
Impact of Home Mobile Phone-Based Telemonitoring in Preventing Exacerbations and Hospitalizations Among Patients with Chronic Obstructive Pulmonary Disease: An IMTEC Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. The Study Design
2.2. Study Population
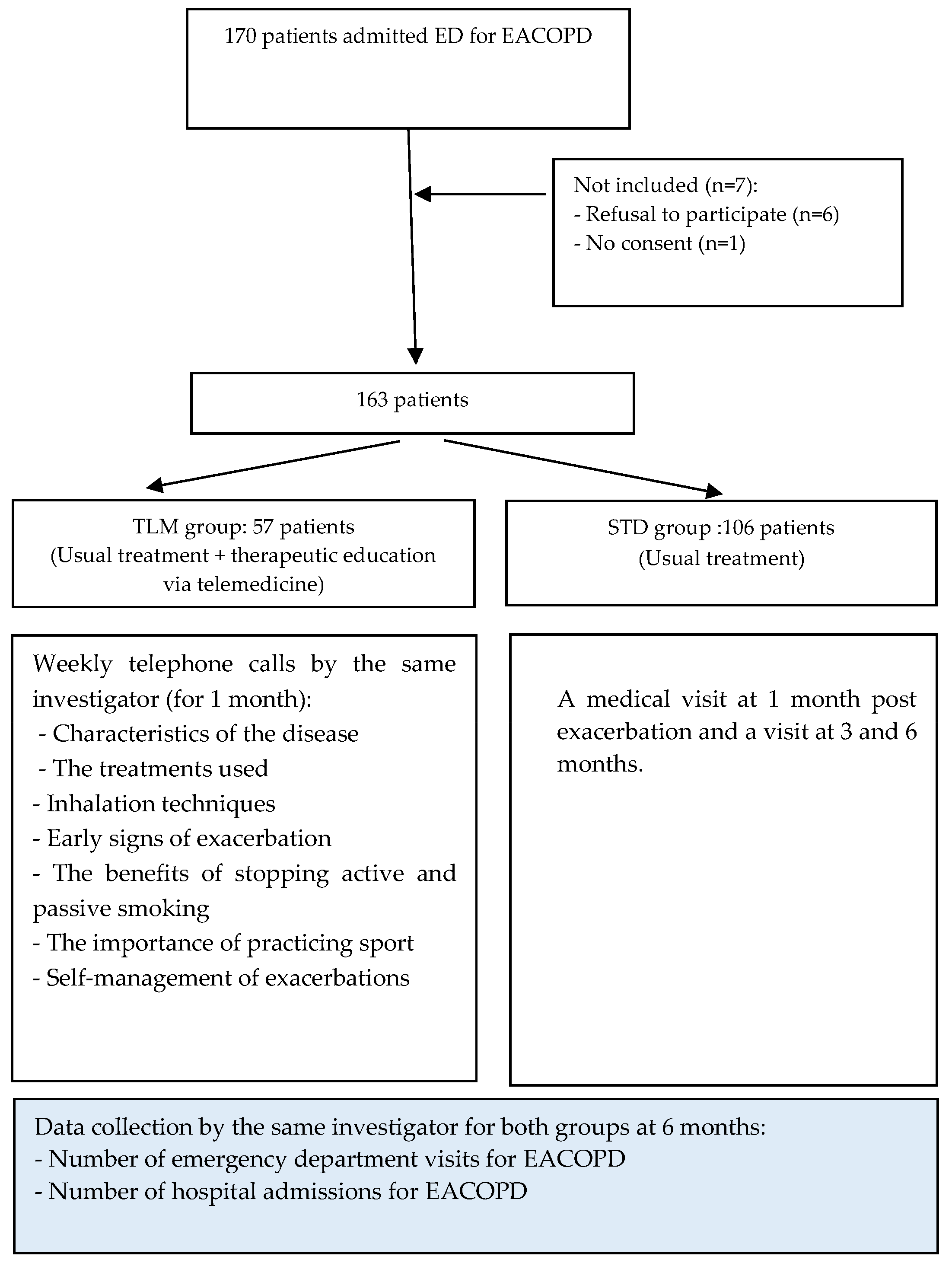
2.3. Study Protocol
- Standard care group (STD): patients will receive usual follow-up via a pulmonology consultation at 1, 3, and 6 months after hospital discharge.
- Telemonitoring group (TLM): patients included in this group will be monitored via weekly telephone calls by the same investigator experienced in COPD and telehealth for 1 month after hospital discharge, and thereafter they have a programmed consultation at 1, 3, and 6 months of follow-up.
2.4. Outcomes
2.4.1. Primary Outcome
2.4.2. Secondary Outcome
2.5. Statical Analyses
- N = total sample size (total number of participants);
- n = number of events require;
- r is the ratio of participants in the experimental group to the control group;
- Zα/2 = 1.96 (for a 5% significance level);
- Zβ = 0.84 (for 80% power);
- Hazard ratio HR = 0.66;
- Proportion of events p = 0.45 (control group);
- EER = expected event rate.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; de Oca, M.M.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur. Respir. J. 2023, 61, 2300239. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A.; Wells, C.K. Evaluation of clinical methods for rating dyspnea. Chest 1988, 93, 580586. [Google Scholar] [CrossRef] [PubMed]
- Marcos, P.J.; Represas, C.R.; Ramos, C.; Álvarez, B.C.; Villar, A.F.; Liste, A.F.; Nocelo, S.F.; Del Río, J.Q.; Sanz, C.Z.; Golpe, R.; et al. Impact of a Home Telehealth Program After a Hospitalized COPD Exacerbation: A Propensity Score Analysis. Arch. Bronconeumol. 2022, 58, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Bivolaru, S.; Constantin, A. The Impact of Technical Skills and Education on Exacerbations, Adherence to Treatment and the Choice of Inhaler Device in Patients with COPD. Intern. Med. 2023, 20, 2741. [Google Scholar] [CrossRef]
- Hurst, J.R.; Han, M.K.; Singh, B.; Sharma, S.; Kaur, G.; de Nigris, E.; Holmgren, U.; Siddiqui, M.K. Prognostic risk factors for moderate-to-severe exacerbations in patients with chronic obstructive pulmonary disease: A systematic literature review. Respir. Res. 2022, 23, 213. [Google Scholar] [CrossRef]
- Virchow, J.C.; Crompton, G.K.; Dal Negro, R.; Pedersen, S.; Magnan, A.; Seidenberg, J.; Barnes, P.J. Importance of inhaler devices in the management of airway disease. Respir. Med. 2008, 102, 1019. [Google Scholar] [CrossRef]
- Yadav, U.N.; Lloyd, J.; Hosseinzadeh, H.; Baral, K.P.; Harris, M.F. Do Chronic Obstructive Pulmonary Diseases (COPD) Self-Management Interventions Consider Health Literacy and Patient Activation? A Systematic Review. J. Clin. Med. 2020, 9, 646. [Google Scholar] [CrossRef]
- Zwerink, M.; Brusse-Keizer, M.; Van Der Valk, P.D.; Zielhuis, G.A.; Monninkhof, E.M.; Van Der Palen, J.; Frith, P.A.; Effing, T. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014, CD002990. [Google Scholar] [CrossRef]
- Kong, C.W.; Wilkinson TM, A. Predicting and preventing hospital readmission for exacerbations of COPD. ERJ Open Res. 2020, 6, 0032502019. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Román-Rodríguez, M.; Singh, D.; Han, M.K.; Rodríguez-Roisin, R.; Ferguson, G.T. Goals of COPD treatment: Focus on symptoms and exacerbations. Respir. Med. 2020, 166, 105938. [Google Scholar] [CrossRef]
- Daher, B.; Bouytse, K.; Zahraoui, R.; Soualhi, M.; Marc, K.; Benamor, J.; Bourkadi, J.E. Effets d’un programme de réhabilitation respiratoire sur la tolérance à l’exercice et la qualité de vie des patients atteints de BPCO expérience marocaine: À propos de 30 cas. Rev. Mal. Respir. Actual. 2020, 12, 278279. [Google Scholar] [CrossRef]
- Gallefoss, F. The effects of patient education in COPD in a 1-year follow-up randomised, controlled trial. Patient Educ. Couns. 2004, 52, 259266. [Google Scholar] [CrossRef] [PubMed]
- Peytremann-Bridevaux, I.; Staeger, P.; Bridevaux, P.-O.; Ghali, W.A.; Burnand, B. Effectiveness of chronic obstructive pulmonary disease-management programs: Systematic review and meta-analysis. Am. J. Med. 2008, 121, 433–443.e4. [Google Scholar] [CrossRef] [PubMed]
- Schrijver, J.; Lenferink, A.; Brusse-Keizer, M.; Zwerink, M.; Van Der Valk, P.D.; Van Der Palen, J.; Effing, T.W. Self-management interventions for people with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2022, CD002990. [Google Scholar] [CrossRef]
- Sedeno, M.F.; Nault, D.; Hamd, D.H.; Bourbeau, J. A self-management education program including an action plan for acute COPD exacerbations. COPD J. Chronic Obstr. Pulm. Dis. 2009, 6, 352358. [Google Scholar] [CrossRef] [PubMed]
- Worth, H.; Dhein, Y. Does patient education modify behaviour in the management of COPD? Patient Educ. Couns. 2004, 52, 267270. [Google Scholar] [CrossRef]
- Vitacca, M.; Bianchi, L.; Guerra, A.; Fracchia, C.; Spanevello, A.; Balbi, B.; Scalvini, S. Tele-assistance in chronic respiratory failure patients: A randomised clinical trial. Eur. Respir. J. 2008, 33, 411418. [Google Scholar] [CrossRef]
- Mariani, M.V.; Pierucci, N.; Forleo, G.B.; Schiavone, M.; Bernardini, A.; Gasperetti, A.; Mitacchione, G.; Mei, M.; Giunta, G.; Piro, A.; et al. The Feasibility, Effectiveness and Acceptance of Virtual Visits as Compared to In-Person Visits among Clinical Electrophysiology Patients during the COVID-19 Pandemic. J. Clin. Med. 2023, 12, 620. [Google Scholar] [CrossRef]
- McDowell, J.E.; McClean, S.; FitzGibbon, F.; Tate, S. A randomised clinical trial of the effectiveness of home-based health care with telemonitoring in patients with COPD. J. Telemed. Telecare 2015, 21, 8087. [Google Scholar] [CrossRef]
- Barbosa, M.T.; Sousa, C.S.; Morais-Almeida, M.; Simões, M.J.; Mendes, P. Telemedicine in COPD: An Overview by Topics. COPD J. Chronic Obstr. Pulm. Dis. 2020, 17, 601–617. [Google Scholar] [CrossRef]
- Rezende, L.C.; Ribeiro, E.G.; Parreiras, L.C.; Guimarães, R.A.; Reis GM, D.; Carajá, A.F.; Franco, T.B.; De Souza Mendes, L.P.; Augusto, V.M.; Silva, K.L. Telehealth and telemedicine in the management of adult patients after hospitalization for COPD exacerbation: A scoping review. J. Bras. Pneumol. 2023, 49, e20220067. [Google Scholar] [CrossRef]
- Zafar, M.A.; Panos, R.J.; Ko, J.; Otten, L.C.; Gentene, A.; Guido, M.; Clark, K.; Lee, C.; Robertson, J.; Alessandrini, E.A. Reliable adherence to a COPD care bundle mitigates system-level failures and reduces COPD readmissions: A system redesign using improvement science. BMJ Qual. Saf. 2017, 26, 908918. [Google Scholar] [CrossRef] [PubMed]
- Henoch, I.; Löfdahl, C.-G.; Ekberg-Jansson, A. Influences of patient education on exacerbations and hospital admissions in patients with COPD—A longitudinal national register study. Eur. Clin. Respir. J. 2018, 5, 1500073. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.; Casan-Clara, P.; Koehler, D.; Tognella, S.; Viejo, J.L.; Dal Negro, R.W.; Díaz-Lobato, S.; Reissig, K.; González-Moro, J.M.; Devouassoux, G.; et al. COMET: A multicom-ponent home-based disease-management programme versus rou-tine care in severe, COPD. Eur. Respir. J. 2018, 51, 1701612. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, J.H.; Mahoney, E.R.; Stockard, J.; Tusler, M. Development and testing of a short form of the patient activation measure. Health Serv. Res. 2005, 40, 19181930. [Google Scholar] [CrossRef]
- Mínguez Clemente, P.; Pascual-Carrasco, M.; Mata Hernández, C.; Malo de Molina, R.; Arvelo, L.A.; Cadavid, B.; López, F.; Sánchez-Madariaga, R.; Sam, A.; Trisan Alonso, A.; et al. Follow-up with Telemedicine in Early Discharge for COPD Exacerbations: Randomized Clinical Trial (TELEMEDCOPD-Trial). COPD J. Chronic Obstr. Pulm. Dis. 2021, 18, 6269. [Google Scholar] [CrossRef]
- Ringbæk, T.; Green, A.; Laursen, L.C.; Frausing, E.; Brøndum, E.; Ulrik, C.S. Effect of tele health care on exacerbations and hospital admissions in patients with chronic obstructive pulmonary disease: A randomized clinical trial. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 18011808. [Google Scholar] [CrossRef]
- Toh, N.; Pawlovich, J.; Grzybowski, S. La télésanté et les relations patient-médecin dans les communautés rurales et éloignées. Can. Fam. Physician Med. Fam. Can. 2016, 62, e715–e717. [Google Scholar]
- Sculley, J.A.; Musick, H.; Krishnan, J.A. Telehealth in chronic obstructive pulmonary disease: Before, during, and after the coronavirus disease 2019 pandemic. Curr. Opin. Pulm. Med. 2022, 28, 9398. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Total (n = 163) | STD Group (n = 106) | TLM Group (n = 57) | p |
|---|---|---|---|---|
| Age, (years ± SD) | 66.5 ± 12.4 | 67.3 ± 12.7 | 65.043 ± 11.8 | 0.27 |
| 0.01 | ||||
| Male | 112 (68.7) | 66 (58.9) | 46 (41.4) | |
| Employment sector | 0.49 | |||
| Healthcare sector | 4 (2.5) | 4 (3.8) | 0 (0.0) | |
| Education sector | 7 (4.3) | 4 (3.8) | 3 (5.3) | |
| An employee of the state | 40 (24.5) | 22 (20.8) | 18 (31.6) | |
| Student | 1 (0.6) | 1 (0.9) | 0 (0.0) | |
| Others | 111 (68.1) | 75 (70.8) | 36 (63.2) | |
| Education level | 0.06 | |||
| Illiterate | 36 (22.1) | 24 (22.6) | 12 (21.1) | |
| Primary school | 56 (34.4) | 30 (28.3) | 26 (45.6) | |
| Secondary school | 44 (27.0) | 28 (26.4) | 16 (28.1) | |
| University | 27 (16.6) | 24 (22.6) | 3 (5.3) | |
| Geographical origin | 0.86 | |||
| Rural area | 59 (36.2) | 39(36.8) | 20 (35.1) | |
| Urban area | 104 (63.8) | 67(63.2) | 37 (64.9) | |
| Distance from home to hospital(km) | 0.06 | |||
| ≤10 | 107 (65.6) | 64 (60.4) | 43 (75.4) | |
| >10 | 56 (34.4) | 42 (9.6) | 14 (24.6) | |
| PA Past medical history | ||||
| Diabetes | 82 (50.3) | 51 (48.1) | 31 (54.4) | 0.445 |
| Hypertension | 103 (63.2) | 67 (63.2) | 36 (63.2) | 0.995 |
| Dyslipidemia | 48 (29.4) | 27 (25.5) | 21 (36.8) | 0.129 |
| AF | 27 (16.6) | 17 (16.0) | 10 (17.5) | 0.805 |
| Heart failure | 38 (23.3) | 31 (29.2) | 7 (12.3) | 0.015 |
| Lung cancer | 1 (0.6) | 0 (0.0) | 1 (1.8) | 0.350 |
| Chronic respiratory failure | 23 (14.1) | 22 (20.8) | 1 (1.8) | 0.001 |
| mMRC | 0.059 | |||
| 1 | 53 (32.5) | 42 (39.6) | 11 (19.3) | |
| 2 | 49 (30.1) | 29 (27.4) | 20 (35.1) | |
| 3 | 57 (35.0) | 32 (30.2) | 25 (43.9) | |
| 4 | 4 (2.5) | 3 (2.8) | 1 (1.8) |
| Secondary Outcomes, n (%) | STD Group (n = 106) | TLM Group (n = 57) | OR (95% CI) | p |
|---|---|---|---|---|
| Hospitalizations for AECOPD | 47 (44.3) | 9 (15.8) | 0.23 (0.10–0.52) | <0.001 |
| All-cause death | 6 (5.7) | 1 (1.8) | 0.29 (0.03–2.53) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaddoussi, R.; Bel Haj Ali, K.; Hajji, E.; Ben Soltane, H.; Chamtouri, I.; Dhaoui, R.; Younes, S.; Fahem, N.; Khalifa, M.; Dhouib, W.; et al. Impact of Home Mobile Phone-Based Telemonitoring in Preventing Exacerbations and Hospitalizations Among Patients with Chronic Obstructive Pulmonary Disease: An IMTEC Study. J. Clin. Med. 2024, 13, 6319. https://doi.org/10.3390/jcm13216319
Kaddoussi R, Bel Haj Ali K, Hajji E, Ben Soltane H, Chamtouri I, Dhaoui R, Younes S, Fahem N, Khalifa M, Dhouib W, et al. Impact of Home Mobile Phone-Based Telemonitoring in Preventing Exacerbations and Hospitalizations Among Patients with Chronic Obstructive Pulmonary Disease: An IMTEC Study. Journal of Clinical Medicine. 2024; 13(21):6319. https://doi.org/10.3390/jcm13216319
Chicago/Turabian StyleKaddoussi, Rania, Khaoula Bel Haj Ali, Ekram Hajji, Houda Ben Soltane, Ikram Chamtouri, Randa Dhaoui, Salma Younes, Nesrine Fahem, Meriem Khalifa, Wafa Dhouib, and et al. 2024. "Impact of Home Mobile Phone-Based Telemonitoring in Preventing Exacerbations and Hospitalizations Among Patients with Chronic Obstructive Pulmonary Disease: An IMTEC Study" Journal of Clinical Medicine 13, no. 21: 6319. https://doi.org/10.3390/jcm13216319
APA StyleKaddoussi, R., Bel Haj Ali, K., Hajji, E., Ben Soltane, H., Chamtouri, I., Dhaoui, R., Younes, S., Fahem, N., Khalifa, M., Dhouib, W., Msolly, M. A., Sekma, A., Boubaker, H., Bouida, W., & Nouira, S. (2024). Impact of Home Mobile Phone-Based Telemonitoring in Preventing Exacerbations and Hospitalizations Among Patients with Chronic Obstructive Pulmonary Disease: An IMTEC Study. Journal of Clinical Medicine, 13(21), 6319. https://doi.org/10.3390/jcm13216319