
Efficacy and Safety of Spinal Collagen Mesotherapy in Patients with Chronic Low Back Pain in a Three-Month Follow-Up—Retrospective Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Inclusion Criteria
- –
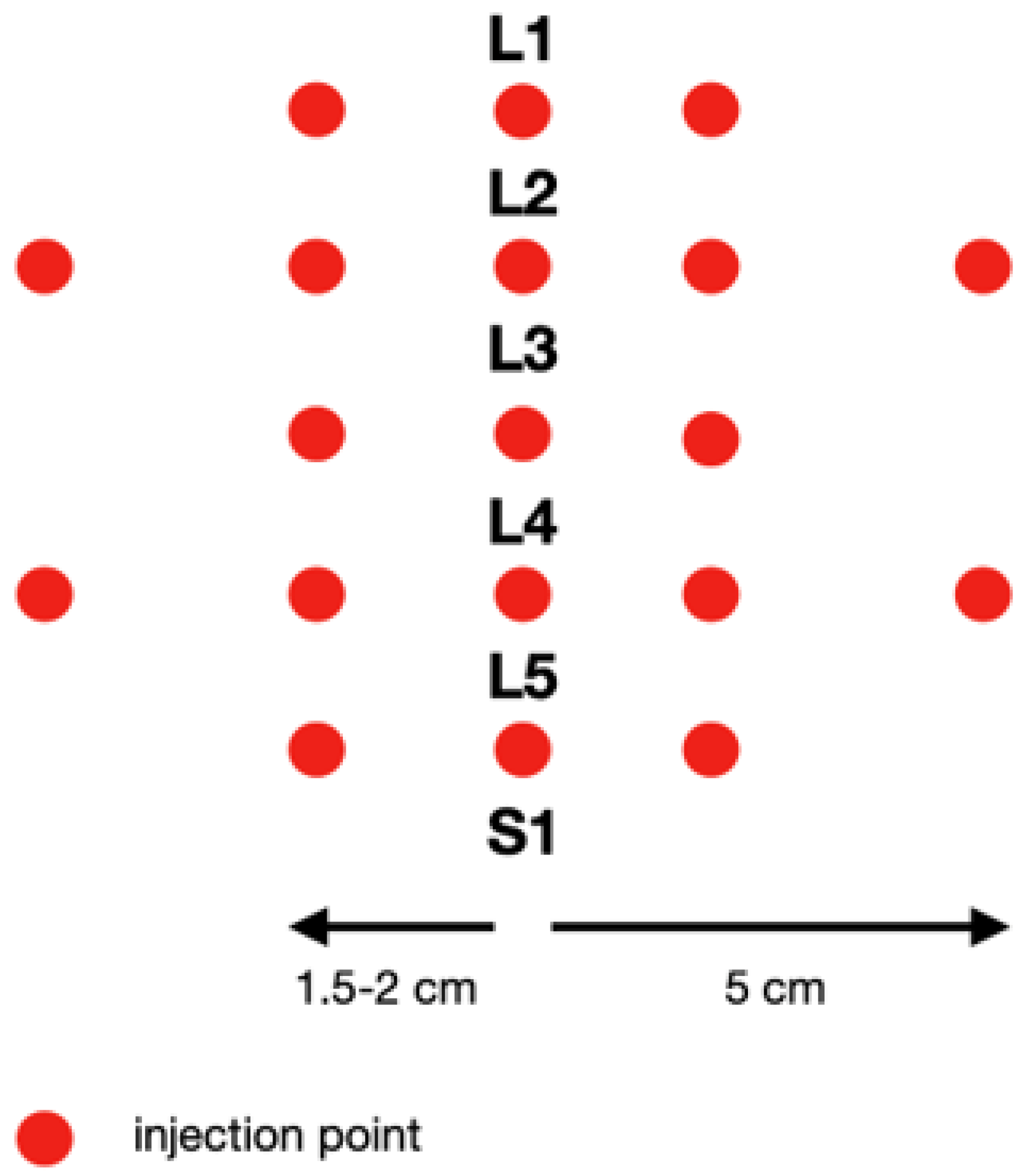
- Pain localized in the triangle area between the posterior superior iliac spine and spinous process of L3, lasting more than three months and increasing during the deep palpation of the area of facet joints, 2–3 cm laterally from spinous processes (in the area of L3/L4 and/or L4/L5 and/or L5/S1;
- –
- No motor or sensory radicular symptoms, which was confirmed in a neurologic examination;
- –
- No lumbar stenosis;
- –
- No other pathologies in the pelvis and lower limbs;
- –
- No allergy to collagen type I or to lignocaine.
2.1.2. Exclusion Criteria
- –
- Lack of appropriate imaging diagnostics;
- –
- Magnetic resonance imaging or computed tomography results (older than six months) confirming tumors, discitis, or spondylolisthesis;
- –
- Pain associated with a systemic disease, e.g., rheumatoid arthritis, fibromyalgia;
- –
- Taking painkillers and/or anti-inflammatory drugs during therapy;
- –
- Prior low back surgery;
- –
- Lack of consent of the patient and/or the guardian to examinations and participation in the program.
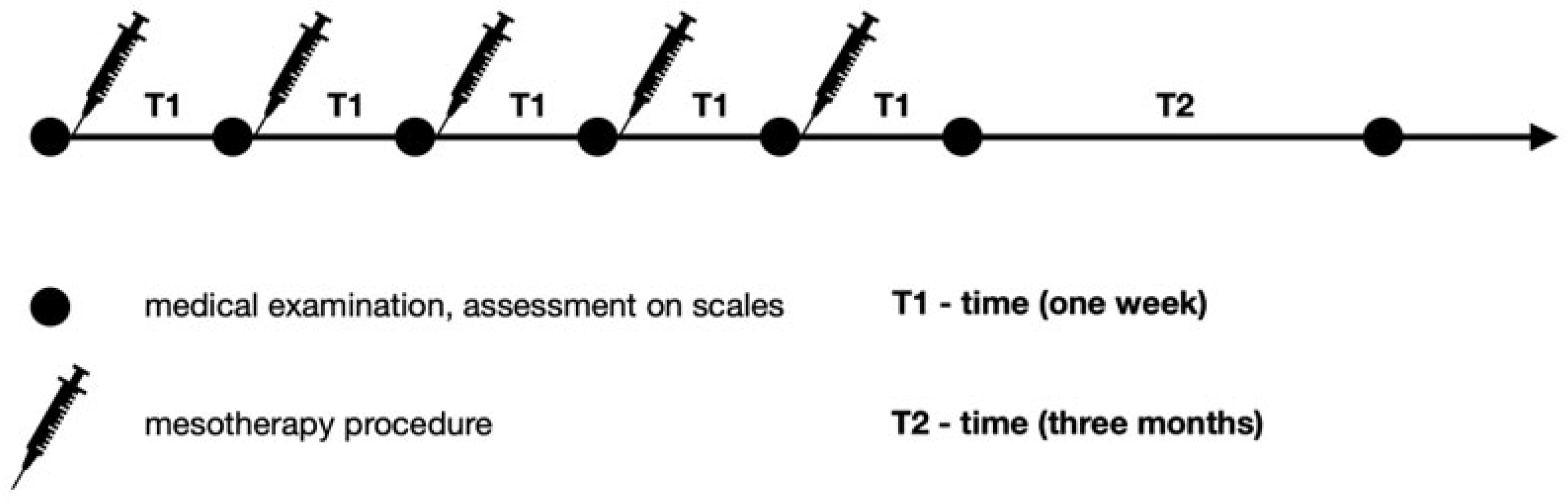
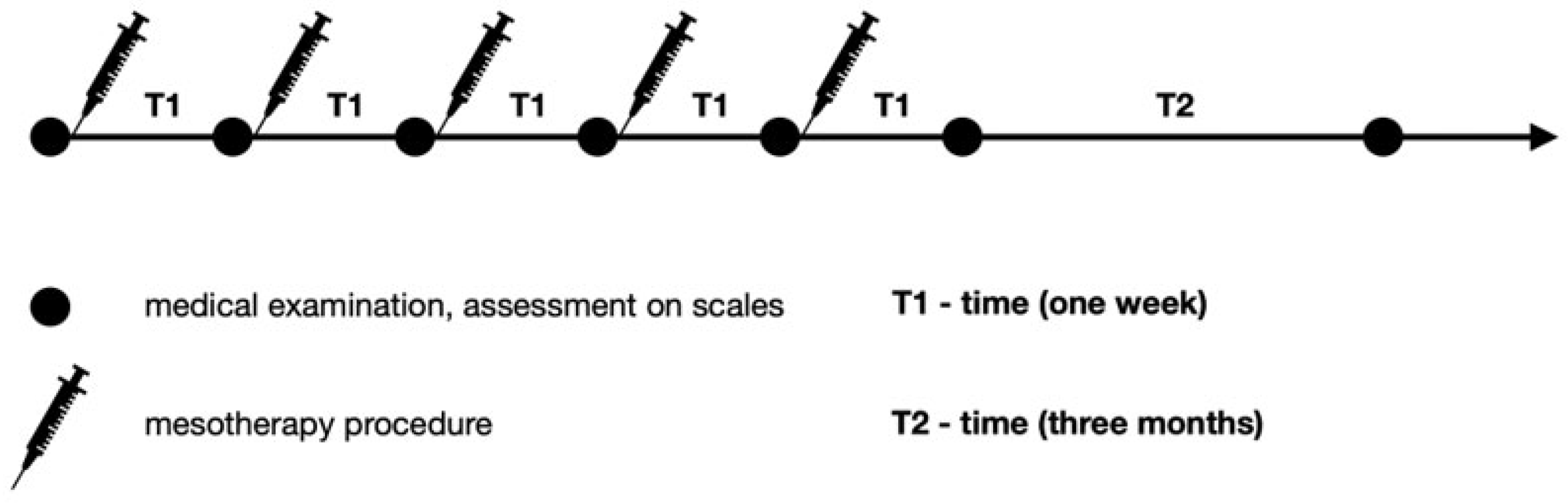
2.2. Study Protocol—Spinal Mesotherapy
2.3. Study Protocol–Assessment on Scales
2.4. Sample Size
2.5. Data Analysis
3. Results
4. Discussion
4.1. Discussion
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602, Erratum in Lancet 2017, 389, e1. [CrossRef]
- Malik, K.M.; Nelson, A.M.; Chiang, T.H.; Imani, F.; Khademi, S.H. The Specifics of Non-specific Low Back Pain: Re-evaluating the Current Paradigm to Improve Patient Outcomes. Anesth. Pain. Med. 2022, 12, e131499. [Google Scholar] [CrossRef] [PubMed]
- Koszela, K.; Krukowska, K.; Woldańska–Okońska, M. Back pain as a lifestyle disease. Pediatr. Med. Rodz. 2017, 13, 344–351. [Google Scholar] [CrossRef]
- Hammi, C.; Schroeder, J.D.; Yeung, B. Trigger Point Injection. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Paolucci, T.; Bellomo, R.G.; Centra, M.A.; Giannandrea, N.; Pezzi, L.; Saggini, R. Mesotherapy in the treatment of musculoskeletal pain in rehabilitation: The state of the art. J. Pain. Res. 2019, 12, 2391–2401. [Google Scholar] [CrossRef]
- Sarkar, R.; Garg, V.K.; Mysore, V. Position paper on mesotherapy. Indian. J. Dermatol. Venereol. Leprol. 2011, 77, 232–237. [Google Scholar] [CrossRef]
- Brauneis, S.; Araimo, F.; Rossi, M.; Russo, D.; Mammuccari, M.; Maggiori, E.; di Marzo, R.; Vellucci, R.; Gori, F.; Bifarini, B.; et al. The role of mesotherapy in the management of spinal pain. A randomized controlled study. Clin. Ter. 2023, 174, 336–342. [Google Scholar] [CrossRef]
- Alves, J.C.; Santos, A.; Jorge, P.; Lafuente, P. A multiple-session mesotherapy protocol for the management of hip osteoarthritis in police working dogs. Am. J. Vet. Res. 2022, 84, ajvr.22.08.0132. [Google Scholar] [CrossRef] [PubMed]
- Kocak, A.O. Intradermal mesotherapy versus systemic therapy in the treatment of musculoskeletal pain: A prospective randomized study. Am. J. Emerg. Med. 2019, 37, 2061–2065. [Google Scholar] [CrossRef]
- Mammucari, M.; Gatti, A.; Maggiori, S.; Sabato, A.F. Role of Mesotherapy in Musculoskeletal Pain: Opinions from the Italian Society of Mesotherapy. Evid. -Based Complement. Altern. Med. 2012, 2012, 436959. [Google Scholar] [CrossRef]
- Mammucari, M.; Gatti, A.; Maggiori, S.; Bartoletti, C.A.; Sabato, A.F. Mesotherapy, definition, rationale and clinical role: A consensus report from the italian society of mesotherapy. Eur. Rev. Med. Pharmacol. Sci. 2011, 15, 682–694. [Google Scholar] [PubMed]
- Laurent, A.; Mistretta, F.; Bottigioli, D.; Dahel, K.; Goujon, C.; Nicolas, J.F.; Hennino, A.; Laurent, P.E. Echographic measurement of skin thickness in adults by high frequency ultrasound to assess the appropriate microneedle length for intradermal delivery of vaccines. Vaccine 2007, 25, 6423–6430. [Google Scholar] [CrossRef] [PubMed]
- Van Mulder, T.J.; de Koeijer, M.; Theeten, H.; Willems, D.; Van Damme, P.; Demolder, M.; De Meyer, G.; Beyers, K.C.; Vankerckhoven, V. High frequency ultrasound to assess skin thickness in healthy adults. Vaccine 2017, 35, 1810–1815. [Google Scholar] [CrossRef] [PubMed]
- Kakasheva–Mazhenkovska, L.; Milenkova, L.; Gjokik, G.; Janevska, V. Variations of the histomorphological characteristics of human skin of different body regions in subjects of different age. Prilozi 2011, 32, 119–128. [Google Scholar] [PubMed]
- Koszela, K. Zastosowanie mezoterapii w zespole bólowym kręgosłupa. In Choroba Zwyrodnieniowa Kręgosłupa W Praktyce Lekarza POZ. Nowe Spojrzenie; PZWL: Warsaw, Poland, 2022; pp. 40–54. [Google Scholar]
- Crenna, P.; Mancia, P. Reflex actions in mesotherapy. J. Mesother. 1981, 1, 29–40. [Google Scholar]
- Di Cesare, A.; Giombini, A.; Di Cesare, M.; Ripani, M.; Vulpiani, M.C.; Saraceni, V.M. Comparison between the effects of trigger point mesotherapy versus acupuncture points mesotherapy in the treatment of chronic low back pain: A short term randomized controlled trial. Complement. Ther. Med. 2011, 19, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, T.; Piccinini, G.; Trifan, P.D.; Zangrando, F.; Saraceni, V.M. Efficacy of trigger points mesotherapy for the treatment of chronic neck pain: A short term retrospective study. Int. J. Phys. Ther. Rehab. 2016, 2, 2. [Google Scholar] [CrossRef]
- Mammucari, M.; Russo, D.; Maggiori, E.; Paolucci, T.; Di Marzo, R.; Brauneis, S.; Bifarini, B.; Ronconi, G.; Ferrara, P.E.; Gori, F.; et al. Evidence based recommendations on mesotherapy: An update from the Italian society of Mesotherapy. Clin. Ter. 2021, 171, e37–e45. [Google Scholar] [CrossRef]
- Lewit, K. The needle effect in the relief of myofascial pain. Pain 1979, 6, 83–90. [Google Scholar] [CrossRef]
- Mammucari, M.; Maggiori, E.; Russo, D.; Giorgio, C.; Ronconi, G.; Ferrara, P.E.; Canzona, F.; Antonaci, L.; Violo, B.; Vellucci, R.; et al. Mesotherapy: From Historical Notes to Scientific Evidence and Future Prospects. Sci. World J. 2020, 2020, 3542848. [Google Scholar] [CrossRef]
- Pavelka, K.; Svobodová, R.; Jarošová, H. MD-Lumbar, MD-Muscle and MD-Neural in the treatment of low back pain. Physiol. Regul. Med. 2012, 4, 3–6. [Google Scholar]
- Faetani, L.; Ghizzoni, D.; Ammendolia, A.; Costantino, C. Safety and efficacy of mesotherapy in musculoskeletal disorders: A systematic review of randomized controlled trials with meta-analysis. J. Rehabil. Med. 2021, 53, jrm00182. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, J. Acupuncture in the treatment of chronic sacrolumbalgia and ischialgia. Am. J. Chin. Med. 1978, 4, 169–175. [Google Scholar] [CrossRef]
- Chiarotto, A.; Maxwell, L.J.; Ostelo, R.W.; Boers, M.; Tugwell, P.; Terwee, C.B. Measurement Properties of Visual Analogue Scale, Numeric Rating Scale, and Pain Severity Subscale of the Brief Pain Inventory in Patients With Low Back Pain: A Systematic Review. J. Pain 2019, 20, 245–263. [Google Scholar] [CrossRef]
- Misterska, E.; Jankowski, R.; Glowacki, M. Quebec Back Pain Disability Scale, Low Back Outcome Score and revised Oswestry low back pain disability scale for patients with low back pain due to degenerative disc disease: Evaluation of Polish versions. Spine (Phila Pa 1976) 2011, 36, E1722–E1729. [Google Scholar] [CrossRef]
- Akbas, I.; Kocak, A.O.; Kocak, M.B.; Cakir, Z. Comparison of intradermal mesotherapy with systemic therapy in the treatment of low back pain: A prospective randomized study. Am. J. Emerg. Med. 2020, 38, 1431–1435. [Google Scholar] [CrossRef]
- Ronconi, G.; Ferriero, G.; Nigito, C.; Foti, C.; Maccauro, G.; Ferrara, P.E. Efficacy of intradermal administration of diclofenac for the treatment of nonspecific chronic low back pain: Results from a retrospective observational study. Eur. J. Phys. Rehabil. Med. 2019, 55, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Godek, P. Collagen Therapy in Lumbar Spondylosis—A Pilot Study. Does the Route of Administration Matter? Ortop. Traumatol. Rehabil. 2019, 21, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Nitecka–Buchta, A.; Walczynska–Dragon, K.; Batko–Kapustecka, J.; Wieckiewicz, M. Comparison between Collagen and Lidocaine Intramuscular Injections in Terms of Their Efficiency in Decreasing Myofascial Pain within Masseter Muscles: A Randomized, Single-Blind Controlled Trial. Pain Res. Manag. 2018, 2018, 8261090. [Google Scholar] [CrossRef]
- Bifarini, B.; Gori, F.; Russo, D.; Mammucari, M.; Maggiori, E.; Di Marzo, R.; Migliore, A.; Massafra, U.; Ronconi, G.; Ferrara, P.E.; et al. Intradermal therapy (mesotherapy): The lower the better. Clin. Ter. 2022, 173, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Li, D.; Zhong, J.; Qiu, B.; Wu, X. Therapeutic Effectiveness and Safety of Mesotherapy in Patients with Osteoarthritis of the Knee. Evid. Based Complement. Alternat. Med. 2018, 2018, 6513049. [Google Scholar] [CrossRef] [PubMed]
- Navarte, D.A.; Rosset–Llobet, J. Safety of subcutaneous microinjections (mesotherapy) in musicians. Med. Probl. Perform. Art 2011, 26, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Mammucari, M.; Paolucci, T.; Russo, D.; Maggiori, E.; Di Marzo, R.; Migliore, A.; Massafra, U.; Ronconi, G.; Ferrara, P.E.; Gori, F.; et al. A Call to Action by the Italian Mesotherapy Society on Scientific Research. Drug Des. Dev. Ther. 2021, 15, 3041–3047. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Study Groups | Spinal Mesotherapy | |||
|---|---|---|---|---|
| A Collagen (n = 65) | % | B Lignocaine 1% (n = 65) | % | |
| Women | 44 | 68% | 39 | 60% |
| Men | 21 | 32% | 26 | 40% |
| Age [minimum] | 24 | 27 | ||
| Age [maximum] | 79 | 81 | ||
| Age [mean, SD] | 51 ± 13.88 | 52 ± 14.01 | ||
| Collagen Group (n = 65) | Lidocaine Group (n = 65) | GLM p-Values | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | Time | Treatment | Interaction Time–Treatment | AIC | |
| VAS-before therapy | 7.7 ± 0.9 | 8 (7–8) | 7.7 ± 0.9 | 8 (7–8) | <0.001 | 0.263 | 0.005 | 1486.3 |
| VAS-after therapy | 2.7 ± 1.3 | 3 (2–3) | 2.5 ± 1.0 | 2 (2–3) | ||||
| VAS-three-months follow-up | 2.0 ± 1.1 | 2 (1–3) | 3.0 ± 1.2 | 3 (2–4) | ||||
| Laitinen Scale-before therapy | 11.0 ± 1.7 | 11 (10–12) | 10.9 ± 1.5 | 11 (10–12) | <0.001 | 0.167 | 0.119 | 1735.3 |
| Laitinen Scale-after therapy | 3.7 ± 1.7 | 4 (3–5) | 2.9 ± 0.8 | 3 (2–3) | ||||
| Laitinen Scale-three-months follow-up | 2.6 ± 1.2 | 3 (2–3) | 3.3 ± 1.1 | 3 (3–4) | ||||
| Revised Oswestry Low Back Pain Disability Scale-before therapy | 30.6 ± 3.0 | 31 (28–32) | 30.2 ± 4.2 | 31 (28–32) | <0.001 | 0.183 | 0.023 | 2501.4 |
| Revised Oswestry Low Back Pain Disability Scale-after therapy | 9.6 ± 3.5 | 9 (7–11) | 8.4 ± 3.2 | 8 (6–10) | ||||
| Revised Oswestry Low Back Pain Disability Scale-three-months follow-up | 6.4 ± 3.1 | 6 (4–8) | 9.3 ± 3.4 | 9 (7–11) | ||||
| VAS | ANOVA for Repeated Measures | ||
|---|---|---|---|
| Treatment | Time | Time–Treatment | |
| % of explained variance | 0.40 | 98.50 | 1.14 |
| power | 0.108 | 1.0 | 0.127 |
| effect size | 0.051 | 0.369 | 0.039 |
| Laitinen Scale | ANOVA for Repeated Measures | ||
| Treatment | Time | Time–Treatment | |
| % of explained variance | 0.009 | 99.7 | 0.290 |
| power | 0.051 | 0.999 | 0.142 |
| effect size | 0.007 | 0.253 | 0.043 |
| Revised Oswestry Low Back Pain Disability Scale | ANOVA for Repeated Measures | ||
| Treatment | Time | Time–Treatment | |
| % of explained variance | 0.040 | 99.40 | 0.550 |
| power | 0.058 | 0.612 | 0.052 |
| effect size | 0.018 | 0.091 | 0.007 |
| VAS | ||||||
|---|---|---|---|---|---|---|
| Collagen-before Therapy | Collagen-after Therapy | Collagen-Three-Months Follow-Up | Lidocaine-before therapy | Lidocaine-after Therapy | Lidocaine-Three-Months Follow-Up | |
| Collagen-before therapy | - | <0.001 | <0.001 | 1.0 | - | - |
| Collagen- after therapy | <0.001 | - | 0.047 | - | 0.986 | 0.974 |
| Collagen-three-months follow-up | <0.001 | 0.047 | - | - | 0.577 | 0.028 |
| Lidocaine-before therapy | 1.0 | - | - | - | <0.001 | <0.001 |
| Lidocaine-after therapy | - | 0.986 | 0.577 | <0.001 | - | 0.19 |
| Lidocaine-three-months follow-up | - | 0.974 | 0.028 | <0.001 | 0.19 | - |
| Laitinen Scale | ||||||
| Collagen-before Therapy | Collagen-after Therapy | Collagen-Three-Months Follow-Up | Lidocaine-before Therapy | Lidocaine-after Therapy | Lidocaine-Three-Months Follow-Up | |
| Collagen-before therapy | - | <0.001 | <0.001 | 1.0 | - | - |
| Collagen-after therapy | <0.001 | - | 0.0045 | - | 0.114 | 0.810 |
| Collagen-three-months follow-up | <0.001 | 0.0045 | - | - | 0.992 | 0.444 |
| Lidocaine-before therapy | 1.0 | - | - | - | <0.001 | <0.001 |
| Lidocaine-after therapy | - | 0.114 | 0.992 | <0.001 | - | 0.25 |
| Lidocaine-three-months follow-up | - | 0.810 | 0.444 | <0.001 | 0.25 | - |
| Revised Oswestry Low Back Pain Disability Scale | ||||||
| Collagen-before Therapy | Collagen-after Therapy | Collagen-Three-Months Follow-Up | Lidocaine-before Therapy | Lidocaine- after Therapy | Lidocaine-Three-Months Follow-Up | |
| Collagen-before therapy | - | <0.001 | <0.001 | 0.999 | - | - |
| Collagen-after therapy | <0.001 | - | 0.013 | - | 0.730 | - |
| Collagen-three-months follow-up | <0.001 | 0.013 | - | - | 0.237 | 0.998 |
| Lidocaine-before therapy | 0.999 | - | - | - | <0.001 | 0.011 |
| Lidocaine-after therapy | - | 0.730 | 0.237 | <0.001 | - | 0.059 |
| Lidocaine-three-months follow-up | - | 0.998 | 0.011 | <0.001 | 0.059 | - |
| Spinal Mesotherapy | ||||
|---|---|---|---|---|
| Collagen (n = 65) | n (%) | Lignocaine 1% (n = 65) | n (%) | |
| Pain during first mesotherapy procedure (VAS ≥ 7) | Yes | 2 (3.0) | Yes | 1 (1.5) |
| Pain during first mesotherapy procedure (VAS 4–6) | Yes | 9 (13.8) | Yes | 6 (9.2) |
| Pain during first mesotherapy procedure (VAS < 4) | Yes | 30 (46.2) | Yes | 21 (32.3) |
| Pain during 5th mesotherapy procedure (VAS ≥ 7) | No | 0 (0) | No | 0 (0) |
| Pain during 5th mesotherapy procedure (VAS 4–6) | Yes | 3 (4.6) | Yes | 4 (6.2) |
| Pain during 5th mesotherapy procedure (VAS < 4) | Yes | 10 (15.4) | Yes | 7 (10.8) |
| Fever after first mesotherapy procedure | No | 0 (0) | Yes | 1 (1.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koszela, K.; Woldańska-Okońska, M.; Gasik, R. Efficacy and Safety of Spinal Collagen Mesotherapy in Patients with Chronic Low Back Pain in a Three-Month Follow-Up—Retrospective Study. J. Clin. Med. 2024, 13, 787. https://doi.org/10.3390/jcm13030787
Koszela K, Woldańska-Okońska M, Gasik R. Efficacy and Safety of Spinal Collagen Mesotherapy in Patients with Chronic Low Back Pain in a Three-Month Follow-Up—Retrospective Study. Journal of Clinical Medicine. 2024; 13(3):787. https://doi.org/10.3390/jcm13030787
Chicago/Turabian StyleKoszela, Kamil, Marta Woldańska-Okońska, and Robert Gasik. 2024. "Efficacy and Safety of Spinal Collagen Mesotherapy in Patients with Chronic Low Back Pain in a Three-Month Follow-Up—Retrospective Study" Journal of Clinical Medicine 13, no. 3: 787. https://doi.org/10.3390/jcm13030787
APA StyleKoszela, K., Woldańska-Okońska, M., & Gasik, R. (2024). Efficacy and Safety of Spinal Collagen Mesotherapy in Patients with Chronic Low Back Pain in a Three-Month Follow-Up—Retrospective Study. Journal of Clinical Medicine, 13(3), 787. https://doi.org/10.3390/jcm13030787