
Management and Treatment for Dysphagia in Neurodegenerative Disorders




Abstract
1. Introduction
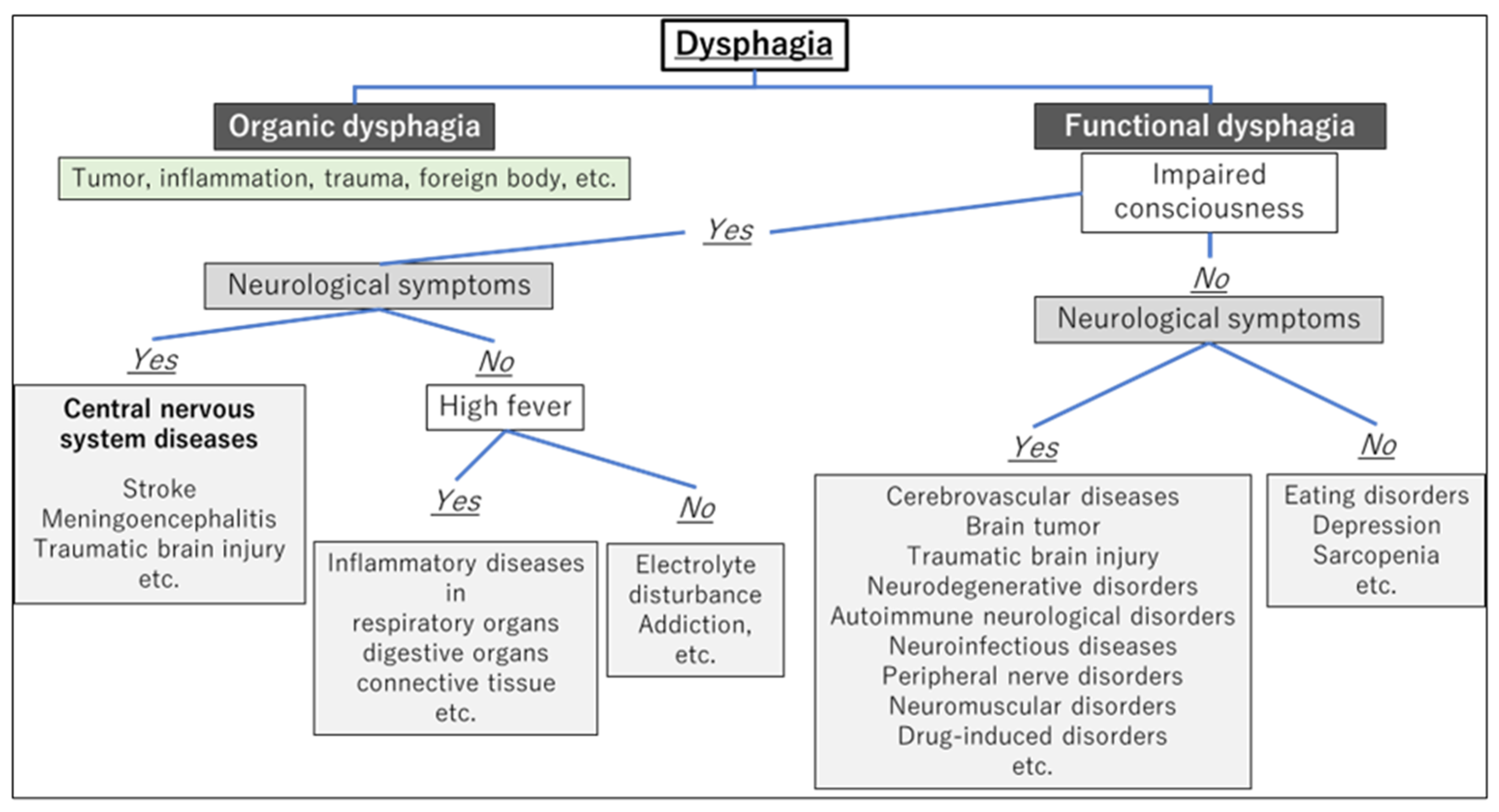
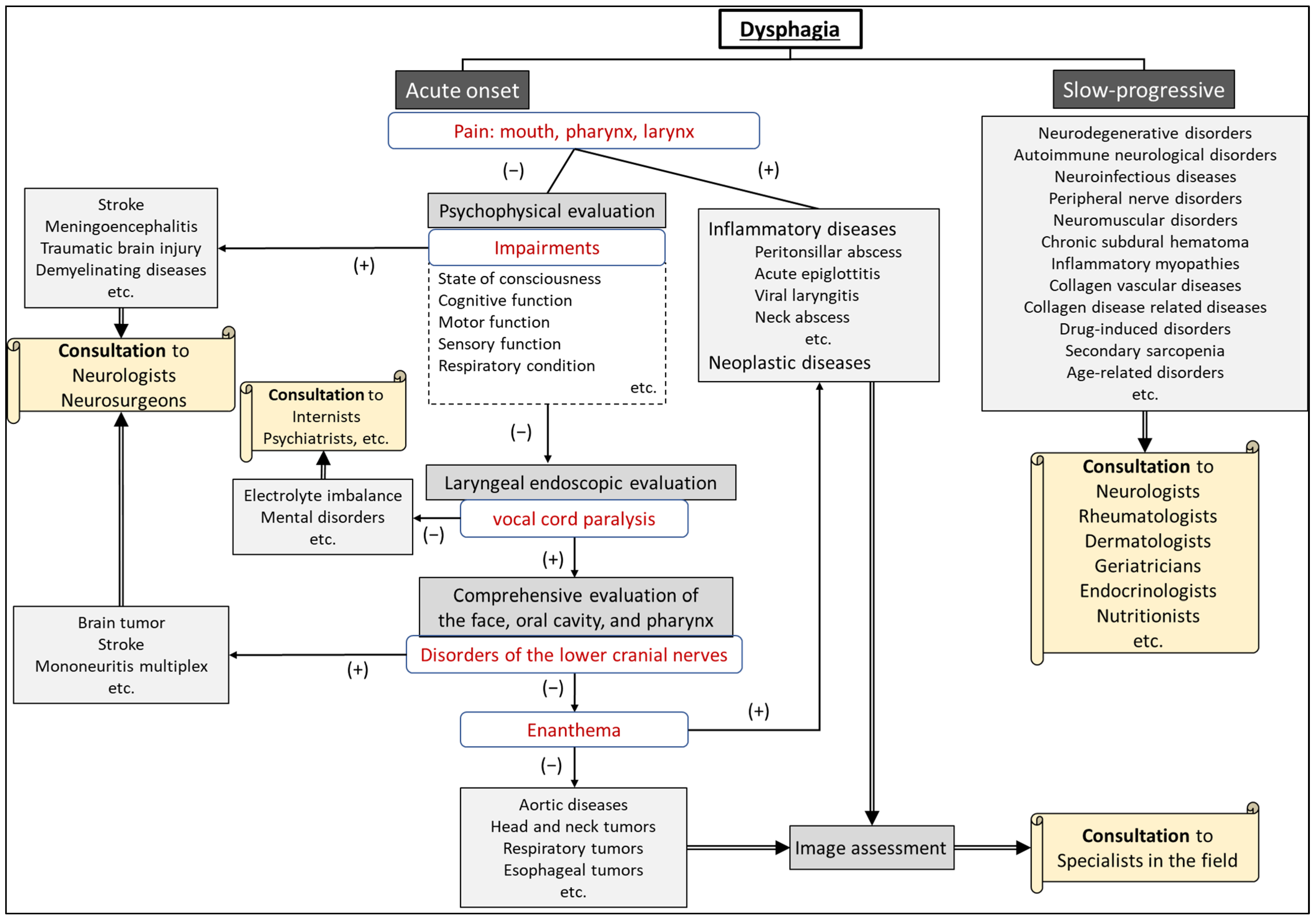
2. The Differentiation of Diseases Causing Dysphagia
3. Neurodegenerative Disorders Causing Dysphagia
3.1. Representative Neurodegenerative Disorders Causing Dysphagia
3.2. Parkinson’s Disease
3.3. Multiple System Atrophy
3.4. Amyotrophic Lateral Sclerosis
3.5. Alzheimer’s Disease
4. The Evaluation of Patients with Suspected Neurodegenerative Disorders
4.1. Patients with Neurodegenerative Disorders among New Outpatient Visits
4.2. Physical Signs and Oro-pharyngo-laryngeal Findings Suggesting Neurodegenerative Disorders
- Weight loss;
- Gait disturbance/stumbling;
- Muscle weakness;
- Tremor;
- Reduced facial expression;
- Cognitive impairment;
- Respiratory dysfunction.
- Dysarthria;
- Speech impairment (hoarseness, low volume);
- Tongue atrophy and limited tongue movement;
- Velopharyngeal insufficiency (during articulation and/or swallowing);
- Vocal fold movement impairment;
- Reduced pharyngeal contraction;
- Decreased pharyngo-laryngeal sensation.
5. The Management of Dysphagia in Neurodegenerative Disorders
5.1. Meal-Time Management
- Modifications of bolus texture (liquid thickness, swallowing diet)
- Modifications of bolus size (the amount of food placed in the mouth at one time)
- Feeding posture
- Compensatory swallowing techniques, such as chin tuck, Supraglottic Swallow, and head rotation (see Section 5.2)
5.2. Swallowing Rehabilitation
- ▪
- Indirect exercises
- Facilitating the swallowing reflex: ice massage [55]
- Cough reflex exercise [63]
- ▪
- Direct exercises
- Multiple swallows [66]
- Alternate swallows [63]
- ▪
- Chin-tuck maneuver [69]
- Supraglottic Swallow [72]
6. Surgical Intervention for Dysphagia
- Tracheostomy
- Swallowing improvement surgeries
- Aspiration prevention surgeries
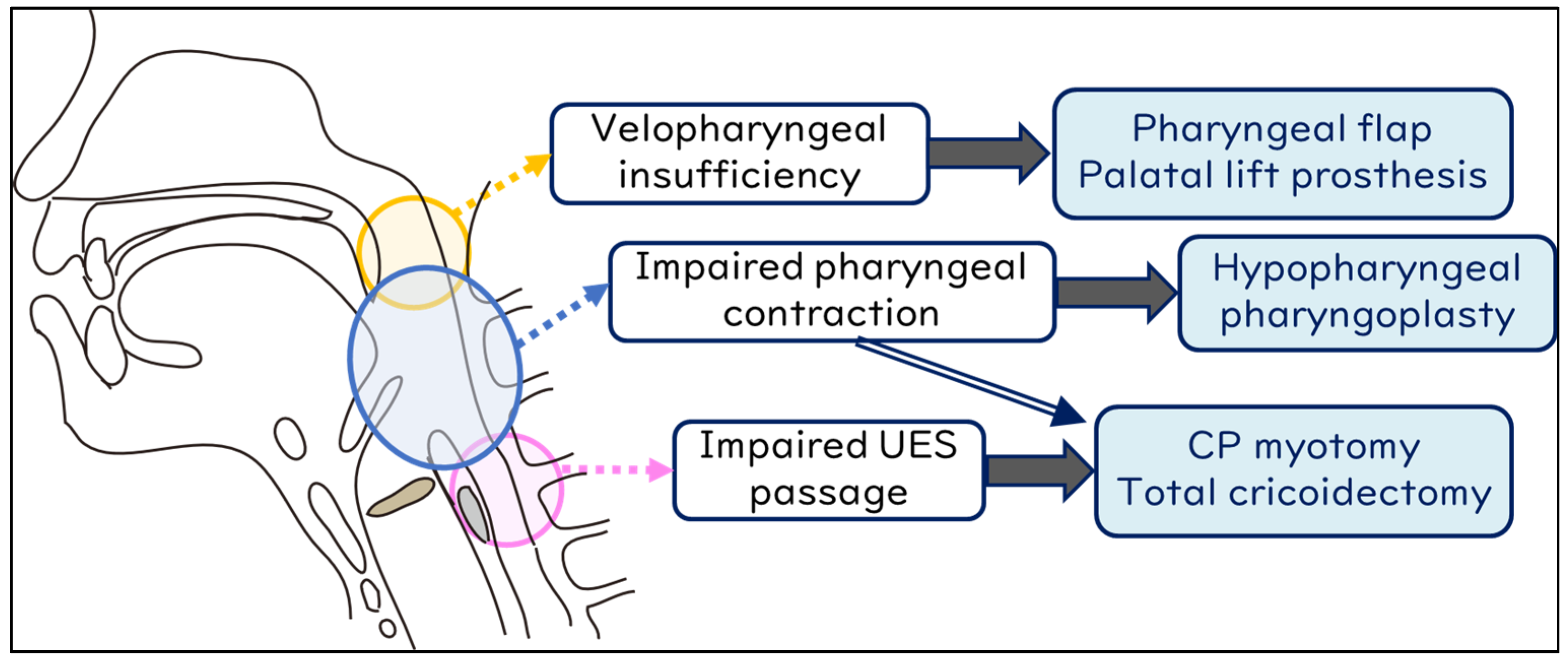
6.1. Swallowing Improvement Surgeries
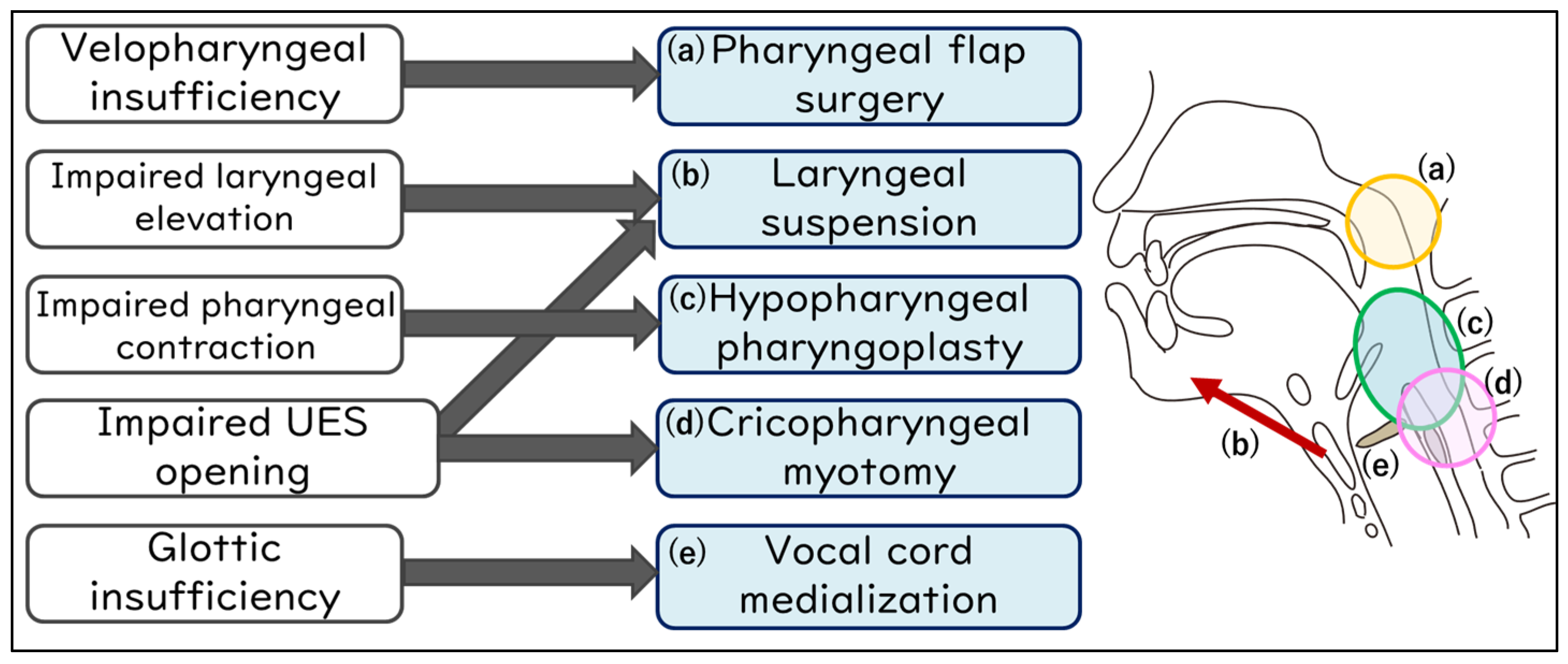
6.2. Surgical Procedure Selection in Swallowing Improvement Surgeries
6.3. Aspiration Prevention Surgeries
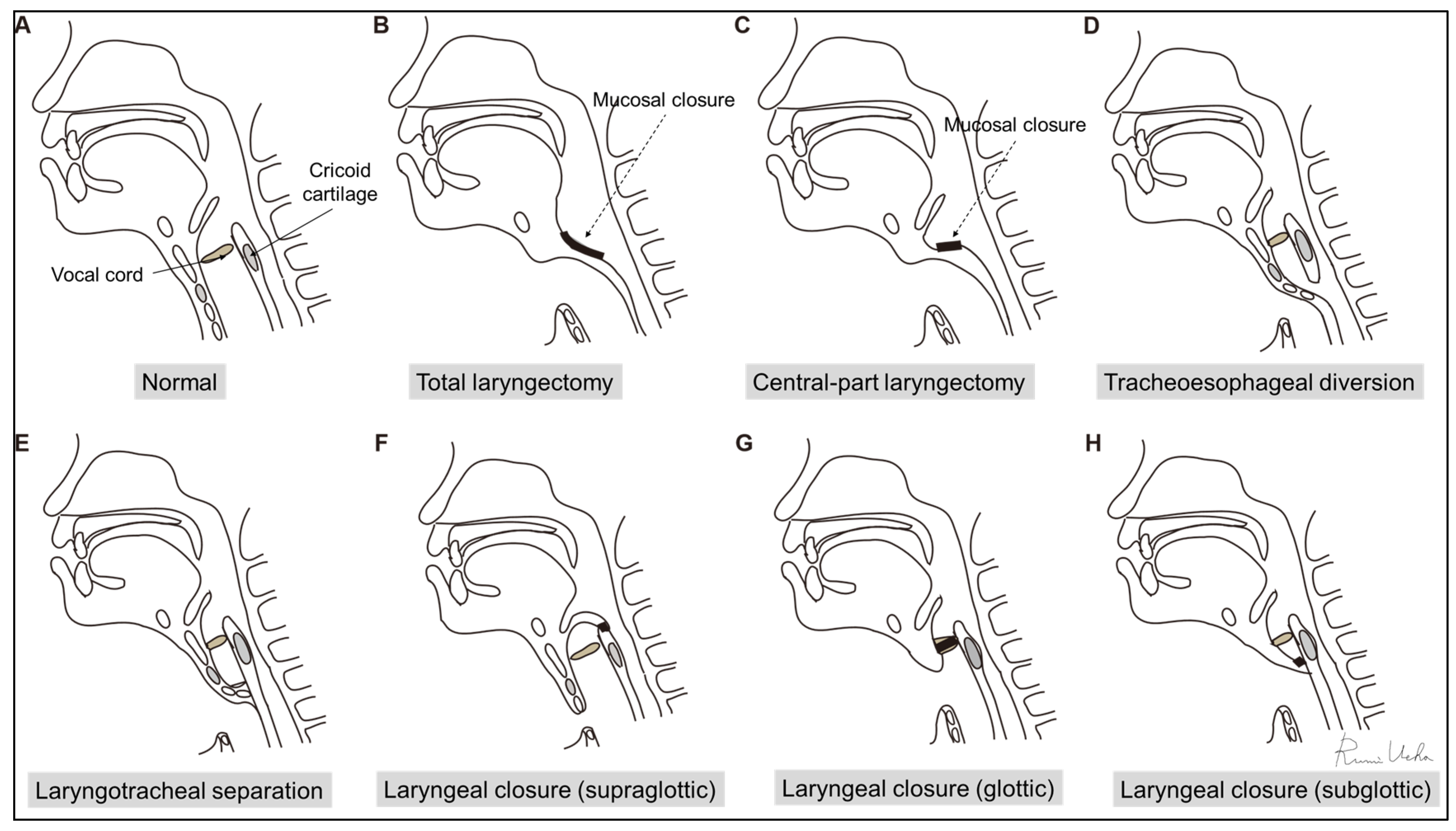
6.4. Surgical Procedure Selection in Aspiration Prevention Surgeries
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matsuo, K.; Palmer, J.B. Anatomy and physiology of feeding and swallowing: Normal and abnormal. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 691–707. [Google Scholar] [CrossRef]
- Palmer, J.B.; Rudin, N.J.; Lara, G.; Crompton, A.W. Coordination of mastication and swallowing. Dysphagia 1992, 7, 187–200. [Google Scholar] [CrossRef]
- Dziewas, R.; Allescher, H.D.; Aroyo, I.; Bartolome, G.; Beilenhoff, U.; Bohlender, J.; Breitbach-Snowdon, H.; Fheodoroff, K.; Glahn, J.; Heppner, H.J.; et al. Diagnosis and treatment of neurogenic dysphagia—S1 guideline of the German Society of Neurology. Neurol. Res. Pract. 2021, 3, 23. [Google Scholar] [CrossRef]
- Willig, T.N.; Paulus, J.; Lacau Saint Guily, J.; Beon, C.; Navarro, J. Swallowing problems in neuromuscular disorders. Arch. Phys. Med. Rehabil. 1994, 75, 1175–1181. [Google Scholar] [CrossRef]
- Wadman, R.I.; Rheenen, W.V.; van der Pol, W.L.; van den Berg, L.H. Major advances in neuromuscular disorders in the past two decades. Lancet Neurol. 2022, 21, 585–587. [Google Scholar] [CrossRef]
- Landfeldt, E. Gene Therapy for Neuromuscular Diseases: Health Economic Challenges and Future Perspectives. J. Neuromuscul. Dis. 2022, 9, 675–688. [Google Scholar] [CrossRef]
- Panebianco, M.; Marchese-Ragona, R.; Masiero, S.; Restivo, D.A. Dysphagia in neurological diseases: A literature review. Neurol. Sci. 2020, 41, 3067–3073. [Google Scholar] [CrossRef]
- Lápez-Liria, R.; Parra-Egeda, J.; Vega-Ramírez, F.A.; Aguilar-Parra, J.M.; Trigueros-Ramos, R.; Morales-Gázquez, M.J.; Rocamora-Pérez, P. Treatment of Dysphagia in Parkinson’s Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4104. [Google Scholar] [CrossRef]
- Lee, J.; Madhavan, A.; Krajewski, E.; Lingenfelter, S. Assessment of dysarthria and dysphagia in patients with amyotrophic lateral sclerosis: Review of the current evidence. Muscle Nerve 2021, 64, 520–531. [Google Scholar] [CrossRef]
- Kim, J.S.; Youn, J.; Suh, M.K.; Kim, T.E.; Chin, J.; Park, S.; Cho, J.W. Cognitive and Motor Aspects of Parkinson’s Disease Associated with Dysphagia. Can. J. Neurol. Sci. 2015, 42, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Kim, G.J.; Ryu, H.; Jung, K.I.; Yoo, W.K.; Ohn, S.H. Pharyngeal Structure and Dysphagia in Patients with Parkinson’s Disease and Related Disorders. Dysphagia 2023. [Google Scholar] [CrossRef]
- Suttrup, I.; Suttrup, J.; Suntrup-Krueger, S.; Siemer, M.L.; Bauer, J.; Hamacher, C.; Oelenberg, S.; Domagk, D.; Dziewas, R.; Warnecke, T. Esophageal dysfunction in different stages of Parkinson’s disease. Neurogastroenterol. Motil. 2017, 29, e12915. [Google Scholar] [CrossRef]
- Labeit, B.; Berkovich, E.; Claus, I.; Roderigo, M.; Schwake, A.L.; Izgelov, D.; Mimrod, D.; Ahring, S.; Oelenberg, S.; Muhle, P.; et al. Dysphagia for medication in Parkinson’s disease. NPJ Parkinsons Dis. 2022, 8, 156. [Google Scholar] [CrossRef]
- Qayyum, A.; Mierzwa, K.; See, M.; Sharma, A.; Montgommery, P.Q. Laser arytenoidectomy for bilateral vocal fold palsy in Parkinson’s disease. J. Laryngol. Otol. 2005, 119, 831–833. [Google Scholar] [CrossRef]
- Lee, D.H.; Lim, S.C.; Lee, J.K. Bilateral vocal cord paralysis in a patient with Parkinson’s disease. B-ENT 2012, 8, 141–142. [Google Scholar]
- Katoh, M.; Ueha, R.; Sato, T.; Sugasawa, S.; Goto, T.; Yamauchi, A.; Yamasoba, T. Choice of Aspiration Prevention Surgery for Patients With Neuromuscular Disorders: Report of Three Cases. Front. Surg. 2019, 6, 66. [Google Scholar] [CrossRef]
- Calandra-Buonaura, G.; Alfonsi, E.; Vignatelli, L.; Benarroch, E.E.; Giannini, G.; Iranzo, A.; Low, P.A.; Martinelli, P.; Provini, F.; Quinn, N.; et al. Dysphagia in multiple system atrophy consensus statement on diagnosis, prognosis and treatment. Parkinsonism Relat. Dis. 2021, 86, 124–132. [Google Scholar] [CrossRef]
- Tsuchiya, K.; Ueha, R.; Suzuki, S.; Goto, T.; Sato, T.; Nito, T.; Yamasoba, T. Heightened risk of early vocal fold motion impairment onset and dysphagia in the parkinsonian variant of multiple system atrophy: A comparative study. Clin. Park. Relat. Disord. 2020, 3, 100037. [Google Scholar] [CrossRef]
- Ueha, R.; Goto, T.; Sato, T.; Nativ-Zeltzer, N.; Shen, S.C.; Nito, T.; Belafsky, P.C.; Yamasoba, T. High Resolution Manofluorographic Study in Patients With Multiple System Atrophy: Possible Early Detection of Upper Esophageal Sphincter and Proximal Esophageal Abnormality. Front. Med. 2018, 5, 286. [Google Scholar] [CrossRef] [PubMed]
- Ueha, R.; Sato, T.; Goto, T.; Yamauchi, A.; Nativ-Zeltzer, N.; Mitsui, J.; Belafsky, P.C.; Yamasoba, T. Esophageal Dysmotility is Common in Patients With Multiple System Atrophy. Laryngoscope 2021, 131, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Gandor, F.; Vogel, A.; Claus, I.; Ahring, S.; Gruber, D.; Heinze, H.J.; Dziewas, R.; Ebersbach, G.; Warnecke, T. Laryngeal Movement Disorders in Multiple System Atrophy: A Diagnostic Biomarker? Mov. Disord. 2020, 35, 2174–2183. [Google Scholar] [CrossRef]
- Ueha, R.; Maeda, E.; Ino, K.; Shimizu, T.; Sato, T.; Goto, T.; Yamasoba, T. Sleep-Induced Glottis Closure in Multiple System Atrophy Evaluated by Four-Dimensional Computed Tomography. Front. Med. 2020, 7, 132. [Google Scholar] [CrossRef]
- Ueha, R.; Nito, T.; Sakamoto, T.; Yamauchi, A.; Tsunoda, K.; Yamasoba, T. Post-operative swallowing in multiple system atrophy. Eur. J. Neurol. 2016, 23, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Hardiman, O.; Al-Chalabi, A.; Chio, A.; Corr, E.M.; Logroscino, G.; Robberecht, W.; Shaw, P.J.; Simmons, Z.; van den Berg, L.H. Amyotrophic lateral sclerosis. Nat. Rev. Dis. Primers 2017, 3, 17071. [Google Scholar] [CrossRef]
- Ruoppolo, G.; Schettino, I.; Frasca, V.; Giacomelli, E.; Prosperini, L.; Cambieri, C.; Roma, R.; Greco, A.; Mancini, P.; De Vincentiis, M.; et al. Dysphagia in amyotrophic lateral sclerosis: Prevalence and clinical findings. Acta Neurol. Scand. 2013, 128, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Rugaitiene, M.; Damuleviciene, G.; Lesauskaite, V.; Uloziene, I. Oropharyngeal Dysphagia as the Main Expression of Amyotrophic Lateral Sclerosis. Medicina 2022, 58, 647. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, H.; Nakayama, H.; Hori, K.; Nishizawa, M.; Inoue, M.; Shimohata, T. Esophageal Involvement in Multiple System Atrophy. Dysphagia 2015, 30, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Onesti, E.; Schettino, I.; Gori, M.C.; Frasca, V.; Ceccanti, M.; Cambieri, C.; Ruoppolo, G.; Inghilleri, M. Dysphagia in amyotrophic lateral sclerosis: Impact on Patient Behavior, Diet adaptation, and riluzole Management. Front. Neurol. 2017, 8, 94. [Google Scholar] [CrossRef]
- Soga, T.; Suzuki, N.; Kato, K.; Kawamoto-Hirano, A.; Kawauchi, Y.; Izumi, R.; Toyoshima, M.; Mitsuzawa, S.; Shijo, T.; Ikeda, K.; et al. Long-term outcomes after surgery to prevent aspiration for patients with amyotrophic lateral sclerosis. BMC Neurol. 2022, 22, 94. [Google Scholar] [CrossRef]
- Kaneoka, A.; Ueha, R.; Nagatomo, M.; Matsunaga, A.; Umezaki, S.; Inokuchi, H.; Ogata, T. Esophageal Speech for a Patient with Amyotrophic Lateral Sclerosis Who Underwent a Central-part Laryngectomy to Prevent Aspiration: A Case Report. Prog. Rehabil. Med. 2022, 7, 20220064. [Google Scholar] [CrossRef]
- Priefer, B.A.; Robbins, J. Eating changes in mild-stage Alzheimer’s disease: A pilot study. Dysphagia 1997, 12, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Mira, A.; Gonçalves, R.; Rodrigues, I.T. Dysphagia in Alzheimer’s disease: A systematic review. Dement. Neuropsychol. 2022, 16, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Guener, M.; Bas, A.O.; Ceylan, S.; Kahyaoglu, Z.; Coeteli, S.; Uensal, P.; Cavusoglu, C.; Oezsuerekci, C.; Dogu, B.B.; Cankurtaran, M.; et al. Dysphagia is closely related to frailty in mild-to-moderate Alzheimer’s disease. BMC Geriatr. 2023, 23, 304. [Google Scholar] [CrossRef] [PubMed]
- Seçil, Y.; Arıcı, Ş.; İncesu, T.K.; Gürgör, N.; Beckmann, Y.; Ertekin, C. Dysphagia in Alzheimer’s disease. Neurophysiol. Clin. 2016, 46, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.A.; Kindell, J.; Baldwin, R.C.; Waterman, D.; Makin, A.J. Swallowing problems and dementia in acute hospital settings: Practical guidance for the management of dysphagia. Clin. Med. 2009, 9, 544–548. [Google Scholar] [CrossRef]
- Boccardi, V.; Ruggiero, C.; Patriti, A.; Marano, L. Diagnostic Assessment and Management of Dysphagia in Patients with Alzheimer’s Disease. J. Alzheimers Dis. 2016, 50, 947–955. [Google Scholar] [CrossRef]
- Vásquez-Correa, J.C.; Orozco-Arroyave, J.R.; Bocklet, T.; Nöth, E. Towards an automatic evaluation of the dysarthria level of patients with Parkinson’s disease. J. Commun. Disord. 2018, 76, 21–36. [Google Scholar] [CrossRef]
- Erriu, M.; Pili, F.M.; Cadoni, S.; Garau, V. Diagnosis of Lingual Atrophic Conditions: Associations with Local and Systemic Factors. A Descriptive Review. Open Dent. J. 2016, 10, 619–635. [Google Scholar] [CrossRef]
- Kaindlstorfer, C.; Granata, R.; Wenning, G.K. Tremor in Multiple System Atrophy—A review. Tremor Other Hyperkinet Mov. 2013, 3, 1–20. [Google Scholar] [CrossRef]
- Fabbri, M.; Abreu, L.; Santos, T.; Ferreira, J.J. Resting and Reemergent Tongue Tremor as Presenting Symptoms of Parkinson’s Disease. Mov. Disord. Clin. Pract. 2017, 4, 273–274. [Google Scholar] [CrossRef]
- Yaguchi, H.; Sakuta, K.; Mukai, T.; Miyagawa, S. Fiberoptic laryngoscopic neurological examination of amyotrophic lateral sclerosis patients with bulbar symptoms. J. Neurol. Sci. 2022, 440, 120325. [Google Scholar] [CrossRef] [PubMed]
- Glade, R.S.; Deal, R. Diagnosis and Management of Velopharyngeal Dysfunction. Oral. Maxillofac. Surg. Clin. N. Am. 2016, 28, 181–188. [Google Scholar] [CrossRef]
- Van der Graaff, M.M.; Grolman, W.; Westermann, E.J.; Boogaardt, H.C.; Koelman, H.; van der Kooi, A.J.; Tijssen, M.A.; de Visser, M. Vocal Cord Dysfunction in Amyotrophic Lateral Sclerosis. Arch. Neurol. 2009, 66, 1329–1333. [Google Scholar] [CrossRef]
- Bahk, J.; Yang, W.D.; Fishman, J. Bilateral vocal cord paralysis in Miller Fisher syndrome/Guillain-Barre overlap syndrome and a review of previous case series. BMJ Case Rep. 2021, 14, e240386. [Google Scholar] [CrossRef]
- Logemann, J.A. Approaches to management of disordered swallowing. Baillieres Clin. Gastroenterol. 1991, 5, 269–280. [Google Scholar] [CrossRef]
- Gandhi, P.; Peladeau-Pigeon, M.; Simmons, M.; Steele, C.M. Exploring the Efficacy of the Effortful Swallow Maneuver for Improving Swallowing in People With Parkinson Disease-A Pilot Study. Arch. Rehabil. Res. Clin. Transl. 2023, 5, 100276. [Google Scholar] [CrossRef]
- Cosentino, G.; Todisco, M.; Giudice, C.; Tassorelli, C.; Alfonsi, E. Assessment and treatment of neurogenic dysphagia in stroke and Parkinson’s disease. Curr. Opin. Neurol. 2022, 35, 741–752. [Google Scholar] [CrossRef]
- Brent, J.R.; Franz, C.K.; Coleman, J.M., 3rd; Ajroud-Driss, S. ALS: Management Problems. Neurol. Clin. 2020, 38, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Masuda, H.; Ueha, R.; Sato, T.; Goto, T.; Koyama, M.; Yamauchi, A.; Kaneoka, A.; Suzuki, S.; Yamasoba, T. Risk Factors for Aspiration Pneumonia After Receiving Liquid-Thickening Recommendations. Otolaryngol. Head Neck Surg. 2022, 167, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Cheng, I.; Hamad, A.; Sasegbon, A.; Hamdy, S. Advances in the Treatment of Dysphagia in Neurological Disorders: A Review of Current Evidence and Future Considerations. Neuropsychiatr. Dis. Treat. 2022, 18, 2251–2263. [Google Scholar] [CrossRef]
- Hoffman, M.R.; Ciucci, M.R.; Mielens, J.D.; Jiang, J.J.; McCulloch, T.M. Pharyngeal swallow adaptations to bolus volume measured with high-resolution manometry. Laryngoscope 2010, 120, 2367–2373. [Google Scholar] [CrossRef]
- Kao, T.H.; Perry, B.J. The Current State and Future Directions of Swallowing Care in Amyotrophic Lateral Sclerosis. Curr. Phys. Med. Rehabil. Rep. 2023, 11, 199–211. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Zafar, H.; Al-Eisa, E.S.; Iqbal, Z.A. Effect of posture on swallowing. Afr. Health Sci. 2017, 17, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, M.; Nagakawa, K.; Tanaka, R.; Yamawaki, K.; Mori, T.; Hiraoka, A.; Higa, C.; Nishikawa, Y.; Yoshida, M.; Tsuga, K. Improper sitting posture while eating adversely affects maximum tongue pressure. J. Dent. Sci. 2021, 16, 467–473. [Google Scholar] [CrossRef]
- Nakamura, T.; Fujishima, I. Usefulness of ice massage in triggering the swallow reflex. J. Stroke Cerebrovasc. Dis. 2013, 22, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Burkhead, L.M.; Sapienza, C.M.; Rosenbek, J.C. Strength-training exercise in dysphagia rehabilitation: Principles, procedures, and directions for future research. Dysphagia 2007, 22, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Groher, M.E.; Crary, M.A.; Mann, G.C.; Akagawa, Y. Comparison of surface electromyographic (sEMG) activity of submental muscles between the head lift and tongue press exercises as a therapeutic exercise for pharyngeal dysphagia. Gerodontology 2007, 24, 111–116. [Google Scholar] [CrossRef]
- Sze, W.P.; Yoon, W.L.; Escoffier, N.; Rickard Liow, S.J. Evaluating the Training Effects of Two Swallowing Rehabilitation Therapies Using Surface Electromyography—Chin Tuck Against Resistance (CTAR) Exercise and the Shaker Exercise. Dysphagia 2016, 31, 195–205. [Google Scholar] [CrossRef]
- Pitts, T.; Bolser, D.; Rosenbek, J.; Troche, M.; Okun, M.S.; Sapienza, C. Impact of expiratory muscle strength training on voluntary cough and swallow function in Parkinson disease. Chest 2009, 135, 1301–1308. [Google Scholar] [CrossRef]
- Reyes, A.; Ziman, M.; Nosaka, K. Respiratory muscle training for respiratory deficits in neurodegenerative disorders: A systematic review. Chest 2013, 143, 1386–1394. [Google Scholar] [CrossRef]
- Heijnen, B.J.; Speyer, R.; Baijens, L.W.J.; Bogaardt, H.C.A. Neuromuscular electrical stimulation versus traditional therapy in patients with Parkinson’s disease and oropharyngeal dysphagia: Effects on quality of life. Dysphagia 2012, 27, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Schindler, A.; Pizzorni, N.; Cereda, E.; Cosentino, G.; Avenali, M.; Montomoli, C.; Abbruzzese, G.; Antonini, A.; Barbiera, F.; Benazzo, M.; et al. Consensus on the treatment of dysphagia in Parkinson’s disease. J. Neurol. Sci. 2021, 430, 120008. [Google Scholar] [CrossRef]
- Balou, M.; Herzberg, E.G.; Kamelhar, D.; Molfenter, S.M. An intensive swallowing exercise protocol for improving swallowing physiology in older adults with radiographically confirmed dysphagia. Clin. Interv. Aging 2019, 14, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Lin, C.Y.; Chen, C.L.; Chen, K.T.; Lee, C.; Yu, Y.H.; Shih, C.Y. Long-Term Effectiveness of Physical Exercise-Based Swallowing Interventions for Older Adults with Dementia in a Day-Care Center. Healthcare 2023, 11, 1262. [Google Scholar] [CrossRef]
- Bahia, M.M.; Lowell, S.Y. A Systematic Review of the Physiological Effects of the Effortful Swallow Maneuver in Adults With Normal and Disordered Swallowing. Am. J. Speech Lang. Pathol. 2020, 29, 1655–1673. [Google Scholar] [CrossRef]
- Drulia, T.C.; Ludlow, C.L. Relative Efficacy of Swallowing versus Non-swallowing Tasks in Dysphagia Rehabilitation: Current Evidence and Future Directions. Curr. Phys. Med. Rehabil. Rep. 2013, 1, 242–256. [Google Scholar] [CrossRef]
- Kunieda, K.; Sugiyama, J.; Nomoto, A.; Ohno, T.; Shigematsu, T.; Fujishima, I. Compensatory swallowing methods in a patient with dysphagia due to lateral medullary syndrome-vacuum and prolonged swallowing: A case report. Medicine 2022, 101, e28524. [Google Scholar] [CrossRef]
- Huckabee, M.L.; Flynn, R.; Mills, M. Expanding Rehabilitation Options for Dysphagia: Skill-Based Swallowing Training. Dysphagia 2023, 38, 756–767. [Google Scholar] [CrossRef]
- Saconato, M.; Chiari, B.M.; Lederman, H.M.; Gonçalves, M.I. Effectiveness of Chin-tuck Maneuver to Facilitate Swallowing in Neurologic Dysphagia. Int. Arch. Otorhinolaryngol. 2016, 20, 13–17. [Google Scholar] [CrossRef]
- Logemann, J.A.; Kahrilas, P.J.; Kobara, M.; Vakil, N.B. The Benefit of Head Rotation on Pharyngoesophageal Dysphagia. Arch. Phys. Med. Rehabil. 1989, 70, 767–771. [Google Scholar]
- Seo, M.; Park, J.W. Head rotation as an effective compensatory technique for dysphagia caused by unilateral cervical osteophytes. J. Int. Med. Res. 2022, 50, 1–9. [Google Scholar] [CrossRef]
- Chaudhuri, G.; Hildner, C.D.; Brady, S.; Hutchins, B.; Aliga, N.; Abadilla, E. Cardiovascular effects of the supraglottic and super-supraglottic swallowing maneuvers in stroke patients with dysphagia. Dysphagia 2002, 17, 19–23. [Google Scholar] [CrossRef]
- Shin, T.; Tsuda, K.; Takagi, S. Surgical treatment for dysphagia of neuromuscular origin. Folia Phoniatr. Logop. 1999, 51, 213–219. [Google Scholar] [CrossRef]
- Ueha, R.; Magdayao, R.B.; Koyama, M.; Sato, T.; Goto, T.; Yamasoba, T. Aspiration prevention surgeries: A review. Respir. Res. 2023, 24, 43, Erratum in Respir. Res. 2023, 24, 123. [Google Scholar] [CrossRef]
- Ito, H.; Nagao, A.; Maeda, S.; Nakahira, M.; Hyodo, M. Clinical Significance of Surgical Intervention to Restore Swallowing Function for Sustained Severe Dysphagia. J. Clin. Med. 2023, 12, 5555. [Google Scholar] [CrossRef]
- Buchholz, D.W. Cricopharyngeal Myotomy May Be Effective Treatment for Selected Patients with Neurogenic Oropharyngeal Dysphagia. Dysphagia 1995, 10, 255–258. [Google Scholar] [CrossRef]
- Damati, M.T.; Saadah, M.A.; Al-Natour, S.M.; Nazzal, M.M.; Alhaj Ali, M.A.; Inshasi, J.S. Cricopharyngeal myotomy in neurogenic oropharyngeal dysphagia. Neurosciences 2000, 5, 105–109. [Google Scholar]
- Chitose, S.; Sato, K.; Fukahori, M.; Kurita, T.; Sato, K.; Sato, F.; Umeno, H. Lateral pharyngeal flap with a double pedicle for repair of unilateral velopharyngeal insufficiency. Auris Nasus Larynx 2020, 47, 245–249. [Google Scholar] [CrossRef]
- Kos, M.P.; David, E.F.L.; Aalders, I.J.; Smit, C.F.; Mahieu, H.F. Long-term results of laryngeal suspension and upper esophageal sphincter myotomy as treatment for life-threatening aspiration. Ann. Otol. Rhinol. Laryngol. 2008, 117, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Fayoux, P.; Bonne, N.X.; Hosana, G. Hypopharyngeal Pharyngoplasty in the Treatment of Severe Aspiration Following Skull Base Tumor Removal. Arch. Otolaryngol. 2011, 137, 60–64. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Modi, V.K. Vocal fold injection medialization laryngoplasty. Pediatr. Airw. Surg. 2012, 73, 90–94. [Google Scholar] [CrossRef]
- Cates, D.J.; Venkatesan, N.N.; Strong, B.; Kuhn, M.A.; Belafsky, P.C. Effect of Vocal Fold Medialization on Dysphagia in Patients with Unilateral Vocal Fold Immobility. Otolaryngol. Head Neck Surg. 2016, 155, 454–457. [Google Scholar] [CrossRef] [PubMed]
- Koyama, M.S.; Ueha, R.; Goto, T.; Sato, T.; Tachibana, A.; Mizumoto, Y.; Nito, T.; Yamasoba, T. Aspiration Prevention Surgery under Local Anesthesia for Palliative Care in Patients with Head and Neck Cancer: A Report of Two Cases. ORL J. Oto-Rhino-Larynhol. 2021, 83, 52–58. [Google Scholar] [CrossRef]
- Koyama, M.; Ueha, R.; Sato, T.; Goto, T.; Yamauchi, A.; Kaneoka, A.; Suzuki, S.; Nito, T.; Yamasoba, T. Aspiration Prevention Surgery: Clinical Factors Associated With Improvements in Oral Status Intake and Suction Frequency. Otolaryngol. Head Neck Surg. 2023, 168, 1146–1155. [Google Scholar] [CrossRef]
- Yokoi, S.; Nishio, N.; Maruo, T.; Hiramatsu, M.; Mukoyama, N.; Tsuzuki, H.; Wada, A.; Atsuta, N.; Ito, D.; Tsuboi, T.; et al. Safety and Clinical Benefits of Laryngeal Closure in Patients with Amyotrophic Lateral Sclerosis. Dysphagia 2023, 38, 211–219. [Google Scholar] [CrossRef]
- Mizuno, K.; Takeuchi, M.; Kanazawa, Y.; Kishimoto, Y.; Suehiro, A.; Iwanaga, K.; Kawakami, K.; Omori, K. Outcomes of Aspiration Prevention Surgery: A Retrospective Cohort Study Using a Japanese Claims Database. Dysphagia 2022, 37, 1532–1541. [Google Scholar] [CrossRef] [PubMed]
- Japanese Society of Neurology. Amyotrophic Lateral Sclerosis, Clinical Practice Guideline 2023; Nankodo Co., Ltd.: Tokyo, Japan, 2023. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Aspiration Prevention Surgeries | |
|---|---|
| Surgeries to remove the larynx | Total laryngectomy |
| Central-part laryngectomy | |
| Surgeries to change the tracheal structure | Tracheoesophageal diversion |
| Laryngotracheal Separation | |
| Tracheal flap method | |
| Surgeries to close the larynx | Supraglottic laryngeal closure |
| Epiglottic flap | |
| Vertical Laryngoplasty | |
| Transoral supraglottic closure | |
| Glottic laryngeal closure | |
| Subglottic laryngeal closure | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ueha, R.; Cotaoco, C.; Kondo, K.; Yamasoba, T. Management and Treatment for Dysphagia in Neurodegenerative Disorders. J. Clin. Med. 2024, 13, 156. https://doi.org/10.3390/jcm13010156
Ueha R, Cotaoco C, Kondo K, Yamasoba T. Management and Treatment for Dysphagia in Neurodegenerative Disorders. Journal of Clinical Medicine. 2024; 13(1):156. https://doi.org/10.3390/jcm13010156
Chicago/Turabian StyleUeha, Rumi, Carmel Cotaoco, Kenji Kondo, and Tatsuya Yamasoba. 2024. "Management and Treatment for Dysphagia in Neurodegenerative Disorders" Journal of Clinical Medicine 13, no. 1: 156. https://doi.org/10.3390/jcm13010156
APA StyleUeha, R., Cotaoco, C., Kondo, K., & Yamasoba, T. (2024). Management and Treatment for Dysphagia in Neurodegenerative Disorders. Journal of Clinical Medicine, 13(1), 156. https://doi.org/10.3390/jcm13010156