
Outcomes of Isolated Biceps Tenodesis/Tenotomy or Partial Rotator Cuff Repair Associated with Biceps Tenodesis/Tenotomy for Massive Irreparable Tears: A Systematic Review

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
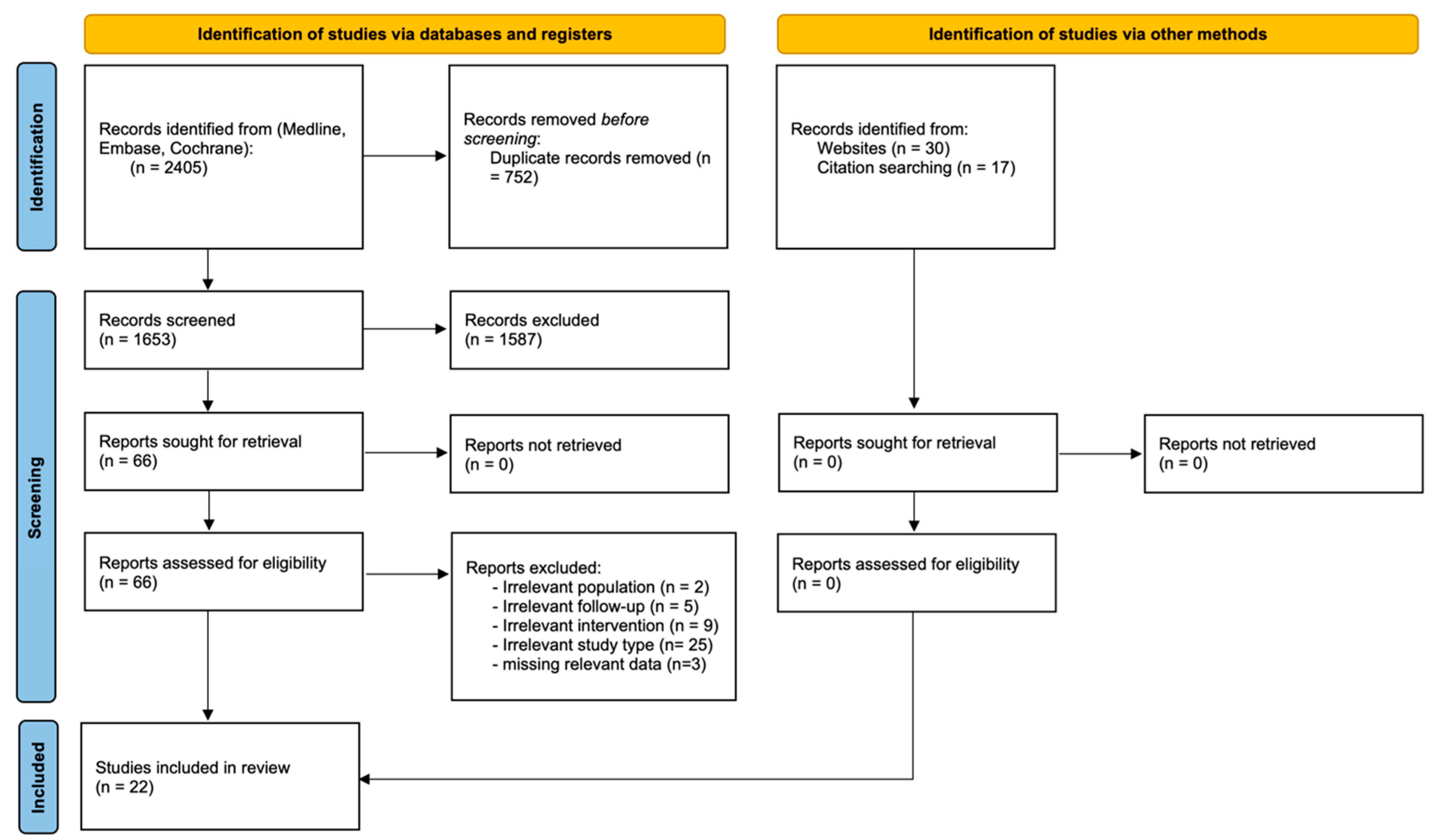
2.1. Search Strategy
2.2. Selection of Studies
2.3. Study Quality Assessment
Study
2.4. Extraction and Review of the Data
2.5. Statistical Analyses
3. Results
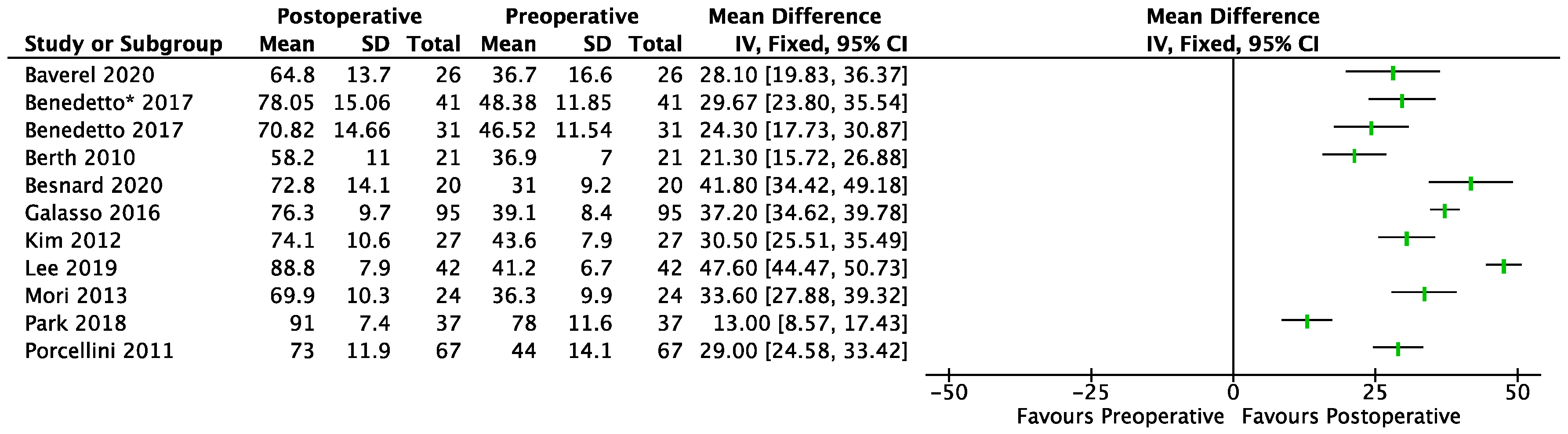
3.1. Functional Evaluation
PCR-BT
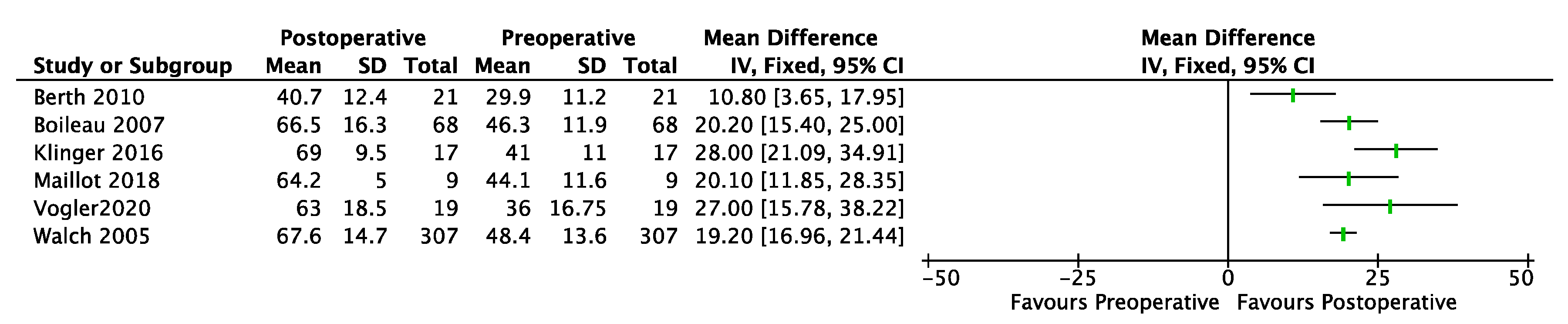
3.2. BT
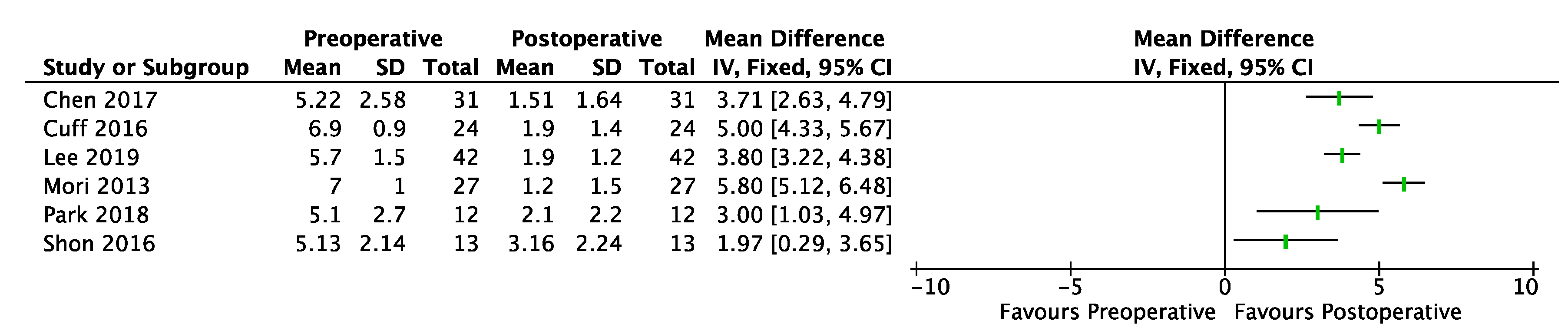
3.3. Pain (VAS)
3.4. Shoulder Motion (Forward Flexion, External Rotation, Abduction)
3.5. Acromiohumeral Distance (AHD)
3.6. Complications
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Conflicts of Interest
References
- Novi, M.; Kumar, A.; Paladini, P.; Porcellini, G.; Merolla, G. Irreparable rotator cuff tears: Challenges and solutions. Orthop. Res. Rev. Vol. 2018, 10, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Nové-Josserand, L.; Edwards, T.B.; O’Connor, D.P.; Walch, G. The Acromiohumeral and Coracohumeral Intervals Are Abnormal in Rotator Cuff Tears with Muscular Fatty Degeneration. Clin. Orthop. NA 2005, 433, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Cofield, R.H. Subscapular muscle transposition for repair of chronic rotator cuff tears. Surg. Gynecol. Obstet. 1982, 154, 667–672. [Google Scholar] [PubMed]
- Gerber, C.; Fuchs, B.; Hodler, J. The results of repair of massive tears of the rotator cuff. J. Bone Jt. Surg. Am. 2000, 82, 505–515. [Google Scholar] [CrossRef]
- Shepet, K.H.; Liechti, D.J.; Kuhn, J.E. Nonoperative Treatment of Chronic, Massive Irreparable Rotator Cuff Tears. J. Shoulder Elb. Surg. 2020, 30, 1431–1444. [Google Scholar] [CrossRef]
- Collin, P.; Matsumura, N.; Lädermann, A.; Denard, P.J.; Walch, G. Relationship between massive chronic rotator cuff tear pattern and loss of active shoulder range of motion. J. Shoulder Elb. Surg. 2014, 23, 1195–1202. [Google Scholar] [CrossRef]
- Takayama, K.; Yamada, S.; Kobori, Y. Clinical outcomes and temporal changes in the range of motion following superior capsular reconstruction for irreparable rotator cuff tears: Comparison based on the Hamada classification, presence or absence of shoulder pseudoparalysis, and status of the subscapularis tendon. J. Shoulder Elb. Surg. 2021, 30, e659–e675. [Google Scholar]
- Deranlot, J.; Herisson, O.; Nourissat, G.; Zbili, D.; Werthel, J.D.; Vigan, M.; Bruchou, F. Arthroscopic Subacromial Spacer Implantation in Patients With Massive Irreparable Rotator Cuff Tears: Clinical and Radiographic Results of 39 Retrospectives Cases. Arthrosc. J. Arthrosc. Relat. Surg. 2017, 33, 1639–1644. [Google Scholar] [CrossRef]
- Burnier, M.; Elhassan, B.T.; Sanchez-Sotelo, J. Surgical Management of Irreparable Rotator Cuff Tears: What Works, What Does Not, and What Is Coming. J. Bone Jt. Surg. 2019, 101, 1603–1612. [Google Scholar] [CrossRef]
- Ahrens, P.M.; Boileau, P. The long head of biceps and associated tendinopathy. J. Bone Joint. Surg. Br. 2007, 89, 1001–1009. [Google Scholar] [CrossRef]
- Boileau, P.; McClelland, W.B.; Rumian, A.P. Massive irreparable rotator cuff tears: How to rebalance the cuff-deficient shoulder. Instr. Course Lect 2014, 63, 71–83. [Google Scholar] [PubMed]
- Burkhart, S.S.; Nottage, W.M.; Ogilvie-Harris, D.J.; Kohn, H.S.; Pachelli, A. Partial repair of irreparable rotator cuff tears. Arthrosc. J. Arthrosc. Relat. Surg. 1994, 10, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Mazzocca, A.D.; Bollier, M.; Fehsenfeld, D.; Romeo, A.; Stephens, K.; Solovyoya, O.; Obopilwe, E.; Ciminiello, A.; Nowak, M.D.; Arciero, R. Biomechanical Evaluation of Margin Convergence. Arthrosc. J. Arthrosc. Relat. Surg. 2011, 27, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Carver, T.J.; Kraeutler, M.J.; Smith, J.R.; Bravman, J.T.; McCarty, E.C. Nonarthroplasty Surgical Treatment Options for Massive, Irreparable Rotator Cuff Tears. Orthop J Sports Med 2018, 6, 232596711880538. [Google Scholar] [CrossRef]
- Berth, A.; Neumann, W.; Awiszus, F.; Pap, G. Massive rotator cuff tears: Functional outcome after debridement or arthroscopic partial repair. J. Orthop Traumatol. 2010, 11, 13–20. [Google Scholar] [CrossRef]
- Franceschi, F.; Papalia, R.; Vasta, S.; Leonardi, F.; Maffulli, N.; Denaro, V. Surgical management of irreparable rotator cuff tears. Knee Surg Sports. Traumatol. Arthrosc. 2015, 23, 494–501. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. Lond. Engl. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies ( MINORS ): Development and validation of a new instrument: Methodological index for non-randomized studies. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Kanto, K.; Lähdeoja, T.; Paavola, M.; Aronen, P.; Järvinen, T.L.N.; Jokihaara, J.; Ardern, C.L.; Karjalainen, T.V.; Taimela, S. Minimal important difference and patient acceptable symptom state for pain, Constant-Murley score and Simple Shoulder Test in patients with subacromial pain syndrome. BMC Med. Res. Methodol. 2021, 21, 45. [Google Scholar] [CrossRef]
- Kukkonen, J.; Kauko, T.; Vahlberg, T.; Joukainen, A.; Äärimaa, V. Investigating minimal clinically important difference for Constant score in patients undergoing rotator cuff surgery. J. Shoulder Elb. Surg. 2013, 22, 1650–1655. [Google Scholar] [CrossRef]
- Malavolta, E.A.; Yamamoto, G.J.; Bussius, D.T.; Assunção, J.H.; Andrade-Silva, F.B.; Gracitelli, M.E.C.; Ferreira Neto, A.A. Establishing minimal clinically important difference for the UCLA and ASES scores after rotator cuff repair. Orthop. Traumatol. Surg. Res. 2021, 108, 102894. [Google Scholar] [CrossRef] [PubMed]
- Maillot, C.; Harly, E.; Demezon, H.; Le Huec, J.-C. Surgical repair of large-to-massive rotator cuff tears seems to be a better option than patch augmentation or débridement and biceps tenotomy: A prospective comparative study. J. Shoulder Elb. Surg. 2018, 27, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Benedetto, E.D.D.; Benedetto, P.D.; Fiocchi, A.; Beltrame, A.; Causero, A. Partial repair in irreparable rotator cuff tear: Our experience in long-term follow-up. Acta Bio Med. Atenei Parm. 2017, 88 (Suppl. S4), 69. [Google Scholar]
- Baverel, L.P.; Bonnevialle, N.; Joudet, T.; Valenti, P.; Kany, J.; Grimberg, J.; van Rooij, F.; Collin, P. Short-term outcomes of arthroscopic partial repair vs. latissimus dorsi tendon transfer in patients with massive and partially repairable rotator cuff tears. J. Shoulder Elb. Surg. 2021, 30, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Besnard, M.; Freychet, B.; Clechet, J.; Hannink, G.; Saffarini, M.; Carrillon, Y.; Godenèche, A. Partial and complete repairs of massive rotator cuff tears maintain similar long-term improvements in clinical scores. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 181–191. [Google Scholar] [CrossRef]
- Galasso, O.; Riccelli, D.A.; De Gori, M.; De Benedetto, M.; Orlando, N.; Gasparini, G.; Castricini, R. Quality of Life and Functional Results of Arthroscopic Partial Repair of Irreparable Rotator Cuff Tears. Arthrosc. J. Arthrosc. Relat. Surg. 2017, 33, 261–268. [Google Scholar] [CrossRef]
- Kim, S.-J.; Lee, I.-S.; Kim, S.-H.; Lee, W.-Y.; Chun, Y.-M. Arthroscopic Partial Repair of Irreparable Large to Massive Rotator Cuff Tears. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 761–768. [Google Scholar] [CrossRef]
- Lee, K.W.; Lee, G.S.; Yang, D.S.; Park, S.H.; Chun, Y.S.; Choy, W.S. Clinical Outcome of Arthroscopic Partial Repair of Large to Massive Posterosuperior Rotator Cuff Tears: Medialization of the Attachment Site of the Rotator Cuff Tendon. Clin. Orthop. Surg. 2020, 12, 353. [Google Scholar] [CrossRef]
- Mori, D.; Funakoshi, N.; Yamashita, F. Arthroscopic Surgery of Irreparable Large or Massive Rotator Cuff Tears With Low-Grade Fatty Degeneration of the Infraspinatus: Patch Autograft Procedure Versus Partial Repair Procedure. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1911–1921. [Google Scholar] [CrossRef]
- Park, S.-R.; Sun, D.-H.; Kim, J.; Lee, H.-J.; Kim, J.-B.; Kim, Y.-S. Is augmentation with the long head of the biceps tendon helpful in arthroscopic treatment of irreparable rotator cuff tears? J. Shoulder Elb. Surg. 2018, 27, 1969–1977. [Google Scholar] [CrossRef]
- Porcellini, G.; Castagna, A.; Cesari, E.; Merolla, G.; Pellegrini, A.; Paladini, P. Partial repair of irreparable supraspinatus tendon tears: Clinical and radiographic evaluations at long-term follow-up. J. Shoulder Elb. Surg. 2011, 20, 1170–1177. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-H.; Chiang, E.-R.; Wang, H.-Y.; Ma, H.-L. Arthroscopic Partial Repair of Irreparable Rotator Cuff Tears: Factors Related to Greater Degree of Clinical Improvement at 2 Years of Follow-Up. Arthrosc. J. Arthrosc. Relat. Surg. 2017, 33, 1949–1955. [Google Scholar] [CrossRef] [PubMed]
- Cuff, D.J.; Pupello, D.R.; Santoni, B.G. Partial rotator cuff repair and biceps tenotomy for the treatment of patients with massive cuff tears and retained overhead elevation: Midterm outcomes with a minimum 5 years of follow-up. J. Shoulder Elb. Surg. 2016, 25, 1803–1809. [Google Scholar] [CrossRef]
- Shon, M.S.; Koh, K.H.; Lim, T.K.; Kim, W.J.; Kim, K.C.; Yoo, J.C. Arthroscopic Partial Repair of Irreparable Rotator Cuff Tears: Preoperative Factors Associated With Outcome Deterioration Over 2 Years. Am. J. Sports Med. 2015, 43, 1965–1975. [Google Scholar] [CrossRef]
- Boileau, P.; Baqué, F.; Valerio, L.; Ahrens, P.; Chuinard, C.; Trojani, C. Isolated Arthroscopic Biceps Tenotomy or Tenodesis Improves Symptoms in Patients with Massive Irreparable Rotator Cuff Tears. J. Bone Jt Surg. 2007, 89, 747–757. [Google Scholar] [CrossRef]
- Klinger, H.-M.; Spahn, G.; Baums, M.H.; Stecket, H. Arthroscopic Debridement of Irreparable Massive Rotator Cuff Tears—A Comparison of Debridement Alone and Combined Procedure with Biceps Tenotomy. Acta Chir. Belg. 2005, 105, 297–301. [Google Scholar] [CrossRef]
- Vogler, T.; Andreou, D.; Gosheger, G.; Kurpiers, N.; Velmans, C.; Ameziane, Y.; Schneider, K.; Rickert, C.; Liem, D.; Schorn, D. Long-term outcome of arthroscopic debridement of massive irreparable rotator cuff tears. PLoS ONE 2020, 15, e0241277. [Google Scholar] [CrossRef]
- Walch, G.; Edwards, T.B.; Boulahia, A.; Nové-Josserand, L.; Neyton, L.; Szabo, I. Arthroscopic tenotomy of the long head of the biceps in the treatment of rotator cuff tears: Clinical and radiographic results of 307 cases. J. Shoulder Elb. Surg. 2005, 14, 238–246. [Google Scholar] [CrossRef]
- Liem, D.; Lengers, N.; Dedy, N.; Poetzl, W.; Steinbeck, J.; Marquardt, B. Arthroscopic Debridement of Massive Irreparable Rotator Cuff Tears. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 743–748. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Barth, J.R.H.; Richards, D.P.; Zlatkin, M.B.; Larsen, M. Arthroscopic Repair of Massive Rotator Cuff Tears With Stage 3 and 4 Fatty Degeneration. Arthrosc. J. Arthrosc. Relat. Surg. 2007, 23, 347–354. [Google Scholar] [CrossRef]
- Lee, S.H.; Nam, D.J.; Kim, S.J.; Kim, J.W. Comparison of Clinical and Structural Outcomes by Subscapularis Tendon Status in Massive Rotator Cuff Tear. Am. J. Sports Med. 2017, 45, 2555–2562. [Google Scholar] [CrossRef]
- Park, J.-Y.; Chung, S.W.; Lee, S.-J.; Cho, H.-W.; Lee, J.H.; Lee, J.-H.; Oh, K.-S. Combined Subscapularis Tears in Massive Posterosuperior Rotator Cuff Tears: Do They Affect Postoperative Shoulder Function and Rotator Cuff Integrity? Am. J. Sports Med. 2016, 44, 183–190. [Google Scholar] [CrossRef]
- Araya-Quintanilla, F.; Gutiérrez-Espinoza, H.; Gana-Hervias, G.; Cavero-Redondo, I.; Álvarez-Bueno, C. Association between type of rotator cuff tear and functional outcomes in patients massive and irreparable rotator cuff tear: A pre-post intervention study. J. Shoulder Elb. Surg. 2021, 30, 1393–1401. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, J.N.; Bishop, J.Y.; Lo, I.K.Y.; Flatow, E.L. Fatty Infiltration and Atrophy of the Rotator Cuff do not Improve after Rotator Cuff Repair and Correlate with Poor Functional Outcome. Am. J. Sports Med. 2007, 35, 719–728. [Google Scholar] [CrossRef] [PubMed]
- McElvany, M.D.; McGoldrick, E.; Gee, A.O.; Neradilek, M.B.; Matsen, F.A. Rotator Cuff Repair: Published Evidence on Factors Associated With Repair Integrity and Clinical Outcome. Am. J. Sports Med. 2015, 43, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.H.; Kim, S.H.; Ji, H.M.; Jo, K.H.; Bin, S.W.; Gong, H.S. Prognostic Factors Affecting Anatomic Outcome of Rotator Cuff Repair and Correlation With Functional Outcome. Arthrosc. J. Arthrosc. Relat. Surg. 2009, 25, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Pagán-Conesa, A.; García-Ortiz, M.T.; Salmerón-Martínez, E.J.; Moya-Martínez, A.; López-Prats, F. Diagnostic Ultrasound Shows Reversal of Supraspinatus Muscle Atrophy Following Arthroscopic Rotator Cuff Repair. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 3039–3048. [Google Scholar] [CrossRef]
- Lee, Y.S.; Jeong, J.Y.; Park, C.-D.; Kang, S.G.; Yoo, J.C. Evaluation of the Risk Factors for a Rotator Cuff Retear After Repair Surgery. Am. J. Sports Med. 2017, 45, 1755–1761. [Google Scholar] [CrossRef]
- Godenèche, A.; Freychet, B.; Lanzetti, R.M.; Clechet, J.; Carrillon, Y.; Saffarini, M. Should massive rotator cuff tears be reconstructed even when only partially repairable? Knee Surg Sports Traumatol. Arthrosc. 2017, 25, 2164–2173. [Google Scholar] [CrossRef]
- Heuberer, P.R.; Kölblinger, R.; Buchleitner, S.; Pauzenberger, L.; Laky, B.; Auffarth, A.; Moroder, P.; Salem, S.; Kriegleder, B.; Anderl, W. Arthroscopic management of massive rotator cuff tears: An evaluation of debridement, complete, and partial repair with and without force couple restoration. Knee Surg Sports Traumatol. Arthrosc. 2016, 24, 3828–3837. [Google Scholar] [CrossRef]
- Iannotti, J.P.; Deutsch, A.; Green, A.; Rudicel, S.; Christensen, J.; Marraffino, S.; Rodeo, S. Time to failure after rotator cuff repair: A prospective imaging study. J. Bone Joint. Surg. Am. 2013, 95, 965–971. [Google Scholar] [CrossRef]
- Lee, S.; Park, I.; Lee, H.A.; Shin, S.-J. Factors Related to Symptomatic Failed Rotator Cuff Repair Leading to Revision Surgeries After Primary Arthroscopic Surgery. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 36, 2080–2088. [Google Scholar] [CrossRef] [PubMed]
- Lambers Heerspink, F.O.; Dorrestijn, O. Editorial Commentary: Rotator Cuff Tear: Know When Not to Operate So You Don’t Make It Worse. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 36, 2091–2093. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BT | PCR | ||||
|---|---|---|---|---|---|
| n = | 506 | 590 | |||
| Male | 237 | 46.8% | 312 | 52.9% | NS |
| Female | 269 | 53.2% | 278 | 47.1% | |
| Age (mean ± SD) | 67.6 | ±5.9 | 6.5 | ±7.7 | NS |
| Follow-up (mean ± SD) | 4.7 | ±1.1 | 4.5 | ±1.2 | NS |
| Subscapularis | <0.001 | ||||
| Normal | 265 | 65.9% | 480 | 85.3% | |
| Partial tear | 76 | 18.9% | 81 | 14.4% | |
| Complete tear | 61 | 15.2% | 2 | 0.4% | |
| Cuff tear Large | 19 | 9.5% | 51 | 13.5% | 0.011 |
| Massive | 180 | 90.5% | 328 | 86.5% | |
| Number of Tendons involved | <0.001 | ||||
| 1 | 124 | 25.6% | 19 | 4.8% | |
| 2 | 219 | 45.2% | 298 | 75.3% | |
| 3 | 141 | 29.1% | 79 | 19.9% | |
| Fatty infiltration (Goutallier) | 0.324 | ||||
| 1 | 2 | 1.5% | 1 | 0.4% | |
| 2 | 18 | 13.6% | 30 | 12.3% | |
| 3 | 89 | 67.4% | 150 | 61.7% | |
| 4 | 23 | 17.4% | 62 | 25.5% | |
| Osteoarthritis (Grade) | <0.001 | ||||
| 0 | 9 | 1.9% | 225 | 56.3% | |
| 1 | 233 | 49.4% | 136 | 34.0% | |
| 2 | 181 | 38.3% | 30 | 7.5% | |
| ≥3 | 49 | 10.4% | 9 | 2.3% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Descamps, J.; Kierszbaum, E.; Protais, M.; Marion, B.; Bouché, P.-A.; Aïm, F. Outcomes of Isolated Biceps Tenodesis/Tenotomy or Partial Rotator Cuff Repair Associated with Biceps Tenodesis/Tenotomy for Massive Irreparable Tears: A Systematic Review. J. Clin. Med. 2023, 12, 2565. https://doi.org/10.3390/jcm12072565
Descamps J, Kierszbaum E, Protais M, Marion B, Bouché P-A, Aïm F. Outcomes of Isolated Biceps Tenodesis/Tenotomy or Partial Rotator Cuff Repair Associated with Biceps Tenodesis/Tenotomy for Massive Irreparable Tears: A Systematic Review. Journal of Clinical Medicine. 2023; 12(7):2565. https://doi.org/10.3390/jcm12072565
Chicago/Turabian StyleDescamps, Jules, Elliott Kierszbaum, Marie Protais, Blandine Marion, Pierre-Alban Bouché, and Florence Aïm. 2023. "Outcomes of Isolated Biceps Tenodesis/Tenotomy or Partial Rotator Cuff Repair Associated with Biceps Tenodesis/Tenotomy for Massive Irreparable Tears: A Systematic Review" Journal of Clinical Medicine 12, no. 7: 2565. https://doi.org/10.3390/jcm12072565
APA StyleDescamps, J., Kierszbaum, E., Protais, M., Marion, B., Bouché, P.-A., & Aïm, F. (2023). Outcomes of Isolated Biceps Tenodesis/Tenotomy or Partial Rotator Cuff Repair Associated with Biceps Tenodesis/Tenotomy for Massive Irreparable Tears: A Systematic Review. Journal of Clinical Medicine, 12(7), 2565. https://doi.org/10.3390/jcm12072565