in view of global warming. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 3493–3501. [Google Scholar] [CrossRef] [PubMed]
- Moliterno, D.J.; Willard, J.E.; Lange, R.A.; Negus, B.H.; Boehrer, J.D.; Glamann, D.B.; Landau, C.; Rossen, J.D.; Winniford, M.D.; Hillis, L.D. Coronary-Artery Vasoconstriction Induced by Cocaine, Cigarette Smoking, or Both. New Engl. J. Med. 1994, 330, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Modesti, P.A.; Cecchi, L.; Crisci, A.; Orlandini, S.; Maracchi, G.; Gensini, G.F. Relationships between weather and myocardial infarction: A biometeorological approach. Int. J. Cardiol. 2005, 105, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Fa-Binefa, M.; Clará, A.; Pérez-Fernández, S.; Grau, M.; Dégano, I.R.; Marti-Lluch, R.; Ramos, R.; Marrugat, J.; Elosua, R. Early smoking-onset age and risk of cardiovascular disease and mortality. Prev. Med. 2019, 124, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Rosengren, A.; Hawken, S.; Ôunpuu, S.; Sliwa, K.; Zubaid, M.; A Almahmeed, W.; Blackett, K.N.; Sitthi-Amorn, C.; Sato, H.; Yusuf, S. Association of psychosocial risk factors with risk of acute myocardial infarction in 11,119 cases and 13,648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 953–962. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Menezes, A.R.; De Schutter, A.; Milani, R.V.; Blumenthal, J.A. Impact of Cardiac Rehabilitation and Exercise Training on Psychological Risk Factors and Subsequent Prognosis in Patients with Cardiovascular Disease. Can. J. Cardiol. 2016, 32 (Suppl. 2), S365–S373. [Google Scholar] [CrossRef] [PubMed]
- Klug, G.; Schenk, S.; Dörler, J.; Mayr, A.; Haubner, B.J.; Alber, H.; Schächinger, V.; Pachinger, O.; Metzler, B. Occur-rence of acute myocardial infarction in winter tourists: Data from a retrospective questionnaire. Clin Res Cardiol. 2011, 100, 669–674. [Google Scholar] [CrossRef]
- Mittleman, M.A.; Maclure, M.; Tofler, G.H.; Sherwood, J.B.; Goldberg, R.J.; Muller, J.E. Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. Determinants of Myocardial Infarction Onset Study Investigators. N. Engl. J. Med. 1993, 329, 1677–1683. [Google Scholar] [CrossRef]
- Zeng, Y.; Gu, D.; Purser, J.; Hoenig, H.; Christakis, N. Associations of Environmental Factors with Elderly Health and Mortality in China. Am. J. Public Health 2010, 100, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Rocklöv, J.; Forsberg, B.; Ebi, K.; Bellander, T. Susceptibility to mortality related to temperature and heat and cold wave duration in the population of Stockholm County, Sweden. Glob. Health Action 2014, 7, 22737. [Google Scholar] [CrossRef]
- Davidkovova, H.; Plavcova, E.; Kyncl, J.; Kysely, J. Impacts of hot and cold spells differ for acute and chronic ischaemic heart diseases. BMC Public Health 2014, 14, 480. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Soim, A.; Gleason, K.A.; Hwang, S.A. Association Between Low Temperature During Winter Season and Hospitalizations for Ischemic Heart Diseases in New York State. J. Environ. Health 2016, 78, 66–74. [Google Scholar]
- Liu, X.; Kong, D.; Fu, J.; Zhang, Y.; Liu, Y.; Zhao, Y.; Lian, H.; Zhao, X.; Yang, J.; Fan, Z. Association between extreme temperature and acute myocardial infarction hospital admissions in Beijing, China: 2013–2016. PLoS ONE 2018, 13, e0204706. [Google Scholar] [CrossRef] [PubMed]
- Kienbacher, C.L.; Kaltenberger, R.; Schreiber, W.; Tscherny, K.; Fuhrmann, V.; Roth, D.; Herkner, H. Extreme weather conditions as a gender-specific risk factor for acute myocardial infarction. Am. J. Emerg. Med. 2021, 43, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Su, H.; Xu, Z.; Tong, S. Extreme temperature exposure and acute myocardial infarction: Elevated risk within hours? Environ. Res. 2021, 202, 111691. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Wang, J.; Li, Q.; Yagouti, A.; Lavigne, E.; Foty, R.; Burnett, R.T.; Villeneuve, P.J.; Cakmak, S.; Copes, R. Assessment of the effect of cold and hot temperatures on mortality in Ontario, Canada: A population-based study. CMAJ Open 2016, 4, E48–E58. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Yamada, K.P.; Kariya, T.; Aikawa, T.; Ishikawa, K. Effects of Therapeutic Hypothermia on Normal and Ischemic Heart. Front. Cardiovasc. Med. 2021, 8, 642843. [Google Scholar] [CrossRef]
- Hausenloy, D.J.; Yellon, D.M. Preconditioning and postconditioning: New strategies for cardioprotection. Diabetes Obes. Metab. 2007, 10, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Nia, H.S.; Chan, Y.H.; Froelicher, E.S.; Sharif, S.P.; Yaghoobzadeh, A.; Jafari, A.; Goudarzian, A.H.; Pourkia, R.; Haghdoost, A.A.; Arefinia, F.; et al. Weather fluctuations: Predictive factors in the prevalence of acute coronary syndrome. Health Promot. Perspect. 2019, 9, 123–130. [Google Scholar] [CrossRef]
- Ravljen, M.; Bilban, M.; Kajfež-Bogataj, L.; Hovelja, T.; Vavpotič, D. Influence of daily individual meteorological parameters on the incidence of acute coronary syndrome. Int. J. Environ. Res. Public Health 2014, 11, 11616–11626. [Google Scholar] [CrossRef]
- Abrignani, M.G.; Lombardo, A.; Braschi, A.; Renda, N.; Abrignani, V. Climatic influences on cardiovascular diseases. World J. Cardiol. 2022, 14, 152–169. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Warm Period | |||||
|---|---|---|---|---|---|
| Tmax | Tmean | RH | Wind | Mslp | |
| Tmin | 0.85 | 0.95 | −0.56 | −0.15 | −0.05 |
| Tmax | 0.97 | −0.52 | −0.04 | −0.05 | |
| Tmean | −0.56 | −0.09 | −0.05 | ||
| RH | 0.16 | −0.24 | |||
| Wind | −0.55 | ||||
| Cold period | |||||
| Tmax | Tmean | RH | Wind | Mslp | |
| Tmin | 0.86 | 0.96 | 0.06 | −0.21 | −0.10 |
| Tmax | 0.97 | −0.30 | −0.08 | −0.03 | |
| Tmean | −0.20 | −0.14 | −0.07 | ||
| RH | −0.03 | −0.09 | |||
| Wind | −0.38 | ||||
| Parameters | Overall Population (n = 2478) | Warm Period (May/October) (n = 1312) | Cold Period (November/April) (n = 1166) | p Value |
|---|---|---|---|---|
| Age (years) | 67 ∓ 13 | 67 ∓ 13 | 68 ∓ 13 | ≤0.05 |
| Age (>77 yrs–75th percentile) | 616 (25) | 312 (24) | 304 (26) | ns |
| Age (<50 yrs–10th percentile) | 227 (9) | 126 (10) | 101 (9) | ns |
| Males | 1779 (72) | 937 (71) | 842 (72) | ns |
| Diabetes | 515 (21) | 248 (19) | 267 (23) | ≤0.01 |
| Hypertension | 1418 (57) | 738 (56) | 680 (58) | ns |
| Dyslipidemia | 740 (30) | 371 (28) | 369 (31) | ≤0.01 |
| Current smokers | 981 (40) | 544 (41) | 437 (37) | ns |
| Creatinine (mg/dL, at admission) | 1.2 ∓ 0.8 | 1.2 ∓ 0.8 | 1.2 ∓ 0.7 | ns |
| CAD familiarity | 628 (25) | 341 (26) | 287 (25) | ns |
| Previous MI, PCI/CABG | 337 (14) | 171 (13) | 166 (14) | ns |
| Left ventricular ejection fraction-LVEF (at admission) (%) | 44 ∓ 10 | 44 ∓ 10 | 43 ∓ 10 | ns |
| LVEF < 40% | 312 (13) | 154 (12) | 158 (13) | ns |
| Periprocedural cardiovascular complications | 60 (2.4) | 23 (1.7) | 37 (3.2) | <0.05 |
| In-hospital mortality | 89 (3.6) | 39 (3.0) | 50 (4.3) | 0.08 |
| Approach 1—November/April vs. May/October | |
|---|---|
| Parameters | OR (95% CI) p |
| Age (one year) | 1.006 (1–1.01) ≤ 0.05 |
| Type 2 diabetes | 1.28 (1.1–1.6) ≤ 0.01 |
| Dyslipidemia | 1.27 (1.1–1.5) ≤ 0.01 |
| Periprocedural complications | 1.8 (1.1–3.1) < 0.05 |
| Approach 2—Period Extremes (November/April vs. May/October) | |||
|---|---|---|---|
| Parameters | Coldest Extremes of the Cold Period (Tmin < 25th Percentile and/or Tmax < 25th Percentile) | Warmer Extremes of the Cold Period (≥ 7 days Tmin > 75th Percentile and/or Tmax > 75th Percentile) | Warmest Extremes of the Warm Period (≥7 days Tmax > 75th Percentile) |
| OR (95% CI) p | |||
| Type 2 diabetes | 1.3 (1.1–1.6) < 0.05 | - | - |
| Dyslipidemia | 1.6 (1.3–1.6) < 0.001 | 0.7 (0.5–0.9) < 0.01 | - |
| Smokers | - | - | 1.2 (1–1.5) ≤ 0.05 |
| Periprocedural complications | 2.0 (1.2–3.4) < 0.01 | - | - |
| In-hospital mortality | 1.7 (1.1–2.7) < 0.05 | - | - |
| Approach 3—Monthly Extremes | ||||
|---|---|---|---|---|
| Parameters | Coldest Extremes of the Cold Period (Tmin < 25th Percentile and/or Tmax < 25th Percentile) | Warmer Extremes of the Cold Period (≥7 Days Tmin > 75th Percentile and/or Tmax > 75th Percentile) | Warmest Extremes of the Warm Period (≥7 Days Tmax > 75th Percentile) | Coldest Extremes of the Warm Period (≥7 Days Tmin < 25th Percentile) |
| OR (95% CI) p | ||||
| Age (one year) | 1.008 (1.001–1.002) p < 0.05 | 0.98 (0.98–0.99) < 0.001 | ||
| Type 2 diabetes | 1.3 (1.1–1.6) ≤ 0.01 | - | - | 0.7 (0.6–1) < 0.05 |
| Dyslipidemia | 1.4 (1.2–1.7) < 0.001 | 0.7 (0.5–1) < 0.05 | - | 0.7 (0.5–0.9) < 0.01 |
| Smokers | - | - | 1.2 (1–1.5) ≤ 0.01 | |
| Periprocedural complications | - | - | - | |
| In-hospital mortality | 1.6 (1.1–2.5) < 0.05 | - | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassalle, C.; Grifoni, D.; Gozzini, B.; Parlanti, A.; Fibbi, L.; Marchi, F.; Messeri, G.; Pylypiv, N.; Messeri, A.; Paradossi, U.; et al. Environmental Temperature, Other Climatic Variables, and Cardiometabolic Profile in Acute Myocardial Infarction. J. Clin. Med. 2024, 13, 2098. https://doi.org/10.3390/jcm13072098
Vassalle C, Grifoni D, Gozzini B, Parlanti A, Fibbi L, Marchi F, Messeri G, Pylypiv N, Messeri A, Paradossi U, et al. Environmental Temperature, Other Climatic Variables, and Cardiometabolic Profile in Acute Myocardial Infarction. Journal of Clinical Medicine. 2024; 13(7):2098. https://doi.org/10.3390/jcm13072098
Chicago/Turabian StyleVassalle, Cristina, Daniele Grifoni, Bernardo Gozzini, Alessandra Parlanti, Luca Fibbi, Federica Marchi, Gianni Messeri, Nataliya Pylypiv, Alessandro Messeri, Umberto Paradossi, and et al. 2024. "Environmental Temperature, Other Climatic Variables, and Cardiometabolic Profile in Acute Myocardial Infarction" Journal of Clinical Medicine 13, no. 7: 2098. https://doi.org/10.3390/jcm13072098
APA StyleVassalle, C., Grifoni, D., Gozzini, B., Parlanti, A., Fibbi, L., Marchi, F., Messeri, G., Pylypiv, N., Messeri, A., Paradossi, U., & Berti, S. (2024). Environmental Temperature, Other Climatic Variables, and Cardiometabolic Profile in Acute Myocardial Infarction. Journal of Clinical Medicine, 13(7), 2098. https://doi.org/10.3390/jcm13072098