
The Prognostic Value of Right Ventricular Function in Patients with Chronic Heart Failure—A Prospective Study

 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
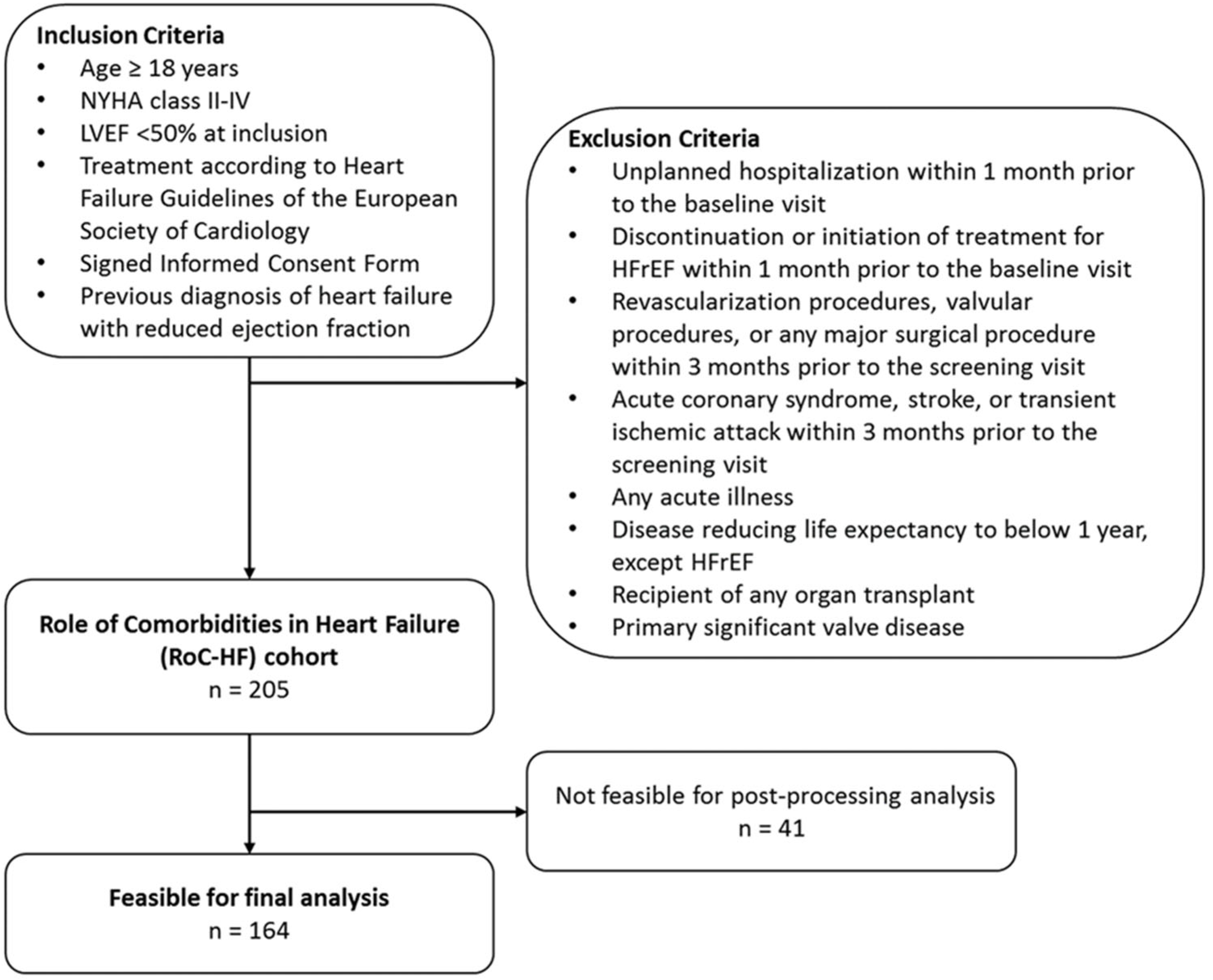
2.1. Study Population
2.2. Echocardiographic Assessment
2.3. Laboratory Parameters
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Study Population
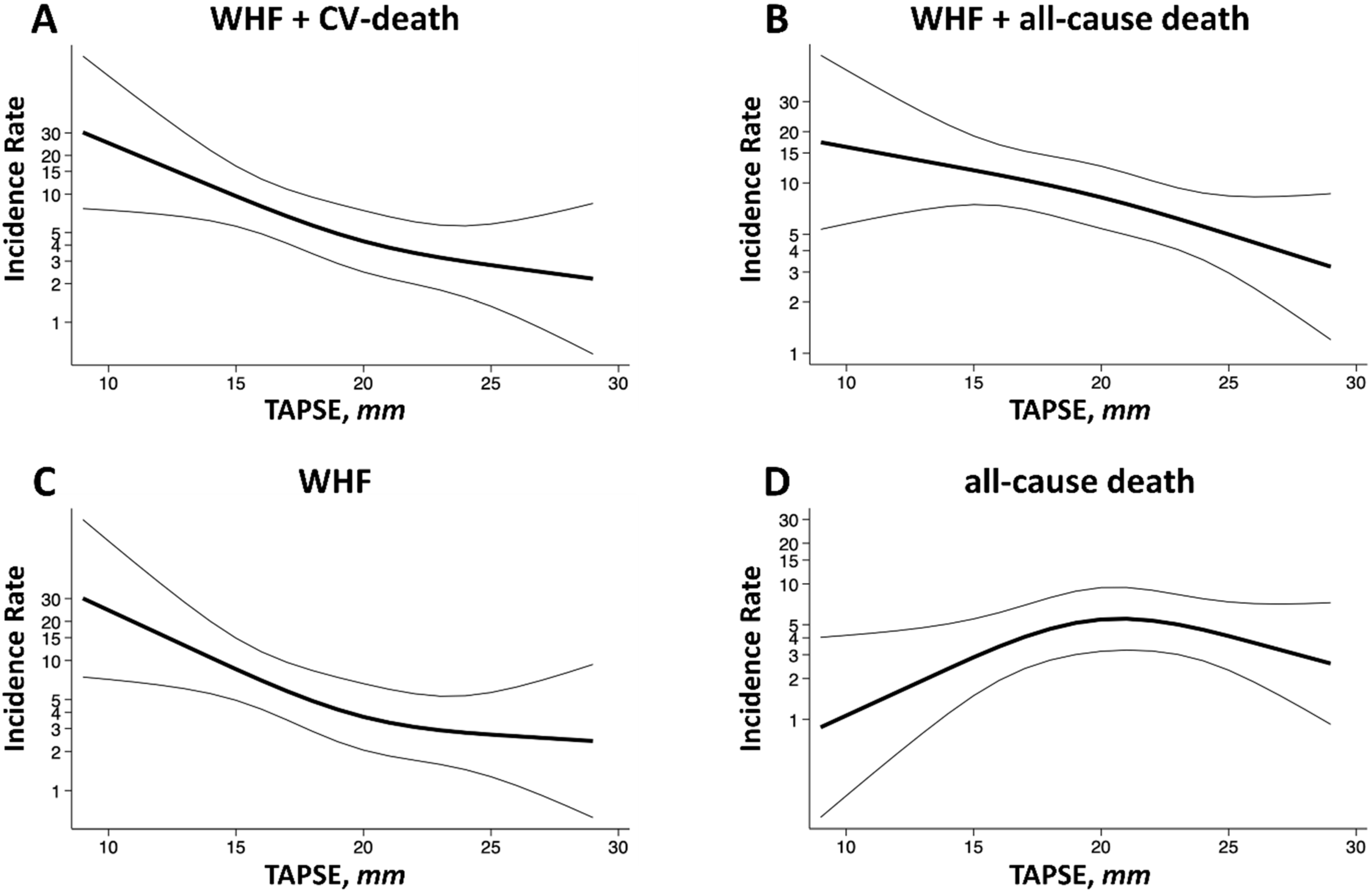
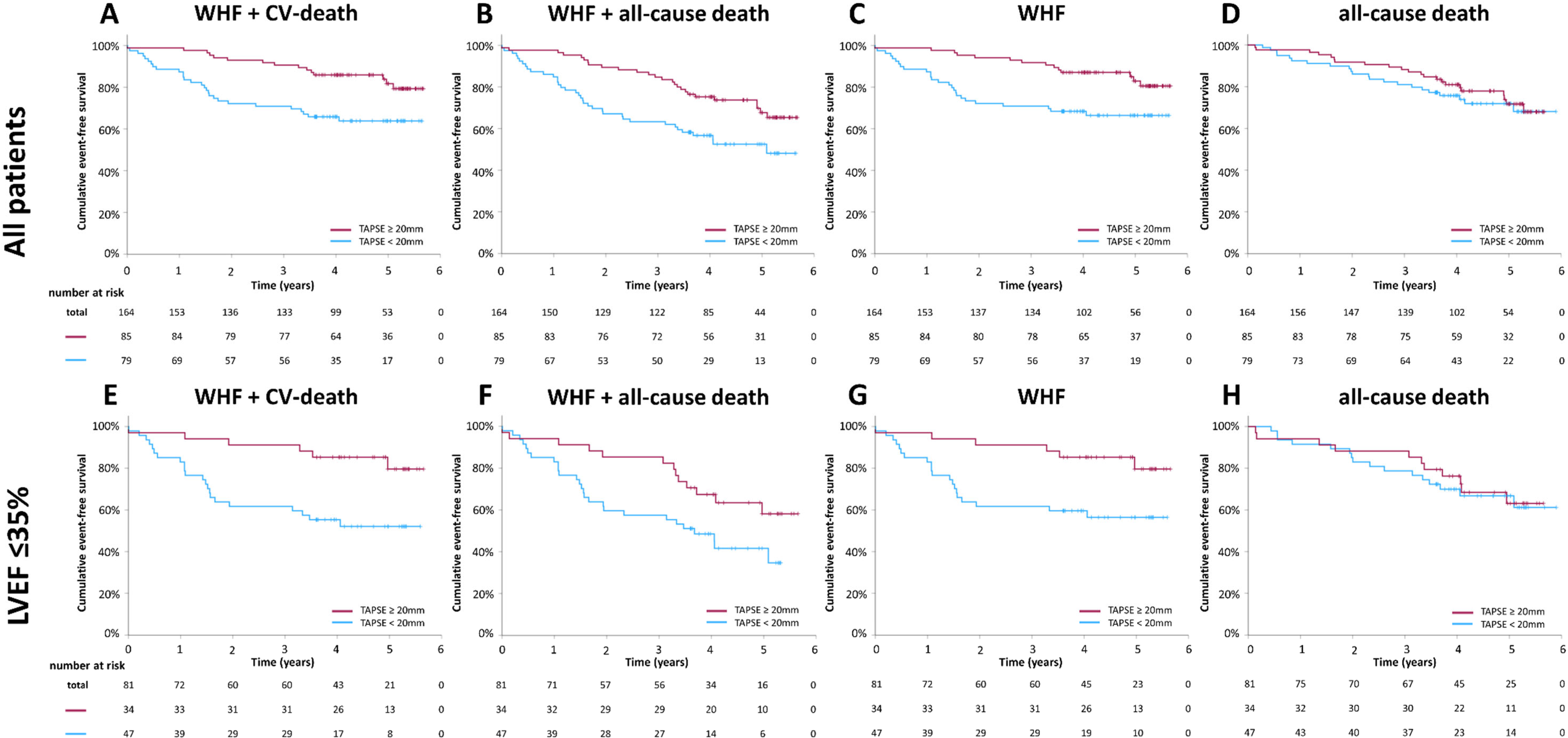
3.2. Outcome Analysis
3.3. Outcomes in a Subgroup with a Left Ventricular Ejection Fraction ≤ 35%
4. Discussion
4.1. Prognostic Value of Right Ventricular Function in Chronic Heart Failure
4.2. Normal Right Ventricular Systolic Function in Heart Failure
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar]
- Santner, V.; Riepl, H.S.; Posch, F.; Wallner, M.; Rainer, P.P.; Ablasser, K.; Kolesnik, E.; Hoeller, V.; Zach, D.; Schwegel, N.; et al. Non-eligibility for pivotal HFpEF/HFmrEF outcome trials and mortality in a contemporary heart failure cohort. Eur. J. Intern. Med. 2023, 118, 73–81. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Investigators, S.; Yusuf, S.; Pitt, B.; Davis, C.E.; Hood, W.B.; Cohn, J.N. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N. Engl. J. Med. 1991, 325, 293–302. [Google Scholar] [CrossRef]
- Swedberg, K.; Kjekshus, J.; CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N. Engl. J. Med. 1987, 316, 1429–1435. [Google Scholar] [CrossRef]
- Packer, M.; Coats, A.J.; Fowler, M.B.; Katus, H.A.; Krum, H.; Mohacsi, P.; Rouleau, J.L.; Tendera, M.; Castaigne, A.; Roecker, E.B.; et al. Effect of carvedilol on survival in severe chronic heart failure. N. Engl. J. Med. 2001, 344, 1651–1658. [Google Scholar] [CrossRef] [PubMed]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc. Imaging 2018, 11, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Anavekar, N.; Skali, H.; McMurray, J.J.; Swedberg, K.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Wang, D.; Pocock, S.; et al. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005, 112, 3738–3744. [Google Scholar] [CrossRef] [PubMed]
- Lundorff, I.J.; Sengelov, M.; Pedersen, S.; Modin, D.; Bruun, N.E.; Fritz-Hansen, T.; Biering-Sørensen, T.; Jørgensen, P.G. Prognostic value of right ventricular echocardiographic measures in patients with heart failure with reduced ejection fraction. J. Clin. Ultrasound. 2021, 49, 903–913. [Google Scholar] [CrossRef]
- Ghio, S.; Guazzi, M.; Scardovi, A.B.; Klersy, C.; Clemenza, F.; Carluccio, E.; Temporelli, P.L.; Rossi, A.; Faggiano, P.; Traversi, E.; et al. Different correlates but similar prognostic implications for right ventricular dysfunction in heart failure patients with reduced or preserved ejection fraction. Eur. J. Heart Fail. 2017, 19, 873–879. [Google Scholar] [CrossRef]
- Lejeune, S.; Roy, C.; Ciocea, V.; Slimani, A.; de Meester, C.; Amzulescu, M.; Pasquet, A.; Vancraeynest, D.; Beauloye, C.; Vanoverschelde, J.-L.; et al. Right Ventricular Global Longitudinal Strain and Outcomes in Heart Failure with Preserved Ejection Fraction. J. Am. Soc. Echocardiogr. 2020, 33, 973–984.e2. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, V.; Papazoglou, A.S.; Moysidis, D.V.; Daios, S.; Tsalikakis, D.; Giannakoulas, G.; Karamitsos, T.; Delgado, V.; Ziakas, A.; Kamperidis, V. The prognostic value of right ventricular longitudinal strain in heart failure: A systematic review and meta-analysis. Heart Fail. Rev. 2023, 28, 1383–1394. [Google Scholar] [CrossRef]
- Verheyen, N.; Schmid, J.; Kolesnik, E.; Schwegel, N.; Späth, J.; Kattnig, L.; Riepl, H.; Zach, D.; Santner, V.; Höller, V.; et al. Prevalence and prognostic impact of bone disease in chronic heart failure with reduced ejection fraction. ESC Heart Fail. 2024. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; 3rd Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef] [PubMed]
- Höller, V.; Seebacher, H.; Zach, D.; Schwegel, N.; Ablasser, K.; Kolesnik, E.; Gollmer, J.; Waltl, G.; Rainer, P.P.; Verheyen, S.; et al. Myocardial Deformation Analysis in MYBPC3 and MYH7 Related Sarcomeric Hypertrophic Cardiomyopathy-The Graz Hypertrophic Cardiomyopathy Registry. Genes 2021, 12, 1469. [Google Scholar] [CrossRef] [PubMed]
- Zach, D.K.; Schwegel, N.; Santner, V.; Winkelbauer, L.; Hoeller, V.; Kolesnik, E.; Gollmer, J.; Seggewiss, H.; Batzner, A.; Perl, S.; et al. Low-grade systemic inflammation and left ventricular dysfunction in hypertensive compared to non-hypertensive hypertrophic cardiomyopathy. Int. J. Cardiol. 2023, 399, 131661. [Google Scholar] [CrossRef] [PubMed]
- Hicks, K.A.; Mahaffey, K.W.; Mehran, R.; Nissen, S.E.; Wiviott, S.D.; Dunn, B.; Solomon, S.D.; Marler, J.R.; Teerlink, J.R.; Farb, A.; et al. 2017 Cardiovascular and Stroke Endpoint Definitions for Clinical Trials. Circulation 2018, 137, 961–972. [Google Scholar] [CrossRef]
- Carluccio, E.; Biagioli, P.; Alunni, G.; Murrone, A.; Zuchi, C.; Coiro, S.; Riccini, C.; Mengoni, A.; D’Antonio, A.; Ambrosio, G. Prognostic Value of Right Ventricular Dysfunction in Heart Failure with Reduced Ejection Fraction: Superiority of Longitudinal Strain Over Tricuspid Annular Plane Systolic Excursion. Circ. Cardiovasc. Imaging 2018, 11, e006894. [Google Scholar] [CrossRef]
- Parrinello, G.; Torres, D.; Buscemi, S.; Di Chiara, T.; Cuttitta, F.; Cardillo, M.; Pluchinotta, F.R.; Scaglione, R.; Paterna, S.; Pinto, A. Right ventricular diameter predicts all-cause mortality in heart failure with preserved ejection fraction. Intern. Emerg. Med. 2019, 14, 1091–1100. [Google Scholar] [CrossRef]
- Kanagala, P.; Arnold, J.R.; Singh, A.; Khan, J.N.; Gulsin, G.S.; Gupta, P.; Squire, I.B.; Ng, L.L.; McCann, G.P. Prevalence of right ventricular dysfunction and prognostic significance in heart failure with preserved ejection fraction. Int. J. Cardiovasc. Imaging 2021, 37, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Damy, T.; Kallvikbacka-Bennett, A.; Goode, K.; Khaleva, O.; Lewinter, C.; Hobkirk, J.; Nikitin, N.P.; Dubois-Randé, J.-L.; Hittinger, L.; Clark, A.L.; et al. Prevalence of, associations with, and prognostic value of tricuspid annular plane systolic excursion (TAPSE) among out-patients referred for the evaluation of heart failure. J. Card. Fail. 2012, 18, 216–225. [Google Scholar] [CrossRef]
- Legris, V.; Thibault, B.; Dupuis, J.; White, M.; Asgar, A.W.; Fortier, A.; Pitre, C.; Bouabdallaoui, N.; Henri, C.; O’Meara, E.; et al. Right ventricular function and its coupling to pulmonary circulation predicts exercise tolerance in systolic heart failure. ESC Heart Fail. 2022, 9, 450–464. [Google Scholar] [CrossRef] [PubMed]
- Menegazzo, W.R.; Santos, A.B.S.; Foppa, M.; Scolari, F.L.; Barros, F.C.; Stein, R.; da Silveira, A.D. Prognostic value of right ventricular strain and peak oxygen consumption in heart failure with reduced ejection fraction. Int. J. Cardiovasc. Imaging 2023, 39, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Modin, D.; Mogelvang, R.; Andersen, D.M.; Biering-Sorensen, T. Right Ventricular Function Evaluated by Tricuspid Annular Plane Systolic Excursion Predicts Cardiovascular Death in the General Population. J. Am. Heart Assoc. 2019, 8, e012197. [Google Scholar] [CrossRef] [PubMed]
- Monitillo, F.; Di Terlizzi, V.; Gioia, M.I.; Barone, R.; Grande, D.; Parisi, G.; Brunetti, N.D.; Iacoviello, M. Right Ventricular Function in Chronic Heart Failure: From the Diagnosis to the Therapeutic Approach. J Cardiovasc. Dev. Dis. 2020, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Arrigo, M.; Huber, L.C.; Winnik, S.; Mikulicic, F.; Guidetti, F.; Frank, M.; Flammer, A.J.; Ruschitzka, F. Right Ventricular Failure: Pathophysiology, Diagnosis and Treatment. Card. Fail. Rev. 2019, 5, 140–146. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: Rationale for and design of the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur. J. Heart Fail. 2013, 15, 1062–1073. [Google Scholar]
- Levy, W.C.; Mozaffarian, D.; Linker, D.T.; Sutradhar, S.C.; Anker, S.D.; Cropp, A.B.; Anand, I.; Maggioni, A.; Burton, P.; Sullivan, M.D.; et al. The Seattle Heart Failure Model: Prediction of survival in heart failure. Circulation 2006, 113, 1424–1433. [Google Scholar] [CrossRef]
- Senni, M.; Parrella, P.; De Maria, R.; Cottini, C.; Böhm, M.; Ponikowski, P.; Filippatos, G.; Tribouilloy, C.; Di Lenarda, A.; Oliva, F.; et al. Predicting heart failure outcome from cardiac and comorbid conditions: The 3C-HF score. Int. J. Cardiol. 2013, 163, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Rich, J.D.; Burns, J.; Freed, B.H.; Maurer, M.S.; Burkhoff, D.; Shah, S.J. Meta-Analysis Global Group in Chronic (MAGGIC) Heart Failure Risk Score: Validation of a Simple Tool for the Prediction of Morbidity and Mortality in Heart Failure with Preserved Ejection Fraction. J. Am. Heart Assoc. 2018, 7, e009594. [Google Scholar] [CrossRef] [PubMed]
- Greene, S.J.; Butler, J.; Albert, N.M.; DeVore, A.D.; Sharma, P.P.; Duffy, C.I.; Hill, C.L.; McCague, K.; Mi, X.; Patterson, J.H.; et al. Medical Therapy for Heart Failure with Reduced Ejection Fraction: The CHAMP-HF Registry. J. Am. Coll. Cardiol. 2018, 72, 351–366. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L. Epidemiology of Heart Failure: A Contemporary Perspective. Circ. Res. 2021, 128, 1421–1434. [Google Scholar] [CrossRef]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Køber, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure: A risk score based on 39 372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| All Patients | LVEF > 35% | LVEF ≤ 35% | p-Value * | |
|---|---|---|---|---|
| n = 164 | n = 83 | n = 81 | ||
| Demographics | ||||
| Female, n (%) | 36 (22) | 23 (28) | 13 (16) | 0.090 |
| Age, years | 64.8 ± 10.4 | 64.8 ± 10.7 | 64.8 ± 10.1 | 0.927 |
| BMI, kg/m2 | 28.5 ± 4.7 | 28.8 ± 5.1 | 28.2 ± 4.3 | 0.638 |
| Heart failure duration, years | 9.0 ± 7.0 | 7.1 ± 6.4 | 11.0 ± 7.0 | <0.001 |
| Caucasian ethnicity, n (%) | 164 (100) | 83 (100) | 81 (100) | - |
| Symptoms | ||||
| NYHA functional class | ||||
| NYHA II, n (%) | 110 (67) | 57 (69) | 53 (65) | 0.563 |
| NYHA II-III, n (%) | 30 (18) | 13 (16) | 17 (21) | |
| NYHA III, n (%) | 23 (14) | 13 (16) | 10 (12) | |
| NYHA IV, n (%) | 1 (1) | 0 (0) | 1 (1) | |
| Angina, n (%) | 30 (18) | 16 (20) | 14 (17) | 0.498 |
| Clinical characteristics | ||||
| Ischemic-origin, n (%) | 66 (40) | 30 (36) | 36 (44) | 0.279 |
| Non-ischemic-origin, n (%) | 98 (60) | 53 (64) | 45 (56) | |
| SBP, mmHg | 123 ± 20 | 127 ± 23 | 118 ± 16 | 0.006 |
| DBP, mmHg | 77 ± 13 | 79 ± 14 | 74 ± 11 | 0.007 |
| 24 h SBP, mmHg | 111 ± 13 | 114 ± 14 | 108 ± 12 | 0.003 |
| 24 h DBP, mmHg | 68 ± 9 | 69 ± 9 | 67 ± 9 | 0.066 |
| Heart rate, bpm | 66 ± 12 | 64 ± 11 | 67 ± 13 | 0.194 |
| 24 h-heart rate, bpm | 67 ± 10 | 68 ± 11 | 66 ± 9 | 0.349 |
| Device therapy | ||||
| Pacemaker, n (%) | 47 (29) | 21 (25) | 26 (32) | 0.370 |
| ICD, n (%) | 106 (65) | 47 (57) | 59 (73) | 0.032 |
| CRT, n (%) | 53 (32) | 27 (33) | 26 (32) | 0.933 |
| Comorbidities | ||||
| Atrial fibrillation, n (%) | 69 (42) | 34 (41) | 35 (43) | 0.874 |
| Diabetes mellitus, n (%) | 44 (27) | 20 (24) | 24 (30) | 0.381 |
| Arterial hypertension, n (%) | 112 (68) | 55 (66) | 57 (70) | 0.662 |
| Hyperlipidemia, n (%) | 78 (48) | 44 (53) | 34 (42) | 0.271 |
| COPD, n (%) | 34 (21) | 13 (16) | 21 (26) | 0.253 |
| Smoker, n (%) | 105 (64) | 56 (68) | 49 (61) | 0.648 |
| Pharmacological treatment | ||||
| ACE/ARB/ARNI, n (%) | 151 (92) | 77 (93) | 74 (91) | 0.780 |
| Beta-blocker, n (%) | 158 (96) | 81 (98) | 77 (95) | 0.440 |
| MRA, n (%) | 129 (79) | 64 (77) | 65 (80) | 0.704 |
| Thiazide, n (%) | 18 (11) | 8 (10) | 10 (12) | 0.625 |
| Loop-diuretics, n (%) | 96 (59) | 48 (58) | 48 (59) | 0.875 |
| SGLT2 inhibitors, n (%) | 6 (4) | 5 (6) | 1 (1) | 0.210 |
| Laboratory parameters | ||||
| NT-proBNP, pg/mL | 978 (332–2279) | 511 (200–1507) | 1583 (612–3266) | <0.001 |
| Creatinine, mg/dL | 1.25 ± 0.55 | 1.22 ± 0.43 | 1.28 ± 0.65 | 0.669 |
| eGFR, mL/min/1.73 m2 | 65 ± 22 | 64 ± 22 | 66 ± 23 | 0.644 |
| Echocardiography | ||||
| LVEF, % | 35.8 ± 8.2 | 42.5 ± 4.6 | 29.0 ± 4.7 | <0.001 |
| LVEDV, mL | 155 ± 61 | 126 ± 38 | 184 ± 67 | <0.001 |
| LVESV, mL | 102 ± 50 | 73 ± 24 | 132 ± 53 | <0.001 |
| GLS, % | −12.1 ± 3.6 | −14.4 ± 3.0 | −9.7 ± 2.6 | <0.001 |
| E/e’ | 16 ± 8 | 13 ± 6 | 18 ± 9 | <0.001 |
| TAPSE, mm | 20 ± 5 | 21 ± 5 | 18 ± 5 | 0.002 |
| TR-Vmax, m/s | 2.7 ± 0.5 | 2.6 ± 0.4 | 2.8 ± 0.5 | 0.023 |
| sPAP, mmHg | 41 ± 12 | 39 ± 10 | 43 ± 13 | 0.038 |
| LAVI, mL/m2 | 52 ± 21 | 47 ± 19 | 57 ± 21 | 0.001 |
| All Patients | LVEF ≤ 35% | |||||
|---|---|---|---|---|---|---|
| Univariate | Model 1 * | Model 2 ** | Univariate | Model 1 * | Model 2 ** | |
| Hazard Ratio (95% Confidence Interval), p-Value | Hazard Ratio (95% Confidence Interval), p-Value | |||||
| Composite endpoint I | ||||||
| TAPSE | 0.859 (0.800–0.921) p ≤ 0.001 | 0.884 (0.817–0.958) p = 0.002 | 0.878 (0.800–0.964), p = 0.006 | 0.838 (0.761–0.923), p ≤ 0.001 | 0.836 (0.749–0.933), p = 0.001 | 0.791 (0.680–0.920), p = 0.002 |
| TR-Vmax | 2.168 (1.082–4.348) p = 0.029 | 1.737 (0.781–3.863) p = 0.176 | 1.375 (0.526–3.593), p = 0.516 | 2.246 (0.947–5.327), p = 0.066 | ||
| sPAP | 1.043 (1.017–1.069) p ≤ 0.001 | 1.038 (1.007–1.071) p = 0.017 | 1.032 (0.996–1.070), p = 0.082 | 1.037 (1.008–1.068), p = 0.013 | 1.058 (1.016–1.101), p = 0.006 | 1.059 (1.006–1.115), p = 0.028 |
| LVEF | 0.953 (0.920–0.987) p = 0.008 | 0.959 (0.929–0.997) p = 0.036 | 0.982 (0.912–1.058), p = 0.633 | |||
| LV GLS | 1.152 (1.058–1.255) p = 0.001 | 1.131 (1.028–1.249) p = 0.011 | 1.068 (0.927–1.231), p = 0.361 | |||
| Composite endpoint II | ||||||
| TAPSE | 0.885 (0.836–0.937) p ≤ 0.001 | 0.902 (0.844–0.964) p = 0.002 | 0.918 (0.853–0.988), p = 0.023 | 0.890 (0.825–0.960), p = 0.003 | 0.894 (0.823–0.972), p = 0.008 | 0.840 (0.749–0.941), p = 0.003 |
| TR-Vmax | 2.445 (1.406–4.250) p = 0.002 | 2.199 (1.133–4.265), p = 0.020 | 1.903 (0.820–4.418), p = 0.134 | 2.060 (1.053–4.029), p = 0.035 | 2.498 (1.006–6.202), p = 0.048 | 3.080 (1.064–8.915), p = 0.038 |
| sPAP | 1.039 (1.019–1.060) p ≤ 0.001 | 1.033 (1.007–1.060), p = 0.013 | 1.025 (0.994–1.057), p = 0.113 | 1.025 (1.002–1.050), p = 0.037 | 1.035 (1.001–1.070), p = 0.046 | 1.037 (0.998–1.078), p = 0.066 |
| LVEF | 0.960 (0.932–0.988) p = 0.005 | 0.974 (0.942–1.006), p = 0.112 | 1.016 (0.948–1.088), p = 0.654 | |||
| LV GLS | 1.106 (1.033–1.184) p = 0.004 | 1.071 (0.989–1.160), p = 0.092 | 0.989 (0.878–1.115), p = 0.862 | |||
| Worsening heart failure hospitalization | ||||||
| TAPSE | 0.857 (0.796–0.922) p ≤ 0.001 | 0.881 (0.811–0.957), p = 0.003 | 0.880 (0.800–0.968), p = 0.008 | 0.836 (0.756–0.925), p ≤ 0.001 | 0.830 (0.739–0.931), p = 0.002 | 0.781 (0.667–0.916), p = 0.002 |
| TR-Vmax | 2.015 (0.984–4.125) p = 0.055 | 1.737 (0.712–4.236), p = 0.225 | ||||
| sPAP | 1.038 (1.012–1.065) p = 0.004 | 1.030 (0.999–1.063), p = 0.059 | 1.030 (0.992–1.069), p = 0.121 | 1.027 (0.995–1.059), p = 0.095 | ||
| LVEF | 0.951 (0.917–0.987) p = 0.007 | 0.958 (0.920–0.998), p = 0.038 | 0.983 (0.910–1.061), p = 0.659 | |||
| LV GLS | 1.165 (1.066–1.273) p ≤ 0.001 | 1.146 (1.037–1.265), p = 0.007 | 1.074 (0.927–1.244), p = 0.342 | |||
| All-cause mortality | ||||||
| TAPSE | 0.954 (0.896–1.016) p = 0.140 | 0.959 (0.882–1.042), p = 0.321 | ||||
| TR-Vmax | 2.226 (1.155–4.288) p = 0.017 | 2.817 (1.209–6.559), p = 0.016 | 2.735 (0.942–7.942), p = 0.064 | 1.486 (0.674–3.278), p = 0.326 | ||
| sPAP | 1.029 (1.005–1.053) p = 0.016 | 1.030 (0.999–1.062), p = 0.059 | 1.025 (0.986–1.066), p = 0.210 | 1.009 (0.981–1.038), p = 0.528 | ||
| LVEF | 0.979 (0.945–1.014) p = 0.226 | 1.053 (0.957–1.158), p = 0.289 | ||||
| LV GLS | 1.045 (0.964–1.132) p = 0.283 | 0.957 (0.827–1.107), p = 0.555 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwegel, N.; Zach, D.; Peikert, A.; Santner, V.; Höller, V.; Gollmer, J.; Späth, J.; Riepl, H.; Rainer, P.P.; Wallner, M.; et al. The Prognostic Value of Right Ventricular Function in Patients with Chronic Heart Failure—A Prospective Study. J. Clin. Med. 2024, 13, 1930. https://doi.org/10.3390/jcm13071930
Schwegel N, Zach D, Peikert A, Santner V, Höller V, Gollmer J, Späth J, Riepl H, Rainer PP, Wallner M, et al. The Prognostic Value of Right Ventricular Function in Patients with Chronic Heart Failure—A Prospective Study. Journal of Clinical Medicine. 2024; 13(7):1930. https://doi.org/10.3390/jcm13071930
Chicago/Turabian StyleSchwegel, Nora, David Zach, Alexander Peikert, Viktoria Santner, Viktoria Höller, Johannes Gollmer, Johannes Späth, Hermann Riepl, Peter P. Rainer, Markus Wallner, and et al. 2024. "The Prognostic Value of Right Ventricular Function in Patients with Chronic Heart Failure—A Prospective Study" Journal of Clinical Medicine 13, no. 7: 1930. https://doi.org/10.3390/jcm13071930
APA StyleSchwegel, N., Zach, D., Peikert, A., Santner, V., Höller, V., Gollmer, J., Späth, J., Riepl, H., Rainer, P. P., Wallner, M., Pilz, S., Zirlik, A., von Lewinski, D., Ablasser, K., Verheyen, N., & Kolesnik, E. (2024). The Prognostic Value of Right Ventricular Function in Patients with Chronic Heart Failure—A Prospective Study. Journal of Clinical Medicine, 13(7), 1930. https://doi.org/10.3390/jcm13071930