
Frailty and In-Hospital Outcomes for Management of Cardiogenic Shock without Acute Myocardial Infarction

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
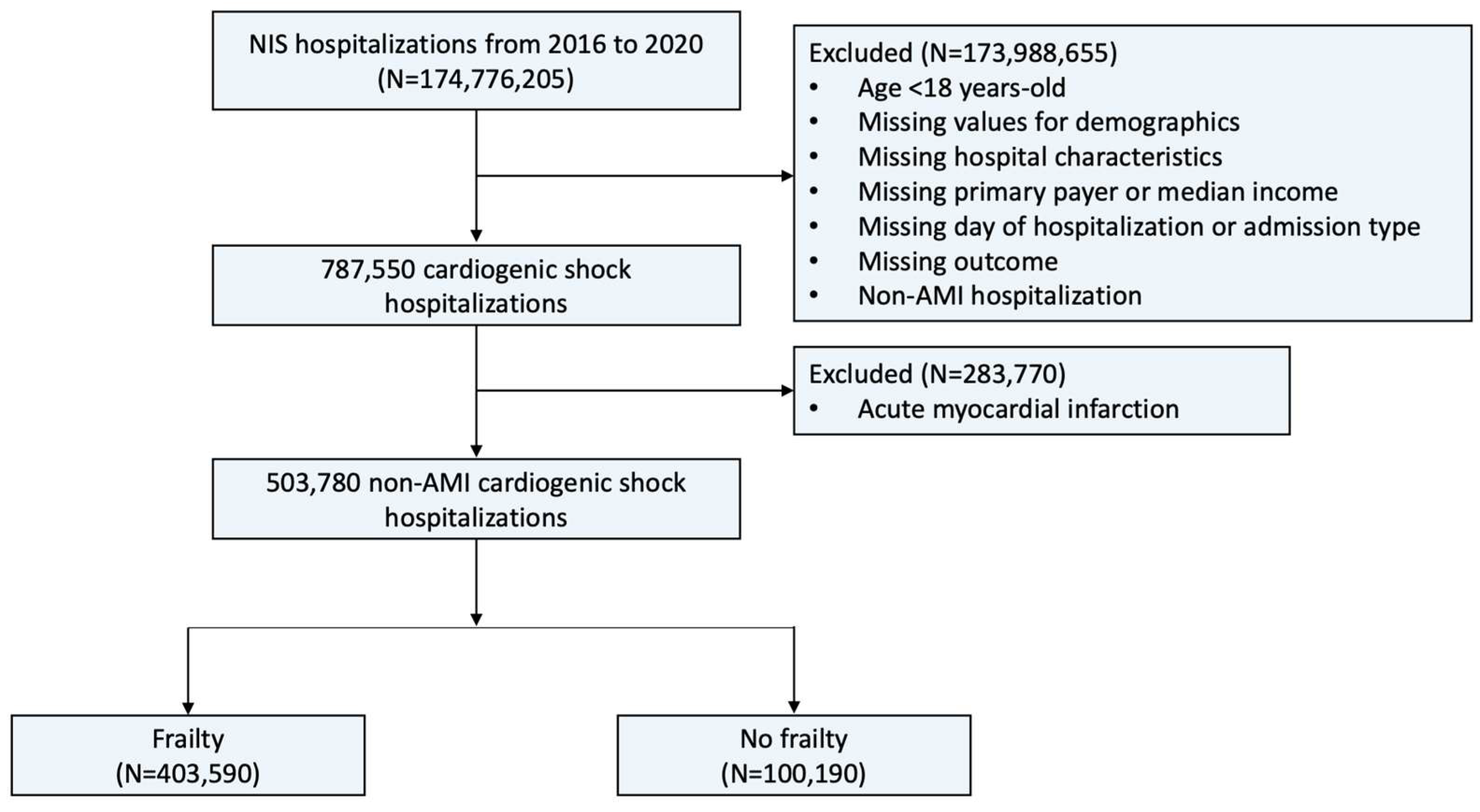
2.1. Data Source
2.2. Study Population and Covariates
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results

{kind=link}
{kind=link}
| Frailty (+) | Frailty (−) | p-Value | |
|---|---|---|---|
| Number of admissions | 403,590 | 100,190 | |
| Male sex (%) | 61.1 | 63.3 | <0.001 |
| Age, mean (Q1–Q3), years | 68 (57–77) | 65 (54–73) | <0.001 |
| Race (%) | <0.001 | ||
| White | 64.9 | 67.1 | |
| Black | 19.8 | 17.7 | |
| Hispanic | 8.7 | 8.6 | |
| Asian | 3.0 | 3.0 | |
| AI/AN | 0.6 | 0.7 | |
| Other | 3.0 | 3.0 | |
| Comorbidities (%) | |||
| Smoking | 33.3 | 33.6 | 0.442 |
| Hypertension | 11.8 | 20.2 | <0.001 |
| Diabetes mellitus | 38.6 | 34.5 | <0.001 |
| Hyperlipidemia | 39.2 | 45.2 | <0.001 |
| Obesity | 18.2 | 18.1 | 0.761 |
| Heart failure | 71.7 | 63.2 | <0.001 |
| Chronic ischemic heart disease | 17.5 | 15.6 | <0.001 |
| Atrial fibrillation | 45.1 | 38.5 | <0.001 |
| Valvular heart disease | 13.0 | 15.4 | <0.001 |
| Peripheral artery disease | 6.9 | 6.1 | <0.001 |
| Previous PCI | 0.9 | 1.3 | <0.001 |
| Previous CABG | 7.9 | 8.9 | <0.001 |
| Previous stroke | 10.0 | 7.3 | <0.001 |
| Previous pacemaker | 3.5 | 3.8 | 0.087 |
| COPD | 24.9 | 20.1 | <0.001 |
| Pulmonary hypertension | 20.8 | 19.6 | <0.001 |
| Chronic kidney disease | 47.7 | 22.5 | <0.001 |
| End-stage renal disease | 9.8 | 4.0 | <0.001 |
| Liver cirrhosis | 8.0 | 5.9 | <0.001 |
| History of malignancy | 7.3 | 8.1 | <0.001 |
| Deficiency anemia | 7.4 | 5.9 | <0.001 |
| Malnutrition | 17.3 | 8.8 | <0.001 |
| Dementia | 6.6 | 0.9 | <0.001 |
| Major depression | 0.9 | 0.8 | 0.173 |
| HFRS, median (Q1-Q3) | 8.8 (7.0–11.3) | 3.4 (2.2–4.2) | <0.001 |
| Hospital characteristics (%) | |||
| Hospital region | <0.001 | ||
| Northwest | 16.5 | 19.8 | |
| Midwest | 22.8 | 19.5 | |
| South | 40.1 | 41.5 | |
| West | 20.7 | 19.2 | |
| Hospital bed size | <0.001 | ||
| Small | 12.9 | 11.9 | |
| Medium | 23.6 | 22.2 | |
| Large | 63.5 | 65.9 | |
| Urban location | <0.001 | ||
| Rural | 3.5 | 3.7 | |
| Urban non-teaching | 14.5 | 13.4 | |
| Urban teaching | 82.0 | 82.9 | |
| Primary payer (%) | <0.001 | ||
| Medicare | 63.5 | 53.6 | |
| Medicaid | 13.1 | 14.1 | |
| Private insurance | 17.9 | 25.5 | |
| Self-pay | 2.9 | 3.5 | |
| No charge | 0.2 | 0.3 | |
| Others | 2.6 | 3.1 | |
| Median income (%) | 0.002 | ||
| Quartile 1 | 31.5 | 30.2 | |
| Quartile 2 | 26.1 | 26.9 | |
| Quartile 3 | 23.2 | 23.4 | |
| Quartile 4 | 19.1 | 19.5 | |
| Day of admission (%) | <0.001 | ||
| Weekday | 77.2 | 81.9 | |
| Weekend | 22.8 | 18.1 | |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walsh, B.; Fogg, C.; Harris, S.; Roderick, P.; de Lusignan, S.; England, T.; Clegg, A.; Brailsford, S.; Fraser, S.D. Frailty transitions and prevalence in an ageing population: Longitudinal analysis of primary care data from an open cohort of adults aged 50 and over in England, 2006–2017. Age Ageing 2023, 52, afad058. [Google Scholar] [CrossRef] [PubMed]
- Ijaz, N.; Buta, B.; Xue, Q.-L.; Mohess, D.T.; Bushan, A.; Tran, H.; Batchelor, W.; deFilippi, C.R.; Walston, J.D.; Bandeen-Roche, K.; et al. Interventions for Frailty Among Older Adults With Cardiovascular Disease. J. Am. Coll. Cardiol. 2022, 79, 482–503. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, N.; Marcantonio, E.R.; Inouye, S.K.; Gill, T.M.; Kamholz, B.; Rudolph, J.L. Vulnerability: The crossroads of frailty and delirium. J. Am. Geriatr. Soc. 2011, 59 (Suppl. S2), S262–S268. [Google Scholar] [CrossRef] [PubMed]
- Damluji, A.A.; Chung, S.-E.; Xue, Q.-L.; Hasan, R.K.; Moscucci, M.; Forman, D.E.; Bandeen-Roche, K.; Batchelor, W.; Walston, J.D.; Resar, J.R.; et al. Frailty and cardiovascular outcomes in the National Health and Aging Trends Study. Eur. Heart J. 2021, 42, 3856–3865. [Google Scholar] [CrossRef] [PubMed]
- Damluji, A.A.; Cohen, M.G. The Influence of Frailty on Cardiovascular Disease: The Time for a “Frailty Academic Research Consortium” Is Now! Circ. Cardiovasc. Interv. 2022, 15, e011669. [Google Scholar] [CrossRef] [PubMed]
- Vahdatpour, C.; Collins, D.; Goldberg, S. Cardiogenic Shock. J. Am. Heart Assoc. 2019, 8, e011991. [Google Scholar] [CrossRef] [PubMed]
- Damluji, A.A.; Alfaraidhy, M.; AlHajri, N.; Rohant, N.N.; Kumar, M.; Al Malouf, C.; Bahrainy, S.; Ji Kwak, M.; Batchelor, W.B.; Forman, D.E.; et al. Sarcopenia and Cardiovascular Diseases. Circulation 2023, 147, 1534–1553. [Google Scholar] [CrossRef] [PubMed]
- Papolos, A.I.; Kenigsberg, B.B.; Berg, D.D.; Alviar, C.L.; Bohula, E.; Burke, J.A.; Carnicelli, A.P.; Chaudhry, S.-P.; Drakos, S.; Gerber, D.A.; et al. Management and Outcomes of Cardiogenic Shock in Cardiac ICUs With Versus Without Shock Teams. J. Am. Coll. Cardiol. 2021, 78, 1309–1317. [Google Scholar] [CrossRef]
- Berg, D.D.; Bohula, E.A.; Morrow, D.A. Epidemiology and causes of cardiogenic shock. Curr. Opin. Crit. Care 2021, 27, 401–408. [Google Scholar] [CrossRef]
- Berg, D.D.; Bohula, E.A.; Diepen, S.v.; Katz, J.N.; Alviar, C.L.; Baird-Zars, V.M.; Barnett, C.F.; Barsness, G.W.; Burke, J.A.; Cremer, P.C.; et al. Epidemiology of Shock in Contemporary Cardiac Intensive Care Units. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005618. [Google Scholar] [CrossRef]
- Thiele, H.; Ohman, E.M.; Desch, S.; Eitel, I.; de Waha, S. Management of cardiogenic shock. Eur. Heart J. 2015, 36, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.M.; Gale, C.P.; Lip, G.; Martin-Sanchez, F.J.; McIntyre, H.F.; Mueller, C.; Price, S.; Sanchis, J.; Vidan, M.T.; Wilkinson, C.; et al. Editor’s Choice—Frailty and the management of patients with acute cardiovascular disease: A position paper from the Acute Cardiovascular Care Association. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 176–193. [Google Scholar] [CrossRef] [PubMed]
- HCUP Databases. Healthcare Cost and Utilization Project (HCUP). 2022. Available online: https://www.hcup-us.ahrq.gov/nisoverview.jsp (accessed on 28 November 2022).
- Damluji, A.A.; Bandeen-Roche, K.; Berkower, C.; Boyd, C.M.; Al-Damluji, M.S.; Cohen, M.G.; Forman, D.E.; Chaudhary, R.; Gerstenblith, G.; Walston, J.D.; et al. Percutaneous Coronary Intervention in Older Patients With ST-Segment Elevation Myocardial Infarction and Cardiogenic Shock. J. Am. Coll. Cardiol. 2019, 73, 1890–1900. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, T.; Neuburger, J.; Kraindler, J.; Keeble, E.; Smith, P.; Ariti, C.; Arora, S.; Street, A.; Parker, S.; Roberts, H.C.; et al. Development and validation of a Hospital Frailty Risk Score focusing on older people in acute care settings using electronic hospital records: An observational study. Lancet 2018, 391, 1775–1782. [Google Scholar] [CrossRef]
- McAlister, F.A.; Savu, A.; Ezekowitz, J.A.; Armstrong, P.W.; Kaul, P. The hospital frailty risk score in patients with heart failure is strongly associated with outcomes but less so with pharmacotherapy. J. Intern. Med. 2020, 287, 322–332. [Google Scholar] [CrossRef]
- Orlandi, M.; Dover, D.C.; Sandhu, R.K.; Hawkins, N.M.; Kaul, P.; McAlister, F.A. The Introduction of Direct Oral Anticoagulants Has Not Resolved Treatment Gaps for Frail Patients With Nonvalvular Atrial Fibrillation. Can. J. Cardiol. 2022, 38, 77–84. [Google Scholar] [CrossRef]
- Rottler, M.; Ocskay, K.; Sipos, Z.; Görbe, A.; Virág, M.; Hegyi, P.; Molnár, T.; Erőss, B.; Leiner, T.; Molnár, Z. Clinical Frailty Scale (CFS) indicated frailty is associated with increased in-hospital and 30-day mortality in COVID-19 patients: A systematic review and meta-analysis. Ann. Intensive Care 2022, 12, 17. [Google Scholar] [CrossRef]
- Eckart, A.; Hauser, S.I.; Haubitz, S.; Struja, T.; Kutz, A.; Koch, D.; Neeser, O.; Meier, M.A.; Mueller, B.; Schuetz, P. Validation of the hospital frailty risk score in a tertiary care hospital in Switzerland: Results of a prospective, observational study. BMJ Open 2019, 9, e026923. [Google Scholar] [CrossRef] [PubMed]
- Cost-to-Charge Ratio for Inpatient Files. Healthcare Cost and Utilization Project (HCUP). 2022. Available online: https://www.hcup-us.ahrq.gov/db/ccr/ip-ccr/ip-ccr.jsp (accessed on 28 November 2022).
- Ekerstad, N.; Javadzadeh, D.; Alexander, K.P.; Bergström, O.; Eurenius, L.; Fredrikson, M.; Gudnadottir, G.; Held, C.; Ängerud, K.H.; Jahjah, R.; et al. Clinical Frailty Scale classes are independently associated with 6-month mortality for patients after acute myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2022, 11, 89–98. [Google Scholar] [CrossRef]
- Volle, K.; Delmas, C.; Ferrières, J.; Toulza, O.; Blanco, S.; Lairez, O.; Lhermusier, T.; Biendel, C.; Galinier, M.; Carrié, D.; et al. Prevalence and Prognosis Impact of Frailty Among Older Adults in Cardiac Intensive Care Units. CJC Open 2021, 3, 1010–1018. [Google Scholar] [CrossRef]
- Jain, R.; Duval, S.; Adabag, S. How Accurate Is the Eyeball Test? Circ. Cardiovasc. Qual. Outcomes 2014, 7, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Howlett, S.E.; MacKnight, C.; Beattie, B.L.; Bergman, H.; Hébert, R.; Hogan, D.B.; Wolfson, C.; McDowell, I. Prevalence, attributes, and outcomes of fitness and frailty in community-dwelling older adults: Report from the Canadian study of health and aging. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- Hongisto, M.; Lassus, J.; Tarvasmäki, T.; Sionis, A.; Sans-Rosello, J.; Tolppanen, H.; Kataja, A.; Jäntti, T.; Sabell, T.; Lindholm, M.G.; et al. Mortality risk prediction in elderly patients with cardiogenic shock: Results from the CardShock study. ESC Heart Fail 2021, 8, 1398–1407. [Google Scholar] [CrossRef] [PubMed]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Lopez Samaniego, L.; Rodríguez-Mañas, L.; Bernabei, R.; Onder, G. Frailty and Multimorbidity: A Systematic Review and Meta-analysis. J. Gerontol. Ser. A 2018, 74, 659–666. [Google Scholar] [CrossRef]
- Afilalo, J.; Lauck, S.; Kim, D.H.; Lefèvre, T.; Piazza, N.; Lachapelle, K.; Martucci, G.; Lamy, A.; Labinaz, M.; Peterson, M.D.; et al. Frailty in Older Adults Undergoing Aortic Valve Replacement. J. Am. Coll. Cardiol. 2017, 70, 689–700. [Google Scholar] [CrossRef]
- Lujic, S.; Randall, D.A.; Simpson, J.M.; Falster, M.O.; Jorm, L.R. Interaction effects of multimorbidity and frailty on adverse health outcomes in elderly hospitalised patients. Sci. Rep. 2022, 12, 14139. [Google Scholar] [CrossRef]
- Docherty, N.G.; Delles, C.; D’Haese, P.; Layton, A.T.; Martínez-Salgado, C.; Vervaet, B.A.; López-Hernández, F.J. Haemodynamic frailty—A risk factor for acute kidney injury in the elderly. Ageing Res. Rev. 2021, 70, 101408. [Google Scholar] [CrossRef] [PubMed]
- Debain, A.; Loosveldt, F.A.; Knoop, V.; Costenoble, A.; Lieten, S.; Petrovic, M.; Bautmans, I. Frail older adults are more likely to have autonomic dysfunction: A systematic review and meta-analysis. Ageing Res. Rev. 2023, 87, 101925. [Google Scholar] [CrossRef] [PubMed]
- Sanchis, J.; Bueno, H.; Miñana, G.; Guerrero, C.; Martí, D.; Martínez-Sellés, M.; Domínguez-Pérez, L.; Díez-Villanueva, P.; Barrabés, J.A.; Marín, F.; et al. Effect of Routine Invasive vs Conservative Strategy in Older Adults With Frailty and Non-ST-Segment Elevation Acute Myocardial Infarction: A Randomized Clinical Trial. JAMA Intern. Med. 2023, 183, 407–415. [Google Scholar] [CrossRef]
- Dodson, J.A.; Hochman, J.S.; Roe, M.T.; Chen, A.Y.; Chaudhry, S.I.; Katz, S.; Zhong, H.; Radford, M.J.; Udell, J.A.; Bagai, A.; et al. The Association of Frailty With In-Hospital Bleeding Among Older Adults With Acute Myocardial Infarction. JACC Cardiovasc. Interv. 2018, 11, 2287–2296. [Google Scholar] [CrossRef]
- Boyer, S.; Trimouillas, J.; Cardinaud, N.; Gayot, C.; Laubarie-Mouret, C.; Dumoitier, N.; Rudelle, K.; Druet-Cabanac, M.; Laroche, M.-L.; Tchalla, A. Frailty and functional dependence in older population: Lessons from the FREEDOM Limousin—Nouvelle Aquitaine Cohort Study. BMC Geriatr. 2022, 22, 128. [Google Scholar] [CrossRef] [PubMed]
- Noriega, F.J.; Vidán, M.T.; Sánchez, E.; Díaz, A.; Serra-Rexach, J.A.; Fernández-Avilés, F.; Bueno, H. Incidence and impact of delirium on clinical and functional outcomes in older patients hospitalized for acute cardiac diseases. Am. Heart J. 2015, 170, 938–944. [Google Scholar] [CrossRef] [PubMed]
- Pauley, E.; Lishmanov, A.; Schumann, S.; Gala, G.J.; van Diepen, S.; Katz, J.N. Delirium is a robust predictor of morbidity and mortality among critically ill patients treated in the cardiac intensive care unit. Am. Heart J. 2015, 170, 79–86.e1. [Google Scholar] [CrossRef] [PubMed]
- Loecker, C.; Schmaderer, M.; Zimmerman, L. Frailty in Young and Middle-Aged Adults: An Integrative Review. J. Frailty Aging 2021, 10, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, P.; Blane, D.N.; Macdonald, S.; Mair, F.S.; O’Donnell, C.A. Our response to rising frailty in younger people must address prevention burden. Lancet Healthy Longev. 2021, 2, e245. [Google Scholar] [CrossRef] [PubMed]
- Matsuzawa, Y.; Konishi, M.; Akiyama, E.; Suzuki, H.; Nakayama, N.; Kiyokuni, M.; Sumita, S.; Ebina, T.; Kosuge, M.; Hibi, K.; et al. Association between gait speed as a measure of frailty and risk of cardiovascular events after myocardial infarction. J. Am. Coll. Cardiol. 2013, 61, 1964–1972. [Google Scholar] [CrossRef] [PubMed]
- Damluji, A.A.; Forman, D.E.; Wang, T.Y.; Chikwe, J.; Kunadian, V.; Rich, M.W.; Young, B.A.; Page, R.L.; DeVon, H.A.; Alexander, K.P. Management of Acute Coronary Syndrome in the Older Adult Population: A Scientific Statement From the American Heart Association. Circulation 2023, 147, e32–e62. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Segar, M.W.; Usman, M.S.; Singh, S.; Greene, S.J.; Fonarow, G.C.; Anker, S.D.; Felker, G.M.; Januzzi, J.L.; Butler, J.; et al. Frailty, Guideline-Directed Medical Therapy, and Outcomes in HFrEF: From the GUIDE-IT Trial. JACC Heart Fail. 2022, 10, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Murali-Krishnan, R.; Iqbal, J.; Rowe, R.; Hatem, E.; Parviz, Y.; Richardson, J.; Sultan, A.; Gunn, J. Impact of frailty on outcomes after percutaneous coronary intervention: A prospective cohort study. Open Heart 2015, 2, e000294. [Google Scholar] [CrossRef]
- Muthiah, K.; Wilhelm, K.; Robson, D.; Raju, H.; Aili, S.R.; Jha, S.R.; Pierce, R.; Fritis-Lamora, R.; Montgomery, E.; Gorrie, N.; et al. Impact of frailty on mortality and morbidity in bridge to transplant recipients of contemporary durable mechanical circulatory support. J. Heart Lung Transplant. 2022, 41, 829–839. [Google Scholar] [CrossRef]


| Outcome | Frailty (+) | Frailty (−) | Crude Odds Ratio | p-Value | Adjusted Odds Ratio a | p-Value |
|---|---|---|---|---|---|---|
| In-hospital mortality (%) | 35.1 | 20.4 | 2.11 (2.03–2.20) | <0.001 | 2.11 (2.03–2.20) | <0.001 |
| Do not resuscitate (%) | 30.2 | 16.2 | 2.24 (2.14–2.33) | <0.001 | 2.03 (1.95–2.12) | <0.001 |
| Palliative care consultation (%) | 23.3 | 12.1 | 2.21 (2.10–2.31) | <0.001 | 2.00 (1.90–2.10) | <0.001 |
| Skilled nursing facility (%) | 26.2 | 12.9 | 2.39 (2.28–2.51) | <0.001 | 2.06 (1.96–2.16) | <0.001 |
| MCS (%) | 11.2 | 13.4 | 0.82 (0.77–0.87) | <0.001 | 0.91 (0.86–0.97) | 0.003 |
| Heart transplant (%) | 1.3 | 1.5 | 0.88 (0.75–1.04) | 0.125 | 0.96 (0.81–1.13) | 0.619 |
| Intracranial hemorrhage (%) | 1.7 | 0.6 | 2.98 (2.46–3.61) | <0.001 | 3.16 (2.60–3.84) | <0.001 |
| Gastrointestinal hemorrhage (%) | 6.8 | 2.3 | 3.05 (2.76–3.37) | <0.001 | 2.83 (2.56–3.13) | <0.001 |
| Acute kidney injury (%) | 73.1 | 29.2 | 6.59 (6.35–6.84) | <0.001 | 8.10 (7.79–8.43) | <0.001 |
| Delirium (%) | 5.8 | 0.4 | 15.92 (12.69–19.97) | <0.001 | 14.91 (11.88–18.71) | <0.001 |
| Length of stay (days ± SD) | 13.1 ± 15.6 | 8.4 ± 10.1 | 4.77 (4.55–5.00) b | <0.001 | 4.12 (3.90–4.33) c | <0.001 |
| Total hospital cost (USD ± SD) | 60,777 ± 88,028 | 42,792 ± 59,142 | 17,985 (16,699–19,270) b | <0.001 | 17,277 (16,031–18,522) c | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, D.Y.; Jamil, Y.; Ahmad, Y.; Coles, T.; Bosworth, H.B.; Sikand, N.; Davila, C.; Babapour, G.; Damluji, A.A.; Rao, S.V.; et al. Frailty and In-Hospital Outcomes for Management of Cardiogenic Shock without Acute Myocardial Infarction. J. Clin. Med. 2024, 13, 2078. https://doi.org/10.3390/jcm13072078
Park DY, Jamil Y, Ahmad Y, Coles T, Bosworth HB, Sikand N, Davila C, Babapour G, Damluji AA, Rao SV, et al. Frailty and In-Hospital Outcomes for Management of Cardiogenic Shock without Acute Myocardial Infarction. Journal of Clinical Medicine. 2024; 13(7):2078. https://doi.org/10.3390/jcm13072078
Chicago/Turabian StylePark, Dae Yong, Yasser Jamil, Yousif Ahmad, Theresa Coles, Hayden Barry Bosworth, Nikhil Sikand, Carlos Davila, Golsa Babapour, Abdulla A. Damluji, Sunil V. Rao, and et al. 2024. "Frailty and In-Hospital Outcomes for Management of Cardiogenic Shock without Acute Myocardial Infarction" Journal of Clinical Medicine 13, no. 7: 2078. https://doi.org/10.3390/jcm13072078
APA StylePark, D. Y., Jamil, Y., Ahmad, Y., Coles, T., Bosworth, H. B., Sikand, N., Davila, C., Babapour, G., Damluji, A. A., Rao, S. V., Nanna, M. G., & Samsky, M. D. (2024). Frailty and In-Hospital Outcomes for Management of Cardiogenic Shock without Acute Myocardial Infarction. Journal of Clinical Medicine, 13(7), 2078. https://doi.org/10.3390/jcm13072078