
Cardiac Arrest During Exertion as a Presentation of Undiagnosed Kawasaki Disease: A Case Report

 , , and
, , and
Abstract
1. Introduction
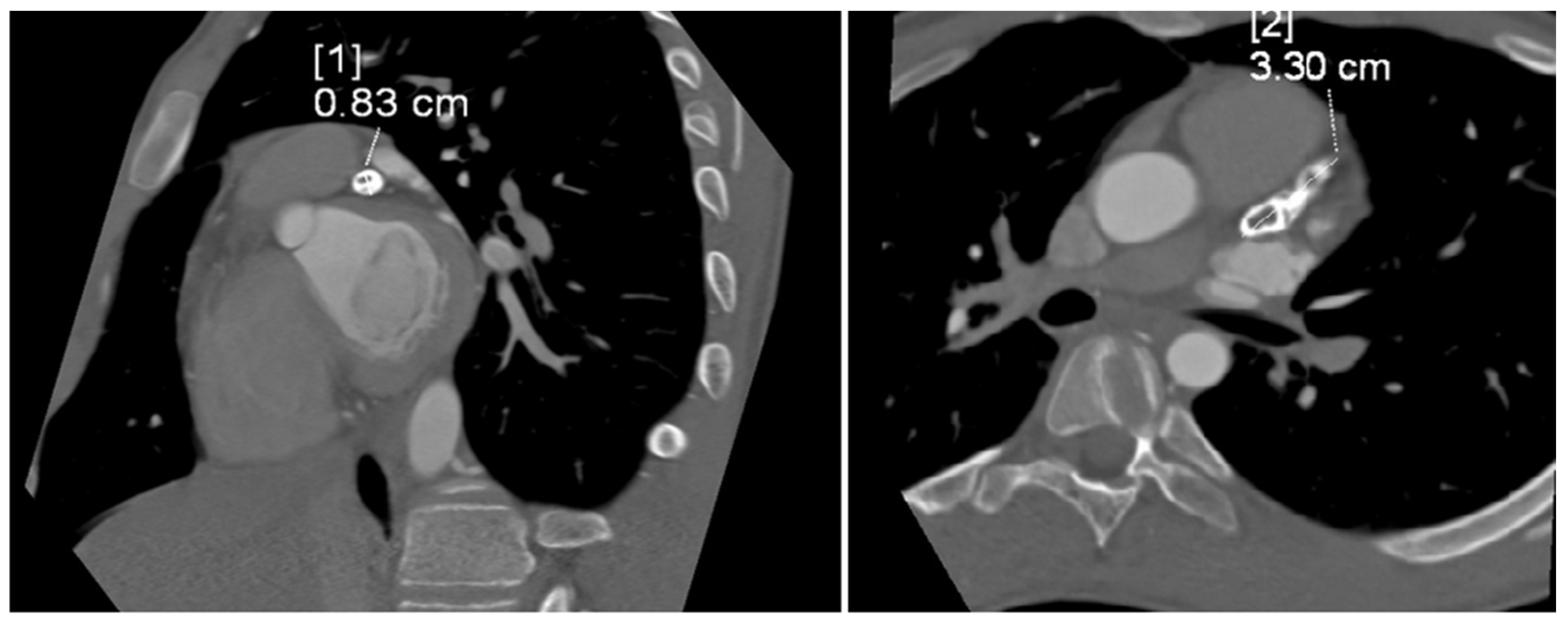
Case Presentation
2. Discussion
3. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alexoudi, I.; Kanakis, M.; Kapsimali, V.; Vaiopoulos, G. Kawasaki disease: Current aspects on aetiopathogenesis and therapeutic management. Autoimmun. Rev. 2011, 10, 544–547. [Google Scholar] [CrossRef] [PubMed]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals from the American Heart Association. Circulation 2017, 135, e927–e999, Correction in Circulation 2019, 140, e181–e184. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, T. Acute febril mucocutaneous syndrome with lymphoid involvement with specific sesquamation of fingers and toes in children. Arerugi 1967, 16, 178–222. [Google Scholar] [PubMed]
- Newburger, J.W.; Takahashi, M.; Gerber, M.A.; Gewitz, M.H.; Tani, L.Y.; Burns, J.C.; Shulman, S.T.; Bolger, A.F.; Ferrieri, P.; Baltimore, R.S.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004, 110, 2747–2771. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.H.; Phi, J.H.; Kang, H.S.; Wang, K.C.; Cho, B.K.; Lee, J.Y.; Kim, G.B.; Kim, S.K. A ruptured middle cerebral artery aneurysm in a 13-month-old boy with Kawasaki disease. J. Neurosurg. Pediatr. 2010, 6, 150–153. [Google Scholar] [CrossRef]
- Fukazawa, R.; Kobayashi, J.; Ayusawa, M.; Hamada, H.; Miura, M.; Mitani, Y.; Tsuda, E.; Nakajima, H.; Matsuura, H.; Ikeda, K.; et al. JCS/JSCS 2020 Guideline on Diagnosis and Management of Cardiovascular Sequelae in Kawasaki Disease. Circ. J. 2020, 84, 1348–1407. [Google Scholar] [CrossRef]
- Li, T.; Feng, J.; Li, N.; Liu, T. Correct identification of incomplete Kawasaki disease. J. Int. Med. Res. 2021, 49, 03000605211001712. [Google Scholar] [CrossRef]
- Rife, E.; Gedalia, A. Kawasaki Disease: An Update. Rev. Curr. Rheumatol. Rep. 2020, 22, 75. [Google Scholar] [CrossRef]
- Kuo, H.C. Diagnosis, Progress, and Treatment Update of Kawasaki Disease. Int. J. Mol. Sci. 2023, 24, 13948. [Google Scholar] [CrossRef]
- Seki, M.; Minami, T. Kawasaki Disease: Pathology, Risks, and Management. Rev. Vasc. Health Risk Manag. 2022, 18, 407–416. [Google Scholar] [CrossRef]
- Scherler, L.; Haas, N.A.; Tengler, A.; Pattathu, J.; Mandilaras, G.; Jakob, A. Acute phase of Kawasaki disease: A review of national guideline recommendations. Eur. J. Pediatr. 2022, 181, 2563–2573. [Google Scholar] [CrossRef] [PubMed]
- Eleftheriou, D.; Levin, M.; Shingadia, D.; Tulloh, R.; Klein, N.J.; Brogan, P.A. Management of Kawasaki disease. Arch. Dis. Child. 2014, 99, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Brogan, P.; Burns, J.C.; Cornish, J.; Diwakar, V.; Eleftheriou, D.; Gordon, J.B.; Gray, H.H.; Johnson, T.W.; Levin, M.; Malik, I.; et al. Kawasaki Disease Writing Group, on behalf of the Royal College of Paediatrics and Child Health, and the British Cardiovascular Society. Lifetime cardiovascular management of patients with previous Kawasaki disease. Heart 2020, 106, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Singhal, M.; Vignesh, P.; Khandelwal, N.; Singh, S. Calcified Saccular Coronary Artery Aneurysm of Kawasaki Disease. J. Clin. Rheumatol. 2020, 26, e96. [Google Scholar] [CrossRef]
- Langen, H.J.; Schirp, B.; Hofstetter, R. Verkalktes Koronararterienaneurysma nach Kawasaki-Syndrom [A calcified coronary artery aneurysm following Kawasaki syndrome]. Radiologe 1991, 31, 571–573. [Google Scholar]
- Yokouchi, Y.; Oharaseki, T.; Asakawa, N.; Makino, H.; Takahashi, K. Histological studies shed new light on the initiation and characteristics of calcification of coronary artery aneurysms in Kawasaki disease. Cardiovasc. Pathol. 2022, 61, 107456. [Google Scholar] [CrossRef]
- Song, J.; Gong, S.J.; Yu, Y.H. Coronary aneurysm with calcification in a young adult: An unusual cause of cardiac arrest. Med. Intensiv. (Engl. Ed.) 2019, 43, 453–454. [Google Scholar] [CrossRef]
- Pilania, R.K.; Singhal, M.; Singh, S. Dense calcifications of giant coronary aneurysms in an 11-year-old girl with Kawasaki disease. Rheumatology 2021, 60, 4441–4442. [Google Scholar] [CrossRef]
- Kobayashi, T.; Inoue, Y.; Takeuchi, K.; Okada, Y.; Tamura, K.; Tomomasa, T.; Kobayashi, T.; Morikawa, A. Prediction of intravenous immunoglobulin unresponsiveness in patients with Kawasaki disease. Circulation 2006, 113, 606–612. [Google Scholar] [CrossRef]
- Suzuki, D.; Suzuki, T.; Fujino, M.; Asai, Y.; Kojima, A.; Uchida, H.; Saito, K.; Kusuki, H.; Li, Y.; Yatsuya, H.; et al. The electrophysiological index can effectively predict subsequent coronary artery aneurysm in children with Kawasaki disease. Fujita Med. J. 2023, 4, 275–281. [Google Scholar] [CrossRef]
- Burns, J.C. The etiologies of Kawasaki disease. J. Clin. Investig. 2024, 134, e176938. [Google Scholar] [CrossRef] [PubMed]
- Ayusawa, M.; Namiki, H.; Abe, Y.; Ichikawa, R.; Morioka, I. Sudden Death in Patients with a History of Kawasaki Disease under School Supervision. Children 2022, 21, 1593. [Google Scholar] [CrossRef] [PubMed]
- Pham, V.; de Hemptinne, Q.; Grinda, J.M.; Duboc, D.; Varenne, O.; Picard, F. Giant coronary aneurysms, from diagnosis to treatment: A literature review. Arch. Cardiovasc. Dis. 2020, 113, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.C.; Shike, H.; Gordon, J.B.; Malhotra, A.; Schoenwetter, M.; Kawasaki, T. Sequelae of Kawasaki disease in adolescents and young adults. J. Am. Coll. Cardiol. 1996, 28, 253–257. [Google Scholar] [CrossRef]
- Rizk, S.R.Y.; El Said, G.; Daniels, L.B.; Burns, J.C.; El Said, H.; Sorour, K.A.; Gharib, S.; Gordon, J.B. Acute myocardial ischemia in adults secondary to missed Kawasaki disease in childhood. Am. J. Cardiol. 2015, 115, 423–427. [Google Scholar] [CrossRef]
- Pahlavan, P.S.; Niroomand, F. Coronary artery aneurysm: A review. Clin. Cardiol. 2006, 29, 39–43. [Google Scholar] [CrossRef]
- Sheikh, A.S.; Hailan, A.; Kinnaird, T.; Choudhury, A.; Smith, D. Coronary Artery Aneurysm: Evaluation, Prognosis, and Proposed Treatment Strategies. Heart Views 2019, 20, 101–108. [Google Scholar] [CrossRef]
- Uzdavinyte Gateliene, E.; Cesnaite, G.; Sadauskiene, E.; Barysiene, J. Late diagnosis of Kawasaki disease with major cardiovascular complications: A case report. Eur. Heart J. Case Rep. 2023, 7, ytad486. [Google Scholar] [CrossRef]
- Sliem, A.; Siu, A.; Zheng, J.; Magana, S.; Alagha, Z.; Ghallab, M.; Lopez, M. Cardiac Arrest as the Initial Presentation of Undiagnosed Kawasaki Disease: A Case Report and Literature Review. Cureus 2023, 15, e40855. [Google Scholar] [CrossRef]
- Zhang, J.; Tuokan, T.; Shi, Y. Sudden Death as a Sequel of Ruptured Giant Coronary Artery Aneurysm in Kawasaki Disease. Am. J. Forensic. Med. Pathol. 2018, 39, 375–377. [Google Scholar] [CrossRef]
- Fukazawa, R.; Kobayashi, T.; Mikami, M.; Saji, T.; Hamaoka, K.; Kato, H.; Suzuki, H.; Tsuda, E.; Ayusawa, M.; Miura, M.; et al. Nationwide Survey of Patients with Giant Coronary Aneurysm Secondary to Kawasaki Disease 1999–2010 in Japan. Circ. J. 2017, 82, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Stahl, E.P.; Forouzandeh, F.; Little, B.P.; Samady, H. Young Athlete with Complex Aneurysmal Coronary Stenosis. J. Invasive Cardiol. 2017, 12, E197–E198. [Google Scholar]
- Zhu, K.F.; Tang, L.J.; Wu, S.Z.; Tang, Y.M. Out-of-hospital cardiac arrest in a young adult survivor with sequelae of childhood Kawasaki disease: A case report. World J. Clin. Cases 2019, 21, 3583–3589. [Google Scholar] [CrossRef] [PubMed]
- Motta, J.; Abozenah, M.; Farah, M.; Khawaja, U.; McAuliffe, M.T.; Kadado, A.J.; Chalhoub, F. Kawasaki disease: A rare cause of sudden cardiac death. JACC 2024, 83, 4557. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Authors, Date of Publication | Sex, Age | Initial Diagnosis | Coronary Artery Involvement | Follow-Up |
|---|---|---|---|---|
| Uzdavinyte Gateliene et al., 2023 [28] | F, 25 years old | myocarditis | LAD, RCA | survived |
| Sliem et al., 2023 [29] | F, 29 years old | myocardial infarction | LAD | survived |
| Zhang et al., 2018 [30] | M, 5 years old | mumps and scarlet fever | LAD | died |
| Stahl et al., 2019 [32] | M, 14 years old | cardiac arrest | LAD, RCA | survived |
| Zhu et al., 2019 [33] | M, 29 years old | cardiac arrest, embolism | LAD, RCA | survived |
| Motta et al., 2024 [34] | M, 17 years old | cardiac arrest | LMCA, RCA | survived |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamojska, J.; Kędziora, P.; Januś, A.; Kaczmarek, K.; Smolewska, E. Cardiac Arrest During Exertion as a Presentation of Undiagnosed Kawasaki Disease: A Case Report. J. Clin. Med. 2024, 13, 6380. https://doi.org/10.3390/jcm13216380
Zamojska J, Kędziora P, Januś A, Kaczmarek K, Smolewska E. Cardiac Arrest During Exertion as a Presentation of Undiagnosed Kawasaki Disease: A Case Report. Journal of Clinical Medicine. 2024; 13(21):6380. https://doi.org/10.3390/jcm13216380
Chicago/Turabian StyleZamojska, Justyna, Piotr Kędziora, Agnieszka Januś, Krzysztof Kaczmarek, and Elżbieta Smolewska. 2024. "Cardiac Arrest During Exertion as a Presentation of Undiagnosed Kawasaki Disease: A Case Report" Journal of Clinical Medicine 13, no. 21: 6380. https://doi.org/10.3390/jcm13216380
APA StyleZamojska, J., Kędziora, P., Januś, A., Kaczmarek, K., & Smolewska, E. (2024). Cardiac Arrest During Exertion as a Presentation of Undiagnosed Kawasaki Disease: A Case Report. Journal of Clinical Medicine, 13(21), 6380. https://doi.org/10.3390/jcm13216380