
Thirteen Years of Impactful, Minimally Invasive Coronary Surgery: Short- and Long-Term Results for Single and Multi-Vessel Disease †

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgical Strategy and Approach
2.3. Statistical Analysis
3. Results
3.1. In-Hospital Outcomes
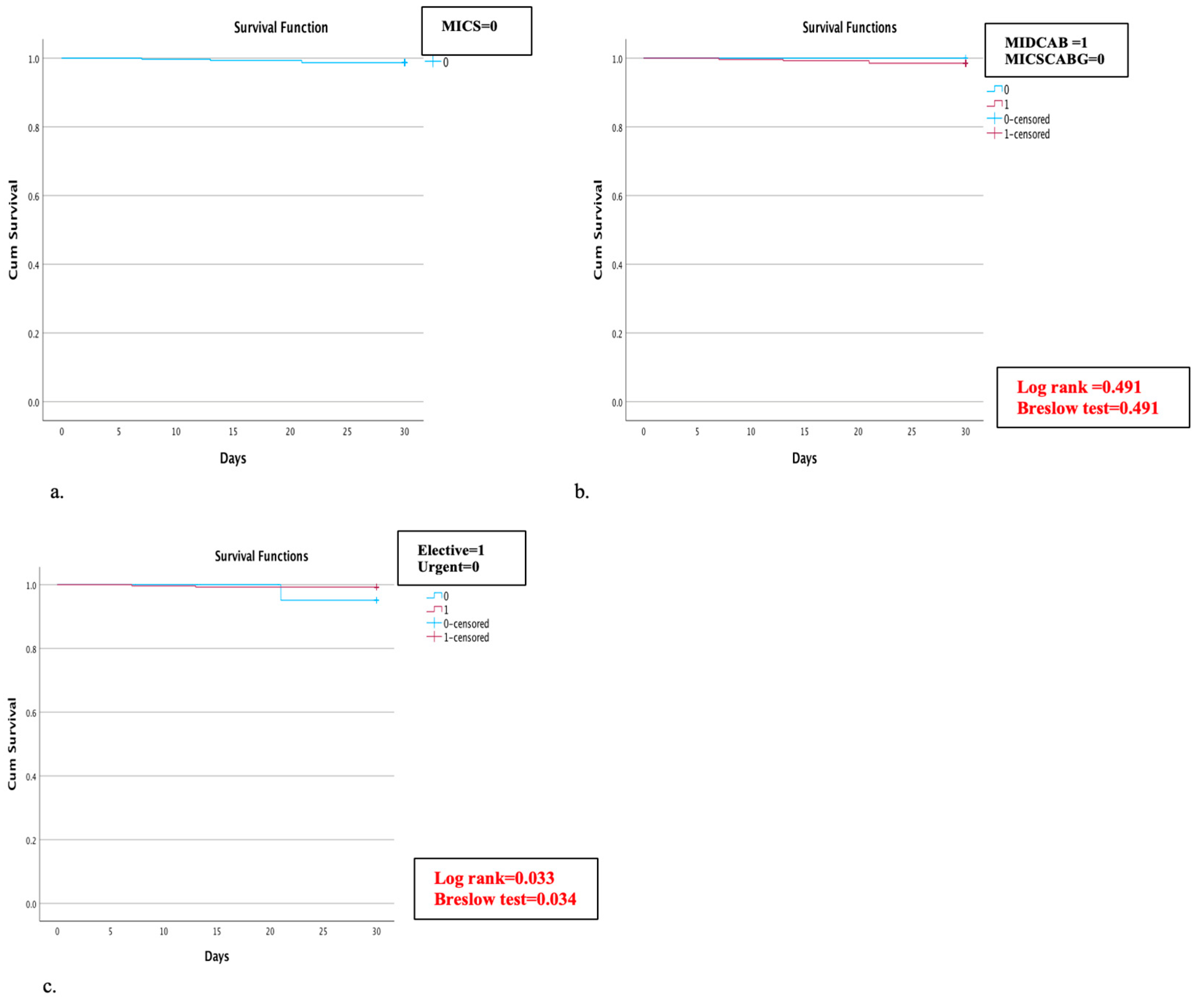
3.2. 30-Day Mortality
4. Follow-Up Data
5. Discussion
6. Study Limitation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hill, J.D.; Gibbon, J.H., Jr. Part I. The development of the first successful heart-lung machine. Ann. Thorac. Surg. 1982, 34, 337–341. [Google Scholar]
- Repossini, A.; Di Bacco, L.; Nicoli, F.; Passaretti, B.; Stara, A.; Jonida, B.; Muneretto, C. Minimally invasive coronary artery bypass: Twenty-year experience. J. Thorac. Cardiovasc. Surg. 2019, 158, 127–138.e1. [Google Scholar] [CrossRef]
- Kolessov, V.I. Mammary artery-coronary artery anastomosis as method of treatment for angina pectoris. J. Thorac. Cardiovasc. Surg. 1967, 54, 535–544. [Google Scholar] [CrossRef]
- Benetti, F.J.; Mariani, M.A.; Ballester, C. Direct coronary surgery without cardiopulmonary bypass in acute myocardial infarction. J. Cardiovasc. Surg. 1996, 37, 391–395. [Google Scholar]
- Calafiore, A.M.; Di Giammarco, G.; Teodori, G.; Bosco, G.; D’Annunzio, E.; Barsotti, A.; Maddestra, N.; Paloscia, L.; Vitolla, G.; Sciarra, A.; et al. Left anterior descending coronary artery grafting via left anterior small thoracotomy without cardiopulmonary bypass. Ann. Thorac. Surg. 1996, 61, 1658–1663; discussion 1654. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, V.A.; McCabe, J.C.; Geller, C.M. Minimally invasive direct coronary artery bypass grafting: Two-year clinical experience. Ann. Thorac. Surg. 1997, 64, 1648–1655. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, P.W.; Grandjean, J.G.; Mariani, M.A. Improved method for direct coronary grafting without CPB via anterolateral small thoracotomy. Ann. Thorac. Surg. 1997, 63, 567–569. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, V.A. MIDCAB approach for single vessel coronary artery bypass graft. Oper. Tech. Card. Thorac. Surg. 1998, 3, 2–15. [Google Scholar] [CrossRef]
- Marin-Cuartas, M.; Sá, M.P.; Torregrossa, G.; Davierwala, P.M. Minimally invasive coronary artery surgery: Robotic and nonrobotic minimally invasive direct coronary artery bypass techniques. JTCVS Tech. 2021, 10, 170–177. [Google Scholar] [CrossRef]
- Mourad, F.; Duncan, A.J. Tissue stabilizer reverse mounting in minimally invasive direct coronary artery bypass, a simple tool in difficult times. Innovations 2009, 4, 117. [Google Scholar]
- Borst, C.; Jansen, E.W.; Tulleken, C.A.; Grundeman, P.F.; Beck, H.J.M.; van Dongen, J.W.; Hodde, K.C.; Bredée, J.J. Coronary artery bypass grafting without cardiopulmonary bypass and without interruption of native coronary flow using a novel anastomosis site restraining device (“Octopus”). J. Am. Coll. Cardiol. 1996, 27, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Cremer, J.; Strüber, M.; Wittwer, T.; Ruhparwar, A.; Harringer, W.; Zuk, J.; Mehler, D.; Haverich, A. Off-bypass coronary bypass grafting via minithoracotomy using mechanical epicardial stabilization. Ann. Thorac. Surg. 1997, 63, S79–S83. [Google Scholar] [CrossRef]
- Heres, E.K.; Marquez, J.; Malkowski, M.J.; Magovern, J.A.; Gravlee, G.P. Minimally invasive direct coronary artery bypass: Anesthetic, monitoring, and pain control considerations. J. Cardiothorac. Vasc. Anesth. 1998, 12, 385–389. [Google Scholar] [CrossRef]
- Raja, S.G.; Garg, S.; Rochon, M.; Daley, S.; De Robertis, F.; Bahrami, T. Short-term clinical outcomes and long-term survival of minimally invasive direct coronary artery bypass grafting. Ann. Cardiothorac. Surg. 2018, 7, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Saadat, S.; Habib, R.; Engoren, M.; Mentz, G.; Gaudino, M.; Engelman, D.T.; Schwann, T.A. Multiarterial coronary artery bypass grafting practice patterns in the united states: Analysis of the society of thoracic surgeons adult cardiac surgery database. Ann. Thorac. Surg. 2022, 115, 1411–1419. [Google Scholar] [CrossRef] [PubMed]
- Bonatti, J.; Wallner, S.; Crailsheim, I.; Grabenwöger, M.; Winkler, B. Minimally invasive and robotic coronary artery bypass grafting—A 25-year review. J. Thorac. Dis. 2021, 13, 1922–1944. [Google Scholar] [CrossRef]
- Chikwe, J.; Lee, T.; Itagaki, S.; Adams, D.H.; Egorova, N.N. Long-Term Outcomes After Off-Pump Versus On-Pump Coronary Artery Bypass Grafting by Experienced Surgeons. J. Am. Coll. Cardiol. 2018, 72, 1478–1486. [Google Scholar] [CrossRef]
- Afilalo, J.; Rasti, M.; Ohayon, S.M.; Shimony, A.; Eisenberg, M.J. Off-pump vs. on-pump coronary artery bypass surgery: An updated meta-analysis and meta-regression of randomized trials. Eur. Heart J. 2011, 33, 1257–1267. [Google Scholar] [CrossRef]
- Thuijs, D.J.F.M.; Kappetein, A.P.; Serruys, P.W.; Mohr, F.-W.; Morice, M.-C.; Mack, M.J.; Holmes, D.R.; Curzen, N.; Davierwala, P.; Noack, T.; et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. Lancet 2019, 394, 1325–1334. [Google Scholar] [CrossRef]
- Park, S.-J.; Ahn, J.-M.; Kim, Y.-H.; Park, D.-W.; Yun, S.-C.; Lee, J.-Y.; Kang, S.-J.; Lee, S.-W.; Lee, C.W.; Park, S.-W.; et al. Trial of everolimus-eluting stents or bypass surgery for coronary disease. N. Engl. J. Med. 2015, 372, 1204–1212. [Google Scholar] [CrossRef]
- Mäkikallio, T.; Holm, N.R.; Lindsay, M.; Spence, M.S.; Erglis, A.; Menown, I.B.A.; Trovik, T.; Eskola, M.; Romppanen, H.; Kellerth, T.; et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis (NOBLE): A prospective, randomised, open-label, non-inferiority trial. Lancet 2016, 388, 2743–2752. [Google Scholar] [CrossRef]
- Hunter, G.W.; Sharma, V.; Varma, C.; Connolly, D. The EXCEL Trial: The Interventionalists’ Perspective. Eur. Cardiol. Rev. 2021, 16, e01. [Google Scholar] [CrossRef]
- Van Praet, K.M.; Kofler, M.; Shafti, T.Z.N.; El Al, A.A.; van Kampen, A.; Amabile, A.; Torregrossa, G.; Kempfert, J.; Falk, V.; Balkhy, H.H.; et al. Minimally invasive coronary revascularisation surgery: A focused review of the available literature. Interv. Cardiol. 2021, 16, e08. [Google Scholar] [CrossRef]
- Diodato, M.; Chedrawy, E.G. Coronary artery bypass graft surgery: The past, present, and future of myocardial revascularisation. Surg. Res. Pract. 2014, 2014, 726158. [Google Scholar] [CrossRef]
- McGinn, J.T.; Usman, S.; Lapierre, H.; Pothula, V.R.; Mesana, T.G.; Ruel, M. Minimally invasive coronary artery bypass grafting: Dual-center experience in 450 consecutive patients. Circulation 2009, 120 (Suppl. S11), S78–S84. [Google Scholar] [CrossRef]
- Ruel, M.; Shariff, M.A.; Lapierre, H.; Goyal, N.; Dennie, C.; Sadel, S.M.; Sohmer, B.; McGinn, J.T. Results of the minimally invasive coronary artery bypass grafting angiographic patency study. J. Thorac. Cardiovasc. Surg. 2013, 147, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, M.L.; Lapierre, H.R.; Sohmer, B.; Glineur, D.; Ruel, M. Mid-Term Follow-up of Minimally Invasive Multivessel Coronary Artery Bypass Grafting: Is the Early Learning Phase Detrimental? Innovations 2017, 12, 116–120. [Google Scholar] [PubMed]
- Kikuchi, K.; Mori, M. Minimally invasive coronary artery bypass grafting: A systematic review. Asian Cardiovasc. Thorac. Ann. 2017, 25, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Davierwala, P.M.; Verevkin, A.; Bergien, L.; von Aspern, K.; Deo, S.V.; Misfeld, M.; Holzhey, D.; Borger, M.A. Twenty-year outcomes of minimally invasive direct coronary artery bypass surgery: The Leipzig experience. J. Thorac. Cardiovasc. Surg. 2021, 165, 115–127.e4. [Google Scholar] [CrossRef] [PubMed]
- Dieberg, G.; Smart, N.A.; King, N. Minimally invasive cardiac surgery: A systematic review and meta-analysis. Int. J. Cardiol. 2016, 223, 554–560. [Google Scholar] [CrossRef]
- Manuel, L.; Fong, L.S.; Betts, K.; Bassin, L.; Wolfenden, H. LIMA to LAD grafting returns patient survival to age-matched population: 20-year outcomes of MIDCAB surgery. Interact. Cardiovasc. Thorac. Surg. 2022, 35, ivac243. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Arghami, A.; Habib, R.; Daneshmand, M.A.; Parsons, N.; Elhalabi, Z.; Krohn, C.; Thourani, V.; Bowdish, M.E. The society of thoracic surgeons adult cardiac surgery database: 2022 update on outcomes and research. Ann. Thorac. Surg. 2023, 115, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Lamy, A.; Devereaux, P.J.; Prabhakaran, D.; Taggart, D.P.; Hu, S.; Straka, Z.; Piegas, L.S.; Avezum, A.; Akar, A.R.; Lanas Zanetti, F.; et al. Five-Year Outcomes after Off-Pump or On-Pump Coronary-Artery Bypass Grafting. N. Engl. J. Med. 2016, 375, 2359–2368. [Google Scholar] [CrossRef] [PubMed]
- Kettering, K.; Dapunt, O.; Baer, F.M. Minimally invasive direct coronary artery bypass grafting: A systematic review. J. Cardiovasc. Surg. 2004, 45, 255–264. [Google Scholar]
- Jonkers, D.; Elenbaas, T.; Terporten, P.; Nieman, F.; Stobberingh, E. Prevalence of 90-days postoperative wound infections after cardiac surgery. Eur. J. Cardio-Thorac. Surg. 2003, 23, 97–102. [Google Scholar] [CrossRef] [PubMed]
- L’Ecuyer, P.B.; Murphy, D.; Little, J.R.; Fraser, V.J. The Epidemiology of chest and leg wound infections following cardiothoracic surgery. Clin. Infect. Dis. 1996, 22, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Lapierre, H.; Chan, V.; Sohmer, B.; Mesana, T.G.; Ruel, M. Minimally invasive coronary artery bypass grafting via a small thoracotomy versus off-pump: A case-matched study. Eur. J. Cardio-Thorac. Surg. 2011, 40, 804–810. [Google Scholar] [CrossRef]
- Kyaruzi, M.; Gülmez, H.; Demirsoy, E. Can minimally invasive multivessel coronary revascularization be a routine approach? Thorac. Cardiovasc. Surg. 2023, 71, 455–461. [Google Scholar] [CrossRef]
- Une, D.; Lapierre, H.; Sohmer, B.; Rai, V.; Ruel, M. Can minimally invasive coronary artery bypass grafting be initiated and practiced safely?: A learning curve analysis. Innovations 2013, 8, 403–409. [Google Scholar]
- Babliak, O.; Demianenko, V.; Melnyk, Y.; Revenko, K.; Babliak, D.; Stohov, O.; Pidgayna, L. Multivessel arterial revascularization via left anterior thoracotomy. Semin. Thorac. Cardiovasc. Surg. 2020, 32, 655–662. [Google Scholar] [CrossRef]
- Elbadawi, A.; Hamed, M.; Elgendy, I.Y.; Omer, M.A.; Ogunbayo, G.O.; Megaly, M.; Denktas, A.; Ghanta, R.; Jimenez, E.; Brilakis, E.; et al. Outcomes of reoperative coronary artery bypass graft surgery in the United States. J. Am. Heart Assoc. 2020, 9, e016282. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Antoniades, C.; Benedetto, U.; Deb, S.; Di Franco, A.; Di Giammarco, G.; Fremes, S.; Glineur, D.; Grau, J.; He, G.-W.; et al. Mechanisms, consequences, and prevention of coronary graft failure. Circulation 2017, 136, 1749–1764. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Di Franco, A.; Bhatt, D.L.; Alexander, J.H.; Abbate, A.; Azzalini, L.; Sandner, S.; Sharma, G.; Rao, S.V.; Crea, F.; et al. The association between coronary graft patency and clinical status in patients with coronary artery disease. Eur. Heart J. 2021, 42, 1433–1441. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Sandner, S.; An, K.R.; Dimagli, A.; Di Franco, A.; Audisio, K.; Harik, L.; Perezgrovas-Olaria, R.; Soletti, G.; Fremes, S.E.; et al. Graft Failure After Coronary Artery Bypass Grafting and Its Association With Patient Characteristics and Clinical Events: A Pooled Individual Patient Data Analysis of Clinical Trials With Imaging Follow-Up. Circulation 2023, 148, 1305–1315. [Google Scholar] [CrossRef]
- Buxton, B.F.; Hayward, P.A.; Raman, J.; Moten, S.C.; Rosalion, A.; Gordon, I.; Seevanayagam, S.; Matalanis, G.; Benedetto, U.; Gaudino, M.; et al. Long-Term Results of the RAPCO Trials. Circulation 2020, 142, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Goldman, S.; Zadina, K.; Moritz, T.; Ovitt, T.; Sethi, G.; Copeland, J.G.; Thottapurathu, L.; Krasnicka, B.; Ellis, N.; Anderson, R.J.; et al. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery: Results from a Department of Veterans Affairs Cooperative Study. J. Am. Coll. Cardiol. 2004, 44, 2149–2156. [Google Scholar] [CrossRef]
- Diegeler, A.; Doll, N.; Rauch, T.; Haberer, D.; Walther, T.; Falk, V.; Gummert, J.; Autschbach, R.; Mohr, F.-W. Humoral immune response during coronary artery bypass grafting: A comparison of limited approach, “off-pump” technique, and conventional cardiopulmonary bypass. Circulation 2000, 102 (Suppl. S3), III95–III100. [Google Scholar] [CrossRef]
- Puskas, J.D.; Martin, J.; Cheng, D.C.; Benussi, S.; Bonatti, J.O.; Diegeler, A.; Ferdiand, F.D.; Kieser, T.M.; Lamy, A.; Mack, M.J.; et al. ISMICS Consensus Conference and Statements of Randomized Controlled Trials of Off-Pump Versus Conventional Coronary Artery Bypass Surgery. Innovations 2015, 10, 219–229. [Google Scholar]
- Lubitz, S.A.; Yin, X.; Rienstra, M.; Schnabel, R.B.; Walkey, A.J.; Magnani, J.W.; Rahman, F.; McManus, D.D.; Tadros, T.M.; Levy, D.; et al. Long-term outcomes of secondary atrial fibrillation in the community: The Framingham Heart Study. Circulation 2015, 131, 1648–1655. [Google Scholar] [CrossRef]
- de Paula Pereira, M.; Lima, E.G.; Pitta, F.G.; Gowdak, L.H.W.; Mioto, B.M.; Carvalho, L.N.S.; da Costa Darrieux, F.C.; Mejia, O.A.V.; Jatene, F.B.; Serrano, C.V., Jr. Rivaroxaban versus warfarin in postoperative atrial fibrillation: Cost-effectiveness analysis in a single-center, randomized, and prospective trial. JTCVS Open 2023, 15, 199–210. [Google Scholar] [CrossRef]
- Melly, L.; Torregrossa, G.; Lee, T.; Jansens, J.-L.; Puskas, J.D. Fifty years of coronary artery bypass grafting. J. Thorac. Dis. 2018, 10, 1960–1967. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, F.; E Cohn, W.; Baribeau, Y.R.; Tryzelaar, J.F.; Charlesworth, D.C.; A Clough, R.; Klemperer, J.D.; Morton, J.R.; Westbrook, B.M.; Olmstead, E.M.; et al. In-hospital outcomes of off-pump versus on-pump coronary artery bypass procedures: A multicenter experience. Ann. Thorac. Surg. 2001, 72, 1528–1533; discussion 1533. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 315) | N (%) |
|---|---|
| Age, years, mean ± SD | 64 ± 11 |
| Female gender, n (%) | 53(16.8%) |
| Hypertension n (%) | 263 (83.5%) |
| Dyslipidemia, n (%) | 280 (88.9%) |
| Diabetes mellitus, n (%) | 94 (29.8%) |
| Current smoker, n (%) | 90 (28.6%) |
| Ex-smoker, n (%) | 109 (34.6%) |
| Peripheral arterial disease, n (%) | 26 (8.3%) |
| COPD, n (%) | 24 (7.6%) |
| Chronic kidney disease, n (%) | 24 (7.6%) |
| BMI kg/m2, median (IQR) | 27.1 (24.4–29.8) |
| Previous cardiac surgeries, n (%) | 3 (1%) |
| Urgent surgery, n (%) | 42 (13.3%) |
| MI in the last 30 days before surgery, n (%) | 64 (20.3%) |
| MI > 30 days before the surgery, n (%) | 96 (30.5%) |
| Previous PCI, n (%) | 118 (37.5%) |
| Preoperative NYHA, n (%) | |
| I | 124 (39.4%) |
| II | 138 (43.8%) |
| III | 46 (14.6%) |
| IV | 2 (0.6%) |
| Preoperative CCS, n (%) | |
| 0 | 83 (26.3%) |
| 1 | 47 (14.9%) |
| 2 | 109 (34.6%) |
| 3 | 54 (17.1%) |
| 4 | 22 (7%) |
| Number of diseased vessels, n (%) | |
| One vessel | 182 (57.8%) |
| Two vessels | 79 (25.1%) |
| Three vessels | 54 (17.1%) |
| Preoperative LVEF (%), median (IQR) | 60% (50–64%) |
| Euroscore II, median (IQR) | 1.2 (0.8–2.2) |
| Preoperative Serum creatine (μmol/L), median (IQR) | 82 (71–92) |
| Intraoperative Details (n = 315) | N (%) |
|---|---|
| MIDCAB | 271 (86%) |
| MICSCABG | 44 (14%) |
| Duration surgery (min), median (IQR) | 139 (115–172) |
| Pulsatility Index (PI), median (IQR) | 1.9 (1.5–2.6) |
| Graft flow (mL/min), median (IQR) | 24 (17–35) |
| Hybrid revascularization | 27 (8.6%) |
| Conversion to MS | 8 (2.5%) |
| Usage of CPB | 12 (3.9%) * |
| Number of bypasses | |
| 1 | 254 (80.6%) |
| 2 | 33 (10.5%) |
| 3 | 1 (0.3%) |
| Conduit | |
| LIMA | 313 (99.4%) |
| RIMA | 3 (1%) |
| GSV | 17 (5.4%) |
| RA | 16 (5.1%) |
| Target vessels | |
| RIVA | 306 (97.1%) |
| D | 27 (8.6%) |
| RCx | 16 (5.1%) |
| RIM | 9 (2.9%) |
| RCA | 3 (1%) |
| In-Hospital Outcomes (n = 307) | N (%) |
|---|---|
| New AF | 26 (8.5%) |
| Rethoracotomy because of bleeding | 5 (1.6%) |
| New postoperative MI | 5 (1.6%) |
| Postoperative AV block | 1 (0.3) |
| Postoperative wound healing complication | 4 (1.3) |
| PPM Implantation | 1 (0.3%) |
| Postoperative stroke | 0 |
| New renal replacement therapy | 0 |
| Direct postoperative myoglobin, mcg/L, median (IQR) | 63 (30–120) |
| Highest postoperative myoglobin, mcg/L, median (IQR) | 114 (44–8456) |
| Direct postoperative Troponin T, ng/L, median (IQR) | 63 (30–120) |
| Highest postoperative Troponin T, ng/L, median (IQR) | 114 (44–8456) |
| Direct postoperative CK, U/L, median (IQR) | 298 (182–595) |
| Highest postoperative CK, U/L, median (IQR) | 584 (401–838) |
| Postoperative Serum Creatinine (μmol/L) median (IQR) | 82 (72–95) |
| Postoperative LVEF %, median (IQR) | 60% (55–63%) |
| Duration of hospitalization, d, median (IQR) | 8 (7–9) |
| Duration on ICU, d, median (IQR) | 2 (1–3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilcheva, L.; Häussler, A.; Cholubek, M.; Ntinopoulos, V.; Odavic, D.; Dushaj, S.; Rodriguez Cetina Biefer, H.; Dzemali, O. Thirteen Years of Impactful, Minimally Invasive Coronary Surgery: Short- and Long-Term Results for Single and Multi-Vessel Disease. J. Clin. Med. 2024, 13, 761. https://doi.org/10.3390/jcm13030761
Ilcheva L, Häussler A, Cholubek M, Ntinopoulos V, Odavic D, Dushaj S, Rodriguez Cetina Biefer H, Dzemali O. Thirteen Years of Impactful, Minimally Invasive Coronary Surgery: Short- and Long-Term Results for Single and Multi-Vessel Disease. Journal of Clinical Medicine. 2024; 13(3):761. https://doi.org/10.3390/jcm13030761
Chicago/Turabian StyleIlcheva, Lilly, Achim Häussler, Magdalena Cholubek, Vasileios Ntinopoulos, Dragan Odavic, Stak Dushaj, Hector Rodriguez Cetina Biefer, and Omer Dzemali. 2024. "Thirteen Years of Impactful, Minimally Invasive Coronary Surgery: Short- and Long-Term Results for Single and Multi-Vessel Disease" Journal of Clinical Medicine 13, no. 3: 761. https://doi.org/10.3390/jcm13030761
APA StyleIlcheva, L., Häussler, A., Cholubek, M., Ntinopoulos, V., Odavic, D., Dushaj, S., Rodriguez Cetina Biefer, H., & Dzemali, O. (2024). Thirteen Years of Impactful, Minimally Invasive Coronary Surgery: Short- and Long-Term Results for Single and Multi-Vessel Disease. Journal of Clinical Medicine, 13(3), 761. https://doi.org/10.3390/jcm13030761