
The Effects of Orthoptic Therapy on the Surgical Outcome in Children with Intermittent Exotropia: Randomised Controlled Clinical Trial

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants’ Inclusion and Exclusion Criteria for the Study
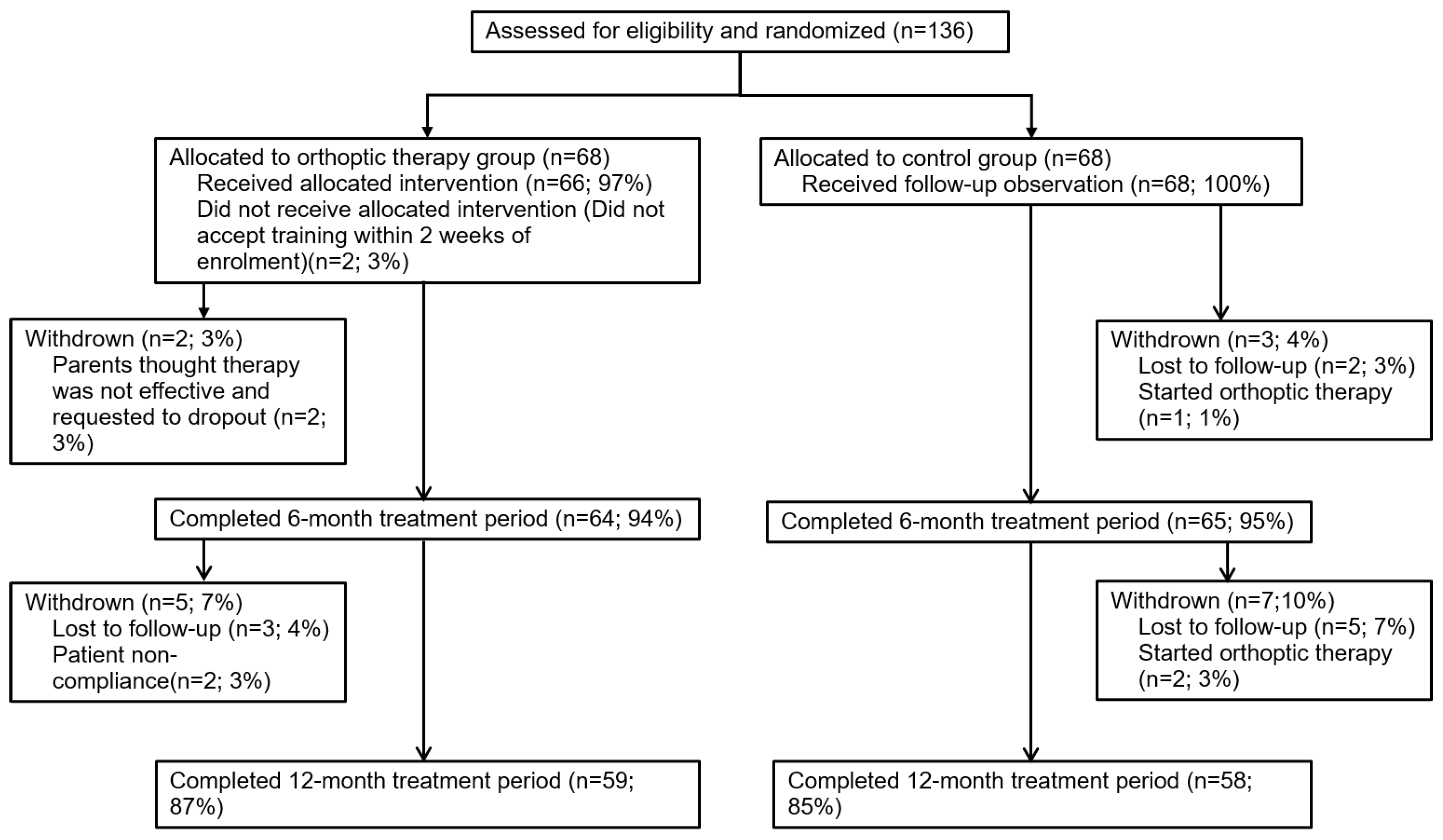
2.3. Enrolment and Randomization Grouping
2.4. Evaluations and Intervention Methods
2.5. Follow-Up Visits
2.6. Safety
2.7. Statistical Analysis
3. Results
3.1. Characteristic of Participants
3.2. Compliance of the Orthoptic Therapy Group
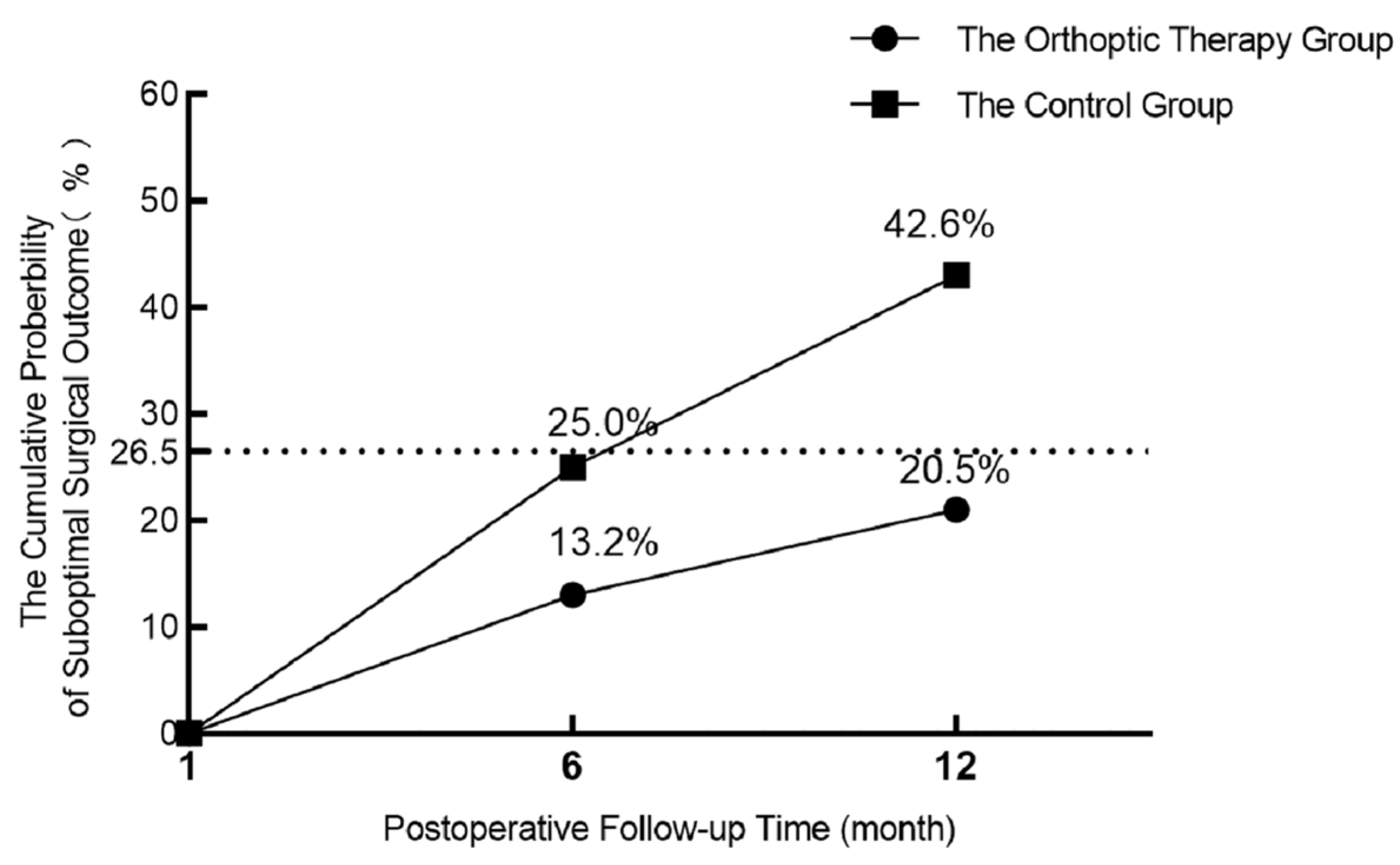
3.3. Suboptimal Surgical Outcome
3.4. Surgical Motor Alignment Success Outcome
3.5. Stereopsis
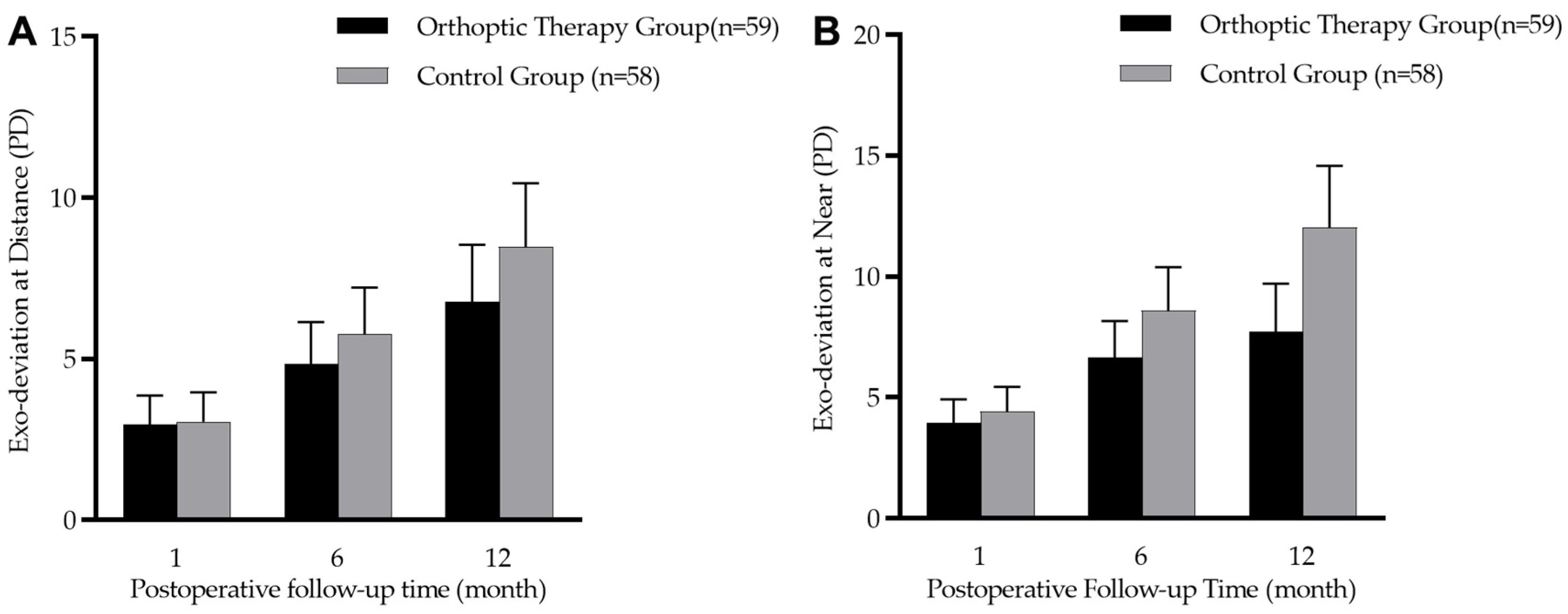
3.6. Exo-Deviation Drift
3.7. Fusional Exotropia Control
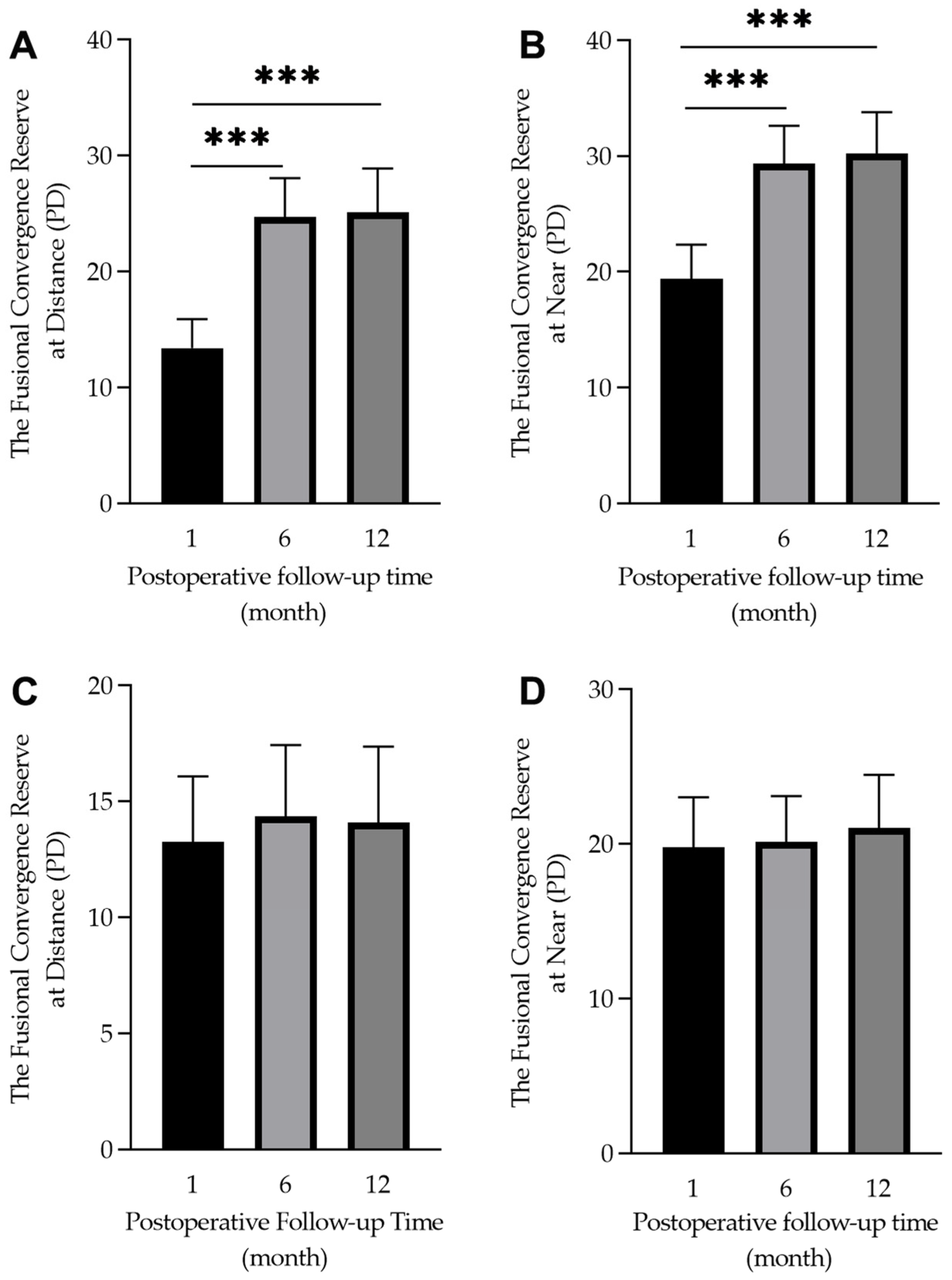
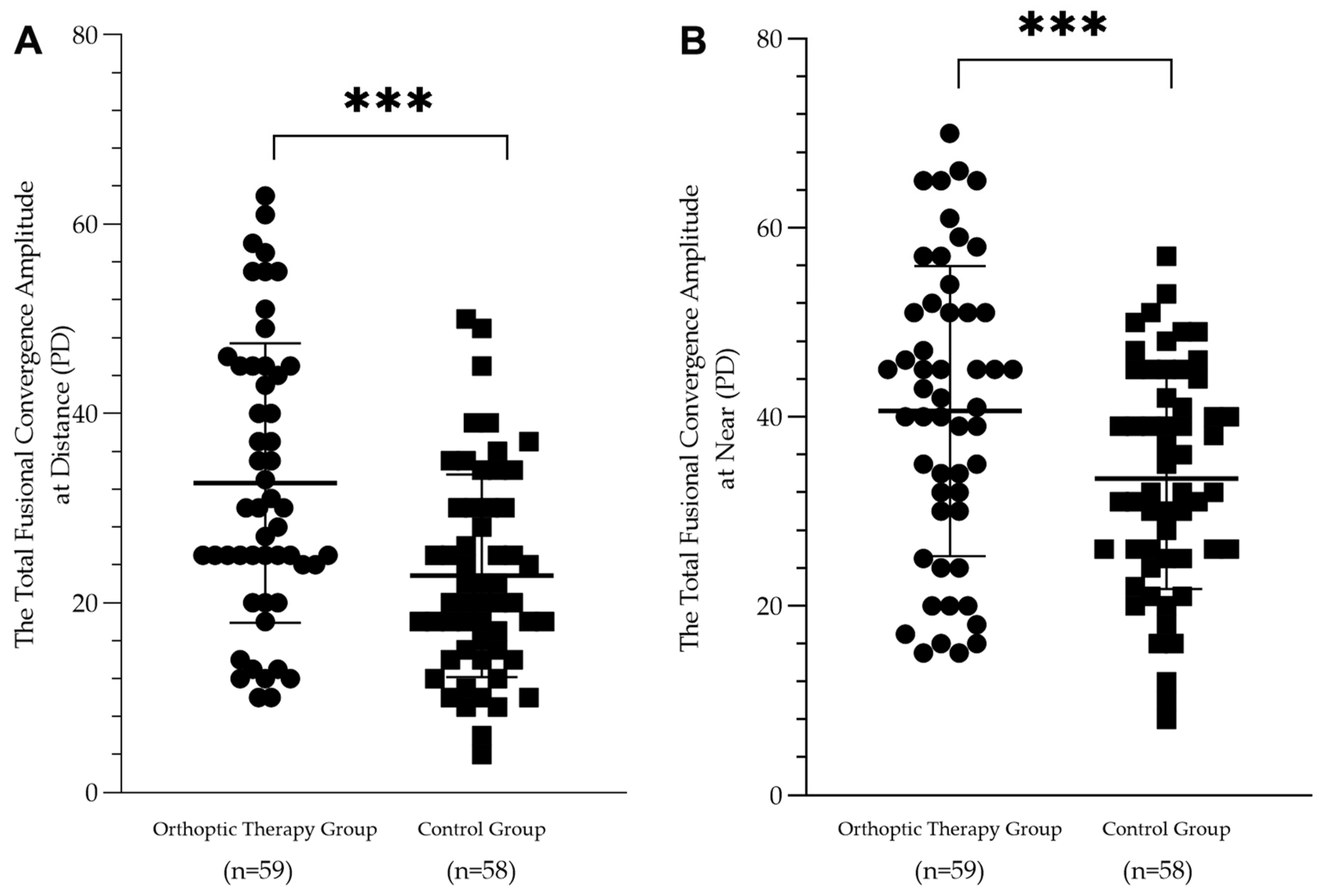
3.8. Fusional Convergence Amplitudes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Govindan, M.; Mohney, B.G.; Diehl, N.N.; Burke, J.P. Incidence and types of childhood exotropia: A population-based study. Ophthalmology 2005, 112, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Mohney, B.G. Common forms of childhood strabismus in an incidence cohort. Am. J. Ophthalmol. 2007, 144, 465–467. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.W.; Zhu, H.; Yu, J.J.; Ding, H.; Bai, J.; Chen, J.; Yu, R.B.; Liu, H. Epidemiology of Intermittent Exotropia in Preschool Children in China. Optom. Vis. Sci. 2016, 93, 57–62. [Google Scholar] [CrossRef]
- Fu, J.; Li, S.M.; Liu, L.R.; Li, J.L.; Li, S.Y.; Zhu, B.D.; Li, H.; Yang, Z.; Li, L.; Wang, N.L.; et al. Prevalence of amblyopia and strabismus in a population of 7th-grade junior high school students in Central China: The Anyang Childhood Eye Study (ACES). Ophthalmic Epidemiol. 2014, 21, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Fu, Z.; Yu, J.; Ding, H.; Bai, J.; Chen, J.; Gong, Y.; Zhu, H.; Yu, R.; Liu, H. Prevalence of amblyopia and strabismus in Eastern China: Results from screening of preschool children aged 36-72 months. Br. J. Ophthalmol. 2016, 100, 515–519. [Google Scholar] [CrossRef]
- Yamada, T.; Hatt, S.R.; Leske, D.A.; Holmes, J.M. Health-related quality of life in parents of children with intermittent exotropia. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2011, 15, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xu, M.; Yu, H.; Xu, J.; Hou, F.; Zhou, J.; Yu, X. Health-related quality of life correlated with the clinical severity of intermittent exotropia in children. Eye 2020, 34, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.M. How to Better Treat Patients with Intermittent Exotropia: A Review of Surgical Treatment of Intermittent Exotropia. Korean J. Ophthalmol. 2022, 36, 550–564. [Google Scholar] [CrossRef] [PubMed]
- Weston, B.; Enzenauer, R.W.; Kraft, S.P.; Gayowsky, G.R. Stability of the postoperative alignment in adjustable-suture strabismus surgery. J. Pediatr. Ophthalmol. Strabismus 1991, 28, 206–211. [Google Scholar] [CrossRef]
- Lee, S.; Lee, Y.C. Relationship between motor alignment at postoperative day 1 and at year 1 after symmetric and asymmetric surgery in intermittent exotropia. Jpn. J. Ophthalmol. 2001, 45, 167–171. [Google Scholar] [CrossRef]
- Oh, J.Y.; Hwang, J.M. Survival analysis of 365 patients with exotropia after surgery. Eye 2006, 20, 1268–1272. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Hong, J.S.; Kim, M.M. Prognostic factors for recurrence with unilateral recess-resect procedure in patients with intermittent exotropia. Eye 2011, 25, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Tibrewal, S.; Singh, N.; Bhuiyan, M.I.; Ganesh, S. Factors affecting residual exotropia after two muscle surgery for intermittent exotropia. Int. J. Ophthalmol. 2017, 10, 1120–1125. [Google Scholar] [PubMed]
- Pediatric Eye Disease Investigator Group; Writing, C.; Donahue, S.P.; Chandler, D.L.; Holmes, J.M.; Arthur, B.W.; Paysse, E.A.; Wallace, D.K.; Petersen, D.B.; Melia, B.M.; et al. A Randomized Trial Comparing Bilateral Lateral Rectus Recession versus Unilateral Recess and Resect for Basic-Type Intermittent Exotropia. Ophthalmology 2019, 126, 305–317. [Google Scholar]
- Lee, H.J.; Kim, S.J. Long-term outcomes following resection-recession versus plication-recession in children with intermittent exotropia. Br. J. Ophthalmol. 2020, 104, 350–356. [Google Scholar] [CrossRef]
- Hardesty, H.H.; Boynton, J.R.; Keenan, J.P. Treatment of intermittent exotropia. Arch. Ophthalmol. 1978, 96, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J. Intermittent exotropia of the divergence excess type. J. Am. Optom. Assoc. 1977, 48, 1261–1273. [Google Scholar]
- Bagolini, B.; Campos, E.C. Practical usefulness of anomalous binocular vision for the strabismic patient. Int. Ophthalmol. 1983, 6, 19–26. [Google Scholar] [CrossRef]
- Hatt, S.R.; Leske, D.A.; Mohney, B.G.; Brodsky, M.C.; Holmes, J.M. Fusional convergence in childhood intermittent exotropia. Am. J. Ophthalmol. 2011, 152, 314–319. [Google Scholar] [CrossRef]
- Yam, J.C.; Chong, G.S.; Wu, P.K.; Wong, U.S.; Chan, C.W.; Ko, S.T. A prospective study of fusional convergence parameters in Chinese patients with intermittent exotropia. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2013, 17, 347–351. [Google Scholar] [CrossRef]
- Kwok, J.J.; Chong, G.S.; Ko, S.T.; Yam, J.C. The Natural Course of Intermittent Exotropia over a 3-year Period and the Factors Predicting the Control Deterioration. Sci. Rep. 2016, 6, 27113. [Google Scholar] [CrossRef]
- Knapp, P. Intermittent exotropia: Evaluation and therapy. Am. Orthopt. J. 1953, 3, 27–33. [Google Scholar] [CrossRef]
- Figueira, E.C.; Hing, S. Intermittent exotropia: Comparison of treatments. Clin. Exp. Ophthalmol. 2006, 34, 245–251. [Google Scholar] [CrossRef]
- Ma, M.M.; Kang, Y.; Chen, C.; Su, C.; Tian, Z.; Le, M. Vision therapy for intermittent exotropia: A case series. J. Optom. 2021, 14, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Zheng, F.; Peng, Y.; Wang, C.; Lou, J.; Yu, H.; Wang, Y.; Yu, X. Effects of orthoptic therapy in children with intermittent exotropia after surgery: Study protocol for a randomized controlled trial. Trials 2022, 23, 289. [Google Scholar] [CrossRef]
- Sloper, J. Clinical Strabismus Management: Principles and Surgical Techniques. Br. J. Ophthalmol. 2000, 84, 1333. [Google Scholar] [CrossRef] [PubMed]
- Stanworth, A. Binocular Vision and Ocular Motility: Theory and Management of Strabismus. Br. J. Ophthalmol. 1975, 59, 742. [Google Scholar] [CrossRef]
- Mohney, B.G.; Holmes, J.M. An office-based scale for assessing control in intermittent exotropia. Strabismus 2006, 14, 147–150. [Google Scholar] [CrossRef]
- Convergence Insufficiency Treatment Trial Study Group. Randomized clinical trial of treatments for symptomatic convergence insufficiency in children. Arch. Ophthalmol. 2008, 126, 1336–1349. [Google Scholar]
- Yang, H.K.; Hwang, J.M. Bilateral vs unilateral medial rectus resection for recurrent exotropia after bilateral lateral rectus recession. Am. J. Ophthalmol. 2009, 148, 459–465. [Google Scholar] [CrossRef]
- Li, Y.; Ding, J.; Zhang, W. Improvement of binocular summation in intermittent exotropia following successful postoperative alignment. Sci. Rep. 2021, 11, 15584. [Google Scholar] [CrossRef]
- Feng, L.; Zhou, J.; Chen, L.; Hess, R.F. Sensory eye balance in surgically corrected intermittent exotropes with normal stereopsis. Sci. Rep. 2015, 5, 13075. [Google Scholar] [CrossRef] [PubMed]
- Hatt, S.R.; Mohney, B.G.; Leske, D.A.; Holmes, J.M. Variability of stereoacuity in intermittent exotropia. Am. J. Ophthalmol. 2008, 145, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Kushner, B.J. Selective surgery for intermittent exotropia based on distance/near differences. Arch. Ophthalmol. 1998, 116, 324–328. [Google Scholar] [CrossRef]
- Wu, H.; Sun, J.; Xia, X.; Xu, L.; Xu, X. Binocular status after surgery for constant and intermittent exotropia. Am. J. Ophthalmol. 2006, 142, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Procianoy, E.; Procianoy, L. Bilateral lateral rectus recession vs unilateral recess-resect procedure for exotropia with a dominant eye. Am. J. Ophthalmol. 2006, 142, 708–709. [Google Scholar] [CrossRef]
- Pineles, S.L.; Ela-Dalman, N.; Zvansky, A.G.; Yu, F.; Rosenbaum, A.L. Long-term results of the surgical management of intermittent exotropia. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2010, 14, 298–304. [Google Scholar] [CrossRef]
- Wang, L.; Wu, Q.; Kong, X.; Li, Z. Comparison of bilateral lateral rectus recession and unilateral recession resection for basic type intermittent exotropia in children. Br. J. Ophthalmol. 2013, 97, 870–873. [Google Scholar] [CrossRef]
- Yang, X.; Man, T.T.; Tian, Q.X.; Zhao, G.Q.; Kong, Q.L.; Meng, Y.; Gao, Y.; Ning, M.Z. Long-term postoperative outcomes of bilateral lateral rectus recession vs unilateral recession-resection for intermittent exotropia. Int. J. Ophthalmol. 2014, 7, 1043–1047. [Google Scholar]
- Christiansen, S.P.; McLoon, L.K. The effect of resection on satellite cell activity in rabbit extraocular muscle. Investig. Ophthalmol. Vis. Sci. 2006, 47, 605–613. [Google Scholar] [CrossRef]
- Christiansen, S.P.; Antunes-Foschini, R.S.; McLoon, L.K. Effects of recession versus tenotomy surgery without recession in adult rabbit extraocular muscle. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5646–5656. [Google Scholar] [CrossRef] [PubMed]
- Pullela, M.; Agaoglu, M.N.; Joshi, A.C.; Agaoglu, S.; Coats, D.K.; Das, V.E. Neural Plasticity Following Surgical Correction of Strabismus in Monkeys. Investig. Ophthalmol. Vis. Sci. 2018, 59, 5011–5021. [Google Scholar] [CrossRef] [PubMed]
- Coffey, B.; Wick, B.; Cotter, S.; Scharre, J.; Horner, D. Treatment options in intermittent exotropia: A critical appraisal. Optom. Vis. Sci. 1992, 69, 386–404. [Google Scholar] [CrossRef]
- France, L.W. The Role of Orthoptic Therapy in Exodeviations: A Basis for Orthoptic Referral. Am. Orthopt. J. 1992, 42, 52–64. [Google Scholar] [CrossRef]
- Asadi, R.; Falavarjani, K.; Sadighi, N. Orthoptic Treatment in the Management of Intermittent Exotropia. Iran. J. Ophthalmol. 2009, 21, 35–40. [Google Scholar]
- Pang, Y.; Gnanaraj, L.; Gayleard, J.; Han, G.; Hatt, S.R. Interventions for intermittent exotropia. Cochrane Database Syst. Rev. 2021, 9, CD003737. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | OTG (n = 68) | CG (n = 68) | p Value | |
|---|---|---|---|---|
| Preoperative | ||||
| Sex (F:M) | 30:38 | 36:32 | 0.954 | |
| Age, y, mean (SD) | 10.2 (2.6) | 10.6 (2.4) | 0.340 | |
| Height, cm, mean (SD) | 142.6 ± 15.2 | 145.2 ± 13.7 | 0.298 | |
| Weight, Kg, mean (SD) | 37.1 ± 14.0 | 38.6 ± 11.6 | 0.470 | |
| SER, D, mean (SD) | OD | −1.1 ± 1.3 | −1.6 ± 1.6 | 0.036 |
| OS | −1.1 ± 1.4 | −1.5 ± 1.5 | 0.089 | |
| Exo-deviation, PD, mean (SD) | Distance | −33.3 ± 10.9 | −33.9 ± 9.9 | 0.738 |
| Near | −37.3 ± 10.5 | −38.4 ± 10.2 | 0.554 | |
| R&R:BLRc:ULRc | 53:14:1 | 43:22:3 | 0.148 | |
| Stereopsis (logarcsec) | Distance | 2.7 ± 0.3 | 2.8 ± 0.2 | 0.200 |
| Near | 2.4 ± 0.4 | 2.3 ± 0.4 | 0.159 | |
| Post-operative | ||||
| Fusional convergence reserve (PD) | Distance | 13.4 ± 10.2 | 13.2 ± 11.7 | 0.942 |
| Near | 19.4 ± 12.1 | 19.7 ± 13.4 | 0.878 | |
| Deviation (PD) | Distance | −2.9 ± 3.7 | −3.1 ± 3.7 | 0.890 |
| Near | −3.9 ± 3.9 | −4.4 ± 4.2 | 0.504 | |
| Stereopsis (logarcsec) | Distance | 2.5 ± 0.4 | 2.5 ± 0.4 | 0.718 |
| Near | 2.1 ± 0.3 | 2.2 ± 0.3 | 0.735 | |
| Characteristic | Completed (n = 117) | Missed (n = 19) | p Value | |
|---|---|---|---|---|
| Preoperative | ||||
| Sex (F:M) | 57:60 | 9:10 | 0.913 | |
| Age, y, mean (SD) | 10.2 ± 2.5 | 11.3 ± 2.3 | 0.065 | |
| Height, cm, mean (SD) | 142.6 ± 15.2 | 142.9 ± 14.3 | 0.048 | |
| Weight, Kg, mean (SD) | 37.1 ± 14.0 | 37.5 ± 13.1 | 0.346 | |
| SER, D, mean (SD) | OD | −1.3 ± 1.5 | −1.0 ± 1.1 | 0.461 |
| OS | −1.3 ± 1.5 | −1.1 ± 1.3 | 0.567 | |
| Exo-deviation, PD, mean (SD) | Distance | −34.1 ± 9.6 | −35.0 ± 9.7 | 0.602 |
| Near | −38.5 ± 9.4 | −39.1 ± 9.9 | 0.645 | |
| Stereoacuity (logarcsec) | Distance | 3.7 ± 0.6 | 3.8 ± 0.5 | 0.526 |
| Near | 2.3 ± 0.4 | 2.3 ± 0.5 | 0.461 | |
| Post-operative | ||||
| Fusional convergence reserve (PD) | Distance | 13.5 ± 11.1 | 11.6 ± 10.1 | 0.522 |
| Near | 19.6 ± 12.7 | 19.4 ± 13.1 | 0.942 | |
| Deviation (PD) | Distance | −3.1 ± 3.7 | −2.1 ± 3.3 | 0.271 |
| Near | −4.2 ± 4.1 | −3.7 ± 3.7 | 0.618 | |
| Stereoacuity (logarcsec) | Distance | 2.5 ± 0.4 | 2.5 ± 0.3 | 0.794 |
| Near | 2.1 ± 0.3 | 2.2 ± 0.3 | 0.318 | |
| 6 Months | 12 Months | Total | ||||
|---|---|---|---|---|---|---|
| OTG | CG | OTG | CG | OTG | CG | |
| No. at risk | 68 | 68 | 59 | 51 | N/A | N/A |
| No. with suboptimal surgical outcome | 9 | 17 | 5 | 12 | 14 | 29 |
| Constant XT | 5 | 11 | 4 | 10 | 9 | 21 |
| Stereo loss | 3 | 4 | 1 | 2 | 4 | 6 |
| Constant XT and Stereo loss | 1 | 2 | 0 | 0 | 1 | 2 |
| Cumulative probability of suboptimal surgical outcome (%) | 13.2 | 25 | 20.5 | 42.6 | N/A | N/A |
| Parameters | The Orthoptic Therapy Group | The Control Group | |||||
|---|---|---|---|---|---|---|---|
| 1 Month (n = 68) | 6 Months (n = 64) | 12 Months (n = 59) | 1 Month (n = 68) | 6 Months (n = 65) | 12 Months (n = 58) | ||
| DRS | Good | 12 | 27 | 21 | 13 | 13 | 13 |
| Moderate | 20 | 27 | 31 | 21 | 30 | 26 | |
| Nil | 36 | 10 | 7 | 34 | 22 | 19 | |
| TNO | Good | 14 | 29 | 27 | 14 | 17 | 21 |
| Moderate | 48 | 32 | 32 | 52 | 46 | 37 | |
| Nil | 6 | 3 | 0 | 2 | 2 | 0 | |
| Distance | Near | |||
|---|---|---|---|---|
| Fusional Exotropia Control Score | OTG n (%) | CG n (%) | OTG n (%) | CG n (%) |
| (0) No exotropia unless dissociated, recovers <1 s (phoria) | 35 (59.3) | 25 (43.1) | 32 (54.2) | 24 (41.4) |
| (1) No exotropia unless dissociated, recovers 1–5 s | 12 (20.3) | 12 (20.7) | 17 (28.8) | 14 (24.1) |
| (2) No exotropia unless dissociated, recovers >5 s | 5 (8.5) | 4 (6.9) | 6 (10.2) | 3 (5.2) |
| (3) Exotropia <50% of 30-s observation | 5 (8.5) | 4 (6.9) | 3 (5.1) | 12 (20.7) |
| (4) Exotropia >50% of 30-s observation | 2 (3.4) | 7 (12.1) | 1 (1.7) | 4 (6.9) |
| (5) Constant exotropia | 6 (10.3) | 1 (1.7) | ||
| Mean (SD) | 0.7 (1.1) | 1.5 (1.8) | 0.7 (0.9) | 1.3 (1.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, M.; Peng, Y.; Zheng, F.; Yu, H.; Zhou, J.; Zheng, J.; Wang, Y.; Hou, F.; Yu, X. The Effects of Orthoptic Therapy on the Surgical Outcome in Children with Intermittent Exotropia: Randomised Controlled Clinical Trial. J. Clin. Med. 2023, 12, 1283. https://doi.org/10.3390/jcm12041283
Xu M, Peng Y, Zheng F, Yu H, Zhou J, Zheng J, Wang Y, Hou F, Yu X. The Effects of Orthoptic Therapy on the Surgical Outcome in Children with Intermittent Exotropia: Randomised Controlled Clinical Trial. Journal of Clinical Medicine. 2023; 12(4):1283. https://doi.org/10.3390/jcm12041283
Chicago/Turabian StyleXu, Meiping, Yiyi Peng, Fuhao Zheng, Huanyun Yu, Jiawei Zhou, Jingwei Zheng, Yuwen Wang, Fang Hou, and Xinping Yu. 2023. "The Effects of Orthoptic Therapy on the Surgical Outcome in Children with Intermittent Exotropia: Randomised Controlled Clinical Trial" Journal of Clinical Medicine 12, no. 4: 1283. https://doi.org/10.3390/jcm12041283
APA StyleXu, M., Peng, Y., Zheng, F., Yu, H., Zhou, J., Zheng, J., Wang, Y., Hou, F., & Yu, X. (2023). The Effects of Orthoptic Therapy on the Surgical Outcome in Children with Intermittent Exotropia: Randomised Controlled Clinical Trial. Journal of Clinical Medicine, 12(4), 1283. https://doi.org/10.3390/jcm12041283