
Sexual Dysfunction in People with Multiple Sclerosis: The Role of Disease Severity, Illness Perception, and Depression

 , ,
, ,  , , ,
, , ,  , , ,
, , ,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Procedures and Participants
2.2. Measures
2.2.1. Socio-Demographic and Clinical Information
2.2.2. Disease Severity
2.2.3. Illness Perceptions
2.2.4. Depressive Symptoms
2.2.5. Sexual Dysfunction
2.3. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
3.2. Descriptive Statistics and Bivariate Correlations
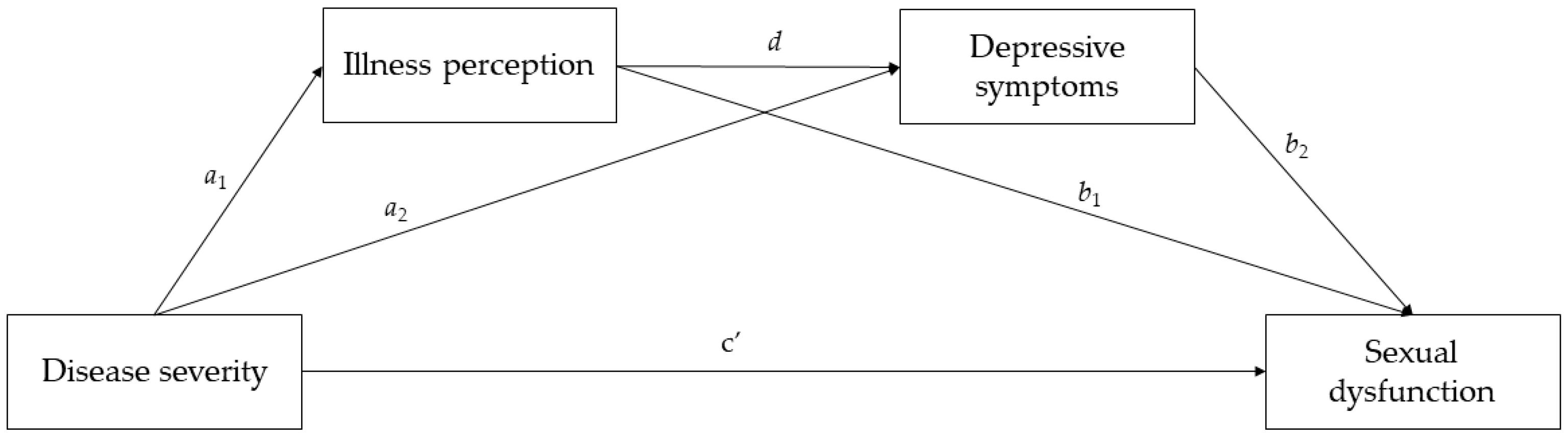
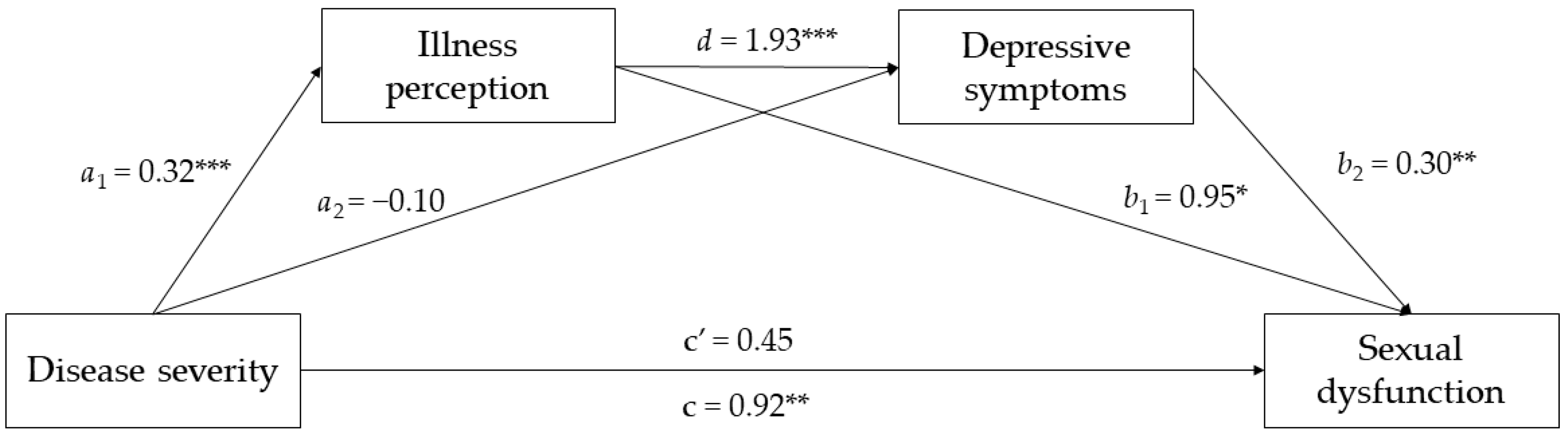
3.3. Serial Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carotenuto, A.; Scandurra, C.; Costabile, T.; Lavorgna, L.; Borriello, G.; Moiola, L.; Inglese, M.; Trojsi, F.; Petruzzo, M.; Ianniello, A.; et al. Physical exercise moderates the effects of disability on depression in people with multiple sclerosis during the COVID-19 outbreak. J. Clin. Med. 2021, 10, 1234. [Google Scholar] [CrossRef]
- Filippi, M.; Bar-Or, A.; Piehl, F.; Preziosa, P.; Solari, A.; Vukusic, S.; Rocca, M.A. Multiple sclerosis. Nat. Rev. Dis. Prim. 2018, 4, 43. [Google Scholar] [CrossRef]
- Hanna, M.; Strober, L.B. Anxiety and depression in Multiple Sclerosis (MS): Antecedents, consequences, and differential impact on well-being and quality of life. Mult. Scler. Relat. Disord. 2020, 44, 102261. [Google Scholar] [CrossRef]
- Petracca, M.; Pontillo, G.; Moccia, M.; Carotenuto, A.; Cocozza, S.; Lanzillo, R.; Brunetti, A.; Brescia Morra, V. Neuroimaging correlates of cognitive dysfunction in adults with multiple sclerosis. Brain Sci. 2021, 11, 346. [Google Scholar] [CrossRef] [PubMed]
- Rosa, L.; Scandurra, C.; Chiodi, A.; Petracca, M.; Costabile, T.; Lauro, F.; Moccia, M.; Carotenuto, A.; Maldonato, N.M.; Brescia Morra, V.; et al. Mental health in multiple sclerosis during the COVID-19 outbreak: A delicate balance between fear of contagion and resilience. J. Clin. Psychol. Med. Settings 2022, 29, 798–807. [Google Scholar] [CrossRef]
- Feinstein, A.; Magalhaes, S.; Richard, J.F.; Audet, B.; Moore, C. The link between multiple sclerosis and depression. Nat. Rev. Neurol. 2014, 10, 507–517. [Google Scholar] [CrossRef]
- Bamer, A.M.; Cetin, K.; Johnson, K.L.; Gibbons, L.E.; Ehde, D.M. Validation study of prevalence and correlates of depressive symptomatology in multiple sclerosis. Gen. Hosp. Psychiatry 2008, 30, 311–317. [Google Scholar] [CrossRef]
- Lewis, V.M.; Williams, K.; KoKo, C.; Woolmore, J.; Jones, C.; Powell, T. Disability, depression and suicide ideation in people with multiple sclerosis. J. Affect. Disord. 2017, 208, 662–669. [Google Scholar] [CrossRef]
- Leventhal, H.; Phillips, L.A.; Burns, E. The Common-Sense Model of Self-Regulation (CSM): A dynamic framework for understanding illness self-management. J. Behav. Med. 2016, 39, 935–946. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, A.T.; Harris, S.L.; Koenig, H.G. Illness perception and high readmission health outcomes. Health Psychol. Open 2019, 6, 2055102919844504. [Google Scholar] [CrossRef] [PubMed]
- Keil, D.C.; Vaske, I.; Kenn, K.; Rief, W.; Stenzel, N.M. With the strength to carry on. Chronic Respir. Dis. 2017, 14, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Bonsaksen, T.; Lerdal, A.; Fagermoen, M.S. Trajectories of illness perceptions in persons with chronic illness: An explorative longitudinal study. J. Health Psychol. 2015, 20, 942–953. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Fang, W.; An, Y.; Wang, L.; Fan, X. The multiple mediating effects of illness perceptions and coping strategies on the relationship between physical symptoms and depressive symptoms in patients with heart failure. Eur. J. Cardiovasc. Nurs. 2020, 19, 125–133. [Google Scholar] [CrossRef] [PubMed]
- De Gucht, V. Illness perceptions mediate the relationship between bowel symptom severity and health-related quality of life in IBS patients. Qual. Life Res. 2015, 24, 1845–1856. [Google Scholar] [CrossRef]
- Zhang, M.; Hong, L.; Zhang, T.; Lin, Y.; Zheng, S.; Zhou, X.; Fan, R.; Wang, Z.; Zhang, C.; Zhong, J. Illness perceptions and stress: Mediators between disease severity and psychological well-being and quality of life among patients with Crohn’s disease. Patient Prefer. Adherence 2016, 10, 2387–2396. [Google Scholar] [CrossRef] [PubMed]
- Hagger, M.S.; Orbell, S. The common sense model of illness self-regulation: A conceptual review and proposed extended model. Health Psychol. Rev. 2022, 16, 347–377. [Google Scholar] [CrossRef]
- Bronner, G.; Elran, E.; Golomb, J.; Korczyn, A.D. Female sexuality in multiple sclerosis: The multidimensional nature of the problem and the intervention. Acta Neurol. Scand. 2010, 121, 289–301. [Google Scholar] [CrossRef]
- Carotenuto, A.; De Giglio, L.; Chiodi, A.; Petracca, M.; Rosa, L.; Bianchi, M.; Ferrante, I.; Lauro, F.; Moccia, M.; Ianniello, A.; et al. Validation of the Italian version of the Multiple Sclerosis Intimacy and Sexuality Questionnaire-19. Neurol. Sci. 2021, 42, 2903–2910. [Google Scholar] [CrossRef]
- Celik, D.B.; Poyraz, E.Ç.; Bingöl, A.; Idiman, E.; Ozakbaş, S.; Kaya, D. Sexual dysfunction ın multiple sclerosis: Gender differences. J. Neurol. Sci. 2013, 324, 17–20. [Google Scholar] [CrossRef]
- Marck, C.H.; Jelinek, P.L.; Weiland, T.J.; Hocking, J.S.; De Livera, A.M.; Taylor, K.L.; Neate, S.L.; Pereira, N.G.; Jelinek, G.A. Sexual function in multiple sclerosis and associations with demographic, disease and lifestyle characteristics: An international cross-sectional study. BMC Neurol. 2016, 16, 210. [Google Scholar] [CrossRef] [PubMed]
- Drulovic, J.; Kisic-Tepavcevic, D.; Pekmezovic, T. Epidemiology, diagnosis and management of sexual dysfunction in multiple sclerosis. Acta Neurol. Belg. 2020, 120, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Basson, R.; Rees, P.; Wang, R.; Montejo, A.L.; Incrocci, L. Sexual function in chronic illness. J. Sex. Med. 2010, 7, 374–388. [Google Scholar] [CrossRef]
- Verschuren, J.E.; Enzlin, P.; Dijkstra, P.U.; Geertzen, J.H.; Dekker, R. Chronic disease and sexuality: A generic conceptual framework. J. Sex. Res. 2010, 47, 153–170. [Google Scholar] [CrossRef]
- Daleboudt, G.M.; Broadbent, E.; McQueen, F.; Kaptein, A.A. The impact of illness perceptions on sexual functioning in patients with systemic lupus erythematosus. J. Psychosom. Res. 2013, 74, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Knowles, S.R.; Gass, C.; Macrae, F. Illness perceptions in IBD influence psychological status, sexual health and satisfaction, body image and relational functioning: A preliminary exploration using Structural Equation Modeling. J. Crohn’s Colitis 2013, 7, e344–e350. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Uitdehaag, B.M.J. Disability outcome measures in phase III clinical trials in multiple sclerosis. CNS Drugs 2018, 32, 543–558. [Google Scholar] [CrossRef]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The brief illness perception questionnaire. J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar] [CrossRef]
- Pain, D.; Miglioretti, M.; Angelino, E. Sviluppo della versione italiana del Brief-IPQ, strumento psicometrico per lo studio delle rappresentazioni di malattia [Development of Italian version of Brief-IPQ, a method for assessing the ù illness representations]. Psicol. Della Salut. 2006, 1, 81–89. [Google Scholar]
- Cella, D.; Lai, J.S.; Nowinski, C.J.; Victorson, D.; Peterman, A.; Miller, D.; Bethoux, F.; Heinemann, A.; Rubin, S.; Cavazos, J.E.; et al. Neuro-QOL: Brief measures of health-related quality of life for clinical research in neurology. Neurology 2012, 78, 1860–1867. [Google Scholar] [CrossRef]
- Sanders, A.S.; Foley, F.W.; LaRocca, N.G.; Zemon, V. The Multiple Sclerosis Intimacy and Sexuality Questionnaire-19 (MSISQ-19). Sex. Disabil. 2000, 18, 3–26. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 1st ed.; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Sadeghi Bahmani, D.; Motl, R.W. Rate, burden, and treatment of sexual dysfunction in multiple sclerosis: The case for exercise training as a new treatment approach. Mult. Scler. Relat. Disord. 2021, 51, 102878. [Google Scholar] [CrossRef]
- Akinwande, M.O.; Hussaini, G.D.; Agboola, S. Variance inflation factor: As a condition for the inclusion of suppressor variable(s) in regression analysis. Open J. Stat. 2015, 5, 754–767. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Danks, N.P.; Ray, S. Mediation analysis. In Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R: A Workbook; Hair, J.F., Hult, G.T.M., Ringle, C.M., Sarstedt, M., Danks, N.P., Ray, S., Eds.; Springer: Cham, Switzerland, 2021; pp. 139–154. [Google Scholar]
- Luca, M.; Eccles, F.; Perez Algorta, G.; Patti, F. Illness perceptions and outcome in multiple sclerosis: A systematic review of the literature. Mult. Scler. Relat. Disord. 2022, 67, 104180. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.; Sousa, C.; Pereira, M.; Pereira, M.G. Quality of life in patients with multiple sclerosis: A study with patients and caregivers. Disabil. Health J. 2019, 12, 628–634. [Google Scholar] [CrossRef]
- Wilski, M.; Kocur, P.; Górny, M.; Koper, M.; Nadolska, A.; Chmielewski, B.; Tomczak, M. Perception of multiple sclerosis impact and treatment efficacy beliefs: Mediating effect of patient’s illness and self-appraisals. J. Pain Symptom Manag. 2019, 58, 437–444. [Google Scholar] [CrossRef]
- Altmann, P.; Leutmezer, F.; Leithner, K.; Monschein, T.; Ponleitner, M.; Stattmann, M.; Rommer, P.S.; Zrzavy, T.; Zulehner, G.; Berek, K.; et al. Predisposing factors for sexual dysfunction in multiple sclerosis. Front. Neurol. 2021, 12, 618370. [Google Scholar] [CrossRef]
- Mohammadi, K.; Rahnama, P.; Rafei, Z.; Ebrahimi-Aveh, S.M.; Montazeri, A. Factors associated with intimacy and sexuality among young women with multiple sclerosis. Reprod. Health 2020, 17, 110. [Google Scholar] [CrossRef] [PubMed]
- Gaviria-Carrillo, M.; Bueno-Florez, S.J.; Ortiz-Salas, P.A. Assessment of sexual dysfunction in patients with multiple sclerosis: A perspective from neurologist. BMC Neurol. 2022, 22, 372. [Google Scholar] [CrossRef] [PubMed]
- Giannopapas, V.; Kitsos, D.; Tsogka, A.; Tzartos, J.S.; Paraskevas, G.; Tsivgoulis, G.; Voumvourakis, K.; Giannopoulos, S.; Bakalidou, D. Sexual dysfunction therapeutic approaches in patients with multiple sclerosis: A systematic review. Neurol. Sci. 2022. Advance Online Publication. [Google Scholar] [CrossRef] [PubMed]
- Bassi, M.; Cilia, S.; Falautano, M.; Grobberio, M.; Niccolai, C.; Pattini, M.; Pietrolongo, E.; Quartuccio, M.E.; Viterbo, R.G.; Allegri, B.; et al. Illness perceptions and psychological adjustment among persons with multiple sclerosis: The mediating role of coping strategies and social support. Disabil. Rehabil. 2020, 42, 3780–3792. [Google Scholar] [CrossRef] [PubMed]
- Bassi, M.; Grobberio, M.; Negri, L.; Cilia, S.; Minacapelli, E.; Niccolai, C.; Pattini, M.; Pietrolongo, E.; Quartuccio, M.E.; Viterbo, R.G.; et al. The contribution of illness beliefs, coping strategies, and social support to perceived physical health and fatigue in multiple sclerosis. J. Clin. Psychol. Med. Settings 2021, 28, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Costabile, T.; Carotenuto, A.; Lavorgna, L.; Borriello, G.; Moiola, L.; Inglese, M.; Petruzzo, M.; Trojsi, F.; Ianniello, A.; Nozzolillo, A.; et al. COVID-19 pandemic and mental distress in multiple sclerosis: Implications for clinical management. Eur. J. Neurol. 2021, 28, 3375–3383. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | M ± SD or Mdn (Range) | |
|---|---|---|---|---|---|
| 1. EDSS | − | 2 (0–8.5) | |||
| 2. Illness perception | 0.38 *** | − | 5.33 ± 1.44 | ||
| 3. Depressive symptoms | 0.16 *** | 0.45 *** | − | 13.63 ± 6.77 | |
| 4. Sexual dysfunction | 0.14 *** | 0.19 *** | 0.19 *** | − | 36.03 ± 15.06 |
| β | BootSE | t | p | BootLLCI | BootULCI | |
|---|---|---|---|---|---|---|
| Outcome: Illness perception | ||||||
| Disease severity | 0.317 | 0.026 | 12.214 | <0.001 | 0.266 | 0.368 |
| Outcome: Depressive symptoms | ||||||
| Disease severity | −0.100 | 0.121 | −0.826 | 0.409 | −0.338 | 0.138 |
| Illness perception | 1.929 | 0.146 | 13.224 | <0.001 | 1.643 | 2.215 |
| Outcome: Sexual dysfunction | ||||||
| Disease severity (direct effect) | 0.450 | 0.310 | 1.453 | 0.147 | −0.158 | 1.058 |
| Illness perception | 0.995 | 0.408 | 2.441 | 0.015 | 0.195 | 1.795 |
| Depressive symptoms | 0.298 | 0.086 | 3.463 | 0.001 | 0.129 | 0.467 |
| Indirect effects | ||||||
| Disease severity → illness perception → sexual dysfunction | 0.315 | 0.141 | − | − | 0.039 | 0.590 |
| Disease severity → depressive symptoms → sexual dysfunction | −0.030 | 0.039 | − | − | −0.116 | 0.042 |
| Disease severity → illness perception → depressive symptoms → sexual dysfunction | 0.182 | 0.060 | − | − | 0.074 | 0.309 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scandurra, C.; Rosa, L.; Carotenuto, A.; Moccia, M.; Arena, S.; Ianniello, A.; Nozzolillo, A.; Turrini, M.; Streito, L.M.; Abbadessa, G.; et al. Sexual Dysfunction in People with Multiple Sclerosis: The Role of Disease Severity, Illness Perception, and Depression. J. Clin. Med. 2023, 12, 2215. https://doi.org/10.3390/jcm12062215
Scandurra C, Rosa L, Carotenuto A, Moccia M, Arena S, Ianniello A, Nozzolillo A, Turrini M, Streito LM, Abbadessa G, et al. Sexual Dysfunction in People with Multiple Sclerosis: The Role of Disease Severity, Illness Perception, and Depression. Journal of Clinical Medicine. 2023; 12(6):2215. https://doi.org/10.3390/jcm12062215
Chicago/Turabian StyleScandurra, Cristiano, Laura Rosa, Antonio Carotenuto, Marcello Moccia, Sebastiano Arena, Antonio Ianniello, Agostino Nozzolillo, Mariavittoria Turrini, Lidia Mislin Streito, Gianmarco Abbadessa, and et al. 2023. "Sexual Dysfunction in People with Multiple Sclerosis: The Role of Disease Severity, Illness Perception, and Depression" Journal of Clinical Medicine 12, no. 6: 2215. https://doi.org/10.3390/jcm12062215
APA StyleScandurra, C., Rosa, L., Carotenuto, A., Moccia, M., Arena, S., Ianniello, A., Nozzolillo, A., Turrini, M., Streito, L. M., Abbadessa, G., Ferraro, E., Mattioli, M., Chiodi, A., Maldonato, N. M., Bonavita, S., Clerico, M., Cordioli, C., Moiola, L., Patti, F., ... Lanzillo, R. (2023). Sexual Dysfunction in People with Multiple Sclerosis: The Role of Disease Severity, Illness Perception, and Depression. Journal of Clinical Medicine, 12(6), 2215. https://doi.org/10.3390/jcm12062215