Abstract
Background/Objectives: Short-stem prostheses were introduced as an alternative to conventional straight-stem prostheses. Despite their benefits, including minimally invasive approaches, soft-tissue- and bone-sparing implantation, and physiological load transfer to the metaphysis, data on postoperative complication and revision rates as well as on implant survival are scarce. Methods: A retrospective analysis of 1327 patients who underwent primary total hip arthroplasty (THA) using the Metha® short stem between 2006 and 2023 was conducted. Complication and revision rates were analysed for the intraoperative, direct postoperative, and follow-up episodes. Implant survival was analysed with the endpoint of all-cause stem revision. Results: Intraoperative complications were observed in 3.77% of the cases and included 44 hairline cracks and 6 fractures. In 15 cases (30.0%), conversion to a straight-stem or revision implant was necessary. The direct postoperative complication rate was 2.44%, and 11 revision procedures were performed during inpatient stay (0.84%). Mean follow-up was 7 years (range 1–17). During follow-up, femoral component revision was performed in 60 cases. Aseptic loosening and stem subsidence accounted for a combined percentage of 80% of all indications. Implant survival rate was 95.66% after 5 years, 95.58% after 10 years, and 95.50% after 15 years. Conclusions: Our study provides a comprehensive analysis of postoperative complication and revision rates in a large sample undergoing primary short-stem THA. Postoperative complication rates were favourable, and the long-term implant survival rates were comparable to conventional straight-stem prostheses. Therefore, short-stem THA may be considered an alternative for younger patients.
1. Introduction
Total hip arthroplasty (THA) is the standard treatment for end-stage osteoarthritis (OA) of the hip. It is considered the “operation of the century”, as it is one of the most successful orthopaedic procedures, leading to substantial improvements in patients’ quality of life [1]. Given the high success rates of modern THA procedures, the volume of primary THA has risen exponentially in the past years [2,3]. Recent models predict a 5% annual growth in THA procedures and forecast an increase in primary THA procedures of 600% by 2060 [3]. In addition, arthroplasty registries indicate an increasing proportion of young, high-demanding, and physically active patients undergoing THA [4,5,6]. Kurtz et al. predicted that by the year 2030, 52% of all primary THAs would be performed in patients younger than 65 years of age, with the greatest increase in patients aged 45–55 years [4]. Given the average implant survival rate of 89% after 15 years and 58% after 25 years, these patients are at a higher risk for consecutive revision procedures [7]. In accordance with this, Bayliss et al. report a significant 29% increase in the lifetime risk of revision (LTRR) for patients aged 50–54 years versus a LTRR of 5% in patients aged 70 years [8].
Despite the favourable long-term outcomes of conventional cementless straight-stem prostheses, there are relevant limitations of these stem designs, including an unphysiological distal load transfer, stress shielding with consecutive periprosthetic bone loss in the proximal femur, and thigh pain due to the diaphyseal anchorage [9,10,11].
Short-stem implants were introduced as a soft-tissue- and bone-preserving alternative to conventional straight-stem THA and have been gaining popularity ever since. They allow for minimally invasive surgical approaches and physiological loading by distributing stress forces solely to the femoral metaphysis, thereby reducing periprosthetic bone remodelling [12,13]. However, data on the postoperative complication rates, long-term outcomes, and survival rates of short stems are scarce.
The purpose of this study was to examine the intra- and postoperative complications and revision rates associated with short-stem THA and to analyse mid- and long-term implant survival rates of the Metha short-stem prosthesis.
2. Materials and Methods
This is a retrospective, single-centre study investigating the intra- and postoperative complication and revision rates using the Metha® short-stem prosthesis (BBraun, Aesculap, Tuttlingen, Germany). Following ethical approval, the institutional database at our tertiary referral centre was screened to identify patients who had undergone THA using the Metha short-stem prosthesis between November 2006 and November 2023. In general, indications for short-stem arthroplasty included younger patient age (<70 years), good femoral bone stock, absence of severe deformities, and a proximal femoral morphology that allows for primary stability of a metaphyseal-anchoring implant. Exclusion criteria were defined as age < 18 years, incomplete digital medical records, and use of the Metha short stem in revision THA (rTHA). In accordance with the aforementioned inclusion and exclusion criteria, 1327 cases were deemed eligible for analysis.
2.1. Implant Characteristics
The Metha short stem is a calcar-loading, partial neck-preserving implant [14]. Metaphyseal anchorage is achieved by the proximal, trapezoidal implant design, which allows for a cortical multipoint contact and a three-point fixation in the medial calcar region, proximal lateral cortex, and proximal posterior cortex [15,16].
The Metha short-stem prosthesis was initially introduced in 2004 as a modular stem with titanium alloy neck adapters (CCD angle specifications: 130°, 135°, 140°; version options: neutral, 7.5° anteversion, 7.5° retroversion). In 2007, the adapter was replaced by a cobalt–chromium alloy modular neck adapter after a series of adapter failures of the titanium alloy adapter had been reported [17,18,19]. In 2008, the monoblock version was introduced (CCD angle specifications: 120°, 130°, 135°). Both stem designs are available in eight sizes (sizes 0–7).
2.2. Surgical Procedure
Preoperative templating was conducted to assess proximal femoral and acetabular anatomy, plan the osteotomy location, and predict component size and implant position [20]. All patients received prophylactic single-shot antibiotics perioperatively. Surgeries were performed using an anterolateral, lateral, or direct anterior approach with the patient in a supine position. For cup placement, an image-free navigation system was used (OrthoPilot®, BBraun Aesculap, Tuttlingen, Germany). Following an intraoperative assessment of the bone quality of the proximal femur, stem preparation and implantation were conducted according to the manufacturer’s instructions. For femoral neck osteotomy, a neck-preserving resection is mandatory to ensure a sufficient proximal anchoring of the prosthesis and specific care is taken to ensure an intact cortical ring of the femoral neck, which is crucial for primary stability. During femoral preparation, specific care is taken to achieve rotational stability within the cortical ring and a sufficient contact with the dorsolateral cortex. Radiographs were taken intraoperatively to confirm the correct implant position.
2.3. Clinical Data
Demographic, clinical, and intraoperative data were retrieved from the digital medical records. Postoperative complications and revision surgeries were documented during clinical follow-up and were analysed at last follow-up. Arthroplasty-related postoperative complications were defined according to Healy et al. and classified as intraoperative, direct postoperative complications during inpatient stay, and late postoperative complications that occurred during the follow-up period after discharge [21]. The primary endpoint was defined as femoral component revision for any reason.
2.4. Statistical Analysis
Descriptive statistics were calculated including counts and frequencies for categorical data. For continuous data, means and standard deviations (SDs) or medians and interquartile ranges (IQRs) are provided. Group differences were calculated using Student’s t-test or the Mann–Whitney U-test. The Kruskal–Wallis test was used for multiple-group comparisons. Bonferroni adjustment was applied for multiple testing. A non-parametric survival analysis was conducted using Kaplan–Meier calculations (observed cumulative survival). Implant survival was defined as the time between primary THA to first revision (event). Patients who did not undergo rTHA were censored at the end of the study period (i.e., 30 November 2023) or at the time of in-hospital death. Subgroups were compared using the log rank test to assess the impact of stem design on implant survival. A p-value < 0.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS Statistics 29 (SPSS Inc., Armonk, NY, USA).
3. Results
Of 1327 patients being included into this study, 725 were female (54.63%). Mean age at the time of surgery was 55 years. Primary OA accounted for 56% of the cases. Baseline characteristics are provided in Table 1.

Table 1.
Baseline characteristics.
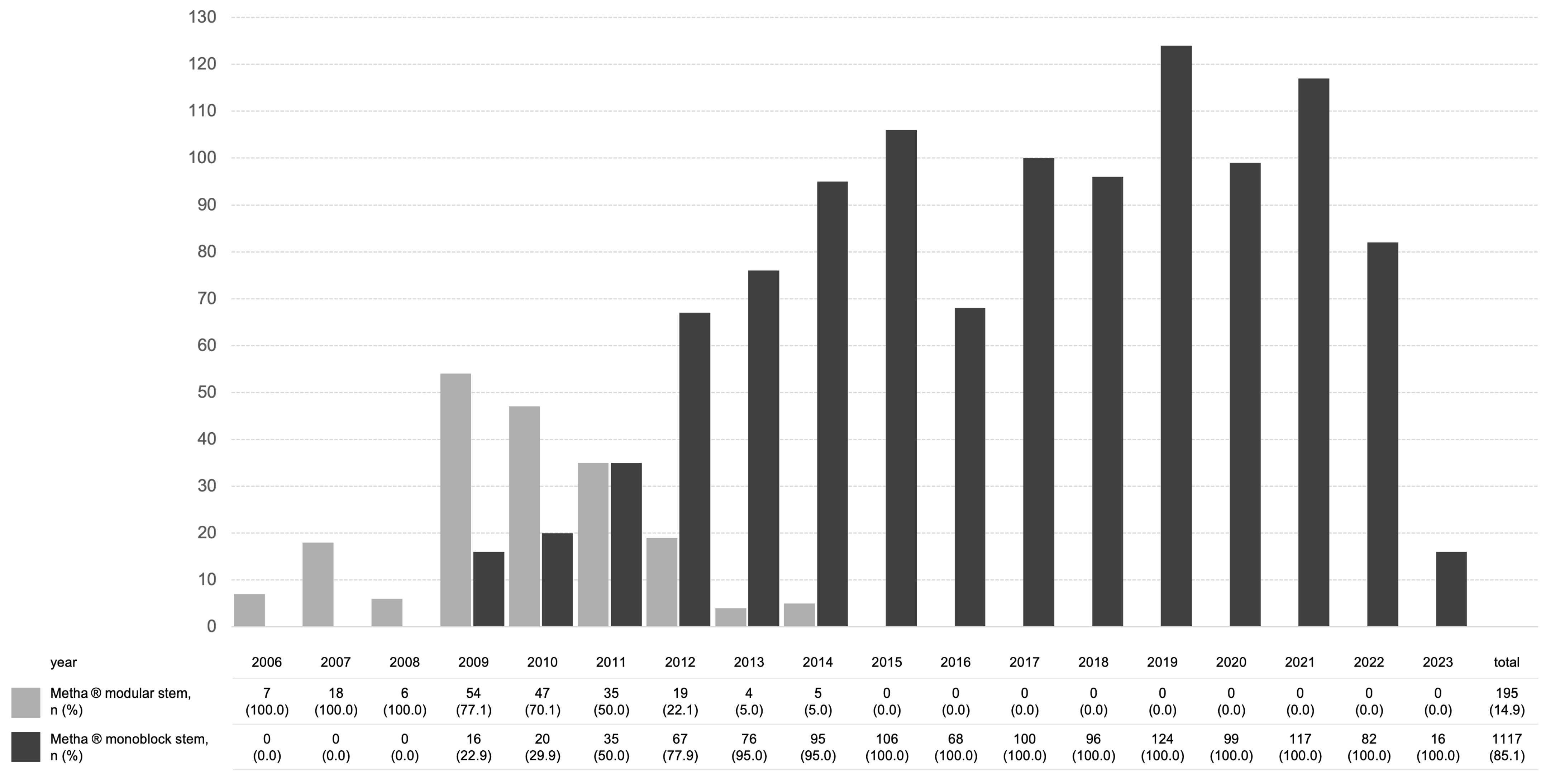
The monoblock stem was used in 84% of cases (Table 2). The modular stem was available from 2006 and was used until 2014; however, the proportion of monoblock stems increased steadily since their introduction in 2008 (Figure 1). An optical navigation system was used for cup placement in 98% of cases.
Table 2.
Intraoperative data.
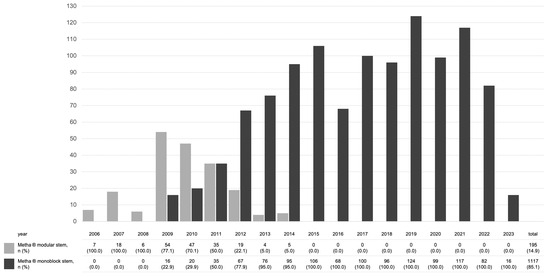
Figure 1.
Overview of implanted stem designs over the years.
3.1. Inpatient Stay
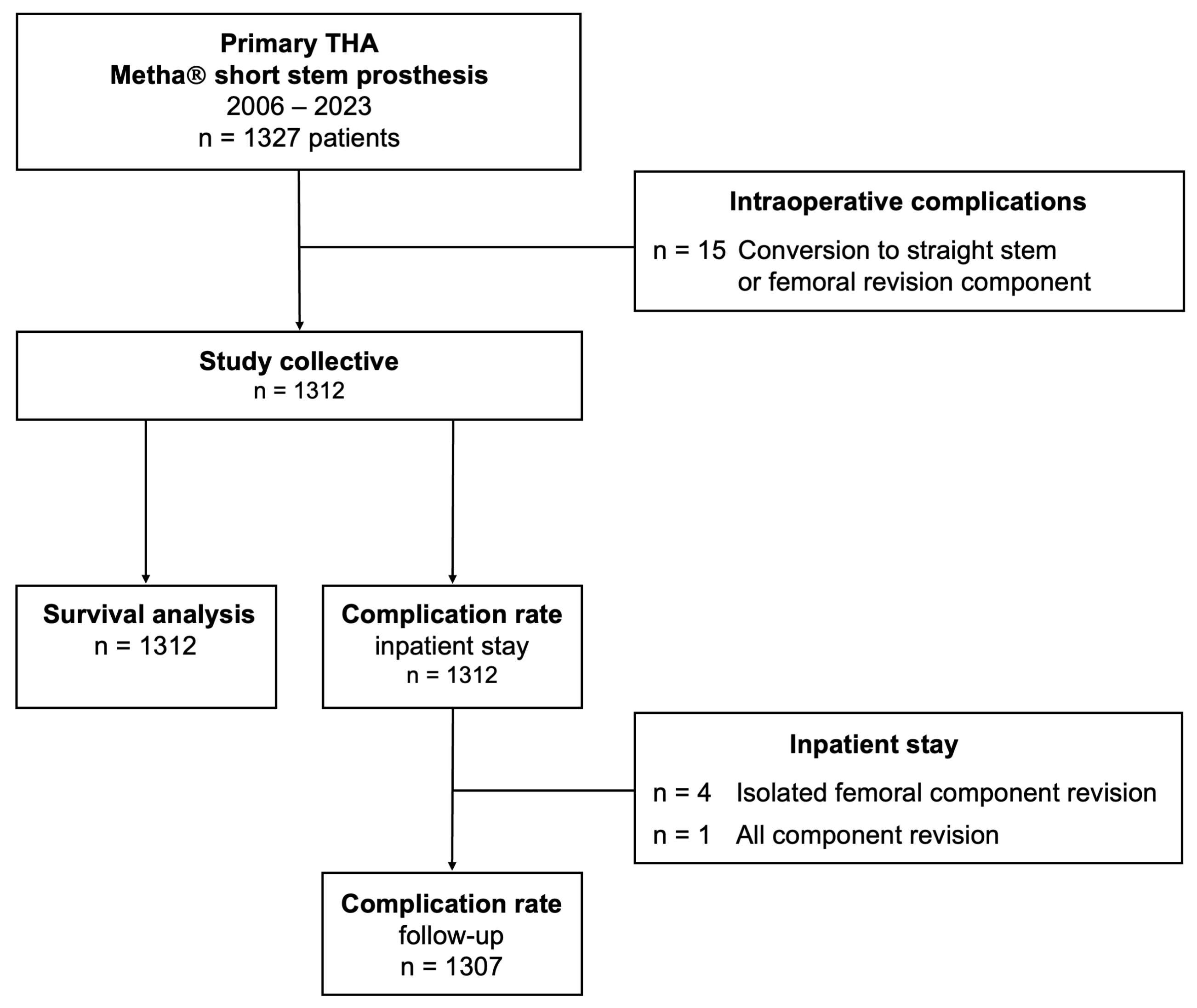
Intraoperative complications were detected in 50 cases (3.77%) and included 44 hairline cracks (3.32%) and 6 intraoperative periprosthetic femur fractures (0.45%) (Table 3). While conservative management was possible in 22 out of 50 cases (44.0%), cerclage cabling was performed in 13 cases (26.0%). In 15 cases (30.0%), intraoperative conversion to a straight stem with diaphyseal anchorage or a femoral revision implant was necessary. These cases were excluded from subsequent analyses (Figure 2).
Table 3.
Intraoperative complications.
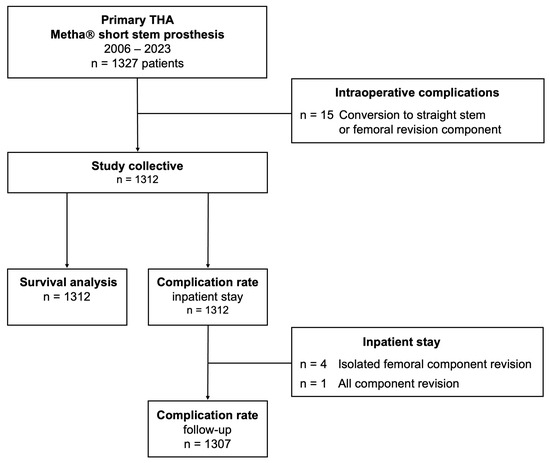
Figure 2.
Flowchart of the study design. THA—total hip arthroplasty.
Direct postoperative complications during inpatient stay were detected in 32 cases, resulting in a complication rate of 2.44% (Table 4). In total, 11 revision procedures were performed during inpatient stay, representing a revision rate of 0.84%. Mean time to revision was 8 days (range 0–12 days). Revision procedures included superficial wound revision (n = 3) and postoperative haematoma evacuation (n = 2). Reasons for early THA revisions were inlay dislocation leading to an isolated head and liner exchange (n = 1; 0.08%); isolated femoral component revisions due to early stem subsidence (n = 2, 0.15%); leg length discrepancy (n = 1, 0.08%); femoral fracture (n = 1, 0.08%); and acetabular component dislocation leading to all component revision (n = 1; 0.08%).
Table 4.
Surgery-related complications and revision procedures during inpatient stay.
Stratified by patient age, overall intraoperative and early postoperative complication rates did not differ significantly between the groups (p = 0.607, p = 0.978).
No statistically significant group differences were observed for intraoperative and early postoperative complication rates stratified by surgical approach (p = 0.097, p = 0.253) or stem design (p = 0.429, p = 0.482).
3.2. Follow-Up
Detailed information on surgery-related complications during the follow-up period is provided in Table 5. Median follow-up period was 86 months (equivalent to approximately 7 years). Of all patients, 857 (65.6%) had a follow-up of minimum 5 years, 386 (45.0%) had a follow-up of minimum 10 years, and 26 (2.0%) had a follow-up of minimum 15 years.
Table 5.
Complications and revision procedures during follow-up.
Postoperative THA-related complications were observed in 89 cases, resulting in a respective complication rate of 6.81%. Overall, complication rates during follow-up did not reveal statistically significant differences between the groups stratified by age (p = 0.636).
Periprosthetic infection was detected in three cases (0.23%), including one acute and one chronic PJI. Mechanical complications following primary short-stem THA accounted for a combined percentage of 5.43%, including three cases of femoral neck adapter fracture (n = 2, 0.15%) or corrosion (n = 1, 0.08%). Stem subsidence was recorded in 44 cases, leading to isolated femoral component revision in 20 cases (1.53%). Periprosthetic femur fractures occurred in five cases (0.38%), of which two Vancouver B1 fractures were treated with open reduction and internal fixation (ORIF), while one case required femoral component revision using a diaphyseal anchoring revision implant.
During the follow-up period, 60 visits to our outpatient clinic were registered due to a prolonged postoperative course with residual functional limitations and hip pain without a mechanical correlate. However, none of these cases resulted in THA revision.
3.3. Survival Analysis
In total, 77 THA revision procedures were performed during inpatient stay and the follow-up period. In 60 cases, the femoral component was revised (Table 6). The majority of femoral stem revisions were attributable to aseptic loosening of the femoral component (46.67%) and stem subsidence (30.00%). Neck adapter failure of the modular stem was observed in 3 out of 195 cases (1.54%). In one case, the reason for rTHA remained unclear, as the surgical procedure was performed in another hospital. Table 6 provides detailed information on the indications leading to femoral component revision.
Table 6.
Indications for stem revisions following primary short-stem THA.
In 25 cases (41.67%), rTHA was performed using a short stem as a revision component. In all of these cases, a larger stem was used and the mean increase in stem size was three sizes (range 1–4 sizes). Femoral stem revision to another primary implant, including anatomic or straight-stem prostheses according to the classification system proposed by Kheir et al. [22], was conducted in 32 cases (53.33%). In one case (1.67%), a femoral revision implant was used.
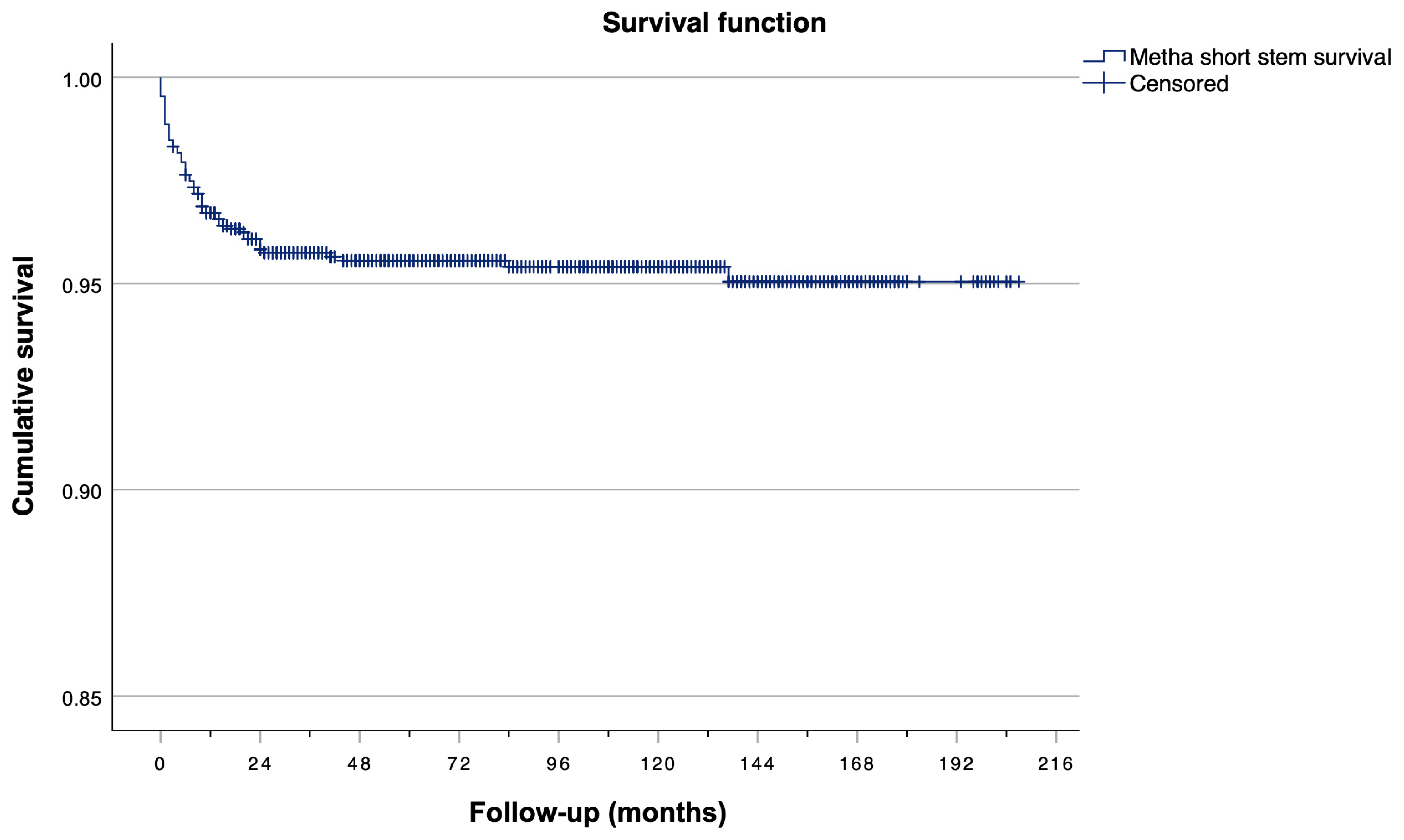
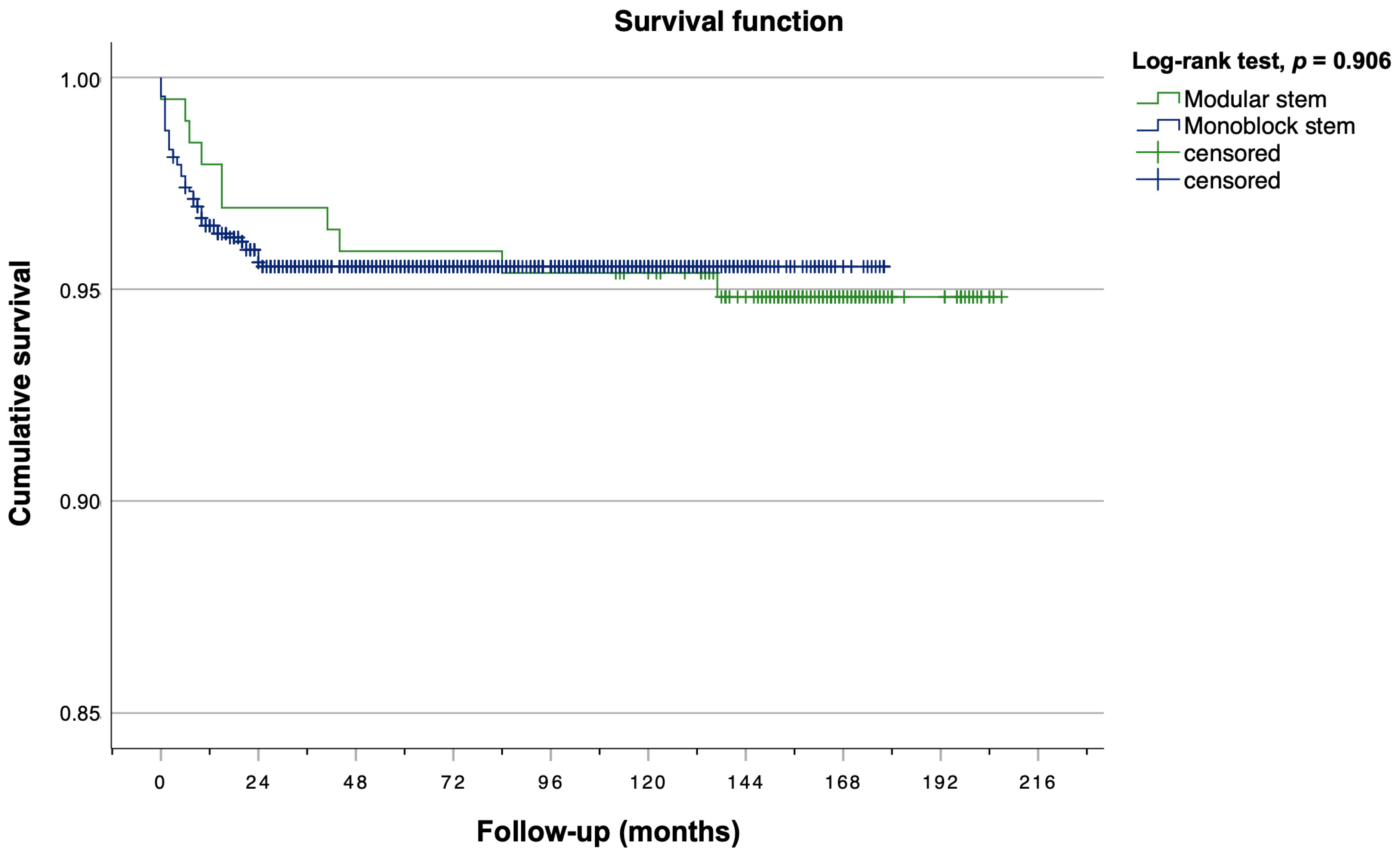
Kaplan–Meier analysis revealed a 5-year survival rate of 95.66% (57/1312), a 10-year survival rate of 95.58% (58/1312), and a 15-year survival rate of 95.50% (59/1312) for both the modular stem and the monoblock stem combined (Figure 3). Moreover, Kaplan–Meier estimators were calculated separately for monoblock and modular stems (Figure 4). No statistically significant between-group differences were observed regarding stem survival (log rank test, p = 0.906). The modular stem exhibited a 5-year survival rate of 95.90% (8/195) and a 10-year survival rate of 95.38% (9/195). For the monoblock stem, 5-year and 10-year survival rates were 96.15% (43/1117) and 95.61% (49/1117), respectively. The most recent stem revision was conducted 25 months after the index surgery.
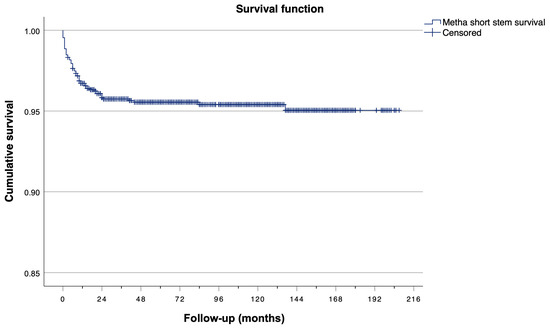
Figure 3.
Kaplan–Meier curve for overall stem survival of the modular stem and monoblock stem combined.
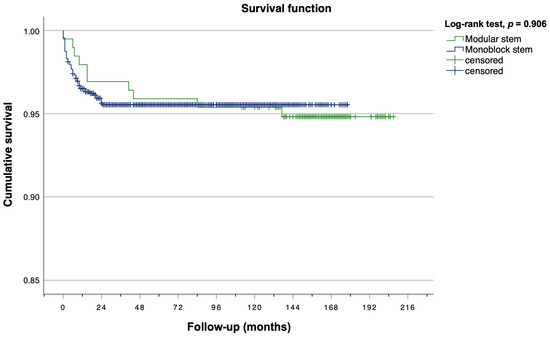
Figure 4.
Kaplan–Meier survival plot for femoral stem revision stratified by stem subgroup.
4. Discussion
The most important finding of this study is that the Metha short-stem prosthesis can achieve comparable long-term survival rates to those of conventional straight-stem prostheses. Moreover, this study demonstrated a low incidence of intra- and postoperative complications and a low rate of required revision surgeries. These findings lend support to the hypothesis that the Metha short-stem prosthesis may be a viable alternative to conventional straight-stem prostheses especially in young patients undergoing THA surgery.
The incidence of intraoperative periprosthetic fractures (IPFF) in primary cementless THA differs, ranging from 0.4% to 6.8% [23,24,25,26]. However, for cementless THA, IPFF rates of up to 28% have been reported in older studies in the literature [27,28]. In our study population, an IPFF rate of 0.45% was observed. This is in line with evidence from previous studies reporting IPFF rates for short-stem THA of 0.8% and 0.4%, respectively [23,25]. Furthermore, we report a total count of 44 intraoperative periprosthetic fissures and calcar cracks, representing 88% of all intraoperative complications. This is consistent with data from the National Joint Registry for England and Wales published in 2019 [29], where calcar cracks were the most common IPFF subtype and the risk of intraoperative calcar cracks was highest in the youngest age group (50–59 years). In contrast, the risk of shaft fractures significantly increased in patients aged more than 80 years. Previous studies revealed an association between femoral canal shape and demographic characteristics [30,31,32]. Specifically, lower age is associated with higher cortical thickness and Dorr type A canal shape, whereas Dorr type C femora, characterised by thin cortices and a wide intramedullary canal, are associated with higher age. Consequently, prolonged and more forceful rasping during femoral canal preparation may be required in younger patients, thus contributing to higher IPFF rates in these patients.
We observed a cumulative postoperative periprosthetic fracture (PPFF) rate of 0.46% during inpatient stay and follow-up, which is lower than previously published evidence on PPFF in short-stem THA. Luger et al. found a significant group difference of PPFF rates in short-stem versus straight-stem arthroplasty (1.7% vs. 3.2%) [25]. Nelson et al. report lower 90-day PPFF rates for short-stem (0.31–1.04%) compared to straight-stem implants (1.22%) and the authors were able to prove non-inferiority for 90-day fracture rate in the short-stem subgroup [33]. However, it must be mentioned that the comparability of these results is limited by the varying follow-up periods reported in these studies. Moreover, it has to be kept in mind that differences in fracture rates may be biased by the different demographic characteristics of the short-stem and straight-stem patient populations. While patients undergoing short-stem THA are often younger and more physically active, older age, the female sex, and poor bone quality are associated with higher risks of PPFF [24,34].
The rate of THA-related complications during inpatient stay was 2.44%. leading to early THA revision in 0.46% of cases. This is in line with evidence from Huang et al., who report a THA-related complication rate of 2.12% during inpatient stay and a revision rate of 1.15% [35]. In the literature, early complications following THA include venous thromboembolism, PJI, and mechanical complications including instability or dislocation, LLD and fractures [36,37]. In our study, early complications also included postoperative wound complications or haematoma leading to surgical revision and temporary neural deficits caused by intraoperative retractor placement. However, as there is no consensus on the definition of early THA revisions and the analysed episodes differ remarkable between the studies, the generalisability of different studies’ results is constrained [38,39,40,41]. For future research, it is essential to establish standards for the reporting of early THA-related complications.
During follow-up, THA-related complications were observed in 6.81% of the cases. In our cohort, mechanical complications accounted for a combined percentage of 5.43%. Previously published studies based on large national databases in the US identified instability or dislocation as the most common reason for rTHA (17.3–19.3%), followed by mechanical loosening (16.8–19.7%) and infection (12.8–17.3%) [42,43,44]. Notably, in our study population, instability and dislocation were observed in only 0.30% of patients, which may be attributable to the fact that a navigation system was used for cup placement in 98% of the cases. Moreover, prior studies investigated the reconstruction of hip biomechanics and functional outcomes using a short stem versus conventional stem and revealed promising results for the reconstruction of individual hip anatomy using cementless short-stem arthroplasty [45,46,47,48]. In our study, aseptic stem or acetabular cup loosening were the most common THA-related complications, with aseptic loosening of the femoral component being the predominant reason for stem revision (46.67%), followed by stem subsidence (30.00%). This is in line with evidence from recent studies. In a study by Schwarz et al., aseptic loosening accounted for 40.87% of rTHA procedures [40]. Furthermore, Markel et al. found significant differences in causes for rTHA over time and a steady increase in the incidence of aseptic loosening, as it accounted for 20.5% of rTHA performed within 6–12 months postoperatively and for 31.9% of rTHA performed beyond one year post index procedure. [38] Given the proportion of femoral stem revisions attributable to aseptic loosening and the relatively high lifetime risk of revision for young patients undergoing THA, short stems may be considered a bone-preserving alternative to straight-stem implants in a younger patient population.
Implant survival rates were 95.7%, 95.6%, and 95.5% after 5, 10, and 15 years, respectively, with the primary endpoint of femoral stem revision. The revision rate observed in our study population was higher than those previously reported. Weenders et al. observed a 2.5% ten-year revision rate for the monoblock stem [49], and Schnurr et al. reported a 4.1% all-cause revision rate after a mean follow-up of 6 years and a 7-year stem revision rate of 1.5 and 1.8% for the monoblock and modular stem, respectively [15]. A recent review by Malahias et al. showed a 2.5% revision rate and found failure of the modular neck adapter to be the most common reason for revision [50]. Of note, only three neck adapter failures (0.23%) occurred in our population, which is lower than previously reported rates of up to 6% [15,17,51]. Interestingly, in our study sample, nearly all femoral component revisions were performed within the first two years following the index procedure. As aseptic loosening and stem subsidence were the leading causes for stem revisions, a mismatch between proximal femoral anatomy and implant geometry may be a possible explanation. This hypothesis is supported by evidence from previous studies, which showed an association between early subsidence and increased revision rates due to aseptic loosening [52], and identified undersizing as one of the main reasons for early stem failure [53,54]. In our study cohort, the mean increase of stem size in rTHA using another short-stem implant was three sizes, which may support this finding. However, as no radiological follow-up was conducted, this remains hypothetical. A comprehensive radiological analysis of femoral morphology and femoral component filling, as well as a thorough investigation of the radiological signs of implant failure, would be of value.
The current study exhibits several noteworthy strengths, including large sample size, long-term follow-up, and comprehensive data on THA-related intra- and postoperative complications and revision rates. However, it is essential to acknowledge the study is not without limitations. First, it is limited by its retrospective and single-centre design, as both aspects introduce a risk of bias. Due to the retrospective design, no clinical follow-up was conducted, and consequently, some cases may have been lost to follow-up. However, this limitation may be offset by the fact that most THA-related complications are readmitted to the primary institution, especially given that this study was conducted in a tertiary referral centre. Second, the results presented in this study are based on complication and revision rates only, and patient-reported outcome measures were not available. Third, no radiological data are presented. Future studies are warranted to examine the radiographic changes following short-stem THA in a longitudinal study design including radiological signs of bone remodelling, aseptic loosening, or stem subsidence.
5. Conclusions
In conclusion, our study provides a comprehensive analysis of postoperative complication and revision rates in a large sample undergoing cementless primary THA using the Metha short-stem prosthesis. Postoperative THA-related complication rates were favourable, and the implant survival rate of 96% at ten years is promising. However, as a relevant proportion of stem failures was observed within two years after the index procedure, future studies are required to investigate early radiological outcomes and implant positioning including the analysis of proximal femoral anatomy and the canal fill ratio or modified neck fill ratio of short-stem implants as well as clinical and radiological long-term outcomes.
Author Contributions
Conceptualisation, R.S., M.E. and G.H.S.; methodology, R.S. and G.H.S.; validation, R.S., N.T.B. and G.H.S.; data curation, R.S., N.T.B. and G.H.S.; formal analysis, R.S., N.T.B. and G.H.S.; writing—original draft, R.S.; writing—review and editing, R.S., N.T.B., P.S., M.E. and G.H.S.; supervision, R.S., P.S., M.E. and G.H.S.; project administration, G.H.S. All authors commented on previous versions of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Oldenburg (#2023-261, date of approval: 19 December 2023).
Informed Consent Statement
Patient consent was waived. The legal basis for the processing of data for this study is Art. 6 par. 1 lit. e in connection with Art. 9 para. 2 lit. j GDPR in connection with § 13 NDSG. In accordance with § 13 NDSG, a weighing of interests was carried out prior to this study’s implementation, which was approved by the responsible data protection officer and resulted in a consent waiver. Furthermore, for the hospital involved in this study, church data protection regulations also apply. According to § 11 (2) lit. i. KDG, the processing of health data is permitted even without explicit consent if this is necessary to ensure high quality and safety standards in healthcare. The retrospective evaluation of our routinely collected clinical data for the purpose of analysing the complication and revision rates as well as the implant survival of the Metha® short-stem prosthesis serves the purpose of ensuring high quality and safety standards and thus the protection and promotion of public health.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author due to ethical and data privacy/protection reasons.
Acknowledgments
The authors thank Laura Lee Linngroen for their help with data collection.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ASA | American Society of Anesthesiologists |
| BMI | Body Mass Index |
| DAIR | Debridement, antibiotics, and implant retention |
| FAI | Femoroacetabular Impingement |
| IPFF | Intraoperative periprosthetic femur fractures |
| LCPD | Legg–Calvé–Perthes disease |
| LLD | Leg length discrepancy |
| LTRR | Lifetime risk of revision |
| OA | Osteoarthritis |
| ORIF | Open reduction and internal fixation |
| PJI | Periprosthetic joint infection |
| PPFF | Postoperative periprosthetic femur fractures |
| rTHA | Revision total hip arthroplasty |
| THA | Total hip arthroplasty |
| SCFE | Slipped capital femoral epiphysis |
References
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. Am. Vol. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Shichman, I.; Roof, M.; Askew, N.; Nherera, L.; Rozell, J.C.; Seyler, T.M.; Schwarzkopf, R. Projections and Epidemiology of Primary Hip and Knee Arthroplasty in Medicare Patients to 2040-2060. JBJS Open Access 2023, 8, e22.00112. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.; Ong, K.; Zhao, K.; Kelly, M.; Bozic, K.J. Future young patient demand for primary and revision joint replacement: National projections from 2010 to 2030. Clin. Orthop. Relat. Res. 2009, 467, 2606–2612. [Google Scholar] [CrossRef]
- Kuijpers, M.F.L.; Hannink, G.; van Steenbergen, L.N.; Schreurs, B.W. Total Hip Arthroplasty in Young Patients in The Netherlands: Trend Analysis of >19,000 Primary Hip Replacements in the Dutch Arthroplasty Register. J. Arthroplast. 2018, 33, 3704–3711. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.G.; Sogbein, O.A.; McClure, J.A.; Reid, J.; Welk, B.; Lanting, B.A.; Degen, R.M. Total Hip Arthroplasty in Patients Aged 40 to 60 Years Old: A Population-Based Study. J. Arthroplast. 2023, 38, S83–S88.e82. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.T.; Evans, J.P.; Walker, R.W.; Blom, A.W.; Whitehouse, M.R.; Sayers, A. How long does a hip replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. Lancet 2019, 393, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Bayliss, L.E.; Culliford, D.; Monk, A.P.; Glyn-Jones, S.; Prieto-Alhambra, D.; Judge, A.; Cooper, C.; Carr, A.J.; Arden, N.K.; Beard, D.J.; et al. The effect of patient age at intervention on risk of implant revision after total replacement of the hip or knee: A population-based cohort study. Lancet 2017, 389, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- de Waard, S.; van der Vis, J.; Venema, P.; Sierevelt, I.N.; Kerkhoffs, G.; Haverkamp, D. Short-term success of proximal bone stock preservation in short hip stems: A systematic review of the literature. EFORT Open Rev. 2021, 6, 1040–1051. [Google Scholar] [CrossRef]
- Lavernia, C.; D’Apuzzo, M.; Hernandez, V.; Lee, D. Thigh pain in primary total hip arthroplasty: The effects of elastic moduli. J. Arthroplast. 2004, 19, 10–16. [Google Scholar] [CrossRef]
- Engh, C.A., Jr.; Young, A.M.; Engh, C.A., Sr.; Hopper, R.H., Jr. Clinical consequences of stress shielding after porous-coated total hip arthroplasty. Clin. Orthop. Relat. Res. 2003, 417, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Burchard, R.; Graw, J.A.; Soost, C.; Schmitt, J. Stress shielding effect after total hip arthroplasty varies between combinations of stem design and stiffness-a comparing biomechanical finite element analysis. Int. Orthop. 2023, 47, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Jang, Y.S.; Kim, E.J. A Prospective, Randomized Comparison of the Long-Term Clinical and Radiographic Results of an Ultra-Short vs a Conventional Length Cementless Anatomic Femoral Stem. J. Arthroplast. 2021, 36, 1707–1713. [Google Scholar] [CrossRef] [PubMed]
- Khanuja, H.S.; Banerjee, S.; Jain, D.; Pivec, R.; Mont, M.A. Short bone-conserving stems in cementless hip arthroplasty. J. Bone Jt. Surg. Am. Vol. 2014, 96, 1742–1752. [Google Scholar] [CrossRef] [PubMed]
- Schnurr, C.; Schellen, B.; Dargel, J.; Beckmann, J.; Eysel, P.; Steffen, R. Low Short-Stem Revision Rates: 1-11 Year Results From 1888 Total Hip Arthroplasties. J Arthroplast. 2017, 32, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Loppini, M.; Grappiolo, G. Uncemented short stems in primary total hip arthroplasty: The state of the art. EFORT Open Rev. 2018, 3, 149–159. [Google Scholar] [CrossRef]
- Grupp, T.M.; Weik, T.; Bloemer, W.; Knaebel, H.P. Modular titanium alloy neck adapter failures in hip replacement--failure mode analysis and influence of implant material. BMC Musculoskelet. Disord. 2010, 11, 3. [Google Scholar] [CrossRef]
- Jauch, S.Y.; Huber, G.; Hoenig, E.; Baxmann, M.; Grupp, T.M.; Morlock, M.M. Influence of material coupling and assembly condition on the magnitude of micromotion at the stem-neck interface of a modular hip endoprosthesis. J. Biomech. 2011, 44, 1747–1751. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, H.; Krishnan, S.P.; Blunn, G.; Skinner, J.A.; Hart, A.J. Modular neck femoral stems. Bone Jt. J. 2013, 95-b, 1011–1021. [Google Scholar] [CrossRef]
- Carter, L.W.; Stovall, D.O.; Young, T.R. Determination of accuracy of preoperative templating of noncemented femoral prostheses. J. Arthroplast. 1995, 10, 507–513. [Google Scholar] [CrossRef]
- Healy, W.L.; Iorio, R.; Clair, A.J.; Pellegrini, V.D.; Della Valle, C.J.; Berend, K.R. Complications of Total Hip Arthroplasty: Standardized List, Definitions, and Stratification Developed by The Hip Society. Clin. Orthop. Relat. Res. 2016, 474, 357–364. [Google Scholar] [CrossRef]
- Kheir, M.M.; Drayer, N.J.; Chen, A.F. An Update on Cementless Femoral Fixation in Total Hip Arthroplasty. J. Bone Jt. Surg. Am. Vol. 2020, 102, 1646–1661. [Google Scholar] [CrossRef]
- Molli, R.G.; Lombardi, A.V., Jr.; Berend, K.R.; Adams, J.B.; Sneller, M.A. A short tapered stem reduces intraoperative complications in primary total hip arthroplasty. Clin. Orthop. Relat. Res. 2012, 470, 450–461. [Google Scholar] [CrossRef] [PubMed]
- Abdel, M.P.; Watts, C.D.; Houdek, M.T.; Lewallen, D.G.; Berry, D.J. Epidemiology of periprosthetic fracture of the femur in 32 644 primary total hip arthroplasties: A 40-year experience. Bone Jt. J. 2016, 98-b, 461–467. [Google Scholar] [CrossRef]
- Luger, M.; Feldler, S.; Pisecky, L.; Klasan, A.; Gotterbarm, T.; Schopper, C. Periprosthetic Femoral Fractures in Cementless Short Versus Straight Stem Total Hip Arthroplasty: A Propensity Score Matched Analysis. J. Arthroplast. 2023, 38, 751–756. [Google Scholar] [CrossRef]
- Dietrich, M.; Kabelitz, M.; Dora, C.; Zingg, P.O. Perioperative Fractures in Cementless Total Hip Arthroplasty Using the Direct Anterior Minimally Invasive Approach: Reduced Risk With Short Stems. J. Arthroplast. 2018, 33, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Berend, K.R.; Lombardi, A.V., Jr. Intraoperative femur fracture is associated with stem and instrument design in primary total hip arthroplasty. Clin. Orthop. Relat. Res. 2010, 468, 2377–2381. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.H.; Kyle, R.F. Periprosthetic fractures of the femur. Orthop. Clin. N. Am. 2002, 33, 143–152, ix. [Google Scholar] [CrossRef]
- Lamb, J.N.; Matharu, G.S.; Redmond, A.; Judge, A.; West, R.M.; Pandit, H.G. Risk Factors for Intraoperative Periprosthetic Femoral Fractures During Primary Total Hip Arthroplasty. An Analysis From the National Joint Registry for England and Wales and the Isle of Man. J. Arthroplast. 2019, 34, 3065–3073.e3061. [Google Scholar] [CrossRef] [PubMed]
- Dorr, L.D.; Faugere, M.C.; Mackel, A.M.; Gruen, T.A.; Bognar, B.; Malluche, H.H. Structural and cellular assessment of bone quality of proximal femur. Bone 1993, 14, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Noble, P.C.; Alexander, J.W.; Lindahl, L.J.; Yew, D.T.; Granberry, W.M.; Tullos, H.S. The anatomic basis of femoral component design. Clin. Orthop. Relat. Res. 1988, 235, 148–165. [Google Scholar] [CrossRef]
- Casper, D.S.; Kim, G.K.; Parvizi, J.; Freeman, T.A. Morphology of the proximal femur differs widely with age and sex: Relevance to design and selection of femoral prostheses. J. Orthop. Res. 2012, 30, 1162–1166. [Google Scholar] [CrossRef]
- Nelson, J.T.; Zheng, H.; Hallstrom, B.R.; Hughes, R.E.; Mont, M.A.; Masini, M.A. Are Short Stems Associated With Higher Fracture Rates and Early Revision Rates in Primary Total Hip Arthroplasty? A Noninferiority Analysis. J. Arthroplast. 2023, 38, 1287–1294.e1282. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.P.; Chan, P.H.; Prentice, H.A.; Paxton, E.W.; Hinman, A.D.; Khatod, M. Cause-Specific Stem Revision Risk in Primary Total Hip Arthroplasty Using Cemented vs Cementless Femoral Stem Fixation in a US Cohort. J. Arthroplast. 2022, 37, 89–96.e81. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Yang, Q.; Wang, Z.; Pan, Z.; Zhang, Y.; Shi, Z.; Yang, S. Comparisons of in-hospital complications between total hip arthroplasty and hip resurfacing arthroplasty. BMC Musculoskelet. Disord. 2023, 24, 375. [Google Scholar] [CrossRef] [PubMed]
- Fontalis, A.; Berry, D.J.; Shimmin, A.; Slullitel, P.A.; Buttaro, M.A.; Li, C.; Malchau, H.; Haddad, F.S. Prevention of early complications following total hip replacement. SICOT J. 2021, 7, 61. [Google Scholar] [CrossRef] [PubMed]
- Descamps, J.; Teissier, V.; Graff, W.; Mouton, A.; Bouché, P.A.; Marmor, S. Managing early complications in total hip arthroplasty: The safety of immediate revision. J. Orthop. Traumatol. 2023, 24, 38. [Google Scholar] [CrossRef] [PubMed]
- Markel, J.F.; Driscoll, J.A.; Zheng, T.H.; Hughes, R.E.; Moore, D.D.; Hallstrom, B.R.; Markel, D.C. Causes of Early Hip Revision Vary by Age and Gender: Analysis of Data From a Statewide Quality Registry. J. Arthroplast. 2022, 37, S616–S621. [Google Scholar] [CrossRef] [PubMed]
- Novikov, D.; Mercuri, J.J.; Schwarzkopf, R.; Long, W.J.; Bosco Iii, J.A.; Vigdorchik, J.M. Can some early revision total hip arthroplasties be avoided? Bone Jt. J. 2019, 101-b, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, J.S.; Lygrisse, K.A.; Roof, M.A.; Long, W.J.; Schwarzkopf, R.M.; Hepinstall, M.S. Early, Mid-Term, and Late-Term Aseptic Femoral Revisions After THA: Comparing Causes, Complications, and Resource Utilization. J. Arthroplast. 2021, 36, 3551–3555. [Google Scholar] [CrossRef]
- Shen, T.S.; Gu, A.; Bovonratwet, P.; Ondeck, N.T.; Sculco, P.K.; Su, E.P. Etiology and Complications of Early Aseptic Revision Total Hip Arthroplasty Within 90 Days. J. Arthroplast. 2021, 36, 1734–1739. [Google Scholar] [CrossRef]
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Vail, T.P.; Berry, D.J. The epidemiology of revision total hip arthroplasty in the United States. J. Bone Jt. Surg. Am. 2009, 91, 128–133. [Google Scholar] [CrossRef]
- Gwam, C.U.; Mistry, J.B.; Mohamed, N.S.; Thomas, M.; Bigart, K.C.; Mont, M.A.; Delanois, R.E. Current Epidemiology of Revision Total Hip Arthroplasty in the United States: National Inpatient Sample 2009 to 2013. J Arthroplast. 2017, 32, 2088–2092. [Google Scholar] [CrossRef] [PubMed]
- Hinton, Z.W.; Wu, C.J.; Ryan, S.P.; Cunningham, D.J.; Green, C.L.; Lachiewicz, P.F. Current Trends in Revision Hip Arthroplasty: Indications and Types of Components Revised. J. Arthroplast. 2022, 37, S611–S615.e617. [Google Scholar] [CrossRef] [PubMed]
- Innmann, M.M.; Spier, K.; Streit, M.R.; Aldinger, P.R.; Bruckner, T.; Gotterbarm, T.; Merle, C. Comparative Analysis of the Reconstruction of Individual Hip Anatomy Using 3 Different Cementless Stem Designs in Patients With Primary Hip Osteoarthritis. J. Arthroplast. 2018, 33, 1126–1132. [Google Scholar] [CrossRef] [PubMed]
- Schmidutz, F.; Beirer, M.; Weber, P.; Mazoochian, F.; Fottner, A.; Jansson, V. Biomechanical reconstruction of the hip: Comparison between modular short-stem hip arthroplasty and conventional total hip arthroplasty. Int. Orthop. 2012, 36, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Maurer-Ertl, W.; Friesenbichler, J.; Pfann, M.; Maier, M.; Reinbacher, P.; Leithner, A.; Smolle, M.A. Restoration of hip geometry after total hip arthroplasty: Retrospective comparison of two short stems and one straight stem. BMC Musculoskelet. Disord. 2022, 23, 1035. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, M.; Hein, M.A.; Faschingbauer, M.; Sgroi, M.; Bieger, R.; Reichel, H.; Freitag, T. Abductor Muscle Force after Straight-Stem Compared to Short-Stem Total Hip Arthroplasty through a Modified Direct Lateral Approach: Functional Assessment of 70 Consecutive Patients of a Randomized Controlled Clinical Trial. J. Clin. Med. 2021, 10, 1235. [Google Scholar] [CrossRef] [PubMed]
- Weenders, S.G.M.; Merfort, R.; Eschweiler, J.; Hildebrand, F.; Gruner, A.; Heller, K.D. Ten-year follow-up and clinical outcome of a metaphyseal anchoring short hip stem prosthesis: A retrospective single-centre analysis. Int. Orthop. 2024, 48, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Malahias, M.A.; Tejaswi, P.; Chytas, D.; Kadu, V.; Karanikas, D.; Thorey, F. The clinical outcome of the Metha short hip stem: A systematic scoping review. HIP Int. 2021, 31, 24–33. [Google Scholar] [CrossRef]
- von Lewinski, G.; Floerkemeier, T. 10-year experience with short stem total hip arthroplasty. Orthopedics 2015, 38, S51–S56. [Google Scholar] [CrossRef]
- Streit, M.R.; Haeussler, D.; Bruckner, T.; Proctor, T.; Innmann, M.M.; Merle, C.; Gotterbarm, T.; Weiss, S. Early Migration Predicts Aseptic Loosening of Cementless Femoral Stems: A Long-term Study. Clin. Orthop. Relat. Res. 2016, 474, 1697–1706. [Google Scholar] [CrossRef]
- Mittelstaedt, H.; Anderl, C.; Ortmaier, R.; Johl, C.; Krüger, T.; Wallroth, K.; Weigert, U.; Schagemann, J.C. Subsidence analysis of a cementless short stem THA using EBRA-FCA-A seven-year prospective multicentre study. J. Orthop. 2023, 43, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Kutzner, K.P.; Freitag, T.; Bieger, R. Defining ‘undersizing’ in short-stem total hip arthroplasty: The importance of sufficient contact with the lateral femoral cortex. HIP Int. 2022, 32, 160–165. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).