

Incidence, Risk Factors, and Outcomes of De Novo Malignancy following Kidney Transplantation

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
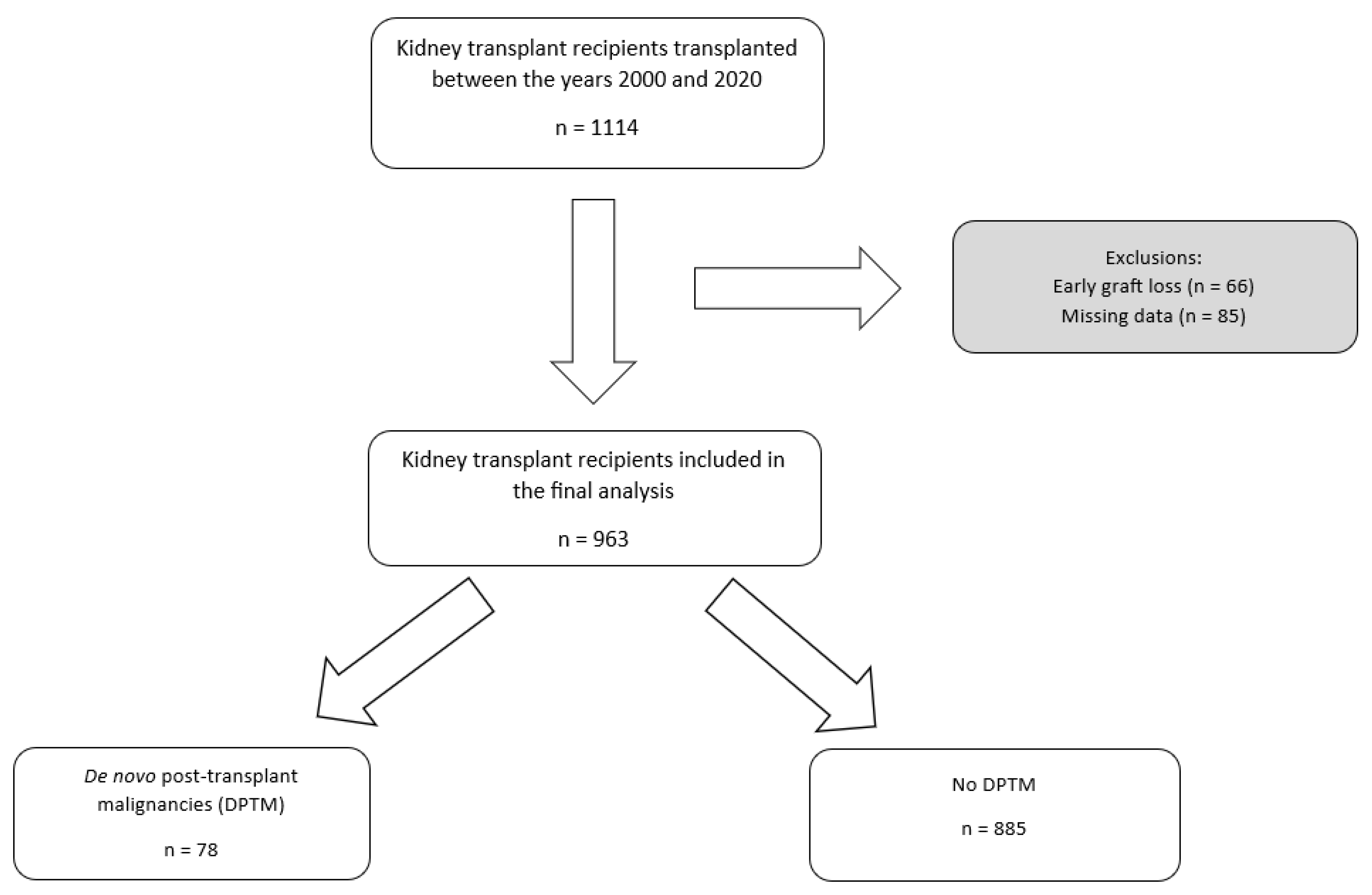
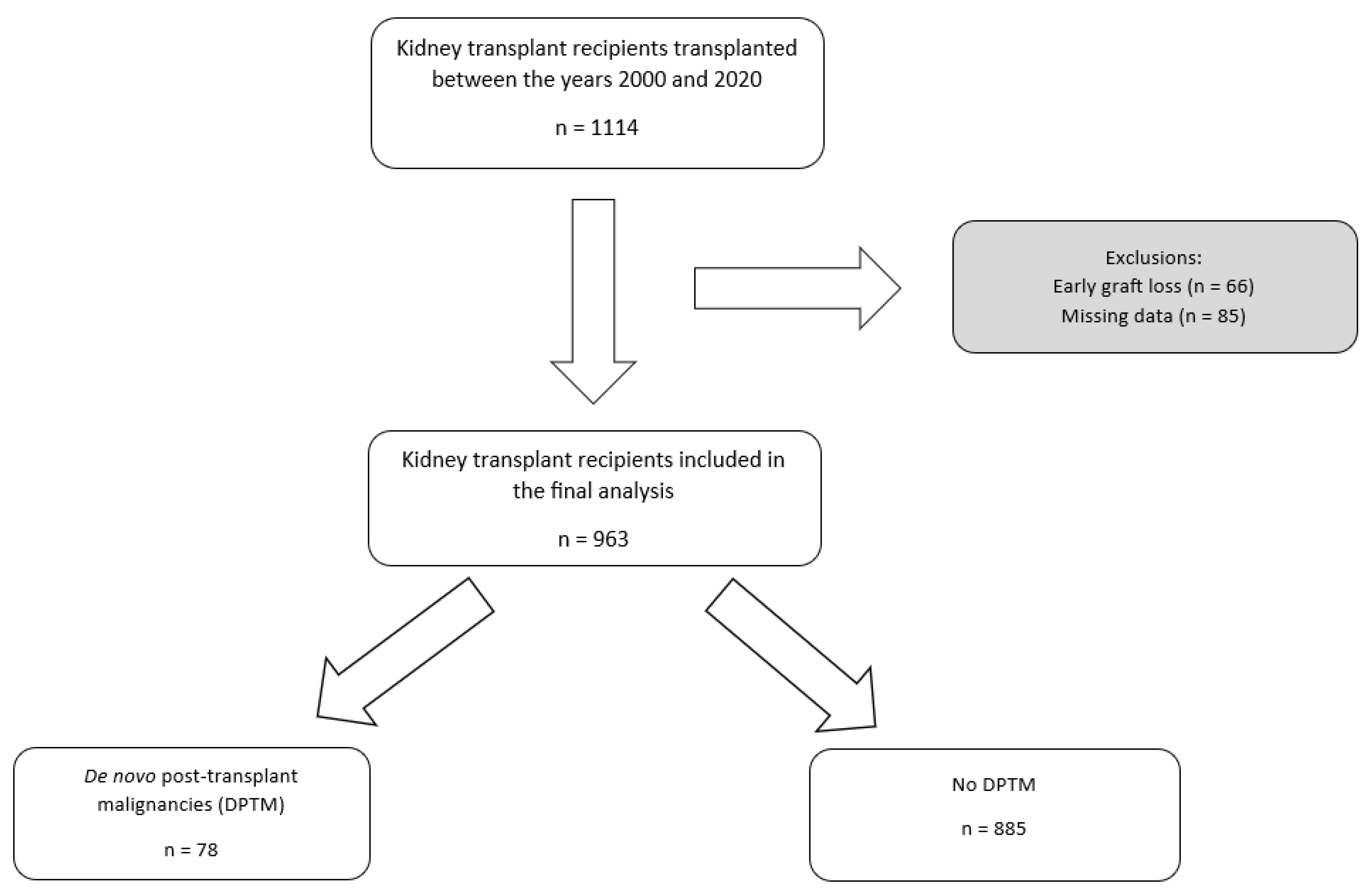
2.1. Study Population
2.2. Data Collection
2.3. Local Post-Transplant Immunosuppression Protocol
2.4. Statistical Analysis
2.5. Ethical Considerations of the Study
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wong, G.; Howard, K.; Chapman, J.R.; Chadban, S.; Cross, N.; Tong, A.; Webster, A.C.; Craig, J.C. Comparative survival and economic benefits of deceased donor kidney transplantation and dialysis in people with varying ages and co-morbidities. PLoS ONE 2012, 7, e29591. [Google Scholar] [CrossRef]
- Al-Adra, D.; Al-Qaoud, T.; Fowler, K.; Wong, G. De novo malignancies after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2022, 17, 434–443. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Zeier, M.G.; Chapman, J.R.; Craig, J.C.; Ekberg, H.; Garvey, C.A.; Green, M.D.; Jha, V.; Josephson, M.A.; Kiberd, B.A.; et al. KDIGO clinical practice guideline for the care of kidney transplant recipients: A summary. Kidney Int. 2010, 77, 299–311. [Google Scholar] [CrossRef]
- Krynitz, B.; Edgren, G.; Lindelöf, B.; Baecklund, E.; Brattström, C.; Wilczek, H.; Smedby, K.E. Risk of skin cancer and other malignancies in kidney, liver, heart and lung transplant recipients 1970 to 2008—A Swedish population-based study. Int. J. Cancer 2013, 132, 1429–1438. [Google Scholar] [CrossRef]
- Zhang, J.; Ma, L.; Xie, Z.; Guo, Y.; Sun, W.; Zhang, L.; Lin, J.; Xiao, J.; Zhu, Y.; Tian, Y. Epidemiology of post-transplant malignancy in Chinese renal transplant recipients: A single-center experience and literature review. Med. Oncol. 2014, 31, 32. [Google Scholar] [CrossRef] [PubMed]
- Villeneuve, P.J.; Schaubel, D.E.; Fenton, S.S.; Shepherd, F.A.; Jiang, Y.; Mao, Y. Cancer incidence among Canadian kidney transplant recipients. Am. J. Transplant. 2007, 7, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Snyder, J.J.; Gilbertson, D.T.; Wang, C. Cancer after kidney transplantation in the United States. Am. J. Transplant. 2004, 4, 905–913. [Google Scholar] [CrossRef] [PubMed]
- Chadban, S.J.; Ahn, C.; Axelrod, D.A.; Foster, B.J.; Kasiske, B.L.; Kher, V.; Kumar, D.; Oberbauer, R.; Pascual, J.; Pilmore, H.L.; et al. KDIGO clinical practice guideline on the evaluation and management of candidates for kidney transplantation. Transplantation 2020, 104, S11–S103. [Google Scholar] [CrossRef]
- Miao, Y.; Everly, J.J.; Gross, T.G.; Tevar, A.D.; First, M.R.; Alloway, R.R.; Woodle, E.S. De novo cancers arising in organ transplant recipients are associated with adverse outcomes compared with the general population. Transplantation 2009, 87, 1347–1359. [Google Scholar] [CrossRef] [PubMed]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Webster, A.C.; Craig, J.C.; Simpson, J.M.; Jones, M.P.; Chapman, J.R. Identifying high risk groups and quantifying absolute risk of cancer after kidney transplantation: A cohort study of 15 183 recipients. Am. J. Transplant. 2007, 7, 2140–2151. [Google Scholar] [CrossRef] [PubMed]
- Webster, A.C.; Wong, G.; Craig, J.C.; Chapman, J.R. Managing cancer risk and decision making after kidney transplantation. Am. J. Transplant. 2008, 8, 2185–2191. [Google Scholar] [CrossRef] [PubMed]
- Adami, J.; Gäbel, H.; Lindelöf, B.; Ekström, K.; Rydh, B.; Glimelius, B.; Ekbom, A.; Adami, H.O.; Granath, F. Cancer risk following organ transplantation: A nationwide cohort study in Sweden. Br. J. Cancer 2003, 89, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Navarro, M.D.; Lopez-Andreu, M.; Rodriguez-Benot, A.; Agüera, M.L.; Del Castillo, D.; Aljama, P. Cancer incidence and survival in kidney transplant patients. Transplant. Proc. 2008, 40, 2936–2940. [Google Scholar] [CrossRef]
- Vajdic, C.M.; McDonald, S.P.; McCredie, M.R.; Van Leeuwen, M.T.; Stewart, J.H.; Law, M.; Chapman, J.R.; Webster, A.C.; Kaldor, J.M.; Grulich, A.E. Cancer incidence before and after kidney transplantation. JAMA 2006, 296, 2823–2831. [Google Scholar] [CrossRef]
- Li, W.-H.; Chen, Y.-J.; Tseng, W.-C.; Lin, M.-W.; Chen, T.-J.; Chu, S.-Y.; Hwang, C.-Y.; Chen, C.-C.; Lee, D.-D.; Chang, Y.-T.; et al. Malignancies after renal transplantation in Taiwan: A nationwide population-based study. Nephrol. Dial. Transplant. 2012, 27, 833–839. [Google Scholar] [CrossRef]
- Lai, M.-N.; Wang, S.-M.; Chen, P.-C.; Chen, Y.-Y.; Wang, J.-D. Population-based case–control study of Chinese herbal products containing aristolochic acid and urinary tract cancer risk. J. Natl. Cancer Inst. 2010, 102, 179–186. [Google Scholar] [CrossRef]
- Mittal, A.; Colegio, O.R. Skin cancers in organ transplant recipients. Am. J.Transplant. 2017, 17, 2509–2530. [Google Scholar] [CrossRef]
- Lim, W.H.; Turner, R.M.; Chapman, J.R.; Ma, M.K.; Webster, A.C.; Craig, J.C.; Wong, G. Acute rejection, T-cell–depleting antibodies, and cancer after transplantation. Transplantation 2014, 97, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.H.; Chapman, J.R.; Wong, G. Peak panel reactive antibody, cancer, graft, and patient outcomes in kidney transplant recipients. Transplantation 2015, 99, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Turner, R.M.; Chapman, J.R.; Howell, M.; Lim, W.H.; Webster, A.C.; Craig, J.C. Time on dialysis and cancer risk after kidney transplantation. Transplantation 2013, 95, 114–121. [Google Scholar] [CrossRef]
- Wong, G.; Hayen, A.; Chapman, J.R.; Webster, A.C.; Wang, J.J.; Mitchell, P.; Craig, J.C. Association of CKD and cancer risk in older people. J. Am. Soc. Nephrol. 2009, 20, 1341–1350. [Google Scholar] [CrossRef]
- Lowrance, W.T.; Ordoñez, J.; Udaltsova, N.; Russo, P.; Go, A.S. CKD and the risk of incident cancer. J. Am. Soc. Nephrol. 2014, 25, 2327–2334. [Google Scholar] [CrossRef]
- Stengel, B. Chronic kidney disease and cancer: A troubling connection. J. Nephrol. 2010, 23, 253–262. [Google Scholar]
- Acuna, S.A.; Huang, J.W.; Dossa, F.; Shah, P.S.; Kim, S.J.; Baxter, N.N. Cancer recurrence after solid organ transplantation: A systematic review and meta-analysis. Transplant. Rev. 2017, 31, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Acuna, S.A.; Sutradhar, R.; Kim, S.J.; Baxter, N.N. Solid organ transplantation in patients with preexisting malignancies in remission: A propensity score matched cohort study. Transplantation 2018, 102, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Livingston-Rosanoff, D.; Foley, D.P.; Leverson, G.; Wilke, L.G. Impact of pre-transplant malignancy on outcomes after kidney transplantation: United Network for Organ Sharing database analysis. J. Am. Coll. Surg. 2019, 229, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Viecelli, A.K.; Lim, W.H.; Macaskill, P.; Chapman, J.R.; Craig, J.C.; Clayton, P.; Cohney, S.; Carroll, R.; Wong, G. Cancer-specific and all-cause mortality in kidney transplant recipients with and without previous cancer. Transplantation 2015, 99, 2586–2592. [Google Scholar] [CrossRef] [PubMed]
- Au, E.H.; Chapman, J.R.; Craig, J.C.; Lim, W.H.; Teixeira-Pinto, A.; Ullah, S.; McDonald, S.; Wong, G. Overall and site-specific cancer mortality in patients on dialysis and after kidney transplant. J. Am. Soc. Nephrol. 2019, 30, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Hayward, J.S.; McArthur, E.; Craig, J.C.; Nash, D.M.; Dixon, S.N.; Zimmerman, D.; Kitchlu, A.; Garg, A.X. Patterns and predictors of screening for breast and cervical cancer in women with CKD. Clin. J. Am. Soc. Nephrol. 2017, 12, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, M.P.; Kelly, P.J.; Jardine, M.; Perkovic, V.; Cass, A.; Craig, J.C.; Eris, J.; Webster, A.C. Long-term cancer risk of immunosuppressive regimens after kidney transplantation. J. Am. Soc. Nephrol. 2010, 21, 852–858. [Google Scholar] [CrossRef]
- Maluccio, M.; Sharma, V.; Lagman, M.; Vyas, S.; Yang, H.; Li, B.; Suthanthiran, M. Tacrolimus enhances transforming growth factor-β1 expression and promotes tumor progression. Transplantation 2003, 76, 597–602. [Google Scholar] [CrossRef]
- Wu, X.; Nguyen, B.C.; Dziunycz, P.; Chang, S.; Brooks, Y.; Lefort, K.; Hofbauer, G.F.; Dotto, G.P. Opposing roles for calcineurin and ATF3 in squamous skin cancer. Nature 2010, 465, 368–372. [Google Scholar] [CrossRef]
- Hojo, M.; Morimoto, T.; Maluccio, M.; Asano, T.; Morimoto, K.; Lagman, M.; Shimbo, T.; Suthanthiran, M. Cyclosporine induces cancer progression by a cell-autonomous mechanism. Nature 1999, 397, 530–534. [Google Scholar] [CrossRef]
- Durnian, J.M.; Stewart, R.M.; Tatham, R.; Batterbury, M.; Kaye, S.B. Cyclosporin-A associated malignancy. Clin. Ophthalmol. 2007, 1, 421–430. [Google Scholar]
- McGurgan, I.J.; McGuigan, C. Nonmelanoma skin cancer risk awareness in azathioprine-treated myasthenia gravis patients. Brain Behav. 2015, 5, e00396. [Google Scholar] [CrossRef]
- Cherikh, W.S.; Kauffman, H.M.; McBride, M.A.; Maghirang, J.; Swinnen, L.J.; Hanto, D.W. Association of the type of induction immunosuppression with posttransplant lymphoproliferative disorder, graft survival, and patient survival after primary kidney transplantation1. Transplantation 2003, 76, 1289–1293. [Google Scholar] [CrossRef] [PubMed]
- Bouvy, A.P.; Kho, M.M.; Klepper, M.; Litjens, N.H.; Betjes, M.G.; Weimar, W.; Baan, C.C. Kinetics of homeostatic proliferation and thymopoiesis after rATG induction therapy in kidney transplant patients. Transplantation 2013, 96, 904–913. [Google Scholar] [CrossRef] [PubMed]
- Müller, T.F.; Grebe, S.O.; Neumann, M.C.; Heymanns, J.; Radsak, K.; Sprenger, H.; Lange, H. Persistent long-term changes in lymphocyte subsets induced by polyclonal antibodies1. Transplantation 1997, 64, 1432–1437. [Google Scholar] [CrossRef] [PubMed]
- Crepin, T.; Carron, C.; Roubiou, C.; Gaugler, B.; Gaiffe, E.; Simula-Faivre, D.; Ferrand, C.; Tiberghien, P.; Chalopin, J.M.; Moulin, B.; et al. ATG-induced accelerated immune senescence: Clinical implications in renal transplant recipients. Am. J. Transplant. 2015, 15, 1028–1038. [Google Scholar] [CrossRef] [PubMed]
- Mossmann, D.; Park, S.; Hall, M.N. mTOR signalling and cellular metabolism are mutual determinants in cancer. Nat. Rev. Cancer 2018, 18, 744–757. [Google Scholar] [CrossRef]
- Grulich, A.E.; Van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef]
- Wong, G.; Howard, K.; Tong, A.; Craig, J.C. Cancer screening in people who have chronic disease: The example of kidney disease. Semin Dial. 2011, 24, 72–78. [Google Scholar] [CrossRef]
- Curry, S.J.; Krist, A.H.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; Kubik, M.; et al. Screening for cervical cancer: US Preventive Services Task Force recommendation statement. JAMA 2018, 320, 674–686. [Google Scholar] [CrossRef]
- Wong, G.; Howard, K.; Chapman, J.R.; Craig, J.C. Cost-effectiveness of breast cancer screening in women on dialysis. Am J Kidney Dis. 2008, 52, 916–929. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Zhao, Y.; Canney, M.; Atiquzzaman, M.; Keown, P.; Levin, A.; Barbour, S. Are patients with primary glomerular disease at increased risk of malignancy? Nephrol. Dial. Transplant. 2023, 9, gfad261. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Chapman, J.R.; Craig, J.C. Cancer screening in renal transplant recipients: What is the evidence? Clin. J. Am. Soc. Nephrol. 2008, 3 (Suppl. 2), S87–S100. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Howard, K.; Webster, A.C.; Chapman, J.R.; Craig, J.C. Screening for renal cancer in recipients of kidney transplants. Nephrol. Dial. Transplant 2011, 26, 1729–1739. [Google Scholar] [CrossRef] [PubMed]
- Elserwy, N.A.; Lotfy, E.E.; Fouda, M.A.; Mahmoud, M.I.; Donia, A.F.; Mashaly, M.E.; Abbas, M.H.; Abuelmagd, M.M.; Abouelenein, R.K.; Ismail, M.I.; et al. Postrenal transplant malignancy: Incidence, risk factors, and prognosis. Saudi J. Kidney Dis. Transplant. 2017, 28, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Foroushani, A.R.; Salesi, M.; Rostami, Z.; Mehrazmay, A.R.; Mohammadi, J.; Einollahi, B.; Eshraghian, M.R. Risk Factors of Graft Survival After Diagnosis of Post-kidney Transplant Malignancy: Using Cox Proportional Hazard Model. Iran. Red Crescent Med. J. 2015, 17, e20281. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No DPTM (n = 885) | DPTM (n = 78) | Total (n = 963) | p-Value |
|---|---|---|---|---|
| Age (years); mean (SD) | 46.8 (15.3) | 53.0 (13.6) | 47.3 (15.2) | <0.001 |
| Gender male | 541 (61.1%) | 56 (71.8%) | 597 (62.0%) | 0.063 |
| Pre-transplant BMI; mean (SD) | 27.1 (8.0) | 26.8 (5.2) | 27.1 (7.8) | 0.785 |
| Ethnicity | 0.421 | |||
| White | 715 (80.8%) | 69 (88.5%) | 784 (81.4%) | |
| Black | 18 (2.0%) | 1 (1.3%) | 19 (2.0%) | |
| Asian | 129 (14.6%) | 7 (9.0%) | 136 (14.1%) | |
| Other | 23 (2.6%) | 1 (1.3%) | 24 (2.5%) | |
| Smoking history | ||||
| Non-smoker | 700 (85.9%) | 64 (87.7%) | 764 (86.0%) | 0.674 |
| Current smoker | 115 (14.1%) | 9 (12.3%) | 124 (14.0%) | |
| Primary aetiology of kidney disease | 0.103 | |||
| ADPKD | 120 (13.6%) | 6 (7.7%) | 126 (13.1%) | |
| Glomerulonephritis | 238 (26.9%) | 30 (38.5%) | 268 (27.8%) | |
| Diabetic kidney disease | 113 (12.8%) | 8 (10.3%) | 121 (12.6%) | |
| Hypertensive kidney disease | 65 (7.3%) | 3 (3.8%) | 68 (7.1%) | |
| Reflux/chronic pyelonephritis | 130 (14.7%) | 7 (9.0%) | 137 (14.2%) | |
| Unknown | 130 (14.7%) | 12 (15.4%) | 142 (14.7%) | |
| Other | 89 (10.1%) | 12 (15.4%) | 101 (10.5%) | |
| Pre-transplant co-morbidities | ||||
| Diabetes mellitus | 153 (17.3%) | 14 (17.9%) | 167 (17.3%) | 0.883 |
| Cardiovascular disease | 202 (22.8%) | 12 (15.4%) | 214 (22.2%) | 0.130 |
| Duration of pre-transplant KRT (months), mean (SD) | 24.7 (33.6) | 25.7(44.3) | 24.8 (34.6) | 0.445 |
| Details relating to transplant procedure | ||||
| Transplant number; mean (SD) | 1.15 (0.42) | 1.12 (0.32) | 1.14 (0.41) | 0.520 |
| Pre-emptive transplant | 263 (31.2%) | 21 (28.0%) | 284 (30.9%) | 0.566 |
| Organ donor status | ||||
| DD | 624 (70.7%) | 60 (76.9%) | 684 (71.2%) | 0.242 |
| LD | 259 (29.3%) | 18 (23.1%) | 277 (28.8%) | |
| Total HLA mismatch; mean (SD) | 2.4 (1.4) | 2.4 (1.5) | 2.4 (1.4) | 0.763 |
| Total ischaemia time; mean (SD) | 12.8 (7.6) | 13.0 (7.0) | 12.8 (7.6) | 0.770 |
| History of acute rejection | 100 (11.3%) | 7 (9.0%) | 107 (11.1%) | 0.531 |
| Post-transplant diabetes | 147 (16.6%) | 10 (12.8%) | 157 (16.3%) | 0.385 |
| Primary immunosuppression | ||||
| Tacrolimus | 788 (90.1%) | 66 (88.0%) | 854 (89.9%) | 0.516 |
| Cyclosporine | 77 (8.8%) | 7 (9.3%) | 84 (8.8%) | |
| Sirolimus | 10 (1.1%) | 2 (2.7%) | 12 (1.3%) | |
| Mycophenolic acid | 683 (78.1%) | 49 (64.5%) | 732 (77.1%) | |
| Azathioprine | 107 (12.2%) | 16 (21.1%) | 123 (12.9%) | |
| No anti-metabolite | 84 (9.6%) | 11 (14.5%) | 95 (10.0%) | |
| Steroid maintenance | 0.027 | |||
| <2 weeks | 466 (53.0%) | 30 (38.5%) | 496 (51.8%) | |
| 2 weeks–6 months | 22 (2.5%) | 1 (1.3%) | 23 (2.4%) | |
| >6 months | 392 (44.5%) | 47 (60.3%) | 439 (45.8%) | |
| CMV status | ||||
| Donor (D) CMV negative | 340 (46.4%) | 21 (33.9%) | 361 (45.5%) | 0.056 |
| Recipient (R) CMV negative | 436 (59.0%) | 33 (55.9%) | 469 (58.8%) | 0.645 |
| Combined donor and recipient CMV status | 0.097 | |||
| CMV D + R- | 127 (18.4%) | 16 (29.1%) | 143 (19.1%) | |
| CMV D-R- | 162 (23.4%) | 9 (16.4%) | 171 (22.9%) | |
| CMV D + R+ | 241 (34.8%) | 22 (40.0%) | 263 (35.2%) | |
| CMV D-R+ | 162 (23.4%) | 8 (14.5%) | 170 (22.8%) | |
| Virology status | ||||
| CMV viremia | 120 (13.6%) | 13 (16.7%) | 133 (13.8%) | 0.446 |
| EBV viremia | 100 (11.3%) | 23 (29.5%) | 123 (12.8%) | <0.001 |
| Polyoma viremia | 111 (12.5%) | 6 (7.7%) | 117 (12.1%) | 0.209 |
| Any DNA virus infection | 258 (29.2%) | 30 (38.5%) | 288 (29.9%) | 0.085 |
| Biochemical parameters | ||||
| Tacrolimus level (ng/mL); Mean (SD) | 5.53 (2.74) | 5.40 (3.34) | 5.53 (2.79) | 0.704 |
| Baseline eGFR (mL/min/1.73 m2); median (IQR) | 51.0(40.0–65.0) | 47(37.7–58.0) | 51.0 (40.0–64.0) | 0.072 |
| eGFR slope (mL/min/1.73 m2/year); mean (SD) | −1.35 (4.05) | −0.90 (2.44) | −1.31 (3.94) | 0.371 |
| Haemoglobin (g/L); mean (SD) | 126.6 (19.5) | 120.8 (17.1) | 126.1 (19.4) | 0.015 |
| uPCR (mg/mmol); median (IQR) | 23.8(11.6–70.8) | 26.7(16.3–53.1) | 24.2(11.8–68.4) | 0.712 |
| CRP (mg/dL); median (IQR) | 12.6(4.0–32.6) | 31.3(13.6–50.2) | 14.0(4.1–34.4) | <0.001 |
| Outcomes | ||||
| Death-censored graft loss | 78 (8.8%) | 10 (12.8%) | 88 (9.1%) | 0.239 |
| Death with functioning graft | 149 (16.8%) | 33 (42.3%) | 182 (18.9%) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chukwu, C.A.; Wu, H.H.L.; Pullerits, K.; Garland, S.; Middleton, R.; Chinnadurai, R.; Kalra, P.A. Incidence, Risk Factors, and Outcomes of De Novo Malignancy following Kidney Transplantation. J. Clin. Med. 2024, 13, 1872. https://doi.org/10.3390/jcm13071872
Chukwu CA, Wu HHL, Pullerits K, Garland S, Middleton R, Chinnadurai R, Kalra PA. Incidence, Risk Factors, and Outcomes of De Novo Malignancy following Kidney Transplantation. Journal of Clinical Medicine. 2024; 13(7):1872. https://doi.org/10.3390/jcm13071872
Chicago/Turabian StyleChukwu, Chukwuma A., Henry H.L. Wu, Kairi Pullerits, Shona Garland, Rachel Middleton, Rajkumar Chinnadurai, and Philip A. Kalra. 2024. "Incidence, Risk Factors, and Outcomes of De Novo Malignancy following Kidney Transplantation" Journal of Clinical Medicine 13, no. 7: 1872. https://doi.org/10.3390/jcm13071872
APA StyleChukwu, C. A., Wu, H. H. L., Pullerits, K., Garland, S., Middleton, R., Chinnadurai, R., & Kalra, P. A. (2024). Incidence, Risk Factors, and Outcomes of De Novo Malignancy following Kidney Transplantation. Journal of Clinical Medicine, 13(7), 1872. https://doi.org/10.3390/jcm13071872