
Placental Cortisol Dysregulation in Mothers with Experiences of Childhood Adversity: Potential Mechanisms and Clinical Implications


{kind=link}
{kind=link}
Abstract
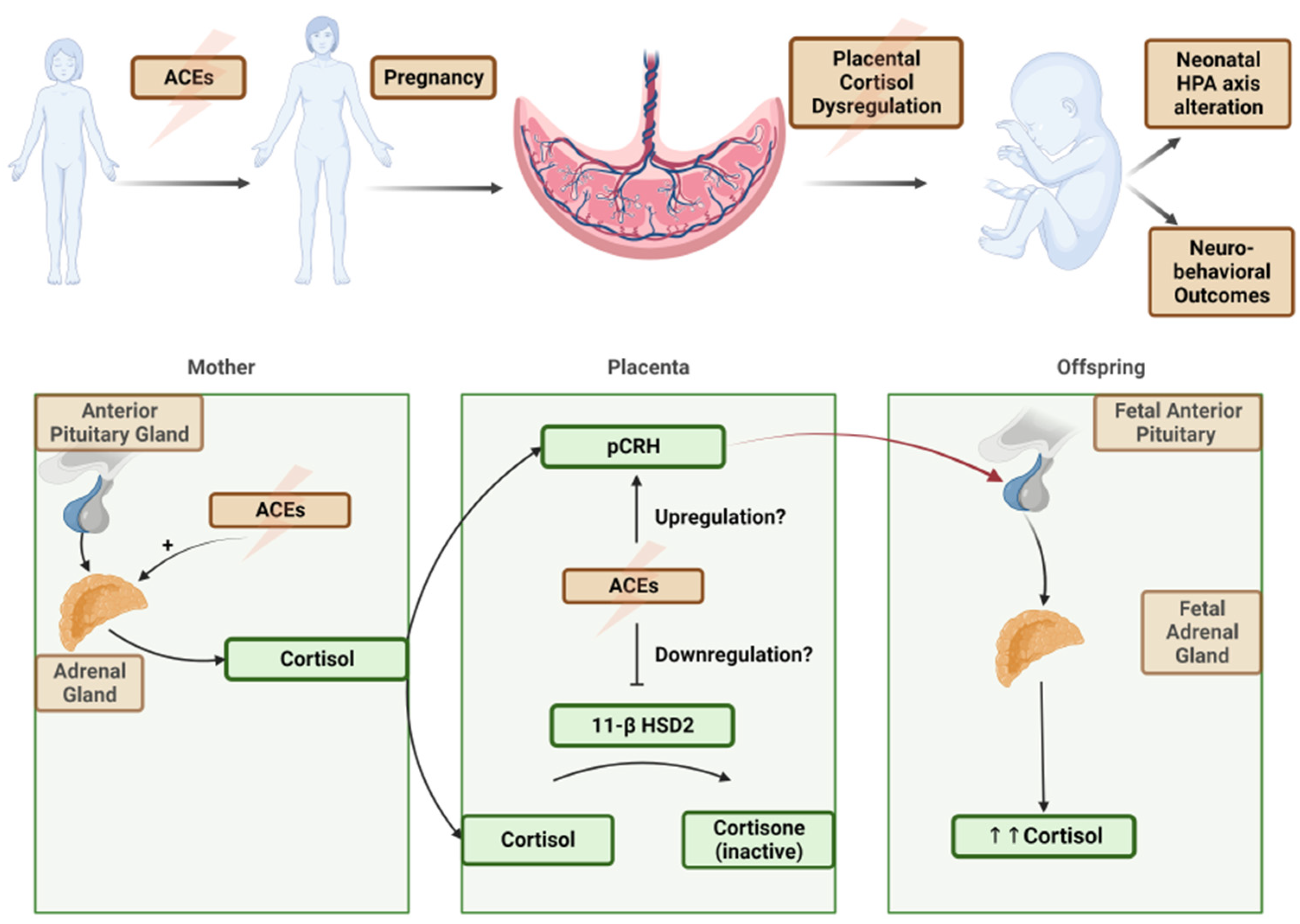
1. Introduction: The Maternal–Placental–Fetal Hypothalamic–Pituitary–Adrenal (HPA) Axis Regulating Fetal Stress
2. The Role of Adverse Childhood Experiences on Placental–Fetal Stress Hormone Cortisol Regulation
3. Connecting the Dots between ACEs and Placental Cortisol Regulation via 11-Beta Hydroxysteroid Dehydrogenase (11β-HSD2)
4. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Kassotaki, I.; Valsamakis, G.; Mastorakos, G.; Grammatopoulos, D.K. Placental CRH as a Signal of Pregnancy Adversity and Impact on Fetal Neurodevelopment. Front. Endocrinol. 2021, 12, 714214. [Google Scholar] [CrossRef] [PubMed]
- Morsi, A.; DeFranco, D.; Witchel, S.F. The Hypothalamic-Pituitary-Adrenal Axis and the Fetus. Horm. Res. Paediatr. 2018, 89, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Swedo, E.A.; Aslam, M.V.; Dahlberg, L.L.; Niolon, P.H.; Guinn, A.S.; Simon, T.R.; Mercy, J.A. Prevalence of Adverse Childhood Experiences Among, U.S. Adults—Behavioral Risk Factor Surveillance System, 2011–2020. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.S.; Fleming, O.; Ekpe, E.E.; Grobman, W.A.; Heard-Garris, N. Association Between Adverse Childhood Experiences and Adverse Pregnancy Outcomes. Obstet. Gynecol. 2021, 138, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Racine, N.; Plamondon, A.; Madigan, S.; McDonald, S.; Tough, S. Maternal Adverse Childhood Experiences and Infant Development. Pediatrics 2018, 141, e20172495. [Google Scholar] [CrossRef] [PubMed]
- Dube, S.R.; Felitti, V.J.; Dong, M.; Chapman, D.P.; Giles, W.H.; Anda, R.F. Childhood abuse, neglect, and household dysfunction and the risk of illicit drug use: The Adverse Childhood Experiences Study. Pediatrics 2003, 111, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Anda, R.F.; Felitti, V.J.; Chapman, D.P.; Croft, J.B.; Williamson, D.F.; Santelli, J.; Dietz, P.M. Abused boys, battered mothers, and male involvement in teen pregnancy. Pediatrics 2002, 109, e19. [Google Scholar] [CrossRef] [PubMed]
- Swales, D.A.; Stout-Oswald, S.A.; Glynn, L.M.; Sandman, C.; Wing, D.A.; Davis, E.P. Exposure to traumatic events in childhood predicts cortisol production among high-risk pregnant women. Biol. Psychol. 2018, 139, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Beijers, R.; Buitelaar, J.K.; de Weerth, C. Mechanisms underlying the effects of prenatal psychosocial stress on child outcomes: Beyond the HPA axis. Eur. Child Adolesc. Psychiatry 2014, 23, 943–956. [Google Scholar] [CrossRef]
- Epstein, C.M.; Houfek, J.F.; Rice, M.J.; Weiss, S.J. Integrative Review of Early Life Adversity and Cortisol Regulation in Pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2021, 50, 242–255. [Google Scholar] [CrossRef] [PubMed]
- Moog, N.K.; Buss, C.; Entringer, S.; Shahbaba, B.; Gillen, D.L.; Hobel, C.J.; Wadhwa, P.D. Maternal Exposure to Childhood Trauma Is Associated during Pregnancy with Placental-Fetal Stress Physiology. Biol. Psychiatry 2016, 79, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Bublitz, M.H.; Stroud, L.R. Childhood sexual abuse is associated with cortisol awakening response over pregnancy: Preliminary findings. Psychoneuroendocrinology 2012, 37, 1425–1430. [Google Scholar] [CrossRef] [PubMed]
- Jahnke, J.R.; Terán, E.; Murgueitio, F.; Cabrera, H.; Thompson, A.L. Maternal stress, placental 11β-hydroxysteroid dehydrogenase type 2, and infant HPA axis development in humans: Psychosocial and physiological pathways. Placenta 2021, 104, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Nazzari, S.; Fearon, P.; Rice, F.; Dottori, N.; Ciceri, F.; Molteni, M.; Frigerio, A. Beyond the HPA-axis: Exploring maternal prenatal influences on birth outcomes and stress reactivity. Psychoneuroendocrinology 2019, 101, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Seth, S.; Lewis, A.J.; Saffery, R.; Lappas, M.; Galbally, M. Maternal Prenatal Mental Health and Placental 11β-HSD2 Gene Expression: Initial Findings from the Mercy Pregnancy and Emotional Wellbeing Study. Int. J. Mol. Sci. 2015, 16, 27482–27496. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, K.J.; Bugge Jensen, A.; Freeman, L.; Khalife, N.; O’Connor, T.G.; Glover, V. Maternal prenatal anxiety and downregulation of placental 11β-HSD2. Psychoneuroendocrinology 2012, 37, 818–826. [Google Scholar] [CrossRef] [PubMed]
- De Weerth, C.; van Hees, Y.; Buitelaar, J.K. Prenatal maternal cortisol levels and infant behavior during the first 5 months. Early Hum. Dev. 2003, 74, 139–151. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, T.G.; Bergman, K.; Sarkar, P.; Glover, V. Prenatal cortisol exposure predicts infant cortisol response to acute stress. Dev. Psychobiol. 2013, 55, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Welberg, L.A.; Thrivikraman, K.V.; Plotsky, P.M. Chronic maternal stress inhibits the capacity to up-regulate placental 11beta-hydroxysteroid dehydrogenase type 2 activity. J. Endocrinol. 2005, 186, R7–R12. [Google Scholar] [CrossRef] [PubMed]
- Hjort, L.; Rushiti, F.; Wang, S.J.; Fransquet, P.; Krasniqi, S.P.; Çarkaxhiu, S.I.; Arifaj, D.; Xhemaili, V.D.; Salihu, M.; Leku, N.A.; et al. Intergenerational effects of maternal post-traumatic stress disorder on offspring epigenetic patterns and cortisol levels. Epigenomics 2021, 13, 967–980. [Google Scholar] [CrossRef] [PubMed]
- Briceño-Pérez, C.; Briceño-Sanabria, L.; Briceño-Sanabria, C.; Reyna-Villasmil, E. Early life corticosteroid overexposure: Epigenetic and fetal origins of adult diseases. Int. J. Gynaecol. Obstet. 2024, 164, 40–46. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
George, J.; Muzik, M.; Townsel, C. Placental Cortisol Dysregulation in Mothers with Experiences of Childhood Adversity: Potential Mechanisms and Clinical Implications. J. Clin. Med. 2024, 13, 2020. https://doi.org/10.3390/jcm13072020
George J, Muzik M, Townsel C. Placental Cortisol Dysregulation in Mothers with Experiences of Childhood Adversity: Potential Mechanisms and Clinical Implications. Journal of Clinical Medicine. 2024; 13(7):2020. https://doi.org/10.3390/jcm13072020
Chicago/Turabian StyleGeorge, Joshua, Maria Muzik, and Courtney Townsel. 2024. "Placental Cortisol Dysregulation in Mothers with Experiences of Childhood Adversity: Potential Mechanisms and Clinical Implications" Journal of Clinical Medicine 13, no. 7: 2020. https://doi.org/10.3390/jcm13072020
APA StyleGeorge, J., Muzik, M., & Townsel, C. (2024). Placental Cortisol Dysregulation in Mothers with Experiences of Childhood Adversity: Potential Mechanisms and Clinical Implications. Journal of Clinical Medicine, 13(7), 2020. https://doi.org/10.3390/jcm13072020