
Applying AI to Safely and Effectively Scale Care to Address Chronic MSK Conditions

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
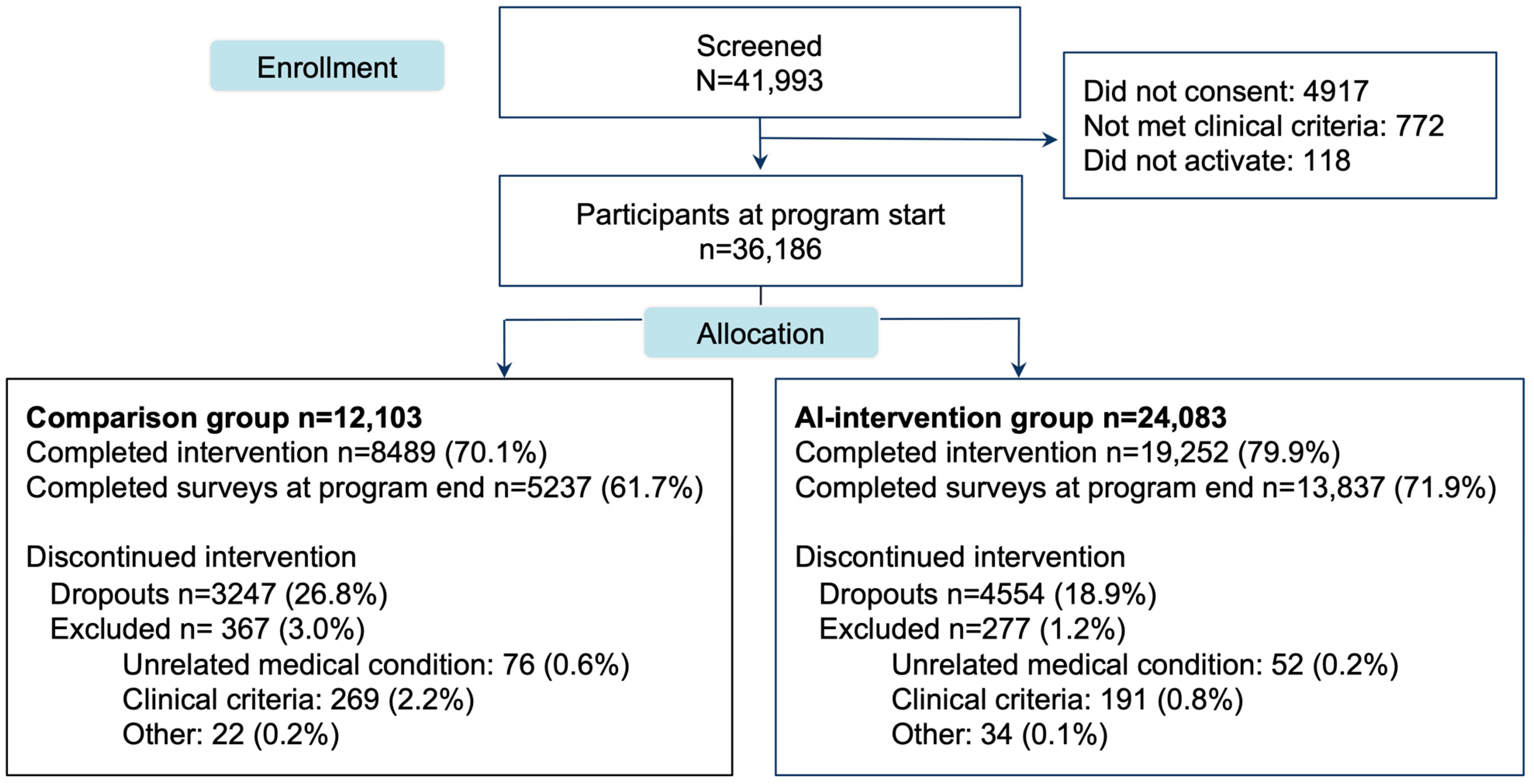
2.2. Population
2.3. Intervention
2.3.1. Digital Care Program
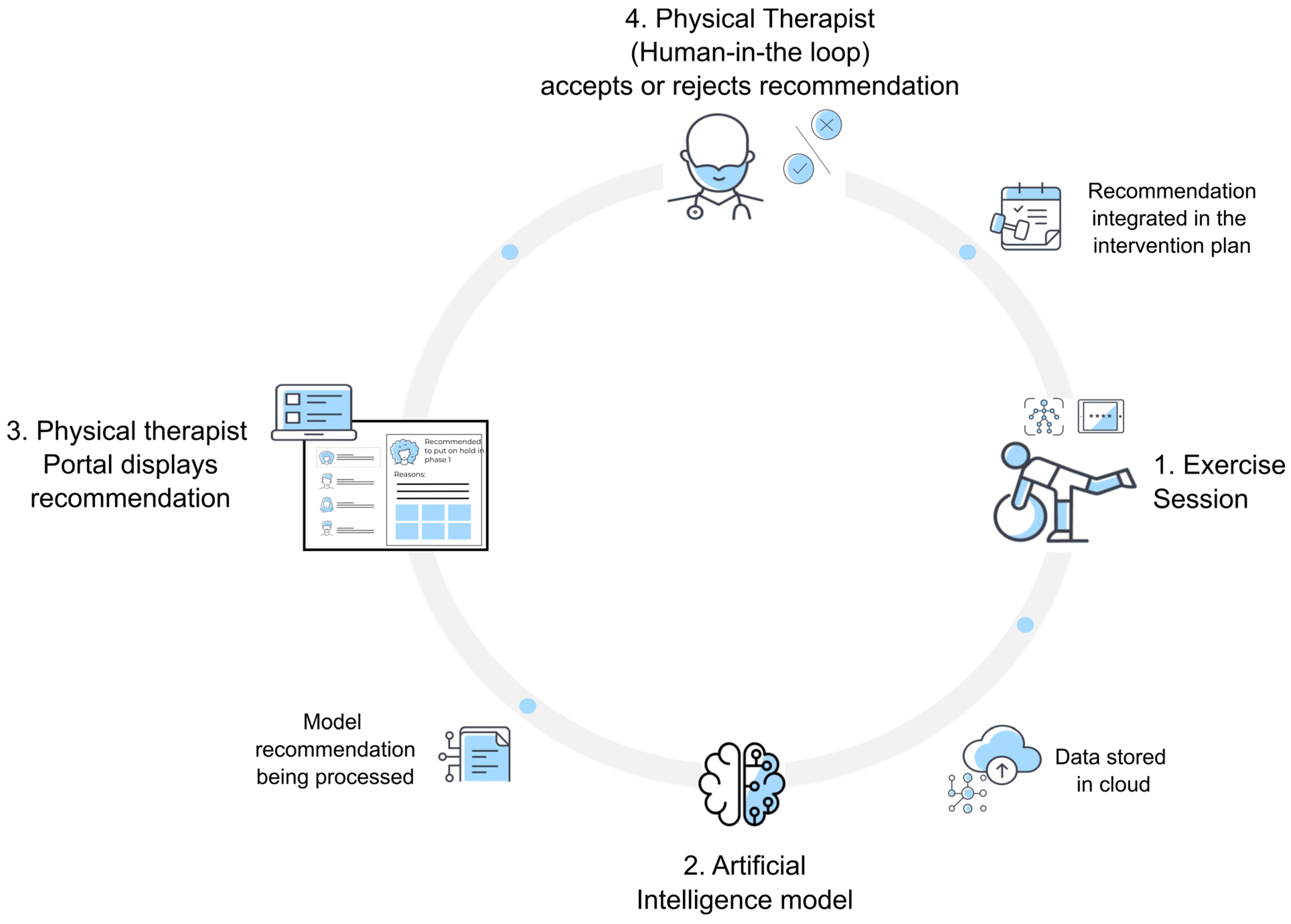
2.3.2. Workflow-Related AI Tool
2.3.3. Comparison Group (CG)
2.3.4. Intervention Group: PT Portal Powered by AI Tool
2.4. Outcomes
2.5. Safety and Adverse Events
2.6. Sample Size
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Outcomes
3.2.1. Clinical Outcomes
3.2.2. Engagement and Satisfaction
3.2.3. Adverse Events
4. Discussion
4.1. Main Findings
4.2. Comparison with Previous Studies
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef]
- Dieleman, J.L.; Cao, J.; Chapin, A.; Chen, C.; Li, Z.; Liu, A.; Horst, C.; Kaldjian, A.; Matyasz, T.; Scott, K.W.; et al. US Health Care Spending by Payer and Health Condition, 1996–2016. JAMA 2020, 323, 863–884. [Google Scholar] [CrossRef]
- Koonin, L.M.; Hoots, B.; Tsang, C.A.; Leroy, Z.; Farris, K.; Jolly, T.; Antall, P.; McCabe, B.; Zelis, C.B.R.; Tong, I.; et al. Trends in the Use of Telehealth during the Emergence of the COVID-19 Pandemic—United States, January–March 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1595–1599. [Google Scholar] [CrossRef] [PubMed]
- Mitchaï, P.M.; Mapinduzi, J.; Verbrugghe, J.; Michiels, S.; Janssens, L.; Kossi, O.; Bonnechère, B.; Timmermans, A. Mobile technologies for rehabilitation in non-specific spinal disorders: A systematic review of the efficacy and potential for implementation in low- and middle-income countries. Eur. Spine J. 2023, 32, 4077–4100. [Google Scholar] [CrossRef] [PubMed]
- Argent, R.; Daly, A.; Caulfield, B. Patient Involvement With Home-Based Exercise Programs: Can Connected Health Interventions Influence Adherence? JMIR Mhealth Uhealth 2018, 6, e47. [Google Scholar] [CrossRef] [PubMed]
- Fiani, B.; Siddiqi, I.; Lee, S.C.; Dhillon, L. Telerehabilitation: Development, Application, and Need for Increased Usage in the COVID-19 Era for Patients with Spinal Pathology. Cureus 2020, 12, e10563. [Google Scholar] [CrossRef] [PubMed]
- Landry, M.D.; Hack, L.M.; Coulson, E.; Freburger, J.; Johnson, M.P.; Katz, R.; Kerwin, J.; Smith, M.H.; Wessman, H.C.; Venskus, D.G.; et al. Workforce Projections 2010–2020: Annual Supply and Demand Forecasting Models for Physical Therapists Across the United States. Phys. Ther. 2016, 96, 71–80. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Family Physicians Innovation Labs. Using and AI Assistant to Reduce Documentation Burden in Family Medicine; AAFP Innovation Labs: Leawood, KS, USA, 2021; Available online: https://resources.suki.ai/i/1437132-using-an-ai-assistant-to-reduce-documentation-burden-in-family-medicine/3? (accessed on 15 April 2024).
- Lanotte, F.; O’Brien, M.K.; Jayaraman, A. AI in Rehabilitation Medicine: Opportunities and Challenges. Ann. Rehabil. Med. 2023, 47, 444–458. [Google Scholar] [CrossRef] [PubMed]
- McGrath, S.P.; Perreard, I.M.; Garland, M.D.; Converse, K.A.; Mackenzie, T.A. Improving Patient Safety and Clinician Workflow in the General Care Setting with Enhanced Surveillance Monitoring. IEEE J. Biomed. Health Inform. 2019, 23, 857–866. [Google Scholar] [CrossRef]
- Annika, G.; Christoff, Z.; Kerstin, L. Evaluation of the accuracy of an artificial intelligence in identifying contraindications to exercise therapy—Comparison with and interrater reliability of physical therapists judgments. Health Technol. 2024, 14, 513–522. [Google Scholar] [CrossRef]
- Tagliaferri, S.D.; Wilkin, T.; Angelova, M.; Fitzgibbon, B.M.; Owen, P.J.; Miller, C.T.; Belavy, D.L. Chronic back pain sub-grouped via psychosocial, brain and physical factors using machine learning. Sci. Rep. 2022, 12, 15194. [Google Scholar] [CrossRef]
- Tschuggnall, M.; Grote, V.; Pirchl, M.; Holzner, B.; Rumpold, G.; Fischer, M.J. Machine learning approaches to predict rehabilitation success based on clinical and patient-reported outcome measures. Inform. Med. Unlocked 2021, 24, 100598. [Google Scholar] [CrossRef]
- Zmudzki, F.; Smeets, R. Machine learning clinical decision support for interdisciplinary multimodal chronic musculoskeletal pain treatment. Front. Pain Res. 2023, 4, 1177070. [Google Scholar] [CrossRef]
- Areias, A.C.; Molinos, M.; Moulder, R.G.; Janela, D.; Scheer, J.K.; Bento, V.; Yanamadala, V.; Cohen, S.P.; Correia, F.D.; Costa, F. The potential of a multimodal digital care program in addressing healthcare inequities in musculoskeletal pain management. NPJ Digit. Med. 2023, 6, 188. [Google Scholar] [CrossRef] [PubMed]
- Cui, D.; Janela, D.; Costa, F.; Molinos, M.; Areias, A.C.; Moulder, R.G.; Scheer, J.K.; Bento, V.; Cohen, S.P.; Yanamadala, V.; et al. Randomized-controlled trial assessing a digital care program versus conventional physiotherapy for chronic low back pain. NPJ Digit. Med. 2023, 6, 121. [Google Scholar] [CrossRef]
- Costa, F.; Janela, D.; Molinos, M.; Moulder, R.G.; Lains, J.; Francisco, G.E.; Bento, V.; Yanamadala, V.; Cohen, S.P.; Correia, F.D. Digital rehabilitation for hand and wrist pain: A single-arm prospective longitudinal cohort study. Pain Rep. 2022, 7, e1026. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Ethics and Governance of Artificial Intelligence for Health. Guidance on Large Multi-Modal Models; WHO: Geneva, Switzerland, 2024; Available online: https://www.who.int/publications/i/item/9789240029200 (accessed on 26 March 2024).
- Chorzewski, R. AAOE Physical Therapy Survey: White Paper with Summary Results; American Association of Orthopedic Executives (AAOE): Indianapolis, IN, USA, 2016; Available online: https://www.multibriefs.com/briefs/aaoe/whitepaper011216.pdf (accessed on 15 July 2024).
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain 2008, 9, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Bijker, L.; Sleijser-Koehorst, M.L.S.; Coppieters, M.W.; Cuijpers, P.; Scholten-Peeters, G.G.M. Preferred Self-Administered Questionnaires to Assess Depression, Anxiety and Somatization in People With Musculoskeletal Pain—A Modified Delphi Study. J. Pain 2020, 21, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Smith, S.M.; Dworkin, R.H.; Turk, D.C.; McDermott, M.P.; Eccleston, C.; Farrar, J.T.; Rowbotham, M.C.; Bhagwagar, Z.; Burke, L.B.; Cowan, P.; et al. Interpretation of chronic pain clinical trial outcomes: IMMPACT recommended considerations. Pain 2020, 161, 2446–2461. [Google Scholar] [CrossRef] [PubMed]
- Scheer, J.; Costa, F.; Molinos, M.; Areias, A.; Janela, D.; Moulder, R.G.; Lains, J.; Bento, V.; Yanamadala, V.; Cohen, S.P.; et al. Racial and Ethnic Differences in Outcomes of a 12-Week Digital Rehabilitation Program for Musculoskeletal Pain: Prospective Longitudinal Cohort Study. J. Med. Internet Res. 2022, 24, e41306. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- McNeish, D.; Matta, T. Differentiating between mixed-effects and latent-curve approaches to growth modeling. Behav. Res. Methods 2018, 50, 1398–1414. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Bulut, O. Evaluating the Performances of Missing Data Handling Methods in Ability Estimation From Sparse Data. Educ. Psychol. Meas. 2020, 80, 932–954. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef]
- Åhlin, P.; Almström, P.; Wänström, C. Solutions for improved hospital-wide patient flows—A qualitative interview study of leading healthcare providers. BMC Health Serv. Res. 2023, 23, 17. [Google Scholar] [CrossRef] [PubMed]
- Mohsen, F.; Ali, H.; El Hajj, N.; Shah, Z. Artificial intelligence-based methods for fusion of electronic health records and imaging data. Sci. Rep. 2022, 12, 17981. [Google Scholar] [CrossRef]
- Huang, J.; Neill, L.; Wittbrodt, M.; Melnick, D.; Klug, M.; Thompson, M.; Bailitz, J.; Loftus, T.; Malik, S.; Phull, A.; et al. Generative Artificial Intelligence for Chest Radiograph Interpretation in the Emergency Department. JAMA Netw. Open 2023, 6, e2336100. [Google Scholar] [CrossRef]
- Oren, O.; Gersh, B.J.; Bhatt, D.L. Artificial intelligence in medical imaging: Switching from radiographic pathological data to clinically meaningful endpoints. Lancet Digit. Health 2020, 2, e486–e488. [Google Scholar] [CrossRef]
- Hyland, S.L.; Faltys, M.; Hüser, M.; Lyu, X.; Gumbsch, T.; Esteban, C.; Bock, C.; Horn, M.; Moor, M.; Rieck, B.; et al. Early prediction of circulatory failure in the intensive care unit using machine learning. Nat. Med. 2020, 26, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Niederer, D.; Schiller, J.; Groneberg, D.A.; Behringer, M.; Wolfarth, B.; Gabrys, L. Machine learning-based identification of determinants for rehabilitation success and future healthcare use prevention in patients with high-grade, chronic, nonspecific low back pain: An individual data 7-year follow-up analysis on 154,167 individuals. Pain 2023, 165, 772–784. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Ethics and Governance of Artifical Intelligence for Health: WHO Guidance; WHO: Geneva, Switzerland, 2021; Available online: https://iris.who.int/bitstream/handle/10665/341996/9789240029200-eng.pdf?sequence=1 (accessed on 27 June 2024).
- U.S. Food & Drug Administration; HealthCanada and Medicines and Healthcare products Regulatory Agency (MHRA). Good Machine Learning Practice for Medical Device Development: Guiding Principles. Available online: https://www.fda.gov/medical-devices/software-medical-device-samd/good-machine-learning-practice-medical-device-development-guiding-principles (accessed on 27 June 2024).
- Chen, R.J.; Wang, J.J.; Williamson, D.F.K.; Chen, T.Y.; Lipkova, J.; Lu, M.Y.; Sahai, S.; Mahmood, F. Algorithmic fairness in artificial intelligence for medicine and healthcare. Nat. Biomed. Eng. 2023, 7, 719–742. [Google Scholar] [CrossRef] [PubMed]
- Cutillo, C.M.; Sharma, K.R.; Foschini, L.; Kundu, S.; Mackintosh, M.; Mandl, K.D.; Beck, T.; Collier, E.; Colvis, C.; Gersing, K.; et al. Machine intelligence in healthcare—Perspectives on trustworthiness, explainability, usability, and transparency. NPJ Digit. Med. 2020, 3, 47. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.G.; Devan, H.; Fioratti, I.; Kamper, S.J.; Williams, C.M.; Saragiotto, B.T. At my own pace, space, and place: A systematic review of qualitative studies of enablers and barriers to telehealth interventions for people with chronic pain. Pain 2022, 163, e165–e181. [Google Scholar] [CrossRef]
- Fernandes, L.G.; Oliveira, R.F.F.; Barros, P.M.; Fagundes, F.R.C.; Soares, R.J.; Saragiotto, B.T. Physical therapists and public perceptions of telerehabilitation: An online open survey on acceptability, preferences, and needs. Braz. J. Phys. Ther. 2022, 26, 100464. [Google Scholar] [CrossRef] [PubMed]
- Crofford, L.J. Psychological aspects of chronic musculoskeletal pain. Best. Pract. Res. Clin. Rheumatol. 2015, 29, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Taccolini Manzoni, A.C.; Bastos de Oliveira, N.T.; Nunes Cabral, C.M.; Aquaroni Ricci, N. The role of the therapeutic alliance on pain relief in musculoskeletal rehabilitation: A systematic review. Physiother. Theory Pract. 2018, 34, 901–915. [Google Scholar] [CrossRef]
- Elliott, T.; Tong, I.; Sheridan, A.; Lown, B.A. Beyond Convenience: Patients’ Perceptions of Physician Interactional Skills and Compassion via Telemedicine. Mayo Clin. Proc. Innov. Qual. Outcomes 2020, 4, 305–314. [Google Scholar] [CrossRef]
- Licciardone, J.C.; Tran, Y.; Ngo, K.; Toledo, D.; Peddireddy, N.; Aryal, S. Physician Empathy and Chronic Pain Outcomes. JAMA Netw. Open 2024, 7, e246026. [Google Scholar] [CrossRef]
- Zayas-Cabán, T.; Okubo, T.H.; Posnack, S. Priorities to accelerate workflow automation in health care. J. Am. Med. Inform. Assoc. 2022, 30, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Bagg, M.K.; Wand, B.M.; Cashin, A.G.; Lee, H.; Hübscher, M.; Stanton, T.R.; O’Connell, N.E.; O’Hagan, E.T.; Rizzo, R.R.N.; Wewege, M.A.; et al. Effect of Graded Sensorimotor Retraining on Pain Intensity in Patients with Chronic Low Back Pain: A Randomized Clinical Trial. JAMA 2022, 328, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Ingwersen, K.G.; Jensen, S.L.; Sørensen, L.; Jørgensen, H.R.; Christensen, R.; Søgaard, K.; Juul-Kristensen, B. Three Months of Progressive High-Load Versus Traditional Low-Load Strength Training Among Patients With Rotator Cuff Tendinopathy: Primary Results From the Double-Blind Randomized Controlled RoCTEx Trial. Orthop. J. Sports Med. 2017, 5, 2325967117723292. [Google Scholar] [CrossRef] [PubMed]
- Jain, D.; Norman, K.; Werner, Z.; Makovoz, B.; Baker, T.; Huber, S. Using Postmarket Surveillance to Assess Safety-Related Events in a Digital Rehabilitation App (Kaia App): Observational Study. JMIR Hum. Factors 2021, 8, e25453. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Yoo, I.; Lancey, R.; Varghese, E. Mobile applications for pain management: An app analysis for clinical usage. BMC Med. Inform. Decis. Mak. 2019, 19, 106. [Google Scholar] [CrossRef] [PubMed]
- Alsobhi, M.; Khan, F.; Chevidikunnan, M.F.; Basuodan, R.; Shawli, L.; Neamatallah, Z. Physical Therapists’ Knowledge and Attitudes Regarding Artificial Intelligence Applications in Health Care and Rehabilitation: Cross-sectional Study. J. Med. Internet Res. 2022, 24, e39565. [Google Scholar] [CrossRef]
- Khullar, D.; Casalino, L.P.; Qian, Y.; Lu, Y.; Krumholz, H.M.; Aneja, S. Perspectives of Patients About Artificial Intelligence in Health Care. JAMA Netw. Open 2022, 5, e2210309. [Google Scholar] [CrossRef]
- Alowais, S.A.; Alghamdi, S.S.; Alsuhebany, N.; Alqahtani, T.; Alshaya, A.I.; Almohareb, S.N.; Aldairem, A.; Alrashed, M.; Bin Saleh, K.; Badreldin, H.A.; et al. Revolutionizing healthcare: The role of artificial intelligence in clinical practice. BMC Med. Educ. 2023, 23, 689. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| IG (N = 24,083) | CG (N = 12,103) | p-Value | |
|---|---|---|---|
| Age (years), mean (SD) | 48.5 (11.6) | 50.0 (11.7) | <0.001 |
| Age categories (years), N (%): | |||
| <25 | 342 (1.4) | 72 (0.6) | <0.001 |
| 25–40 | 6099 (25.3) | 2795 (23.1) | |
| 41–60 | 13,615 (56.5) | 6623 (54.7) | |
| >60 | 4027 (16.7) | 2613 (21.6) | |
| Gender, N (%) a: | |||
| Woman | 14,126 (58.7) | 6984 (57.9) | 0.414 |
| Man | 9849 (41.0) | 5044 (41.8) | |
| Non-binary | 67 (0.3) | 35 (0.3) | |
| Other | 4 (0.0) | 1 (0.0) | |
| BMI (kg/m2), mean (SD) b | 29.7 (7.0) | 29.3 (6.7) | <0.001 |
| BMI categories (kg/m2), N (%) b: | |||
| Underweight (<18.5) | 199 (0.8) | 102 (0.8) | 0.001 |
| Normal (18.5–25) | 6223 (25.9) | 3349 (27.7) | |
| Overweight (≥25–30) | 8100 (33.7) | 4051 (33.5) | |
| Obese (≥30) | 9528 (39.6) | 4584 (37.9) | |
| Race/ethnicity, N (%) c: | |||
| Asian | 2311 (9.8) | 928 (10.2) | 0.017 |
| Black | 2297 (9.8) | 982 (10.8) | |
| Hispanic | 2268 (9.6) | 890 (9.8) | |
| Non-Hispanic White | 15,991(67.9) | 6013 (66.3) | |
| Other | 690 (2.9) | 250 (2.8) | |
| Education level, N (%) d: | |||
| Less than high school diploma | 219 (0.9) | 74 (0.7) | 0.001 |
| High school diploma | 2172 (9.1) | 823 (8.1) | |
| Some college | 6133 (25.8) | 2528 (25.0) | |
| Bachelor’s degree | 9397 (39.5) | 4162 (41.2) | |
| Graduate degree | 5846 (24.6) | 2523 (25.0) | |
| Geographic location, N (%) e: | |||
| Urban | 21,321 (88.8) | 10,767 (89.4) | 0.077 |
| Rural | 2693 (11.2) | 1276 (10.6) | |
| Employment status, N (%) f: | |||
| Full-time job | 20,807 (87.5) | 8987 (75.7) | <0.001 |
| Part-time job | 997 (4.2) | 1908 (16.1) | |
| Retired | 991 (4.2) | 608 (5.1) | |
| Not employed | 990 (4.2) | 376 (3.2) | |
| Clinical data, mean (SD) | |||
| Analgesic intake, N (%) | 5580 (23.2) | 2850 (23.6) | 0.423 |
| Symptomatic anatomical area: | |||
| Ankle | 1395 (5.8) | 482 (4.0) | <0.001 |
| Elbow | 523 (2.2) | 262 (2.2) | |
| Hip | 2592 (10.8) | 1267 (10.5) | |
| Knee | 3633 (15.1) | 1832 (15.1) | |
| Low back | 8589 (35.7) | 4590 (37.9) | |
| Neck | 2601 (10.8) | 1304 (10.8) | |
| Shoulder | 3730 (15.5) | 1928 (15.9) | |
| Wrist | 1020 (4.2) | 438 (3.6) | |
| Pain intensity c, mean (SD) | 4.73 (1.9) | 4.84 (1.9) | <0.001 |
| Mental health ≥ 5, mean (SD): | |||
| GAD-7 g | 8.72 (3.94) | 8.81 (4.06) | 0.083 |
| PHQ-5 h | 9.52 (4.20) | 9.23 (4.27) | 0.688 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Areias, A.C.; Janela, D.; Moulder, R.G.; Molinos, M.; Bento, V.; Moreira, C.; Yanamadala, V.; Correia, F.D.; Costa, F. Applying AI to Safely and Effectively Scale Care to Address Chronic MSK Conditions. J. Clin. Med. 2024, 13, 4366. https://doi.org/10.3390/jcm13154366
Areias AC, Janela D, Moulder RG, Molinos M, Bento V, Moreira C, Yanamadala V, Correia FD, Costa F. Applying AI to Safely and Effectively Scale Care to Address Chronic MSK Conditions. Journal of Clinical Medicine. 2024; 13(15):4366. https://doi.org/10.3390/jcm13154366
Chicago/Turabian StyleAreias, Anabela C., Dora Janela, Robert G. Moulder, Maria Molinos, Virgílio Bento, Carolina Moreira, Vijay Yanamadala, Fernando Dias Correia, and Fabíola Costa. 2024. "Applying AI to Safely and Effectively Scale Care to Address Chronic MSK Conditions" Journal of Clinical Medicine 13, no. 15: 4366. https://doi.org/10.3390/jcm13154366
APA StyleAreias, A. C., Janela, D., Moulder, R. G., Molinos, M., Bento, V., Moreira, C., Yanamadala, V., Correia, F. D., & Costa, F. (2024). Applying AI to Safely and Effectively Scale Care to Address Chronic MSK Conditions. Journal of Clinical Medicine, 13(15), 4366. https://doi.org/10.3390/jcm13154366