

Unraveling Catechol-O-Methyltransferase rs4680 SNP’s Role in Patients’ Response to Tramadol and Its Adverse Effects: A Pharmacogenetics Insight into Postoperative Pain Management
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. The Inclusion Criteria and Exclusion Criteria
2.3. Sampling
2.4. Dependent Variable Assessment
2.5. Genetic Analysis
2.6. Statistical Analysis
3. Results
3.1. Allele Frequency of COMT Rs4680
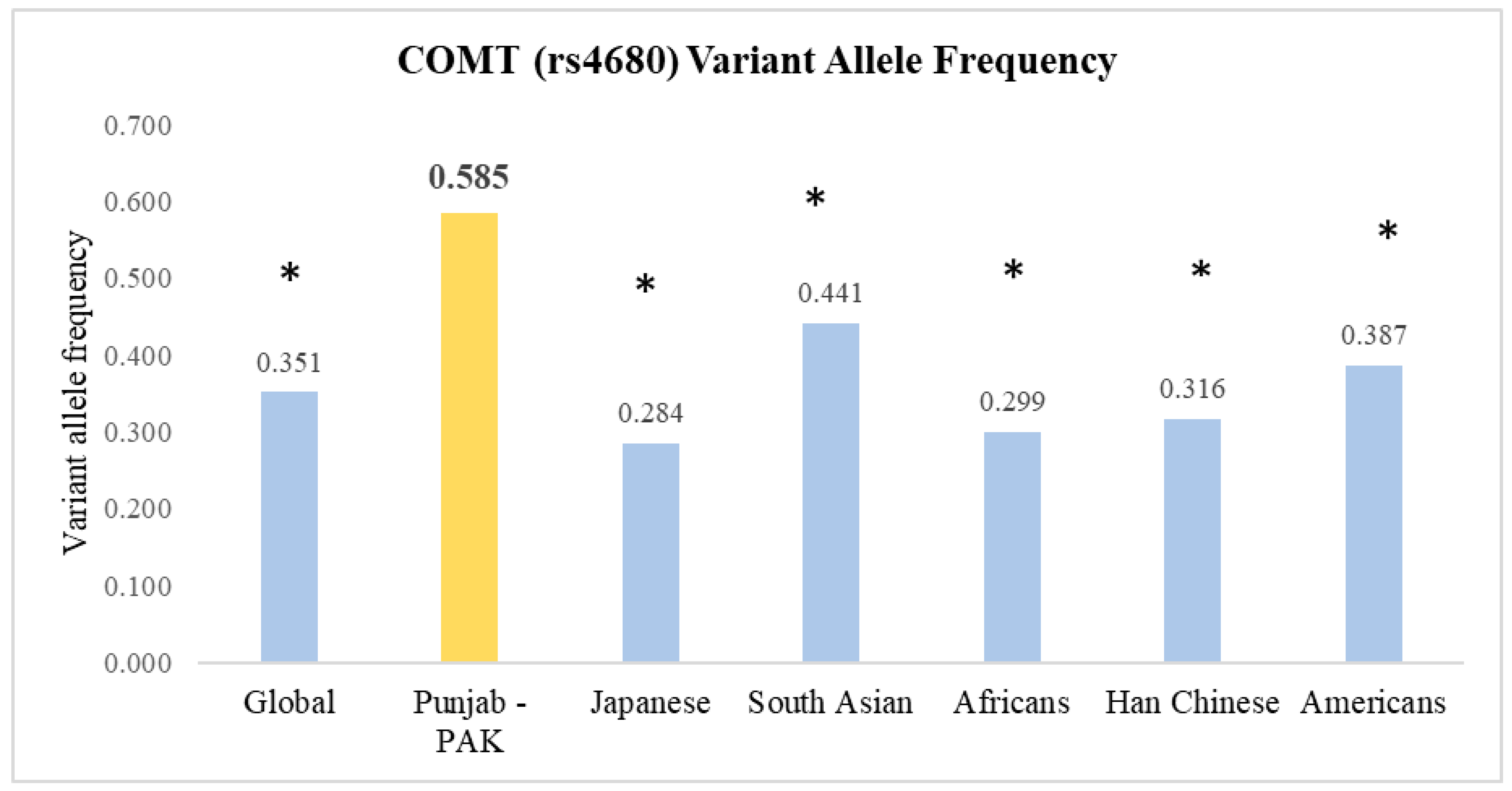
3.2. Comparing rs4680 Allele Frequencies with Global Data
3.3. Post-Operative Pain Scores at Rest and on Raising Head by COMT (rs4680) Genotype
3.4. Incidence of Nausea and Vomiting following Tramadol Administration Based on COMT (rs4680) Genotype at Various Post-Operative Time Points
3.5. Sedation Scores in Patients following Tramadol Administration Based on COMT (rs4680) Genotype
3.6. Incidence of Other Side Effects following Tramadol Administration among COMT (rs4680) Genotypes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Saidi, I.; Russell, A.; Dizdarevic, A. The Acute Perioperative Pain Service: Impact, Organization, and Future Directions. In Current Pain and Headache Reports; Springer: Berlin/Heidelberg, Germany, 2023; Volume 27, pp. 399–405. [Google Scholar] [CrossRef]
- Craig, K.D.; MacKenzie, N.E. What is pain: Are cognitive and social features core components? Paediatr. Neonatal Pain. 2021, 3, 106. [Google Scholar] [CrossRef]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Gan, T.J. Poorly controlled postoperative pain: Prevalence, consequences, and prevention. J. Pain Res. 2017, 10, 2287–2298. [Google Scholar] [CrossRef]
- Ismail, S.; Siddiqui, A.S.; Rehman, A. Postoperative pain management practices and their effectiveness after major gynecological surgery: An observational study in a tertiary care hospital. J. Anaesthesiol. Clin. Pharmacol. 2018, 34, 478–484. [Google Scholar] [CrossRef]
- Obeng, A.O.; Hamadeh, I.; Smith, M. Review of Opioid Pharmacogenetics and Considerations for Pain Management. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 1105–1121. [Google Scholar] [CrossRef]
- Nakhaee, S.; Hoyte, C.; Dart, R.C.; Askari, M.; Lamarine, R.J.; Mehrpour, O. A review on tramadol toxicity: Mechanism of action, clinical presentation, and treatment. Forensic Toxicol. 2021, 39, 293–310. [Google Scholar] [CrossRef]
- Tammimäki, A.; Männistö, P.T. Catechol-O-methyltransferase gene polymorphism and chronic human pain: A systematic review and meta-analysis. Pharmacogenet. Genom. 2012, 22, 673–691. [Google Scholar] [CrossRef]
- Gupta, M.; Kaur, H.; Jajodia, A.; Jain, S.; Satyamoorthy, K.; Mukerji, M.; Thirthalli, J.; Kukreti, R. Diverse facets of COMT: From a plausible predictive marker to a potential drug target for schizophrenia. Curr. Mol. Med. 2011, 11, 732–743. [Google Scholar] [CrossRef]
- Andersen, S.; Skorpen, F. Variation in the COMT gene: Implications for pain perception and pain treatment. Pharmacogenomics 2009, 10, 669–684. [Google Scholar] [CrossRef]
- Weinshilboum, R.M. Pharmacogenomics: Catechol O-Methyltransferase to Thiopurine S-Methyltransferase. Cell. Mol. Neurobiol. 2006, 26, 537–559. [Google Scholar] [CrossRef]
- Chen, J.; Lipska, B.K.; Halim, N.; Ma, Q.D.; Matsumoto, M.; Melhem, S.; Kolachana, B.S.; Hyde, T.M.; Herman, M.M.; Apud, J.; et al. Functional Analysis of Genetic Variation in Catechol-O-Methyltransferase (COMT): Effects on mRNA, Protein, and Enzyme Activity in Postmortem Human Brain. Am. J. Hum. Genet. 2004, 75, 807–821. [Google Scholar] [CrossRef] [PubMed]
- Rakvåg, T.T.; Ross, J.R.; Sato, H.; Skorpen, F.; Kaasa, S.; Klepstad, P. Genetic variation in the Catechol-O-Methyltransferase (COMT) gene and morphine requirements in cancer patients with pain. Mol. Pain. 2008, 4, 1744–8069. [Google Scholar] [CrossRef] [PubMed]
- Candiotti, K.A.; Yang, Z.; Buric, D.; Arheart, K.; Zhang, Y.; Rodriguez, Y.; Gitlin, M.C.; Carvalho, E.; Jaraba, I.; Wang, L. Catechol-O-Methyltransferase Polymorphisms Predict Opioid Consumption in Postoperative Pain. Obstet. Anesth. 2014, 119, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; LI, M.; Chen, G.; Song, H. Effects of COMT G472A genetic polymorphism on postoperative analgesia with fentanyl. Chin. J. Anesthesiol. 2011, 12, 1039–1041. [Google Scholar]
- De Gregori, M.; Diatchenko, L.; Ingelmo, P.M.; Napolioni, V.; Klepstad, P.; Belfer, I.; Molinaro, V.; Garbin, G.; Ranzani, G.N.; Alberio, G.; et al. Human Genetic Variability Contributes to Postoperative Morphine Consumption. J. Pain 2016, 17, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Zhang, X.; Xu, G.; Zhang, Q.; Qian, P.; Liu, S.; Zhu, J.; Shen, R. Association between COMT Polymorphism Val158Met and Opioid Consumption in Patients with Postoperative Pain: A Meta-Analysis. Neurosignals 2018, 26, 11–21. [Google Scholar] [CrossRef]
- Stingl, J.; Brockmöller, J. Study Designs in Clinical Pharmacogenetic and Pharmacogenomic Research. In Pharmacogenomics; Academic Press: Cambridge, CA, USA, 2013; pp. 309–341. [Google Scholar]
- Hong, E.P.; Park, J.W. Sample Size and Statistical Power Calculation in Genetic Association Studies. Genom. Inform. 2012, 10, 117–122. [Google Scholar] [CrossRef]
- Johnson, J.L.; Abecasis, G.R. GAS Power Calculator: Web-based power calculator for genetic association studies. bioRxiv 2017, 164343. [Google Scholar]
- Neskovic, N.; Mandic, D.; Marczi, S.; Skiljic, S.; Kristek, G.; Vinkovic, H.; Mraovic, B.; Debeljak, Z.; Kvolik, S. Different Pharmacokinetics of Tramadol, O-Demethyltramadol and N-Demethyltramadol in Postoperative Surgical Patients From Those Observed in Medical Patients. Front. Pharmacol. 2021, 12, 656748. [Google Scholar] [CrossRef]
- Karcioglu, O.; Topacoglu, H.; Dikme, O.; Dikme, O. A systematic review of the pain scales in adults: Which to use? Am. J. Emerg. Med. 2018, 36, 707–714. [Google Scholar] [CrossRef]
- Nisbet, A.T.; Mooney-Cotter, F. Comparsion of Selected Sedation Scales for Reporting Opioid-Induced Sedation Assessment. Pain Manag. Nurs. 2009, 10, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Mallick-Searle, T.; Fillman, M. The pathophysiology, incidence, impact, and treatment of opioid-induced nausea and vomiting. J. Am. Assoc. Nurse Pract. 2017, 29, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Myles, P.S.; Wengritzky, R. Simplified postoperative nausea and vomiting impact scale for audit and post-discharge review. Br. J. Anaesth. 2012, 108, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Gautam, A. Phenol-Chloroform DNA Isolation Method. In DNA and RNA Isolation Techniques for Non-Experts; Springer: Cham, Switzerland, 2022; pp. 33–39. [Google Scholar]
- Hall, N. Advanced sequencing technologies and their wider impact in microbiology. J. Exp. Biol. 2007, 210, 1518–1525. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. 2018 rs4680 RefSNP Report-dbSNP-NCBI. Available online: https://www.ncbi.nlm.nih.gov/snp/rs4680 (accessed on 16 August 2023).
- Barakat, A. Revisiting Tramadol: A Multi-Modal Agent for Pain Management. CNS Drugs 2019, 33, 481–501. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, A.; Reichl, S.U.; Meyer-Frießem, C.; Zahn, P.K.; Pogatzki-Zahn, E. Tramadol for postoperative pain treatment in children. Cochrane Database Syst. Rev. 2015, 2019, CD009574. [Google Scholar] [CrossRef] [PubMed]
- Matic, M.; de Wildt, S.N.; Tibboel, D.; van Schaik, R.H. Analgesia and Opioids: A Pharmacogenetics Shortlist for Implementation in Clinical Practice. Clin. Chem. 2017, 63, 1204–1213. [Google Scholar] [CrossRef]
- Wise, M.J. On hardy-weinberg in introductory biology: Teaching this fundamental principle in an authentic, engaging, and accurate manner. Bioscene 2018, 44, 37–41. [Google Scholar]
- Kambur, O.; Männistö, P.T. Catechol-O-methyltransferase and pain. Int. Rev. Neurobiol. 2010, 95, 227–279. [Google Scholar]
- Pertovaara, A. The noradrenergic pain regulation system: A potential target for pain therapy. Eur. J. Pharmacol. 2013, 716, 2–7. [Google Scholar] [CrossRef]
- Bastos, P.; Gomes, T.; Ribeiro, L. Catechol-O-methyltransferase (COMT): An update on its role in cancer, neurological and cardiovascular diseases. Rev. Physiol. Biochem. Pharmacol. 2017, 173, 1–39. [Google Scholar] [PubMed]
- Binder, W.; Mousa, S.A.; Sitte, N.; Kaiser, M.; Stein, C.; Schafer, M. Sympathetic activation triggers endogenous opioid release and analgesia within peripheral inflamed tissue. Eur. J. Neurosci. 2004, 20, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, L.M.; Christrup, L.L.; Sato, H.; Drewes, A.M.; Olesen, A.E. Genetic Influences of OPRM1, OPRD1 and COMT on Morphine Analgesia in a Multi-Modal, Multi-Tissue Human Experimental Pain Model. Basic Clin. Pharmacol. Toxicol. 2017, 121, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.L.; Patel, J.N. Pharmacogenomics Personalizing supportive care in oncology. Pharmacogenomics 2016, 17, 417–434. [Google Scholar] [CrossRef] [PubMed]
- Vieira, C.M.P.; Fragoso, R.M.; Pereira, D.; Medeiros, R. Pain polymorphisms and opioids: An evidence based review. Mol. Med. Rep. 2019, 19, 1423–1434. [Google Scholar] [CrossRef] [PubMed]
- Kowarik, M.C.; Einhäuser, J.; Jochim, B.; Büttner, A.; Tölle, T.R.; Riemenschneider, M.; Platzer, S.; Berthele, A. Impact of the COMT Val108/158Met polymorphism on the mu-opioid receptor system in the human brain: Mu-opioid receptor, met-enkephalin and beta-endorphin expression. Neurosci. Lett. 2012, 506, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Lee, K.S.; Kim, J.S.; Kim, Y.I.; Shin, H.E. Genetic Contribution of Catechol-O-methyltransferase Polymorphism in Patients with Migraine without Aura. J. Clin. Neurol. 2007, 3, 24–30. [Google Scholar] [CrossRef]
- Laugsand, E.A.; Fladvad, T.; Skorpen, F.; Maltoni, M.; Kaasa, S.; Fayers, P.; Klepstad, P. Clinical and genetic factors associated with nausea and vomiting in cancer patients receiving opioids. Eur. J. Cancer 2011, 47, 1682–1691. [Google Scholar] [CrossRef]
- Dauvilliers, Y.; Tafti, M.; Landolt, H.P. Catechol-O-methyltransferase, dopamine, and sleep-wake regulation. Sleep Med. Rev. 2015, 22, 47–53. [Google Scholar] [CrossRef]
- Bodenmann, S.; Rusterholz, T.; Dürr, R.; Stoll, C.; Bachmann, V.; Geissler, E.; Jaggi-Schwarz, K.; Landolt, H.P. The functional Val158Met polymorphism of COMT predicts interindividual differences in brain α oscillations in young men. J. Neurosci. 2009, 29, 10855–10862. [Google Scholar] [CrossRef]
- Valomon, A.; Holst, S.C.; Bachmann, V.; Viola, A.U.; Schmidt, C.; Zürcher, J.; Berger, W.; Cajochen, C.; Landolt, H.P. Genetic polymorphisms of DAT1 and COMT differentially associate with actigraphy-derived sleep-wake cycles in young adults. Chronobiol. Int. 2014, 31, 705–714. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Demographic Data | ||
|---|---|---|
| Parameters | Characteristics | Value |
| Gender | Male Female | 37% 63% |
| Material Status | Married Unmarried | 75% 25% |
| Mean Age (Years) | 34.95 ± 13.47 | |
| Mean Weight (Kg) | 70.77 ± 11.13 | |
| Mean Height (feet) | 5.45 ± 0.28 | |
| Mean Body Mass Index | 25.12 ± 4.15 | |
| Smoking Status | Yes No | 5% 95% |
| Mean Serum Creatinine | 0.78 ± 0.20 | |
| Mean Urea | 28.32 ± 7.81 | |
| Previous Medication | Yes No | 2% 98% |
| Mean Serum ALT | 38.01 ± 21.32 | |
| Mean Serum AST | 39.03 ± 22.00 | |
| Alcohol consumption | 0% | |
| ASA Status | ASA Status
| 69% 29% 2% |
| Duration of Surgery (Minutes) | 30.82 ± 4.70 | |
| Gene | SNP | Allele Frequency (%) | Genotype/Haplotype | Observed Frequency (%) | Expected Frequency (%) | 95% Confidence Interval | pHWE |
|---|---|---|---|---|---|---|---|
| COMT (G/A) rs4680 | G | 83 (41.5%) | G/G | 27 | 17 | 0.186–0.368 | 0.788 |
| A | 117 (58.5%) | A/G | 29 | 49 | 0.204–0.389 | ||
| A/A | 44 | 34 | 0.341–0.543 | ||||
| Post-Operative Time | COMT (rs4680) | p-Value ** | GG vs. GA *** | GG vs. AA *** | AA vs. GA *** | ||
|---|---|---|---|---|---|---|---|
| GG * (n = 27) | GA * (n = 29) | AA8 (n = 44) | |||||
| Pain Score at Rest | |||||||
| 1 h | 8.59 ± 0.628 | 6.63 ± 1.275 | 5.704 ± 1.090 | <0.001 | <0.001 (0.99, 2.39) | <0.001 (−3.46, −2.17) | 0.001 (−1.7511, −0.496) |
| 3 h | 7.069 ± 1.193 | 5.59 ± 1.474 | 4.50 ± 0.999 | <0.001 | <0.001 (0.54, 2.09) | <0.001 (−3.23, −1.81) | 0.001 (−1.89, −0.504) |
| 6 h | 5.896 ± 1.046 | 4.629 ± 1.42 | 3.863 ± 0.979 | <0.001 | <0.001 (0.356, 1.83) | <0.001 (−2.66, −1.32) | 0.018 (−1.554, −0.236 |
| 12 h | 5.827 ± 0.848 | 4.148 ± 1.262 | 3.091 ± 0.884 | <0.001 | <0.001 (0.806, 2.13) | <0.001 (−3.29, −2.09) | <0.001 (−1.810, −0.629) |
| 24 h | 5.241 ± 1.214 | 3.778 ± 1.502 | 2.500 ± 0.44 | <0.001 | <0.001 (0.212, 1.87) | <0.001 (−3.33,−1.82) | <0.001 (−2.27, −0.795) |
| Pain Score at movement (Head Raising) | |||||||
| 1 h | 8.69 ± 0.761 | 7.11 ± 1.87 | 6.204 ± 1.25 | <0.001 | <0.001 (0.69, 2.15) | <0.001 (−3.13, −1.79) | 0.003 (−1.69, −0.387) |
| 3 h | 7.103 ± 1.52 | 5.33 ± 1.09 | 5.159 ± 0.805 | <0.001 | <0.001 (1.18, 2.58) | <0.001 (−2.74, −1.46) | 0.798 (−0.848, 0.407) |
| 6 h | 6.65 ± 1.11 | 5.00 ± 1.00 | 4.59 ± 0.731 | <0.001 | <0.001 (0.876, 2.11) | <0.001 (−2.69, −1.57) | 0.076 (−1.19, −0.087) |
| 12 h | 6.34 ±0.936 | 4.74 ± 0.98 | 3.818 ± 1.04 | <0.001 | <0.001 (0.89, 2.19) | <0.001 (−3.14, −1.96) | 0.001 (−0.087, −0.43) |
| 24 h | 5.68 ± 0.806 | 4.07 ± 0.729 | 2.863 ± 1.002 | <0.001 | <0.001 (0.79, 1.98) | <0.001 (−3.31, −2.22) | 0.001 (−1.91, −0.845) |
| Nausea Vomiting 30 Minutes after Tramadol | |||||||
|---|---|---|---|---|---|---|---|
| COMT (rs4680) | p Value ** | GG vs. GA ** | GG vs. AA ** | AA vs. GA ** | |||
| GG (27) * | GA (29) * | AA (44) * | |||||
| 1 h post-operatively | |||||||
| No Nausea (n = 48) | 25 (92.6%) | 10 (34.5.%) | 13 (29.5%) | <0.001 | <0.001 | <0.001 | 0.152 |
| Feel Nausea (n = 42) | 2 (7.4%) | 18 (60.1%) | 22 (50%) | ||||
| Vomit (n = 10) | 0 (0%) | 1 (3.4%) | 9 (20.5%) | ||||
| 3 h post-operatively | |||||||
| No Nausea (n = 60) | 26 (96.3%) | 20 (69%) | 14 (31.8%) | <0.001 | 0.027 | <0.001 | 0.03 |
| Feel Nausea (n = 22) | 1 (3.7%) | 7 (24.1%) | 14 (31.8%) | ||||
| Vomit (n = 18) | 0 (0%) | 2 (6.9%) | 16 (36.4%) | ||||
| 6 h post-operatively | |||||||
| No Nausea (n = 68) | 26 (96.3%) | 24 (82.8%) | 18 (40.9%) | <0.001 | 0.134 | <0.001 | 0.002 |
| Feel Nausea (n = 21) | 0 (0%) | 4 (13.8%) | 17 (38.6%) | ||||
| Vomit (n = 11) | 1 (3.7%) | 1 (3.4%) | 9 (20.5%) | ||||
| 12 h post-operatively | |||||||
| No Nausea (n = 92) | 23 (85.2%) | 25 (86.2%) | 23 (52.3%) | 0.026 | - | 0.062 | 0.05 |
| Feel Nausea (n = 7) | 4 (14.8%) | 4 (13.8%) | 20 (4%) | ||||
| Vomit (n = 1) | 0 (0%) | 0 (0%) | 1 (2.3) | ||||
| 24 h post-operatively | |||||||
| No Nausea (n = 93) | 27 (100%) | 28 (100%) | 38 (91%) | 0.062 | 1.00 | 0.076 | 0.232 |
| Feel Nausea (n = 7) | 0 (0%) | 1 (0%) | 6 (9%) | ||||
| Vomit (n = 0) | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| Sedation Level | |||||||
|---|---|---|---|---|---|---|---|
| COMT (rs4680) | p Value ** | GG vs. GA ** | AA vs. GG ** | GA vs. AA ** | |||
| GG (27) * | GA (29) * | AA (44) * | |||||
| 1 h post-operatively | |||||||
| Awake (n = 16) | 13 (48.1%) | 2 (6.9%) | 1 (2.3%) | <0.001 | 0.001 | <0.001 | 0.078 |
| Easily Awakened by Verbal Command (n = 57) | 13 (48.1%) | 21 (72.4%) | 23 (52.3%) | ||||
| Difficulty in staying awake (n = 27) | 1 (3.7%) | 6 (20.7%) | 20 (40.4%) | ||||
| No awakening (n = 0) | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| 3 h post-operatively | |||||||
| Awake (n = 67) | 27 (100%) | 26 (89.6%) | 14 (31.8%) | <0.001 | 0.083 | <0.001 | 0.001 |
| Easily Awakened by Verbal Command (n = 33) | 0 (0%) | 3 (10.4%) | 30 (68.2%) | ||||
| Difficulty in staying awake (n = 0) | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| No awakening (n = 0) | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| 6 h post-operatively | |||||||
| Awake (n = 87) | 27 (100%) | 29 (99%) | 32 (72.7%) | <0.001 | 0.330 | 0.002 | 0.01 |
| Easily Awakened by Verbal Command (n = 13) | 0 (0) | 1 (1%) | 12 (27.3%) | ||||
| 12 h post-operatively | |||||||
| Awake (n = 88) | 27 (100%) | 28 (96.6%) | 33 (75%) | 0.002 | 0.330 | 0.005 | 0.02 |
| Easily Awakened by Verbal Command (n = 12) | 0 (0%) | 1 (3.4%) | 11 (25%) | ||||
| 24 h post-operatively | |||||||
| Awake (n = 99) | 29 (100%) | 27 (100%) | 43 (99%) | 0.273 | Not possible # | 0.522 | 0.224 |
| Easily Awakened by Verbal Command (n = l) | 0 (0%) | 0 (0%) | 1 (1%) | ||||
| Other Side Effect of Tramadol Administration | |||||||
|---|---|---|---|---|---|---|---|
| COMT (rs4680) | p Value ** | GG vs. GA ** | AA vs. GG ** | AA vs. GA ** | |||
| GG (n = 27) * | GA (n = 29) * | AA (n = 44) * | |||||
| 1 h post-operatively | |||||||
| No side effects (n = 70) | 12 (44.4%) | 22 (75.8%) | 36 (81.8%) | 0.008 | 0.034 | 0.003 | 0.326 |
| Dizziness (n = 16) | 9 (33.3%) | 2 (6.9%) | 5 (11.4%) | ||||
| Headache (n = 11) | 5 (18.5%) | 4 (13.8%) | 2 (4.5%) | ||||
| Sweating (n = 2) | 1 (3.7%) | 1 (3.4%) | 0 (0%) | ||||
| Dry Mouth (n = 1) | 0 (0%) | 0 (0%) | 1 (2.3%) | ||||
| 3 h post-operatively | |||||||
| No side effects (n = 78) | 15 (55.5%) | 24 (82.7%) | 39 (88.6%) | 0.001 | 0.02 | 0.001 | 0.424 |
| Dizziness (n = 2) | 0 (0%) | 0 (0%) | 2 (4.5%) | ||||
| Headache (n = 14) | 10 (37%) | 2 (10.3%) | 2 (4.5%) | ||||
| Sweating (n = 2) | 1 (3.7%) | 1 (3.4%) | 0 (0%) | ||||
| Dry Mouth (n = 4) | 1 (3.7%) | 2 (10.3%) | 1 (2.3%) | ||||
| 6 h post-operatively | |||||||
| No side effects (n = 81) | 17 (63%) | 24 (82.7%) | 40 (90.9%) | 0.02 | 0.439 | 0.003 | 0.248 |
| Dizziness (n = 3) | 1 (3.7%) | 0 (0%) | 2 (4.5%) | ||||
| Headache (n = 11) | 7 (25.9%) | 3 (10.3%) | 1 (2.3%) | ||||
| Sweating (n = 2) | 1 (3.7%) | 1 (3.4%) | 0 (0%) | ||||
| Dry Mouth (n = 3) | 1 (3.7%) | 1 (3.4%) | 1 (2.3%) | ||||
| 12 h post-operatively | |||||||
| No side effects (n = 77) | 15 (55.5%) | 22 (75.8%) | 40 (91%) | 0.003 | 0.121 | 0.001 | 0.072 |
| Dizziness (n = 5) | 3 (11.1%) | 0 (0%) | 2 (4.5%) | ||||
| Headache (n = 11) | 7 (25.9%) | 3 (10.3%) | 1 (2.3%) | ||||
| Sweating (n = 2) | 1 (3.7%) | 1 (3.4%) | 0 (0%) | ||||
| Dry Mouth (n = 5) | 1 (3.7%) | 3 (10.3%) | 1 (2.3%) | ||||
| At 24 h post-operatively | |||||||
| No side effects (n = 77) | 14 (51.8%) | 24 (88.8%) | 39 (88.6%) | 0.003 | 0.019 | 0.002 | 0.310 |
| Dizziness (n = 5) | 3 (11.1%) | 0 (0%) | 2 (4.5%) | ||||
| Headache (n = 12) | 8 (29.6%) | 2 (6.8%) | 2 (4.5%) | ||||
| Sweating (n = 3) | 1 (3.7%) | 2 (6.8%) | 0 (0%) | ||||
| Dry Mouth (n = 3) | 1 (3.7%) | 1 (3.4%) | 1 (2.3%) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, A.; Waheed, A.; Afsar, T.; Abusharha, A.; Shafique, H.; Razak, S. Unraveling Catechol-O-Methyltransferase rs4680 SNP’s Role in Patients’ Response to Tramadol and Its Adverse Effects: A Pharmacogenetics Insight into Postoperative Pain Management. J. Clin. Med. 2024, 13, 249. https://doi.org/10.3390/jcm13010249
Khan A, Waheed A, Afsar T, Abusharha A, Shafique H, Razak S. Unraveling Catechol-O-Methyltransferase rs4680 SNP’s Role in Patients’ Response to Tramadol and Its Adverse Effects: A Pharmacogenetics Insight into Postoperative Pain Management. Journal of Clinical Medicine. 2024; 13(1):249. https://doi.org/10.3390/jcm13010249
Chicago/Turabian StyleKhan, Ammara, Akbar Waheed, Tayyaba Afsar, Ali Abusharha, Huma Shafique, and Suhail Razak. 2024. "Unraveling Catechol-O-Methyltransferase rs4680 SNP’s Role in Patients’ Response to Tramadol and Its Adverse Effects: A Pharmacogenetics Insight into Postoperative Pain Management" Journal of Clinical Medicine 13, no. 1: 249. https://doi.org/10.3390/jcm13010249
APA StyleKhan, A., Waheed, A., Afsar, T., Abusharha, A., Shafique, H., & Razak, S. (2024). Unraveling Catechol-O-Methyltransferase rs4680 SNP’s Role in Patients’ Response to Tramadol and Its Adverse Effects: A Pharmacogenetics Insight into Postoperative Pain Management. Journal of Clinical Medicine, 13(1), 249. https://doi.org/10.3390/jcm13010249