
Treatment of Granulomatous Inflammation in Pulmonary Sarcoidosis

Abstract
1. Introduction
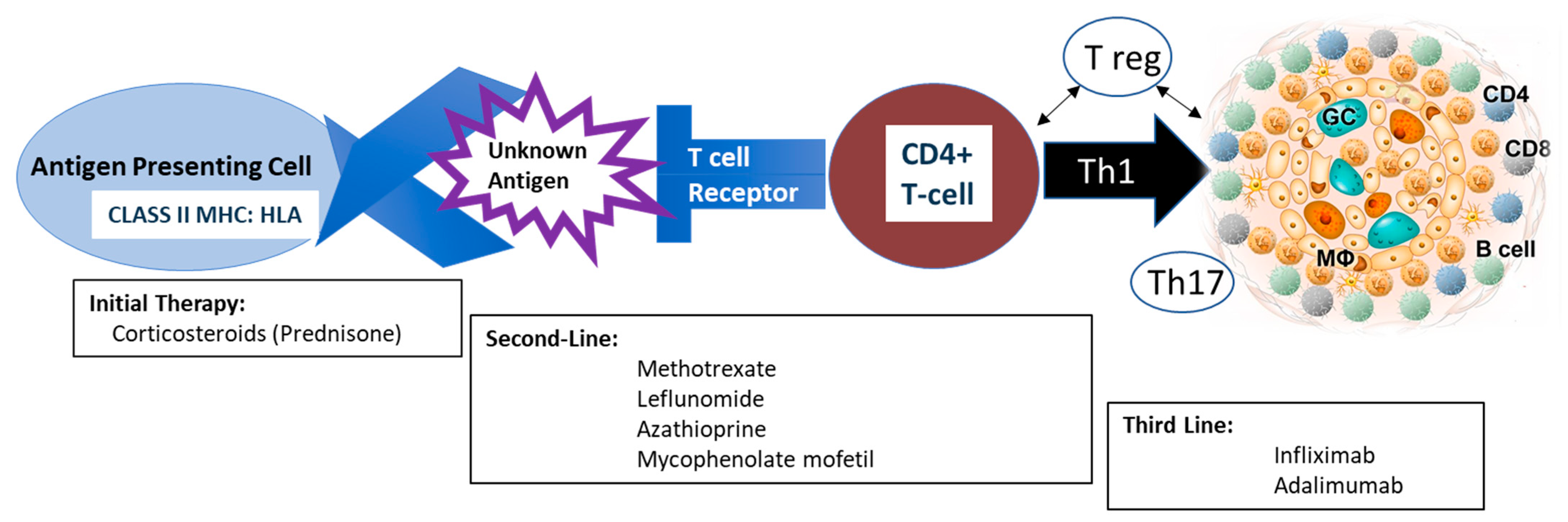
2. Pathophysiology
3. When to Treat
4. Medications Targeting Granulomatous Inflammation
5. Clinical Considerations in the Choice of Corticosteroid-Sparing Therapies
6. Relapses
7. Biomarkers in the Management of Therapy
8. Summary
9. Future Directions
Funding
Conflicts of Interest
References
- Newman, L.S.; Rose, C.S.; Bresnitz, E.A.; Rossman, M.D.; Barnard, J.; Frederick, M.; Terrin, M.L.; Weinberger, S.E.; Moller, D.R.; McLennan, G.; et al. A case control etiologic study of sarcoidosis: Environmental and occupational risk factors. Am. J. Respir. Crit. Care Med. 2004, 170, 1324–1330. [Google Scholar] [CrossRef]
- Izbicki, G.; Chavko, R.; Banauch, G.I.; Weiden, M.D.; Berger, K.I.; Aldrich, T.K.; Hall, C.; Kelly, K.J.; Prezant, D.J. World Trade Center “sarcoid-like” granulomatous pulmonary disease in New York City Fire Department rescue workers. Chest 2007, 131, 1414–1423. [Google Scholar] [CrossRef] [PubMed]
- Kreider, M.E.; Christie, J.D.; Thompson, B.; Newman, L.; Rose, C.; Barnard, J.; Bresnitz, E.; Judson, M.A.; Lackland, D.T.; Rossman, M.D. Relationship of environmental exposures to the clinical phenotype of sarcoidosis. Chest 2005, 128, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Rybicki, B.A.; Kirkey, K.L.; Major, M.; Maliarik, M.J.; Popovich, J., Jr.; Chase, G.A.; Iannuzzi, M.C. Familial risk ratio of sarcoidosis in African-American sibs and parents. Am. J. Epidemiol. 2001, 153, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Rybicki, B.A.; Iannuzzi, M.C.; Frederick, M.M.; Thompson, B.W.; Rossman, M.D.; Bresnitz, E.A.; Terrin, M.L.; Moller, D.R.; Barnard, J.; Baughman, R.P.; et al. Familial aggregation of sarcoidosis. A case-control etiologic study of sarcoidosis (ACCESS). Am. J. Respir. Crit Care Med. 2001, 164, 2085–2091. [Google Scholar] [CrossRef]
- Schürmann, M.; Reichel, P.; Müller-Myhsok, B.; Schlaak, M.; Müller-Quernheim, J.; Schwinger, E. Results from a genome-wide search for predisposing genes in sarcoidosis. Am. J. Respir. Crit. Care Med. 2001, 164, 840–846. [Google Scholar] [CrossRef]
- Culver, D.A.; Newman, L.S.; Kavuru, M.S. Gene-environment interactions in sarcoidosis: Challenge and opportunity. Clin. Dermatol. 2007, 25, 267–275. [Google Scholar] [CrossRef]
- Crouser, E.D.; Maier, L.A.; Wilson, K.C.; Bonham, C.A.; Morgenthau, A.S.; Patterson, K.C.; Abston, E.; Bernstein, R.C.; Blankstein, R.; Chen, E.S.; et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e26–e51. [Google Scholar] [CrossRef]
- Lepzien, R.; Nie, M.; Czarnewski, P.; Liu, S.; Yu, M.; Ravindran, A.; Kullberg, S.; Eklund, A.; Grunewald, J.; Smed-Sörensen, A. Pulmonary and blood dendritic cells from sarcoidosis patients more potently induce IFNgamma-producing Th1 cells compared with monocytes. J. Leukoc. Biol. 2022, 111, 857–866. [Google Scholar] [CrossRef]
- Bennett, D.; Bargagli, E.; Refini, R.M.; Rottoli, P. New concepts in the pathogenesis of sarcoidosis. Expert. Rev. Respir. Med. 2019, 13, 981–991. [Google Scholar] [CrossRef]
- Hawkins, C.; Shaginurova, G.; Shelton, D.A.; Herazo-Maya, J.D.; Oswald-Richter, K.A.; Rotsinger, J.E.; Young, A.; Celada, L.J.; Kaminski, N.; Sevin, C.; et al. Local and Systemic CD4(+) T Cell Exhaustion Reverses with Clinical Resolution of Pulmonary Sarcoidosis. J. Immunol. Res. 2017, 2017, 3642832. [Google Scholar] [CrossRef]
- Baughman, R.P.; Valeyre, D.; Korsten, P.; Mathioudakis, A.G.; Wuyts, W.A.; Wells, A.; Rottoli, P.; Nunes, H.; Lower, E.E.; Judson, M.A.; et al. ERS clinical practice guidelines on treatment of sarcoidosis. Eur. Respir. J. 2021, 58, 2004079. [Google Scholar] [CrossRef]
- Zappala, C.J.; Desai, S.R.; Copley, S.J.; Spagnolo, P.; Sen, D.; Alam, S.M.; du Bois, R.M.; Hansell, D.M.; Wells, A.U. Accuracy of individual variables in the monitoring of long-term change in pulmonary sarcoidosis as judged by serial high-resolution CT scan data. Chest 2014, 145, 101–107. [Google Scholar] [CrossRef]
- Grutters, J.C.; van den Bosch, J.M. Corticosteroid treatment in sarcoidosis. Eur. Respir. J. 2006, 28, 627–636. [Google Scholar] [CrossRef]
- Rahaghi, F.F.; Baughman, R.P.; Saketkoo, L.A.; Sweiss, N.J.; Barney, J.B.; Birring, S.S.; Costabel, U.; Crouser, E.D.; Drent, M.; Gerke, A.K.; et al. Delphi consensus recommendations for a treatment algorithm in pulmonary sarcoidosis. Eur. Respir. Rev. 2020, 29, 190146. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, A.E.; Chapman, K.E. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol. Cell Endocrinol. 2011, 335, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Paramothayan, N.S.; Lasserson, T.J.; Jones, P. Corticosteroids for pulmonary sarcoidosis. Cochrane Database Syst. Rev. 2005, 2, CD001114. [Google Scholar] [CrossRef] [PubMed]
- Schutt, A.C.; Bullington, W.M.; Judson, M.A. Pharmacotherapy for pulmonary sarcoidosis: A Delphi consensus study. Respir. Med. 2010, 104, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Yazaki, Y.; Isobe, M.; Hiroe, M.; Morimoto, S.-I.; Hiramitsu, S.; Nakano, T.; Izumi, T.; Sekiguchi, M.; Central Japan Heart Study Group. Prognostic determinants of long-term survival in Japanese patients with cardiac sarcoidosis treated with prednisone. Am. J. Cardiol. 2001, 88, 1006–1010. [Google Scholar] [CrossRef] [PubMed]
- Broos, C.E.; Poell, L.H.; Looman, C.W.; In ’t Veen, J.C.C.M.; Grootenboers, M.J.; Heller, R.; van den Toorn, L.M.; Wapenaar, M.; Hoogsteden, H.C.; Kool, M. No evidence found for an association between prednisone dose and FVC change in newly-treated pulmonary sarcoidosis. Respir. Med. 2018, 138, S31–S37. [Google Scholar] [CrossRef] [PubMed]
- Broos, C.E.; Wapenaar, M.; Looman, C.W.; In ’t Veen, J.C.C.M.; van den Toorn, L.M.; Overbeek, M.J.; Grootenboers, M.J.; Heller, R.; Mostard, R.L.; Poell, L.H.; et al. Daily home spirometry to detect early steroid treatment effects in newly treated pulmonary sarcoidosis. Eur. Respir. J. 2018, 51, 1702089. [Google Scholar] [CrossRef]
- Gibson, G.J.; Prescott, R.J.; Muers, M.F.; Middleton, W.G.; Mitchell, D.N.; Connolly, C.K.; Harrison, B.D. British Thoracic Society Sarcoidosis study: Effects of long term corticosteroid treatment. Thorax 1996, 51, 238–247. [Google Scholar] [CrossRef]
- Judson, M.A. An approach to the treatment of pulmonary sarcoidosis with corticosteroids: The six phases of treatment. Chest 1999, 115, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Reich, J.M. Mortality of intrathoracic sarcoidosis in referral vs population-based settings: Influence of stage, ethnicity, and corticosteroid therapy. Chest 2002, 121, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Judson, M.A.; Chaudhry, H.; Louis, A.; Lee, K.; Yucel, R. The effect of corticosteroids on quality of life in a sarcoidosis clinic: The results of a propensity analysis. Respir. Med. 2015, 109, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.A.; Donatelli, C.V.; Tonelli, A.R.; Wiesen, J.; Neto, M.L.R.; Sahoo, D.; Culver, D.A. Toxicity risk from glucocorticoids in sarcoidosis patients. Respir. Med. 2017, 132, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Price, D.B.; Trudo, F.; Voorham, J.; Xu, X.; Kerkhof, M.; Jie, J.L.Z.; Tran, T.N. Adverse outcomes from initiation of systemic corticosteroids for asthma: Long-term observational study. J. Asthma Allergy 2018, 11, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Thillai, M.; Chang, W.; Chaudhuri, N.; Forrest, I.; Ho, L.-P.; Lines, S.; Maher, T.M.; Spencer, L.G.; Spiteri, M.; Coker, R. Sarcoidosis in the UK: Insights from British Thoracic Society registry data. BMJ Open Respir. Res. 2019, 6, e000357. [Google Scholar] [CrossRef]
- Selroos, O.; Lofroos, A.B.; Pietinalho, A.; Niemisto, M.; Riska, H. Inhaled budesonide for maintenance treatment of pulmonary sarcoidosis. Sarcoidosis 1994, 11, 126–131. [Google Scholar]
- Erkkilä, S.; Fröseth, B.; E Hellström, P.; Kaltiokallio, K.; Taskinen, E.; Viljanen, A.; Viljanen, B.; Selroos, O. Inhaled budesonide influences cellular and biochemical abnormalities in pulmonary sarcoidosis. Sarcoidosis 1988, 5, 106–110. [Google Scholar]
- Spiteri, M.; Newman, S.; Clarke, S.; Poulter, L. Inhaled corticosteroids can modulate the immunopathogenesis of pulmonary sarcoidosis. Eur. Respir. J. 1989, 2, 218–224. [Google Scholar] [CrossRef]
- Baughman, R.P.; Iannuzzi, M.C.; E Lower, E.; Moller, D.R.; Balkissoon, R.C.; Winget, D.B.; Judson, M.A. Use of fluticasone in acute symptomatic pulmonary sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2002, 19, 198–204. [Google Scholar]
- Milman, N.; Graudal, N.; Grode, G.; Munch, E. No effect of high-dose inhaled steroids in pulmonary sarcoidosis: A double-blind, placebo-controlled study. J. Intern. Med. 1994, 236, 285–290. [Google Scholar] [CrossRef]
- Alberts, C.; van der Mark, T.W.; Jansen, H.M. Inhaled budesonide in pulmonary sarcoidosis: A double-blind, placebo-controlled study. Dutch Study Group on Pulmonary Sarcoidosis. Eur. Respir. J. 1995, 8, 682–688. [Google Scholar] [CrossRef]
- Paramothayan, S.; Lasserson, T.; Walters, E.H. Immunosuppressive and cytotoxic therapy for pulmonary sarcoidosis. Cochrane Database Syst. Rev. 2006, 3, CD003536. [Google Scholar] [CrossRef] [PubMed]
- Vorselaars, A.D.M.; Culver, D.A. Hit-hard and early versus step-up treatment in severe sarcoidosis. Curr. Opin. Pulm. Med. 2022, 28, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Ziegenhagen, M.W.; Rothe, M.E.; Zissel, G.; Muller-Quernheim, J. Exaggerated TNFalpha release of alveolar macrophages in corticosteroid resistant sarcoidosis. Sarcoidosis Vasc. Diffuse Lung Dis. 2002, 19, 185–190. [Google Scholar] [PubMed]
- Fraenkel, L.; Bathon, J.M.; England, B.R.; St. Clair, E.W.; Arayssi, T.; Carandang, K.; Deane, K.D.; Genovese, M.; Huston, K.K.; Kerr, G.; et al. 2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Rheumatol. 2021, 73, 1108–1123. [Google Scholar] [CrossRef] [PubMed]
- Talley, N.J.; Abreu, M.T.; Achkar, J.-P.; Bernstein, C.N.; Dubinsky, M.C.; Hanauer, S.B.; Kane, S.V.; Sandborn, W.J.; Ullman, T.A.; Moayyedi, P.; et al. An evidence-based systematic review on medical therapies for inflammatory bowel disease. Am. J. Gastroenterol. 2011, 106 (Suppl. 1), S2–S25, quiz S6. [Google Scholar] [CrossRef]
- Cremers, J.P.; Drent, M.; Bast, A.; Shigemitsu, H.; Baughman, R.P.; Valeyre, D.; Sweiss, N.J.; Jansen, T.L. Multinational evidence-based World Association of Sarcoidosis and Other Granulomatous Disorders recommendations for the use of methotrexate in sarcoidosis: Integrating systematic literature research and expert opinion of sarcoidologists worldwide. Curr. Opin. Pulm. Med. 2013, 19, 545–561. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.P.; Winget, D.B.; Lower, E.E. Methotrexate is steroid sparing in acute sarcoidosis: Results of a double blind, randomized trial. Sarcoidosis Vasc. Diffuse Lung Dis. 2000, 17, 60–66. [Google Scholar] [PubMed]
- Jekic, B.; Maksimovic, N.; Damnjanovic, T. Methotrexate pharmacogenetics in the treatment of rheumatoid arthritis. Pharmacogenomics 2019, 20, 1235–1245. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Zhang, Q.; Wang, N.; Jing, X.; Xu, Z. Effectiveness and tolerability of methotrexate in pulmonary sarcoidosis: A single center real-world study. Sarcoidosis Vasc. Diffus. Lung Dis. 2019, 36, 217–227. [Google Scholar]
- Shea, B.; Swinden, M.V.; Ghogomu, E.T.; Ortiz, Z.; Katchamart, W.; Rader, T.; Bombardier, C.; Wells, G.A.; Tugwell, P. Folic acid and folinic acid for reducing side effects in patients receiving methotrexate for rheumatoid arthritis. Cochrane Database Syst. Rev. 2013, 2013, CD000951. [Google Scholar] [CrossRef]
- Kahlmann, V.; Janssen Bonás, M.; Moor, C.C.; van Moorsel, C.H.; Kool, M.; Kraaijvanger, R.; Grutters, J.C.; Overgaauw, M.; Veltkamp, M.; Wijsenbeek, M.S.; et al. Design of a randomized controlled trial to evaluate effectiveness of methotrexate versus prednisone as first-line treatment for pulmonary sarcoidosis: The PREDMETH study. BMC Pulm. Med. 2020, 20, 271. [Google Scholar] [CrossRef] [PubMed]
- Vorselaars, A.D.; Wuyts, W.A.; Vorselaars, V.M.; Zanen, P.; Deneer, V.H.; Veltkamp, M.; Thomeer, M.; van Moorsel, C.H.; Grutters, J.C. Methotrexate vs azathioprine in second-line therapy of sarcoidosis. Chest 2013, 144, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Muller-Quernheim, J.; Kienast, K.; Held, M.; Pfeifer, S.; Costabel, U. Treatment of chronic sarcoidosis with an azathioprine/prednisolone regimen. Eur. Respir. J. 1999, 14, 1117–1122. [Google Scholar] [CrossRef]
- Lewis, S.J.; Ainslie, G.M.; Bateman, E.D. Efficacy of azathioprine as second-line treatment in pulmonary sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 1999, 16, 87–92. [Google Scholar]
- Sahoo, D.H.; Bandyopadhyay, D.; Xu, M.; Pearson, K.; Parambil, J.G.; Lazar, C.A.; Chapman, J.T.; Culver, D.A. Effectiveness and safety of leflunomide for pulmonary and extrapulmonary sarcoidosis. Eur. Respir. J. 2011, 38, 1145–1150. [Google Scholar] [CrossRef]
- Baughman, R.P.; Lower, E.E. Leflunomide for chronic sarcoidosis. Sarcoidosis Vasc. Diffuse Lung Dis. 2004, 21, 43–48. [Google Scholar]
- Hamzeh, N.; Voelker, A.; Forssén, A.; Gottschall, E.B.; Rose, C.; Mroz, P.; Maier, L.A. Efficacy of mycophenolate mofetil in sarcoidosis. Respir. Med. 2014, 108, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Brill, A.K.; Ott, S.R.; Geiser, T. Effect and safety of mycophenolate mofetil in chronic pulmonary sarcoidosis: A retrospective study. Respiration 2013, 86, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Lower, E.E.; Sturdivant, M.; Grate, L.; Baughman, R.P. Use of third-line therapies in advanced sarcoidosis. Clin. Exp. Rheumatol. 2020, 38, 834–840. [Google Scholar] [PubMed]
- Baughman, R.P.; Drent, M.; Kavuru, M.; Judson, M.A.; Costabel, U.; Du Bois, R.; Albera, C.; Brutsche, M.; Davis, G.; Donohue, J.F.; et al. Infliximab therapy in patients with chronic sarcoidosis and pulmonary involvement. Am. J. Respir. Crit. Care Med. 2006, 174, 795–802. [Google Scholar]
- Judson, M.A.; Baughman, R.P.; Costabel, U.; Flavin, S.; Lo, K.H.; Kavuru, M.S.; Drent, M. Efficacy of infliximab in extrapulmonary sarcoidosis: Results from a randomised trial. Eur. Respir. J. 2008, 31, 1189–1196. [Google Scholar] [CrossRef]
- Russell, E.; Luk, F.; Manocha, S.; Ho, T.; O’Connor, C.; Hussain, H. Long term follow-up of infliximab efficacy in pulmonary and extra-pulmonary sarcoidosis refractory to conventional therapy. Semin. Arthritis Rheum. 2013, 43, 119–124. [Google Scholar] [CrossRef]
- Judson, M.A.; Adelstein, E.; Fish, K.M.; Feustel, P.J.; Yucel, R.; Preston, S.; Vancavage, R.; Chopra, A.; Steckman, D.A. Outcomes of prednisone-tapering regimens for cardiac sarcoidosis: A retrospective analysis demonstrating a benefit of infliximab. Respir. Med. 2022, 203, 107004. [Google Scholar] [CrossRef]
- Drent, M.; Cremers, J.P.; Jansen, T.L.; Baughman, R.P. Practical eminence and experience-based recommendations for use of TNF-alpha inhibitors in sarcoidosis. Sarcoidosis Vasc. Diffuse Lung Dis. 2014, 31, 91–107. [Google Scholar]
- Radstake, T.R.D.J.; Svenson, M.; Eijsbouts, A.M.; Hoogen, F.H.J.v.D.; Enevold, C.; van Riel, P.L.C.M.; Bendtzen, K. Formation of antibodies against infliximab and adalimumab strongly correlates with functional drug levels and clinical responses in rheumatoid arthritis. Ann. Rheum. Dis. 2009, 68, 1739–1745. [Google Scholar] [CrossRef] [PubMed]
- Pariser, R.J.; Paul, J.; Hirano, S.; Torosky, C.; Smith, M. A double-blind, randomized, placebo-controlled trial of adalimumab in the treatment of cutaneous sarcoidosis. J. Am. Acad. Dermatol. 2013, 68, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Sweiss, N.J.; Noth, I.; Mirsaeidi, M.; Zhang, W.; Naureckas, E.T.; Hogarth, D.K.; Strek, M.; Caligiuri, P.; Machado, R.F.; Niewold, T.B.; et al. Efficacy Results of a 52-week Trial of Adalimumab in the Treatment of Refractory Sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2014, 31, 46–54. [Google Scholar]
- Crommelin, H.A.; van der Burg, L.M.; Vorselaars, A.D.; Drent, M.; van Moorsel, C.H.; Rijkers, G.T.; Deneer, V.H.; Grutters, J.C. Efficacy of adalimumab in sarcoidosis patients who developed intolerance to infliximab. Respir. Med. 2016, 115, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Riancho-Zarrabeitia, L.; Calvo-Río, V.; Blanco, R.; Mesquida, M.; Adan, A.M.; Herreras, J.M.; Aparicio, Á.; Peiteado-Lopez, D.; Cordero-Coma, M.; Serrano, J.L.G.; et al. Anti-TNF-alpha therapy in refractory uveitis associated with sarcoidosis: Multicenter study of 17 patients. Semin. Arthritis Rheum. 2015, 45, 361–368. [Google Scholar] [CrossRef]
- Kamphuis, L.S.; Lam-Tse, W.-K.; Dik, W.A.; van Daele, P.L.; van Biezen, P.; Kwekkeboom, D.J.; Kuijpers, R.W.; Hooijkaas, H.; van Laar, J.A.; Bastiaans, J.; et al. Efficacy of adalimumab in chronically active and symptomatic patients with sarcoidosis. Am. J. Respir. Crit. Care Med. 2011, 184, 1214–1216. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, M.P.; Smith, D.I. Adalimumab for treatment of cutaneous sarcoidosis. Arch. Dermatol. 2006, 142, 17–19. [Google Scholar] [CrossRef]
- Chopra, A.; Nautiyal, A.; Kalkanis, A.; Judson, M.A. Drug-Induced Sarcoidosis-Like Reactions. Chest 2018, 154, 664–677. [Google Scholar] [CrossRef]
- Schimmelpennink, M.C.; Vorselaars, A.D.; van Beek, F.T.; Crommelin, H.A.; Deneer, V.H.; Keijsers, R.G.; Veltkamp, M. Efficacy and safety of infliximab biosimilar Inflectra((R)) in severe sarcoidosis. Respir. Med. 2018, 138, S7–S13. [Google Scholar] [CrossRef]
- Veltkamp, M.; Drent, M.; Baughman, R.P. Infliximab or biosimilars in sarcoidosis; to switch or not to switch? Sarcoidosis Vasc. Diffus. Lung Dis. 2016, 32, 280–283. [Google Scholar]
- Zabel, P.; Entzian, P.; Dalhoff, K.; Schlaak, M. Pentoxifylline in treatment of sarcoidosis. Am. J. Respir. Crit. Care Med. 1997, 155, 1665–1669. [Google Scholar] [CrossRef]
- Tong, Z.; Dai, H.; Chen, B.; Abdoh, Z.; Guzman, J.; Costabel, U. Inhibition of cytokine release from alveolar macrophages in pulmonary sarcoidosis by pentoxifylline: Comparison with dexamethasone. Chest 2003, 124, 1526–1532. [Google Scholar] [CrossRef]
- Utz, J.P.; Limper, A.H.; Kalra, S.; Specks, U.; Scott, J.P.; Vuk-Pavlovic, Z.; Schroeder, D.R. Etanercept for the treatment of stage II and III progressive pulmonary sarcoidosis. Chest 2003, 124, 177–185. [Google Scholar] [CrossRef]
- Judson, M.A.; Baughman, R.P.; Costabel, U.; Drent, M.; Gibson, K.F.; Raghu, G.; Shigemitsu, H.; Barney, J.B.; Culver, D.A.; Hamzeh, N.Y.; et al. Safety and efficacy of ustekinumab or golimumab in patients with chronic sarcoidosis. Eur. Respir. J. 2014, 44, 1296–1307. [Google Scholar] [CrossRef]
- Sweiss, N.J.; Lower, E.E.; Mirsaeidi, M.; Dudek, S.; Garcia, J.G.N.; Perkins, D.; Finn, P.W.; Baughman, R.P. Rituximab in the treatment of refractory pulmonary sarcoidosis. Eur. Respir. J. 2014, 43, 1525–1528. [Google Scholar] [CrossRef] [PubMed]
- Damsky, W.; Wang, A.; Kim, D.J.; Young, B.D.; Singh, K.; Murphy, M.J.; Daccache, J.; Clark, A.; Ayasun, R.; Ryu, C.; et al. Inhibition of type 1 immunity with tofacitinib is associated with marked improvement in longstanding sarcoidosis. Nat. Commun. 2022, 13, 3140. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Huang, Z.; Liu, Q.; Wei, J.C. Tofacitinib for sarcoidosis, a new potential treatment. Int. J. Rheum. Dis. 2022, 25, 1217–1219. [Google Scholar] [CrossRef] [PubMed]
- Collaborative group MIsg. Glucocorticoid sparing in sarcoidosis using the Janus kinase (JAK) inhibitor tofacitinib. Eur. J. Intern. Med. 2022, 98, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Sharp, M.; Donnelly, S.C.; Moller, D.R. Tocilizumab in sarcoidosis patients failing steroid sparing therapies and anti-TNF agents. Respir. Med. X 2019, 1, 100004. [Google Scholar] [CrossRef] [PubMed]
- Julian, M.W.; Shao, G.; Schlesinger, L.S.; Huang, Q.; Cosmar, D.G.; Bhatt, N.Y.; Culver, D.A.; Baughman, R.P.; Wood, K.L.; Crouser, E.D. Nicotine treatment improves Toll-like receptor 2 and Toll-like receptor 9 responsiveness in active pulmonary sarcoidosis. Chest 2013, 143, 461–470. [Google Scholar] [CrossRef]
- Baughman, R.P.; Sweiss, N.; Keijsers, R.; Birring, S.S.; Shipley, R.; Saketkoo, L.A.; Lower, E.E. Repository corticotropin for Chronic Pulmonary Sarcoidosis. Lung 2017, 195, 313–322. [Google Scholar] [CrossRef]
- Mirsaeidi, M.; Baughman, R.P. Repository Corticotropin Injection for the Treatment of Pulmonary Sarcoidosis: A Narrative Review. Pulm. Ther. 2022, 8, 43–55. [Google Scholar] [CrossRef]
- Culver, D.A.; Aryal, S.; Barney, J.; Hsia, C.C.; James, W.E.; Maier, L.A.; Marts, L.T.; Obi, O.N.; Sporn, P.H.; Sweiss, N.J.; et al. Efzofitimod for the Treatment of Pulmonary Sarcoidosis. Chest 2023, 163, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Walker, G.; Adams, R.; Guy, L.; Chandrasekaran, A.; Kinnersley, N.; Ramesh, P.; Zhang, L.; Brown, F.; Niranjan, V. Exposure-response analyses of efzofitimod in patients with pulmonary sarcoidosis. Front. Pharmacol. 2023, 14, 1258236. [Google Scholar] [CrossRef]
- Bass, A.R.; Chakravarty, E.; Akl, E.A.; Bingham, C.O.; Calabrese, L.; Cappelli, L.C.; Johnson, S.R.; Imundo, L.F.; Winthrop, K.L.; Arasaratnam, R.J.; et al. 2022 American College of Rheumatology Guideline for Vaccinations in Patients with Rheumatic and Musculoskeletal Diseases. Arthritis Rheumatol. 2023, 75, 333–348. [Google Scholar] [CrossRef] [PubMed]
- Ledingham, J.; Gullick, N.; Irving, K.; Gorodkin, R.; Aris, M.; Burke, J.; Gordon, P.; Christidis, D.; Galloway, S.; Hayes, E.; et al. BSR and BHPR guideline for the prescription and monitoring of non-biologic disease-modifying anti-rheumatic drugs. Rheumatology 2017, 56, 865–868. [Google Scholar] [CrossRef] [PubMed]
- Wilsdon, T.D.; Hill, C.L. Managing the drug treatment of rheumatoid arthritis. Aust. Prescr. 2017, 40, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Onel, K.B.; Horton, D.B.; Lovell, D.J.; Shenoi, S.; Cuello, C.A.; Angeles-Han, S.T.; Becker, M.L.; Cron, R.Q.; Feldman, B.M.; Ferguson, P.J.; et al. 2021 American College of Rheumatology Guideline for the Treatment of Juvenile Idiopathic Arthritis: Therapeutic Approaches for Oligoarthritis, Temporomandibular Joint Arthritis, and Systemic Juvenile Idiopathic Arthritis. Arthritis Rheumatol. 2022, 74, 553–569. [Google Scholar] [CrossRef]
- Flaherty, K.R.; Wells, A.U.; Cottin, V.; Devaraj, A.; Walsh, S.L.; Inoue, Y.; Richeldi, L.; Kolb, M.; Tetzlaff, K.; Stowasser, S.; et al. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. N. Engl. J. Med. 2019, 381, 1718–1727. [Google Scholar] [CrossRef]
- Taimeh, Z.; I Hertz, M.; Shumway, S.; Pritzker, M. Lung transplantation for pulmonary sarcoidosis. Twenty-five years of experience in the USA. Thorax 2016, 71, 378–379. [Google Scholar] [CrossRef]
- Hider, S.L.; Bruce, I.N.; Thomson, W. The pharmacogenetics of methotrexate. Rheumatology 2007, 46, 1520–1524. [Google Scholar] [CrossRef] [PubMed]
- Cuffari, C.; Dassopoulos, T.; Turnbough, L.; Thompson, R.E.; Bayless, T.M. Thiopurine methyltransferase activity influences clinical response to azathioprine in inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2004, 2, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Wijnen, P.A.; Cremers, J.P.; Nelemans, P.J.; Erckens, R.J.; Hoitsma, E.; Jansen, T.L.; Bekers, O.; Drent, M. Association of the TNF-alpha G-308A polymorphism with TNF-inhibitor response in sarcoidosis. Eur. Respir. J. 2014, 43, 1730–1739. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.P.; Judson, M.A. Relapses of sarcoidosis: What are they and can we predict who will get them? Eur. Respir. J. 2014, 43, 337–339. [Google Scholar] [CrossRef]
- Gottlieb, J.E.; Israel, H.L.; Steiner, R.M.; Triolo, J.; Patrick, H. Outcome in sarcoidosis. The relationship of relapse to corticosteroid therapy. Chest 1997, 111, 623–631. [Google Scholar] [CrossRef]
- McKinzie, B.P.; Bullington, W.M.; Mazur, J.E.; Judson, M.A. Efficacy of short-course, low-dose corticosteroid therapy for acute pulmonary sarcoidosis exacerbations. Am. J. Med. Sci. 2010, 339, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Panselinas, E.; Judson, M.A. Acute pulmonary exacerbations of sarcoidosis. Chest 2012, 142, 827–836. [Google Scholar] [CrossRef]
- Vorselaars, A.D.; Verwoerd, A.; van Moorsel, C.H.; Keijsers, R.G.; Rijkers, G.T.; Grutters, J.C. Prediction of relapse after discontinuation of infliximab therapy in severe sarcoidosis. Eur. Respir. J. 2014, 43, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Jin, R.; Wang, Y.; Li, L.; Li, K.; He, Y. The Utility of (18)F-FDG PET/CT for Monitoring Response and Predicting Prognosis after Glucocorticoids Therapy for Sarcoidosis. Biomed. Res. Int. 2018, 2018, 1823710. [Google Scholar]
- Teirstein, A.S.; Machac, J.; Almeida, O.; Lu, P.; Padilla, M.L.; Iannuzzi, M.C. Results of 188 whole-body fluorodeoxyglucose positron emission tomography scans in 137 patients with sarcoidosis. Chest 2007, 132, 1949–1953. [Google Scholar] [CrossRef]
- Vorselaars, A.D.M.; Crommelin, H.A.; Deneer, V.H.M.; Meek, B.; Claessen, A.M.E.; Keijsers, R.G.M.; Van Moorsel, C.H.M.; Grutters, J.C. Effectiveness of infliximab in refractory FDG PET-positive sarcoidosis. Eur. Respir. J. 2015, 46, 175–185. [Google Scholar] [CrossRef]
- Patterson, K.C.; Strek, M.E. Pulmonary fibrosis in sarcoidosis. Clinical features and outcomes. Ann. Am. Thorac. Soc. 2013, 10, 362–370. [Google Scholar] [CrossRef]
- Francesqui, J.; Marrades, P.; Sellares, J. Personalized medicine in sarcoidosis: Unravelling biomarkers for targeted care. Curr. Opin. Pulm. Med. 2023, 29, 478–484. [Google Scholar] [CrossRef]
- VVorselaars, A.D.; van Moorsel, C.H.; Zanen, P.; Ruven, H.J.; Claessen, A.M.; van Velzen-Blad, H.; Grutters, J.C. ACE and sIL-2R correlate with lung function improvement in sarcoidosis during methotrexate therapy. Respir. Med. 2015, 109, 279–285. [Google Scholar] [CrossRef]
- Drent, M.; Jacobs, J.A.; De Vries, J.; Lamers, R.S.; Liem, I.H.; Wouters, E.F. Does the cellular bronchoalveolar lavage fluid profile reflect the severity of sarcoidosis? Eur. Respir. J. 1999, 13, 1338–1344. [Google Scholar] [CrossRef]
- Ramstein, J.; Broos, C.E.; Simpson, L.J.; Ansel, K.M.; Sun, S.A.; Ho, M.E.; Woodruff, P.G.; Bhakta, N.R.; Christian, L.; Nguyen, C.P.; et al. IFN-gamma-Producing T-Helper 17.1 Cells Are Increased in Sarcoidosis and Are More Prevalent than T-Helper Type 1 Cells. Am. J. Respir. Crit. Care Med. 2016, 193, 1281–1291. [Google Scholar] [CrossRef]
- Broos, C.E.; Koth, L.L.; van Nimwegen, M.; In ’t Veen, J.C.C.M.; Paulissen, S.M.; van Hamburg, J.P.; Annema, J.T.; Heller-Baan, R.; Kleinjan, A.; Hoogsteden, H.C.; et al. Increased T-helper 17.1 cells in sarcoidosis mediastinal lymph nodes. Eur. Respir. J. 2018, 51, 1701124. [Google Scholar] [CrossRef]
- Jiang, Y.; Jiang, D.; Costabel, U.; Dai, H.; Wang, C. A transcriptomics-based meta-analysis identifies a cross-tissue signature for sarcoidosis. Front. Med. 2022, 9, 960266. [Google Scholar] [CrossRef] [PubMed]
- Casanova, N.G.; Reyes-Hernon, V.; Gregory, T.; Sun, B.; Bermudez, T.; Hufford, M.K.; Oita, R.C.; Camp, S.M.; Hernandez-Molina, G.; Serrano, J.R.; et al. Biochemical and genomic identification of novel biomarkers in progressive sarcoidosis: HBEGF, eNAMPT, and ANG-2. Front. Med. 2022, 9, 1012827. [Google Scholar] [CrossRef] [PubMed]
- Lew, D.; Klang, E.; Soffer, S.; Morgenthau, A.S. Current Applications of Artificial Intelligence in Sarcoidosis. Lung 2023, 201, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S.M.; Fingerlin, T.E.; Mroz, M.; Barkes, B.; Hamzeh, N.; Maier, L.A.; Carlson, N.E. Radiomic measures from chest high-resolution computed tomography associated with lung function in sarcoidosis. Eur. Respir. J. 2019, 54, 1900371. [Google Scholar] [CrossRef] [PubMed]
- Bade, G.; Akhtar, N.; Trivedi, A.; Madan, K.; Guleria, R.; Talwar, A. Impulse Oscillometry as a measure of airway dysfunction in Sarcoidosis. Sarcoidosis Vasc. Diffuse Lung Dis. 2021, 38, e2021037. [Google Scholar] [PubMed]
- Baghdadi, N.; Maklad, A.S.; Malki, A.; Deif, M.A. Reliable Sarcoidosis Detection Using Chest X-rays with EfficientNets and Stain-Normalization Techniques. Sensors 2022, 22, 3846. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Corticosteroid Toxicity | Clinical Considerations |
|---|---|
| Suppression of the hypothalamic-pituitary-adrenal axis |
|
| Increased susceptibility to infection |
|
| Weight gain |
|
| Ocular complications: cataracts, glaucoma |
|
| Impaired bone density |
|
| Steroid-induced myopathy |
|
| Dermatologic effects: skin thinning, bruising, acne, Cushingoid features |
|
| Fluid retention |
|
| Hypertension |
|
| Gastric irritation and ulcer disease |
|
| Hyperglycemia |
|
| Insomnia, Dysthymia, and Psychosis |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerke, A.K. Treatment of Granulomatous Inflammation in Pulmonary Sarcoidosis. J. Clin. Med. 2024, 13, 738. https://doi.org/10.3390/jcm13030738
Gerke AK. Treatment of Granulomatous Inflammation in Pulmonary Sarcoidosis. Journal of Clinical Medicine. 2024; 13(3):738. https://doi.org/10.3390/jcm13030738
Chicago/Turabian StyleGerke, Alicia K. 2024. "Treatment of Granulomatous Inflammation in Pulmonary Sarcoidosis" Journal of Clinical Medicine 13, no. 3: 738. https://doi.org/10.3390/jcm13030738
APA StyleGerke, A. K. (2024). Treatment of Granulomatous Inflammation in Pulmonary Sarcoidosis. Journal of Clinical Medicine, 13(3), 738. https://doi.org/10.3390/jcm13030738