
Development and Validation of Nomograms Predicting the 5- and 8-Year Overall and Cancer-Specific Survival of Bladder Cancer Patients Based on SEER Program


Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Information and Survival Analysis
2.2. Nomogram Model Establishment and Risk Classification
2.3. Nomogram Model Validation
3. Results
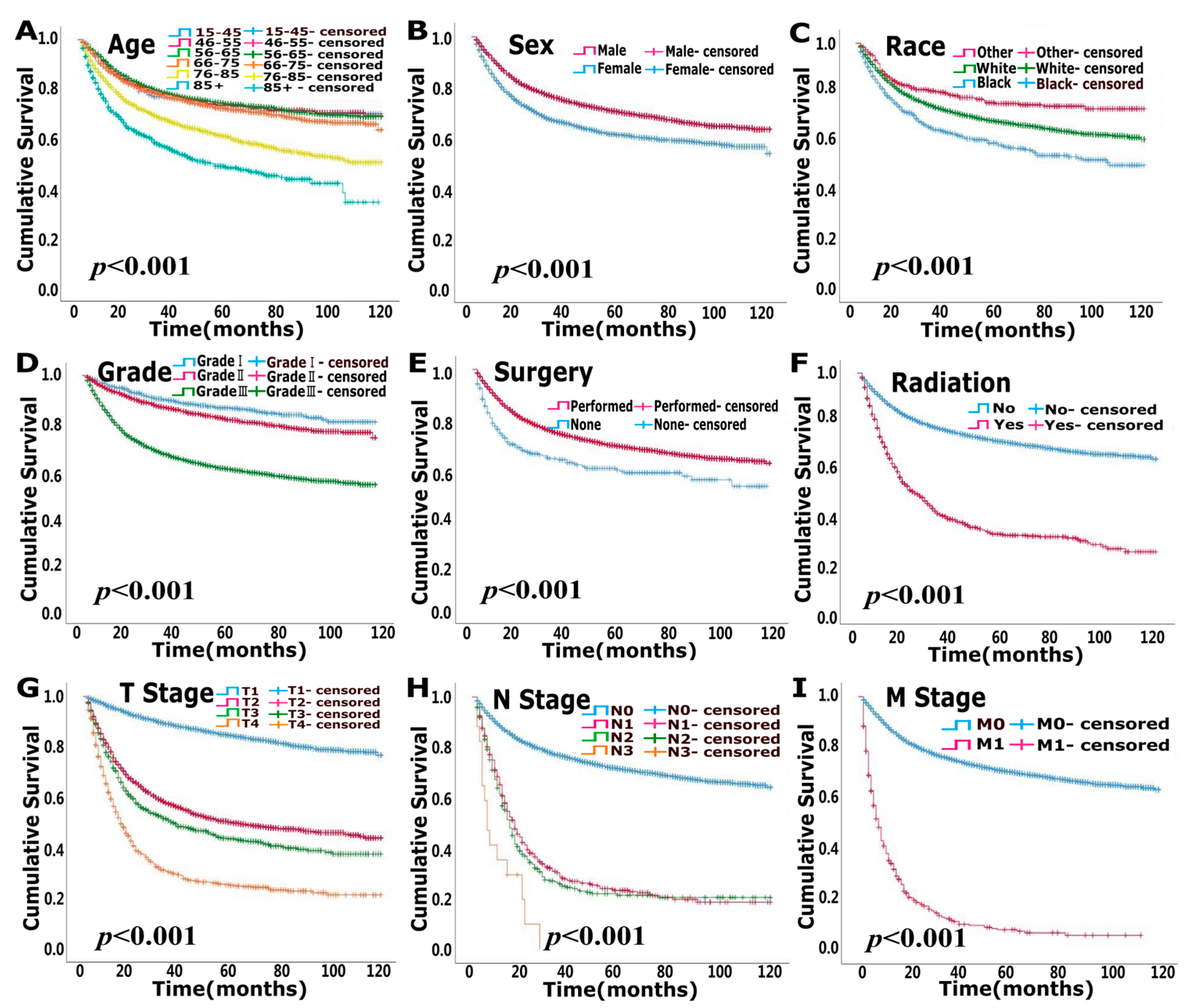
3.1. Clinicopathological Data for Patients and Survival Analysis
3.2. Nomogram Model Establishment and Risk Classification
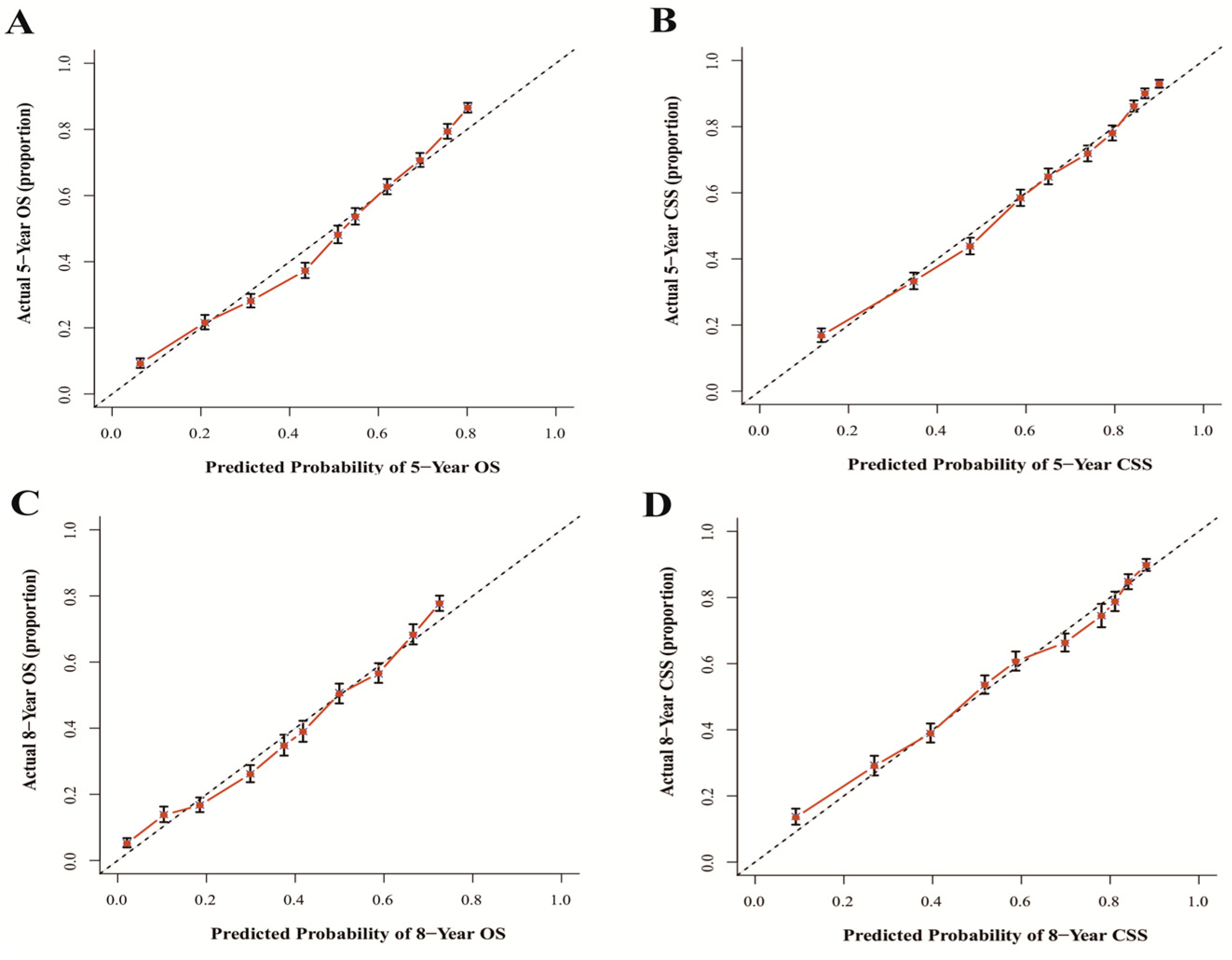
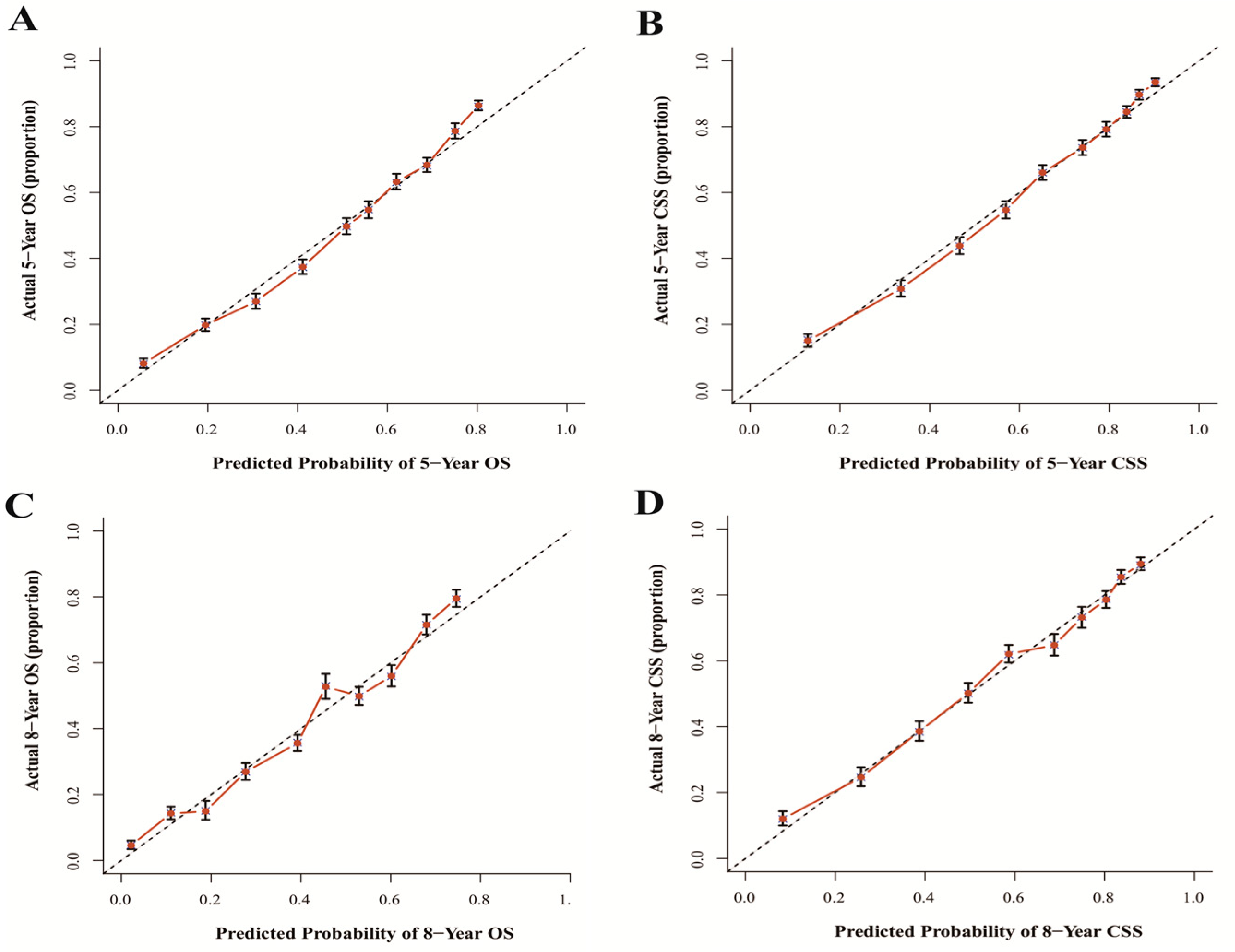
3.3. Nomogram Model Validation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Raghavan, D. Chemotherapy for Muscle-Invasive Bladder Cancer Treated with Definitive Radiotherapy: Persisting Uncertainties. Nat. Clin. Pract. Oncol. 2008, 5, 444–454. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee On Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Jankovic, S.; Radosavljevic, V. Risk Factors for Bladder Cancer. Tumori 2007, 93, 4–12. [Google Scholar] [CrossRef]
- Patel, V.G.; Oh, W.K.; Galsky, M.D. Treatment of Muscle-Invasive and Advanced Bladder Cancer in 2020. CA Cancer J. Clin. 2020, 70, 404–423. [Google Scholar] [CrossRef] [PubMed]
- Cicione, A.; Manno, S.; Ucciero, G.; Cantiello, F.; Damiano, R.; Lima, E.; Posti, A.; Balloni, F.; De Nunzio, C. A Larger Detrusor Wall Thickness Increases the Risk of Non Muscle Invasive Bladder Cancer Recurrence and Progression: Result From a Multicenter Observational Study. Minerva Urol. Nefrol. 2018, 70, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Cantiello, F.; Cicione, A.; Autorino, R.; De Nunzio, C.; Salonia, A.; Briganti, A.; Aliberti, A.; Perdona, S.; Tubaro, A.; Damiano, R. Metabolic Syndrome, Obesity, and Radical Cystectomy Complications: A Clavien Classification System-Based Analysis. Clin. Genitourin Cancer 2014, 12, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zhang, H.; Wen, J.; Zhou, J.; Liu, Y.; Cheng, B.; Chen, X.; Wei, J. Nomograms Forecasting Long-Term Overall and Cancer-Specific Survival of Patients with Oral Squamous Cell Carcinoma. Cancer Med. 2018, 7, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, M.H.; Bahnson, R.R.; Barry, M.; Busby, J.E.; Carroll, P.R.; Carter, H.B.; Catalona, W.J.; Cookson, M.S.; Epstein, J.I.; Etzioni, R.B.; et al. NCCN Clinical Practice Guidelines in Oncology: Prostate Cancer Early Detection. J. Natl. Compr. Cancer Netw. 2010, 8, 240–262. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, Y.; Yan, Z.; Wan, X.; Xia, Y.; Wang, K.; Liu, J.; Lau, W.Y.; Wu, M.; Shen, F. A Nomogram Predicting Pulmonary Metastasis of Hepatocellular Carcinoma Following Partial Hepatectomy. Br. J. Cancer 2014, 110, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wen, J.; Cao, S.; Yang, X.; Yang, Z.; Li, H.; Meng, H.; Thieringer, F.M.; Wei, J. Nomogram Predicting Long-Term Overall and Cancer-Specific Survival of Patients with Buccal Mucosa Cancer. BMC Oral. Health 2022, 22, 138. [Google Scholar] [CrossRef]
- Liu, J.; Geng, Q.; Liu, Z.; Chen, S.; Guo, J.; Kong, P.; Chen, Y.; Li, W.; Zhou, Z.; Sun, X.; et al. Development and External Validation of a Prognostic Nomogram for Gastric Cancer Using the National Cancer Registry. Oncotarget 2016, 7, 35853–35864. [Google Scholar] [CrossRef]
- Snee, R.D. Validation of Regression Models: Methods and Examples. Technometrics 1977, 19, 415–428. [Google Scholar] [CrossRef]
- Harrell, F.E. Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer: New York, NY, USA, 2001. [Google Scholar]
- Austin, P.C.; Steyerberg, E.W. Events Per Variable (EPV) and the Relative Performance of Different Strategies for Estimating the Out-Of-Sample Validity of Logistic Regression Models. Stat. Methods Med. Res. 2017, 26, 796–808. [Google Scholar] [CrossRef]
- Zumsteg, Z.S.; Cook-Wiens, G.; Yoshida, E.; Shiao, S.L.; Lee, N.Y.; Mita, A.; Jeon, C.; Goodman, M.T.; Ho, A.S. Incidence of Oropharyngeal Cancer Among Elderly Patients in the United States. JAMA Oncol. 2016, 2, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Liu, Y.; Yang, J.; Liu, Q.; You, H.; Dong, Y.; Lyu, J. Development and Validation of a Nomogram for Predicting Survival in Male Patients with Breast Cancer. Front. Oncol. 2019, 9, 361. [Google Scholar] [CrossRef]
- Vickers, A.J.; Elkin, E.B. Decision Curve Analysis: A Novel Method for Evaluating Prediction Models. Med. Decis. Making 2006, 26, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Zhu, S.; Cui, X.; Xu, W.; Kong, C.; Zhang, Z.; Qian, W. Identifying Non-Muscle-Invasive and Muscle-Invasive Bladder Cancer Based On Blood Serum Surface-Enhanced Raman Spectroscopy. Biomed. Opt. Express 2019, 10, 3533–3544. [Google Scholar] [CrossRef] [PubMed]
- Goodison, S.; Rosser, C.J.; Urquidi, V. Bladder Cancer Detection and Monitoring: Assessment of Urine- and Blood-Based Marker Tests. Mol. Diagn. Ther. 2013, 17, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Zhan, X.; Jiang, M.; Deng, W.; Liu, X.; Chen, L.; Fu, B. Development and Validation of a Prognostic Nomogram for Predicting Cancer-Specific Survival in Patients with Lymph Node Positive Bladder Cancer: A Study Based on SEER Database. Front. Oncol. 2022, 12, 789028. [Google Scholar] [CrossRef]
- Wang, F.; Wen, J.; Yang, X.; Jia, T.; Du, F.; Wei, J. Applying Nomograms Based On the Surveillance, Epidemiology and End Results Database to Predict Long-Term Overall Survival and Cancer-Specific Survival in Patients with Oropharyngeal Squamous Cell Carcinomas: A Case-Control Research. Medicine 2020, 99, e20703. [Google Scholar] [CrossRef]
- Zhao, R.; Jia, T.; Qiao, B.; Liang, J.; Qu, S.; Zhu, L.; Feng, H.; Xing, L.; Ren, Y.; Wang, F.; et al. Nomogram Predicting Long-Term Overall Survival and Cancer-Specific Survival of Lip Carcinoma Patients Based On the SEER Database: A Retrospective Case-Control Study. Medicine 2019, 98, e16727. [Google Scholar] [CrossRef] [PubMed]
- Goossens-Laan, C.A.; Leliveld, A.M.; Verhoeven, R.H.; Kil, P.J.; de Bock, G.H.; Hulshof, M.C.; de Jong, I.J.; Coebergh, J.W. Effects of Age and Comorbidity On Treatment and Survival of Patients with Muscle-Invasive Bladder Cancer. Int. J. Cancer 2014, 135, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Fonteyne, V.; Ost, P.; Bellmunt, J.; Droz, J.P.; Mongiat-Artus, P.; Inman, B.; Paillaud, E.; Saad, F.; Ploussard, G. Curative Treatment for Muscle Invasive Bladder Cancer in Elderly Patients: A Systematic Review. Eur. Urol. 2018, 73, 40–50. [Google Scholar] [CrossRef]
- Madeb, R.; Messing, E.M. Gender, Racial and Age Differences in Bladder Cancer Incidence and Mortality. Urol. Oncol. 2004, 22, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Jain, M.; Kapoor, R.; Muruganandham, K.; Srivastava, A.; Mandhani, A. Impact of Age and Gender On the Clinicopathological Characteristics of Bladder Cancer. Indian J. Urol. 2009, 25, 207–210. [Google Scholar] [CrossRef]
- Guancial, E.A.; Roussel, B.; Bergsma, D.P.; Bylund, K.C.; Sahasrabudhe, D.; Messing, E.; Mohile, S.G.; Fung, C. Bladder Cancer in the Elderly Patient: Challenges and Solutions. Clin. Interv. Aging 2015, 10, 939–949. [Google Scholar] [CrossRef]
- Rose, T.L.; Deal, A.M.; Nielsen, M.E.; Smith, A.B.; Milowsky, M.I. Sex Disparities in Use of Chemotherapy and Survival in Patients with Advanced Bladder Cancer. Cancer 2016, 122, 2012–2020. [Google Scholar] [CrossRef]
- Mungan, N.A.; Aben, K.K.; Schoenberg, M.P.; Visser, O.; Coebergh, J.W.W.; Witjes, J.A.; Kiemeney, L.A. Gender Differences in Stage-Adjusted Bladder Cancer Survival. Urology 2000, 55, 876–880. [Google Scholar] [CrossRef]
- Micheli, A.; Mariotto, A.; Rossi, A.G.; Gatta, G.; Muti, P. The Prognostic Role of Gender in Survival of Adult Cancer Patients. EUROCARE Working Group. Eur. J. Cancer 1998, 34, 2271–2278. [Google Scholar] [CrossRef]
- Wang, Y.; Chang, Q.; Li, Y. Racial Differences in Urinary Bladder Cancer in the United States. Sci. Rep. 2018, 8, 12521. [Google Scholar] [CrossRef]
- Sakaguchi, M.; Maebayashi, T.; Aizawa, T.; Ishibashi, N.; Saito, T. Clinical Results for Bladder Cancer Treated by Radiotherapy without Concurrent Standard Chemotherapy. Anticancer Res. 2016, 36, 5519–5525. [Google Scholar] [CrossRef] [PubMed]
- Kamat, A.M.; Hahn, N.M.; Efstathiou, J.A.; Lerner, S.P.; Malmström, P.U.; Choi, W.; Guo, C.C.; Lotan, Y.; Kassouf, W. Bladder Cancer. Lancet 2016, 388, 2796–2810. [Google Scholar] [CrossRef]
- Harland, S.J.; Kynaston, H.; Grigor, K.; Wallace, D.M.; Beacock, C.; Kockelbergh, R.; Clawson, S.; Barlow, T.; Parmar, M.K.; Griffiths, G.O. A Randomized Trial of Radical Radiotherapy for the Management of pT1G3 NXM0 Transitional Cell Carcinoma of the Bladder. J. Urol. 2007, 178, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Wyszynski, A.; Tanyos, S.A.; Rees, J.R.; Marsit, C.J.; Kelsey, K.T.; Schned, A.R.; Pendleton, E.M.; Celaya, M.O.; Zens, M.S.; Karagas, M.R.; et al. Body Mass and Smoking are Modifiable Risk Factors for Recurrent Bladder Cancer. Cancer 2014, 120, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Kobeissi, L.H.; Yassine, I.A.; Jabbour, M.E.; Moussa, M.A.; Dhaini, H.R. Urinary Bladder Cancer Risk Factors: A Lebanese Case- Control Study. Asian Pac. J. Cancer Prev. 2013, 14, 3205–3211. [Google Scholar] [CrossRef]
- Gu, J.; Wu, X. Genetic Susceptibility to Bladder Cancer Risk and Outcome. Per. Med. 2011, 8, 365–374. [Google Scholar] [CrossRef]
- Racioppi, M. Advances in Management of Bladder Cancer. J. Clin. Med. 2021, 11, 203. [Google Scholar] [CrossRef]
- Lenis, A.T.; Lec, P.M.; Chamie, K. Bladder Cancer: A Review. JAMA 2020, 324, 1980–1991. [Google Scholar] [CrossRef]
- Chalasani, V.; Chin, J.L.; Izawa, J.I. Histologic Variants of Urothelial Bladder Cancer and Nonurothelial Histology in Bladder Cancer. Can. Urol. Assoc. J. 2009, 3, S193–S198. [Google Scholar] [CrossRef]
- Wucherpfennig, S.; Rose, M.; Maurer, A.; Cassataro, M.A.; Seillier, L.; Morsch, R.; Hammad, E.; Baldia, P.H.; Ecke, T.H.; Vogeli, T.A.; et al. Evaluation of Therapeutic Targets in Histological Subtypes of Bladder Cancer. Int. J. Mol. Sci. 2021, 22, 11547. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.B.; Montgomery, J.S.; Montie, J.E.; Kunju, L.P. Variant (divergent) histologic differentiation in urothelial carcinoma is under-recognized in community practice: Impact of mandatory central pathology review at a large referral hospital. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 1650–1655. [Google Scholar] [CrossRef] [PubMed]
- Abd el-Latif, A.; Watts, K.E.; Elson, P.; Fergany, A.; Hansel, D.E. The sensitivity of initial transurethral resection or biopsy of bladder tumor(s) for detecting bladder cancer variants on radical cystectomy. J. Urol. 2013, 189, 1263–1267. [Google Scholar] [CrossRef] [PubMed]
- Curtis, R.E.; Freedman, D.M.; Ron, E.; Ries, L.A.; Hacker, D.G.; Edwards, B.K.; Tucker, M.A.; Fraumeni, J.F., Jr. New Malignancies among Cancer Survivors: SEER Cancer Registries, 1973–2000; No. 05-5302; National Cancer Institute, NIH Publication: Bethesda, MD, USA, 2006. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Modeling Cohort (n = 10,478) | Validation Cohort (n = 10,379) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Age | ||||
| 15–45 | 271 | 2.6 | 281 | 2.7 |
| 46–55 | 1033 | 9.9 | 954 | 9.2 |
| 56–65 | 2358 | 22.5 | 2366 | 22.8 |
| 66–75 | 3003 | 28.7 | 2940 | 28.3 |
| 76–85 | 2801 | 26.7 | 2855 | 27.5 |
| 85+ | 1012 | 9.7 | 983 | 9.5 |
| Sex | ||||
| Male | 7768 | 74.1 | 7816 | 75.3 |
| Female | 2710 | 25.9 | 2563 | 24.7 |
| Race | ||||
| White | 9234 | 88.1 | 9151 | 88.2 |
| Black | 741 | 7.1 | 747 | 7.2 |
| Others | 503 | 4.8 | 481 | 4.6 |
| Grade | ||||
| I | 852 | 8.1 | 806 | 7.8 |
| II | 2611 | 24.9 | 2706 | 26.1 |
| III | 7015 | 66.9 | 6867 | 66.2 |
| Surgery | ||||
| Performed | 10,145 | 96.8 | 9998 | 96.3 |
| None | 333 | 3.2 | 381 | 3.7 |
| Radiation | ||||
| Yes | 922 | 8.8 | 907 | 8.7 |
| No | 9556 | 91.2 | 9472 | 91.3 |
| T stage | ||||
| T1 | 6037 | 57.6 | 5960 | 57.4 |
| T2 | 2799 | 26.7 | 2757 | 26.6 |
| T3 | 898 | 8.6 | 930 | 9.0 |
| T4 | 744 | 7.1 | 732 | 7.1 |
| N stage | ||||
| N0 | 9682 | 92.4 | 9563 | 92.1 |
| N1 | 443 | 4.2 | 471 | 4.5 |
| N2 | 336 | 3.2 | 322 | 3.1 |
| N3 | 17 | 0.2 | 23 | 0.2 |
| M stage | ||||
| M0 | 10,006 | 95.5 | 9897 | 95.4 |
| M1 | 472 | 4.5 | 482 | 4.6 |
| Variables | Uni-Variate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| p Value | HR (95% CI) | p Value | |||
| Age | <0.001 | <0.001 | |||
| 15–45 | 0.205 (0.163–0.257) | <0.001 | |||
| 46–55 | 0.199 (0.175–0.227) | <0.001 | |||
| 56–65 | 0.248 (0.224–0.273) | <0.001 | |||
| 66–75 | 0.345 (0.316–0.377) | <0.001 | |||
| 76–85 | 0.573 (0.526–0.623) | <0.001 | |||
| 85+ | Reference | ||||
| Race | <0.001 | <0.001 | |||
| White | Reference | ||||
| Black | 1.212 (1.094–1.343) | <0.001 | |||
| Others | 0.719 (0.621–0.832) | <0.001 | |||
| Grade | <0.001 | <0.001 | |||
| I | 0.720 (0.635–0.816) | <0.001 | |||
| II | 0.772 (0.717–0.831) | <0.001 | |||
| III | Reference | ||||
| Surgery | <0.001 | <0.001 | |||
| Performed | Reference | ||||
| None | 1.332 (1.148–1.546) | <0.001 | |||
| Radiation | <0.001 | <0.001 | |||
| Yes | Reference | ||||
| No | 0.775 (0.713–0.843) | <0.001 | |||
| T stage | <0.001 | <0.001 | |||
| T1 | 0.330 (0.298–0.365) | <0.001 | |||
| T2 | 0.637 (0.578–0.702) | <0.001 | |||
| T3 | 0.725 (0.646–0.814) | <0.001 | |||
| T4 | Reference | ||||
| N stage | <0.001 | <0.001 | |||
| N0 | 0.381 (0.232–0.626) | <0.001 | |||
| N1 | 0.599 (0.362–0.991) | 0.046 | |||
| N2 | 0.670 (0.404–1.112) | 0.122 | |||
| N3 | Reference | ||||
| M stage | <0.001 | <0.001 | |||
| M0 | 0.341 (0.306–0.380) | <0.001 | |||
| M1 | Reference | ||||
| Variables | Uni-Variate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| p Value | HR (95% CI) | p Value | |||
| Age | <0.001 | <0.001 | |||
| 15–45 | 0.353 (0.274–0.456) | <0.001 | |||
| 46–55 | 0.326 (0.279–0.381) | <0.001 | |||
| 56–65 | 0.363 (0.320–0.413) | <0.001 | |||
| 66–75 | 0.432 (0.383–0.487) | <0.001 | |||
| 76–85 | 0.639 (0.569–0.717) | <0.001 | |||
| 85+ | Reference | ||||
| Sex | <0.001 | 0.001 | |||
| Male | Reference | ||||
| Female | 1.137 (1.053–1.228) | 0.001 | |||
| Race | <0.001 | <0.001 | |||
| White | Reference | ||||
| Black | 1.243 (1.097–1.407) | 0.001 | |||
| Others | 0.717 (0.593–0.867) | 0.001 | |||
| Grade | <0.001 | <0.001 | |||
| I | 0.575 (0.475–0.697) | <0.001 | |||
| II | 0.676 (0.609–0.749) | <0.001 | |||
| III | Reference | ||||
| Surgery | <0.001 | <0.001 | |||
| Performed | Reference | ||||
| None | 1.538 (1.287–1.838) | <0.001 | |||
| Radiation | <0.001 | <0.001 | |||
| Yes | Reference | ||||
| No | 0.749 (0.680–0.827) | <0.001 | |||
| T stage | <0.001 | <0.001 | |||
| T1 | 0.199 (0.176–0.225) | <0.001 | |||
| T2 | 0.595 (0.533–0.663) | <0.001 | |||
| T3 | 0.702 (0.617–0.799) | <0.001 | |||
| T4 | Reference | ||||
| N stage | <0.001 | <0.001 | |||
| N0 | 0.377 (0.226–0.630) | <0.001 | |||
| N1 | 0.614 (0.365–1.034) | 0.067 | |||
| N2 | 0.700 (0.414–1.182) | 0.182 | |||
| N3 | Reference | ||||
| M stage | <0.001 | <0.001 | |||
| M0 | 0.314 (0.279–0.353) | <0.001 | |||
| M1 | Reference | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, P.; Wen, J.; Huang, X.; Wang, F. Development and Validation of Nomograms Predicting the 5- and 8-Year Overall and Cancer-Specific Survival of Bladder Cancer Patients Based on SEER Program. J. Clin. Med. 2023, 12, 1314. https://doi.org/10.3390/jcm12041314
Wen P, Wen J, Huang X, Wang F. Development and Validation of Nomograms Predicting the 5- and 8-Year Overall and Cancer-Specific Survival of Bladder Cancer Patients Based on SEER Program. Journal of Clinical Medicine. 2023; 12(4):1314. https://doi.org/10.3390/jcm12041314
Chicago/Turabian StyleWen, Peng, Jiao Wen, Xiaolong Huang, and Fengze Wang. 2023. "Development and Validation of Nomograms Predicting the 5- and 8-Year Overall and Cancer-Specific Survival of Bladder Cancer Patients Based on SEER Program" Journal of Clinical Medicine 12, no. 4: 1314. https://doi.org/10.3390/jcm12041314
APA StyleWen, P., Wen, J., Huang, X., & Wang, F. (2023). Development and Validation of Nomograms Predicting the 5- and 8-Year Overall and Cancer-Specific Survival of Bladder Cancer Patients Based on SEER Program. Journal of Clinical Medicine, 12(4), 1314. https://doi.org/10.3390/jcm12041314