

Evaluation of the Efficacy and Safety of Quetiapine in the Treatment of Delirium in Adult ICU Patients: A Retrospective Comparative Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
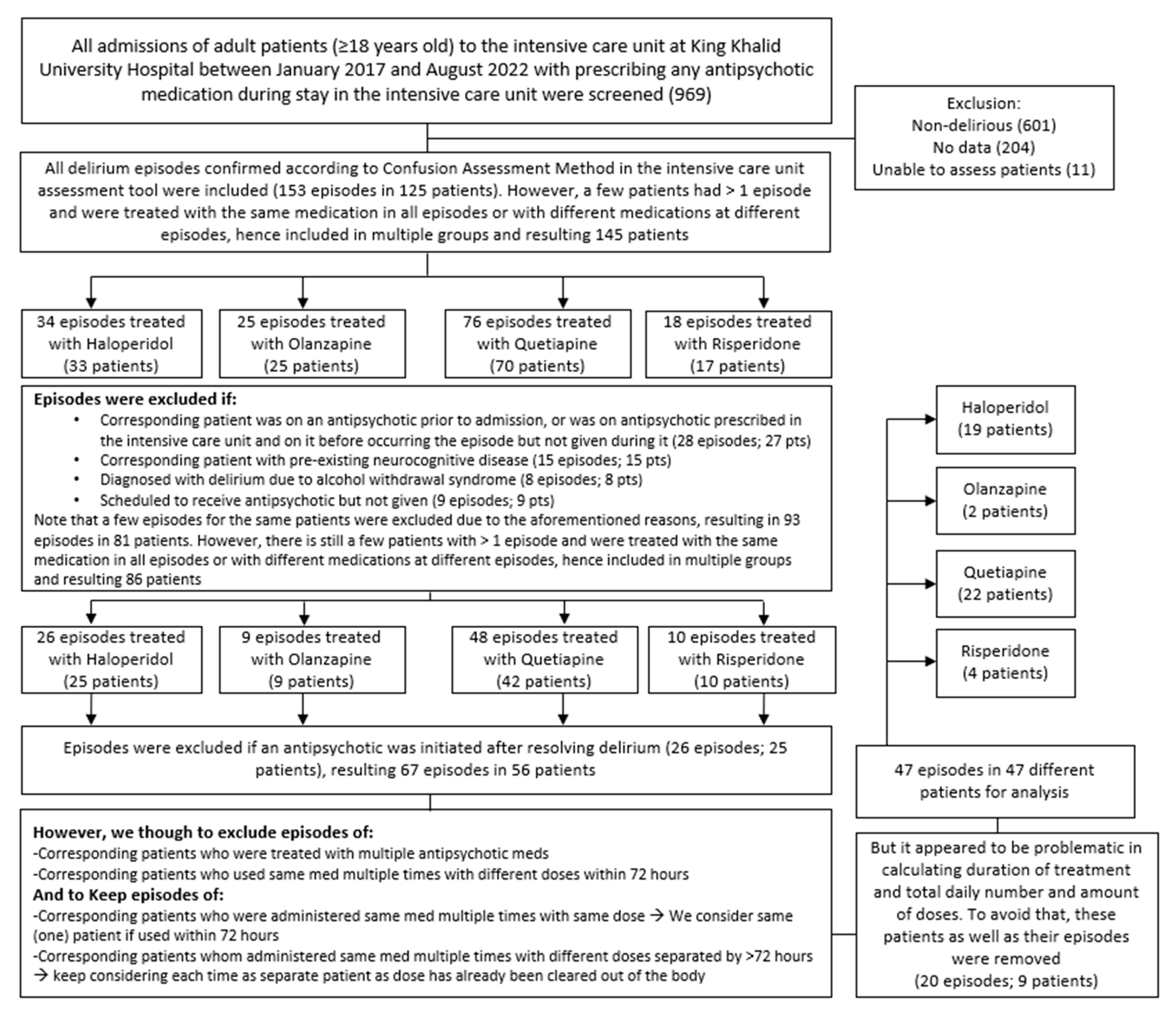
2.2. Participants
2.3. Data Collection
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Primary Outcomes
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Delirium Association; American Delirium Society. The DSM-5 criteria, level of arousal and delirium diagnosis: Inclusiveness is safer. BMC Med. 2014, 12, 141. [Google Scholar] [CrossRef]
- Siddiqi, N.; House, A.O.; Holmes, J.D. Occurrence and outcome of delirium in medical in-patients: A systematic literature review. Age Ageing 2006, 35, 350–364. [Google Scholar] [CrossRef]
- Burry, L.; Mehta, S.; Perreault, M.M.; Luxenberg, J.S.; Siddiqi, N.; Hutton, B.; Fergusson, D.A.; Bell, C.; Rose, L. Antipsychotics for treatment of delirium in hospitalised non-ICU patients. Cochrane Database Syst. Rev. 2018, 6, CD005594. [Google Scholar] [CrossRef] [PubMed]
- Hayhurst, C.J.; Pandharipande, P.P.; Hughes, C.G. Intensive Care Unit Delirium: A Review of Diagnosis, Prevention, and Treatment. Anesthesiology 2016, 125, 1229–1241. [Google Scholar] [CrossRef] [PubMed]
- Barr, J.; Fraser, G.L.; Puntillo, K.; Ely, E.W.; Gélinas, C.; Dasta, J.F.; Davidson, J.E.; Devlin, J.W.; Kress, J.P.; Joffe, A.M.; et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit. Care Med. 2013, 41, 263–306. [Google Scholar] [CrossRef] [PubMed]
- Kukolja, J.; Kuhn, J. SOP: Treatment of delirium. Neurol. Res. Pract. 2021, 3, 12. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.; Gautam, S.; Margolin, R.; Francis, J.; May, L.; Speroff, T.; Truman, B.; Dittus, R.; Bernard, G.; Inouye, S. The impact of delirium in the intensive care unit on hospital length of stay. Intensive Care Med. 2001, 27, 1892–1900. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W.; Shintani, A.; Truman, B.; Speroff, T.; Gordon, S.M.; Harrell, F.E., Jr.; Inouye, S.K.; Bernard, G.R.; Dittus, R.S. Delirium as a Predictor of Mortality in Mechanically Ventilated Patients in the Intensive Care Unit. JAMA 2004, 291, 1753–1762. [Google Scholar] [CrossRef] [PubMed]
- Lat, I.; McMillian, W.; Taylor, S.; Janzen, J.M.; Papadopoulos, S.; Korth, L.; Ehtisham, A.; Nold, J.; Agarwal, S.; Azocar, R.; et al. The impact of delirium on clinical outcomes in mechanically ventilated surgical and trauma patients. Crit. Care Med. 2009, 37, 1898–1905. [Google Scholar] [CrossRef]
- Schwartz, T.L.; Masand, P.S. The role of atypical antipsychotics in the treatment of delirium. Psychosomatics 2002, 43, 171–174. [Google Scholar] [CrossRef]
- Delirium: Prevention, Diagnosis and Management in Hospital and Long-Term Care; National Institute for Health and Care Excellence (NICE): London, UK, 2023.
- Herzig, S.J.; Rothberg, M.B.; Guess, J.R.; Gurwitz, J.H.; Marcantonio, E.R. Antipsychotic medication utilization in nonpsychiatric hospitalizations. J. Hosp. Med. 2016, 11, 543–549. [Google Scholar] [CrossRef]
- Yoon, H.J.; Park, K.M.; Choi, W.J.; Choi, S.-H.; Park, J.-Y.; Kim, J.-J.; Seok, J.-H. Efficacy and safety of haloperidol versus atypical antipsychotic medications in the treatment of delirium. BMC Psychiatry 2013, 13, 240. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [PubMed]
- Sailer, C.F.; Salama, A.I. Seroquel: Biochemical Profile of a Potential Atypical Antipsychotic; Springer: Berlin/Heidelberg, Germany, 1993; Volume 112. [Google Scholar]
- Hawkins, S.B.; Bucklin, M.; Muzyk, A.J. Quetiapine for the treatment of delirium. J. Hosp. Med. 2013, 8, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Roberts, R.J.; Fong, J.J.; Skrobik, Y.; Riker, R.R.; Hill, N.S.; Robbins, T.; Garpestad, E. Efficacy and safety of quetiapine in critically ill patients with delirium: A prospective, multicenter, randomized, double-blind, placebo-controlled pilot study. Crit. Care Med. 2010, 38, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Maneeton, B.; Maneeton, N.; Srisurapanont, M.; Chittawatanarat, K. Quetiapine versus haloperidol in the treatment of delirium: A double-blind, randomized, controlled trial. Drug Des. Dev. Ther. 2013, 7, 657–667. [Google Scholar] [CrossRef]
- Rivière, J.; van der Mast, R.C.; Vandenberghe, J.; Van Den Eede, F. Efficacy and Tolerability of Atypical Antipsychotics in the Treatment of Delirium: A Systematic Review of the Literature. Psychosomatics 2019, 60, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W.; Inouye, S.K.; Bernard, G.R.; Gordon, S.; Francis, J.; May, L.; Truman, B.; Speroff, T.; Gautam, S.; Margolin, R.; et al. Delirium in mechanically ventilated patients: Validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA 2001, 286, 2703–2710. [Google Scholar] [CrossRef] [PubMed]
- Zion, D.; Gillam, L.; Loff, B. The Declaration of Helsinki, CIOMS and the ethics of research on vulnerable populations. Nat. Med. 2000, 6, 615–617. [Google Scholar] [CrossRef]
- General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Sessler, C.N.; Gosnell, M.S.; Grap, M.J.; Brophy, G.M.; O’Neal, P.V.; Keane, K.A.; Tesoro, E.P.; Elswick, R.K. The Richmond Agitation-Sedation Scale: Validity and reliability in adult intensive care unit patients. Am. J. Respir Crit. Care Med. 2002, 166, 1338–1344. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Cook IA: GuidelineWatch: Practice Guideline for the Treatment of Patients with Delirium; American Psychiatric Association: Arlington, VA, USA, 2004; Available online: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm (accessed on 20 November 2023).
- Trzepacz, P.; Breitbart, W.; Franklin, J.; Levenson, J.; Martini, D.R.; Wang, P. Practice guideline for the treatment of patients with delirium. American Psychiatric Association. Am. J. Psychiatry 1999, 156 (Suppl. S5), 1–20. [Google Scholar]
- Canadian Coalition for Seniors’ Mental Health (CCSMH). National Guidelines for Seniors’ Mental Health—The Assessment and Treatment of Delirium; Canadian Coalition for Seniors’ Mental Health: Toronto, ON, Canada, 2006. [Google Scholar]
- Girard, T.D.; Exline, M.C.; Carson, S.S.; Hough, C.L.; Rock, P.; Gong, M.N.; Douglas, I.S.; Malhotra, A.; Owens, R.L.; Feinstein, D.J.; et al. Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness. N. Engl. J. Med. 2018, 379, 2506–2516. [Google Scholar] [CrossRef]
- Andersen-Ranberg, N.C.; Poulsen, L.M.; Perner, A.; Wetterslev, J.; Estrup, S.; Hästbacka, J.; Morgan, M.; Citerio, G.; Caballero, J.; Lange, T.; et al. Haloperidol for the Treatment of Delirium in ICU Patients. N. Engl. J. Med. 2022, 387, 2425–2435. [Google Scholar] [CrossRef]
- Bleck, T.P. Dopamine antagonists in ICU delirium. N. Engl. J. Med. 2018, 379, 2569–2570. [Google Scholar] [CrossRef] [PubMed]
- Luz, M.; Brandão Barreto, B.; de Castro, R.E.V.; Salluh, J.; Dal-Pizzol, F.; Araujo, C.; De Jong, A.; Chanques, G.; Myatra, S.N.; Tobar, E.; et al. Practices in sedation, analgesia, mobilization, delirium, and sleep deprivation in adult intensive care units (SAMDS-ICU): An international survey before and during the COVID-19 pandemic. Ann. Intensive Care 2022, 12, 9. [Google Scholar] [CrossRef]
- Kishi, T.; Hirota, T.; Matsunaga, S.; Iwata, N. Antipsychotic medications for the treatment of delirium: A systematic review and meta-analysis of randomised controlled trials. J. Neurol. Neurosurg. Psychiatry 2016, 87, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Hatta, K.; Kishi, Y.; Wada, K.; Odawara, T.; Takeuchi, T.; Shiganami, T.; Tsuchida, K.; Oshima, Y.; Uchimura, N.; Akaho, R.; et al. Antipsychotics for delirium in the general hospital setting in consecutive 2453 inpatients: A prospective observational study. Int. J. Geriatr. Psychiatry 2014, 29, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Neufeld, K.J.; Yue, J.; Robinson, T.N.; Inouye, S.K.; Needham, D.M. Antipsychotic Medication for Prevention and Treatment of Delirium in Hospitalized Adults: A Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2016, 64, 705–714. [Google Scholar] [CrossRef]
- Tahir, T.A.; Eeles, E.; Karapareddy, V.; Muthuvelu, P.; Chapple, S.; Phillips, B.; Adyemo, T.; Farewell, D.; Bisson, J.I. A randomized controlled trial of quetiapine versus placebo in the treatment of delirium. J. Psychosom. Res. 2010, 69, 485–490. [Google Scholar] [CrossRef]
- Abraham, M.P.; Hinds, M.; Tayidi, I.; Jeffcoach, D.R.; Corder, J.M.; Hamilton, L.A.; Lawson, C.M.; Bollig, R.W.; Heidel, R.E.; Daley, B.J.; et al. Quetiapine for delirium prophylaxis in high-risk critically ill patients. Surgeon 2021, 19, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Thanapluetiwong, S.; Ruangritchankul, S.; Sriwannopas, O.; Chansirikarnjana, S.; Ittasakul, P.; Ngamkala, T.; Sukumalin, L.; Charernwat, P.; Saranburut, K.; Assavapokee, T. Efficacy of quetiapine for delirium prevention in hospitalized older medical patients: A randomized double-blind controlled trial. BMC Geriatr. 2021, 21, 215. [Google Scholar] [CrossRef] [PubMed]
- Michaud, C.J.; Bullard, H.M.; Harris, S.A.; Thomas, W.L. Impact of Quetiapine Treatment on Duration of Hypoactive Delirium in Critically Ill Adults: A Retrospective Analysis. Pharmacotherapy 2015, 35, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Brunton, L.L.; Chabner, B.A.; Knollmann, B.C. (Eds.) Goodman & Gilman’s: The Pharmacological Basis of Therapeutics, 12e; McGraw Hill: New York, NY, USA, 2015; Available online: https://accessmedicine.mhmedical.com/content.aspx?bookid=1613§ionid=102124003 (accessed on 27 December 2023).
- Mangan, K.C.; McKinzie, B.P.; Deloney, L.P.; Leon, S.M.; Eriksson, E.A. Evaluating the risk profile of quetiapine in treating delirium in the intensive care adult population: A retrospective review. J. Crit. Care 2018, 47, 169–172. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All | Haloperidol (n = 19) | Olanzapine (n = 2) | Quetiapine (n = 22) | Risperidone (n = 4) | p-Value |
|---|---|---|---|---|---|---|
| Gender; n (%) | ||||||
| Male | 40 (85.1) | 16 (40) | 2 (5) | 18 (45) | 4 (10) | |
| Female | 7 (14.9) | 3 (42.9) | 0 | 4 (57.1) | 0 | 0.741 |
| Age (median (IQR)) * | 53 (40.5) | 59 (31) | 54 (4) | 35 (37.75) | 90 (25) | 0.157 |
| BMI (median (IQR)) * | 27.5 (8.8) | 30.26 (9.4) | 31.4 (1.28) | 27.3 (8.27) | 24 (2.3) | 0.027 |
| Reason for ICU admission | ||||||
| -Cardiovascular | 20 (42.6) | 11 (55) | 1 (5) | 5 (25) | 3 (15) | 0.068 |
| -Respiratory | 8 (17) | 0 | 1 (12.5) | 7 (87.5) | 0 | 0.022 |
| -Trauma | 16 (34) | 5 (31.3) | 0 | 10 (62.5) | 1 (6.3) | 0.398 |
| -Other | 7 (14.9) | 3 (42.9) | 0 | 3 (42.9) | 1 (14.3) | 0.870 |
| Comorbidities; n (%) | ||||||
| -DM | 22 (46.8) | 11 (50) | 1 (4.5) | 7 (31.8) | 3 (13.6) | 0.240 |
| -HTN | 20 (42.6) | 10 (50) | 1 (5) | 6 (30) | 3 (15) | 0.199 |
| -Stroke | 2 (4.3) | 1 (50) | 0 | 1 (50) | 0 | 0.956 |
| -CHF | 9 (19.1) | 5 (55.6) | 0 | 2 (22.2) | 2 (22.2) | 0.172 |
| -IHD | 11 (23.4) | 7 (63.6) | 0 | 1 (9.1) | 3 (27.3) | 0.005 |
| -a-fib | 4 (8.5) | 2 (50) | 0 | 2 (50) | 0 | 0.881 |
| -Asthma | 4 (8.5) | 3 (75) | 0 | 1 (25) | 0 | 0.513 |
| -CKD | 9 (19.1) | 5 (55.6) | 0 | 3 (33.3) | 1 (11.1) | 0.654 |
| -Seizure/neurological disease | 1 (2.1) | 0 | 1 (100) | 0 | 0 | <0.001 |
| -History of psychiatric disease | 2 (4.3) | 1 (50) | 0 | 1 (50) | 0 | 0.956 |
| -Consumption of alcohol | 3 (6.4) | 1 (33.3) | 0 | 2 (66.7) | 0 | 0.869 |
| -Smoking history | 10 (21.3) | 4 (40) | 1 (10) | 3 (30) | 2 (20) | 0.293 |
| -Cancer | 4 (8.5) | 1 (25) | 0 | 3 (75) | 0 | 0.669 |
| -Other comorbidities | 8 (17) | 1 (12.5) | 0 | 5 (62.5) | 2 (25) | 0.119 |
| Variable | Haloperidol (n = 19) | Olanzapine (n = 2) | Quetiapine (n = 22) | Risperidone (n = 4) | p-Value |
|---|---|---|---|---|---|
| APACHE II score (median (IQR)) * | 17 (11.5) | 21.5 (3.5) | 15.5 (9.5) | 18 (2.75) | 0.453 |
| GCS (median (IQR)) | 11 (11.5) | 4 (1) | 12.5 (10.25) | 14.5 (2.75) | 0.387 |
| Charlson Comorbidity Index (median (IQR)) | 5 (6.5) | 1 (1) | 0.5 (4) | 7 (4) | 0.07 |
| Baseline QTc (median (IQR)) * | 438.5 (75.8) | 442 (0) | 445.5 (36.25) | 489 (22) | 0.143 |
| Mechanical ventilation; n (%) | 5 (35.7) | 1 (7.1) | 6 (42.9) | 2 (14.3) | 0.718 |
| Estimated 10-year survival % (median % (IQR)) | 21 (97) | 94 (4) | 93 (69) | 1 (26) | 0.588 |
| RASS score during delirium occurrence (median (IQR)) * | 1.5 (2) | 2 (1) | 1.5 (1.25) | 1 (1) | 0.837 |
| Delirium incidence; n (%) | |||||
| -Hypoactive | 4 (44.4) | 0 | 4 (44.4) | 1 (11.1) | 0.892 |
| -Hyperactive | 15 (39.5) | 2 (5.3) | 18 (47.4) | 3 (7.9) | |
| Neurological or neurosurgical condition; n (%) | 3 (33.3) | 0 | 6 (66.7) | 0 | 0.438 |
| Antipsychotic | p-Value | ||||
|---|---|---|---|---|---|
| Variable | Haloperidol (n = 19) | Olanzapine (n = 2) | Quetiapine (n = 22) | Risperidone (n = 4) | |
| Duration of antipsychotic use in the ICU [days; median (IQR)] | 3 (2.5) | 12.5 (0.5) | 7.5 (11.5) | 2.5 (3.25) | 0.007 # |
| Patients on antipsychotics after ICU admission and before the onset of delirium (%) | 3 (21.4) | 1 (7.1) | 10 (71.4) | 0 | 0.092 |
| Time required to resolve delirium while in the ICU and on medication [h; median (IQR)] | 23 (28) | 36 (10) | 12 (21.5) | 13 (13.75) | 0.115 |
| Use of antipsychotics; n (%) | |||||
| -Before and during delirium’s occurrence only | 0 | 0 | 0 | 0 | 0.110 |
| -During delirium’s occurrence only | 10 (66.7) | 0 | 3 (20) | 2 (13.3) | |
| -During and after delirium’s occurrence | 6 (31.6) | 1 (5.3) | 10 (52.6) | 2 (10.5) | |
| -Before, during, and after delirium’s occurrence | 3 (23.1) | 1 (7.7) | 9 (69.2) | 0 | |
| Dose change of antipsychotic; n (%) * | |||||
| -No change | 7 (33.3) | 2 (9.5) | 10 (47.6) | 2 (9.5) | 0.493 |
| -Increase | 1 (11.1) | 0 | 8 (88.9) | 0 | |
| -Decrease | 1 (50) | 0 | 1 (50) | 0 | |
| Variable | Haloperidol (n = 19) | Olanzapine (n = 2) | Quetiapine (n = 22) | Risperidone (n = 4) | p-Value |
|---|---|---|---|---|---|
| Length of stay in ICU [days; median (IQR)] | 9 (11) | 15.5 (7.5) | 9.5 (4.75) | 4 (5.75) | 0.834 |
| Length of stay in hospital [days; median (IQR)] | 27 (21) | 42 (26) | 20.5 (22) | 16 (23) | 0.388 |
| % of time spent in delirium in ICU [median % (IQR)] | 10 (11.85) | 21.1 (16.4) | 6.25 (12.3) | 19.2 (35.4) | 0.240 |
| Delirium-free days [days; median (IQR)] | 8 (10.13) | 13.5 (8.45) | 9.3 (6.67) | 3.2 (6.8) | 0.75 |
| Ventilator-free days [days; median (IQR)] | 6 (4) | 2 (0) | 4 (5.5) | 6 (4) | 0.58 |
| New ICU mortality; n (%) | 1 (25) | 0 | 2 (50) | 1 (25) | 0.604 |
| New non-ICU mortality; n (%) | 1 (33.3) | 0 | 2 (66.7) | 0 | 0.869 |
| Overall mortality; n (%) | 2 (28.6) | 0 | 4 (57.1) | 1 (14.3) | 0.766 |
| Use of opiates; n (%) | 11 (44) | 2 (8) | 9 (36) | 3 (12) | 0.259 |
| Duration of opiate use; [days; median (IQR)] * | 1.5 (1) | 1.5 (0.5) | 1 (0) | 1.5 (0.5) | 0.666 |
| Use of BDZ; n (%) | 9 (45) | 1 (5) | 7 (35) | 3 (15) | 0.394 |
| Use of dexmedetomidine; n (%) | 5 (31.3) | 1 (6.3) | 10 (62.5) | 0 | 0.254 |
| Use of propofol; n (%) | 3 (75) | 0 | 1 (25) | 0 | 0.513 |
| Use of clonidine; n (%) | 3 (25) | 0 | 9 (75) | 0 | 0.125 |
| Highest QTC while on antipsychotics [median (IQR)] * | 466 (52) | 421 (0) | 477 (65) | 527 (76.5) | 0.304 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alghadeer, S.; Almesned, R.S.; Alshehri, E.A.; Alwhaibi, A. Evaluation of the Efficacy and Safety of Quetiapine in the Treatment of Delirium in Adult ICU Patients: A Retrospective Comparative Study. J. Clin. Med. 2024, 13, 802. https://doi.org/10.3390/jcm13030802
Alghadeer S, Almesned RS, Alshehri EA, Alwhaibi A. Evaluation of the Efficacy and Safety of Quetiapine in the Treatment of Delirium in Adult ICU Patients: A Retrospective Comparative Study. Journal of Clinical Medicine. 2024; 13(3):802. https://doi.org/10.3390/jcm13030802
Chicago/Turabian StyleAlghadeer, Sultan, Rahaf S. Almesned, Emad A. Alshehri, and Abdulrahman Alwhaibi. 2024. "Evaluation of the Efficacy and Safety of Quetiapine in the Treatment of Delirium in Adult ICU Patients: A Retrospective Comparative Study" Journal of Clinical Medicine 13, no. 3: 802. https://doi.org/10.3390/jcm13030802
APA StyleAlghadeer, S., Almesned, R. S., Alshehri, E. A., & Alwhaibi, A. (2024). Evaluation of the Efficacy and Safety of Quetiapine in the Treatment of Delirium in Adult ICU Patients: A Retrospective Comparative Study. Journal of Clinical Medicine, 13(3), 802. https://doi.org/10.3390/jcm13030802