

A Clinical Prediction Rule for Thrombosis in Critically Ill COVID-19 Patients: Step 1 Results of the Thromcco Study
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Source of Data
2.3. Participants
2.4. Variables
2.5. Statistical Analysis and Predictors
3. Results
3.1. Patient Characteristics
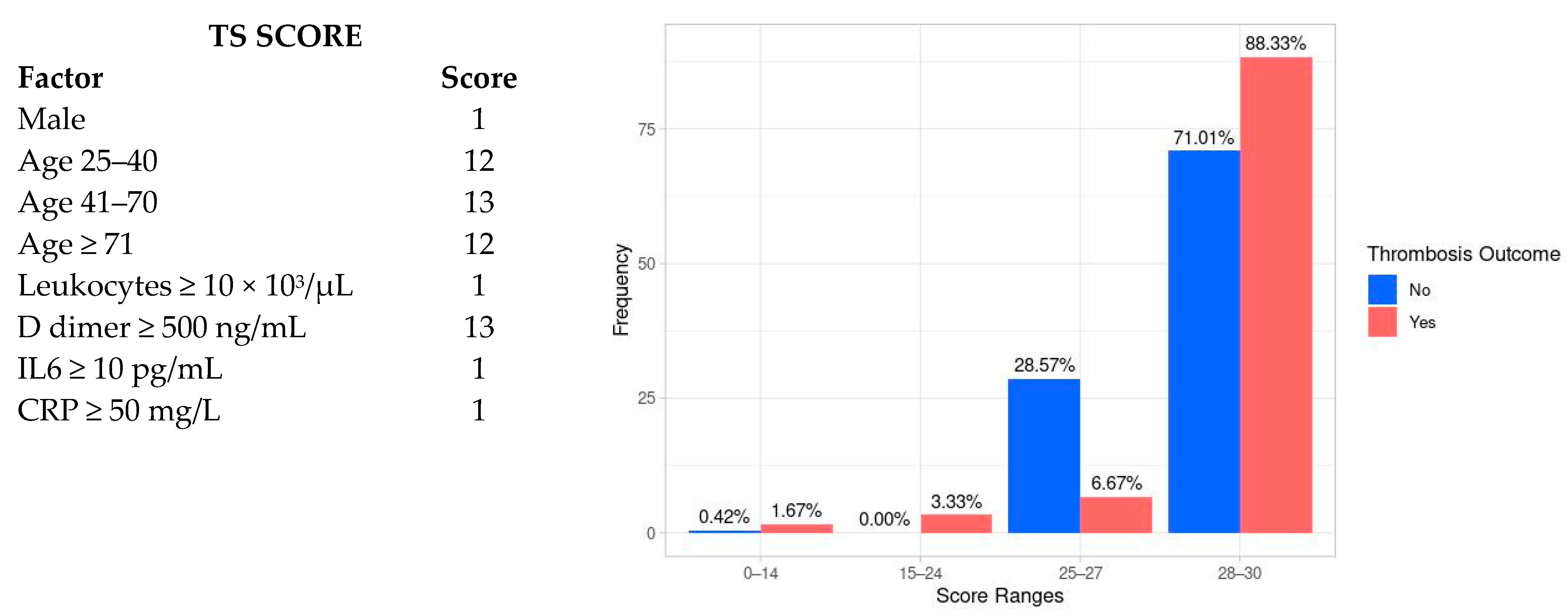
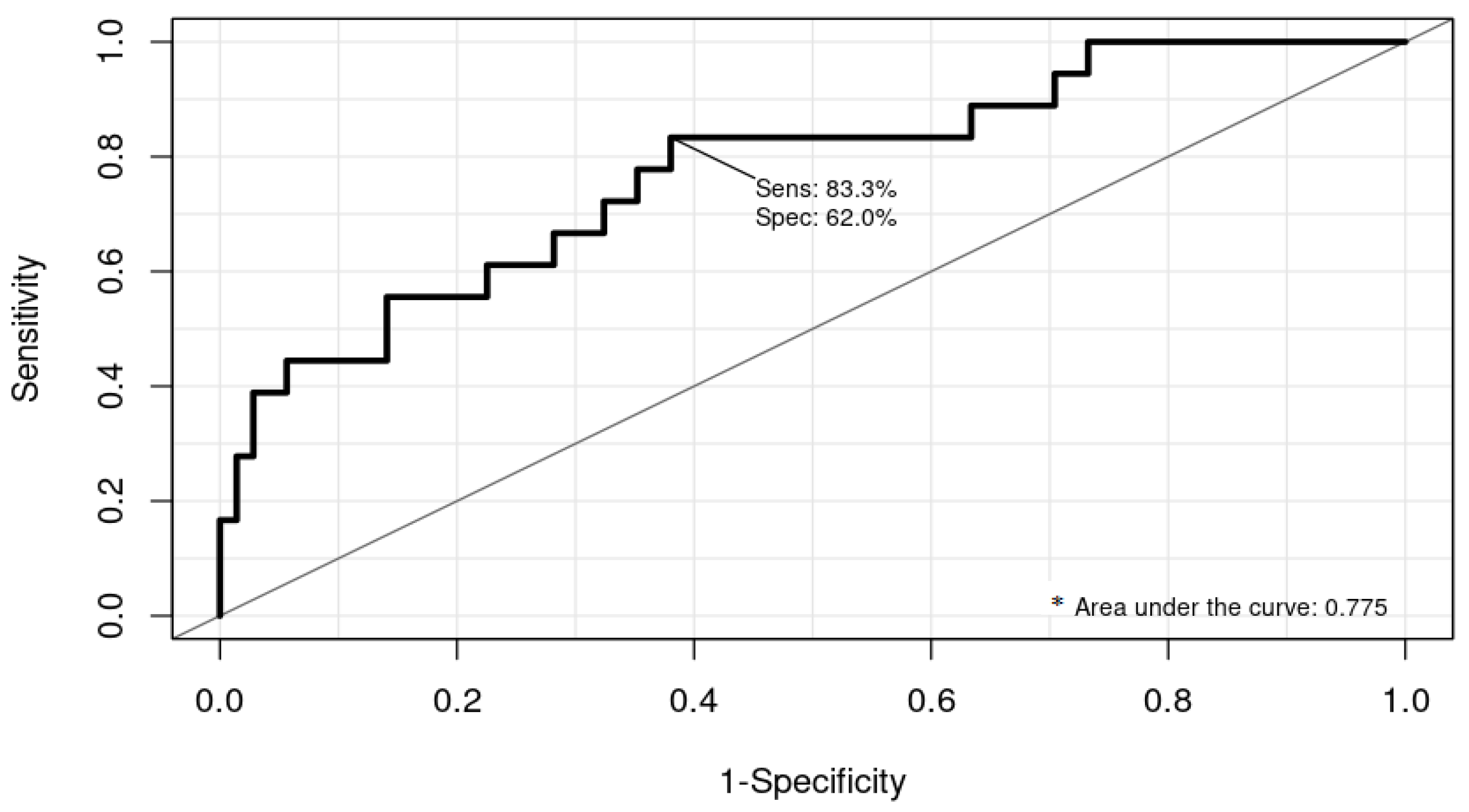
3.2. Risk Prediction Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Suh, Y.J.; Hong, H.; Ohana, M.; Bompard, F.; Revel, M.-P.; Valle, C.; Gervaise, A.; Poissy, J.; Susen, S.; Hékimian, G.; et al. Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and Meta-Analysis. Radiology 2021, 298, E70–E80. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.; Tang, F.; Chen, L.; Gao, H.; Li, X. Cumulative Evidence for the Association of Thrombosis and the Prognosis of COVID-19: Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2021, 8, 2188. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Chi, J.; Gao, Q. Prevalence and risk factors of thrombotic events on patients with COVID-19: A systematic review and meta-analysis. Thromb. J. 2021, 19, 32. [Google Scholar] [CrossRef] [PubMed]
- Law, N.; Chan, J.; Kelly, C.; Auffermann, W.F.; Dunn, D.P. Incidence of pulmonary embolism in COVID-19 infection in the ED: Ancestral, Delta, Omicron variants and vaccines. Emerg. Radiol. 2022, 29, 625–629. [Google Scholar] [CrossRef] [PubMed]
- di Gennaro, C.; Galdiero, M.; Scherillo, G.; Parlamento, S.; Poggiano, M.R.; Arturo, C.; Vasta, A.; Giordano, B.; Pisano, V.; Lobasso, A.; et al. Editorial COVID-19 and Thrombosis 2023: New Waves of SARS-CoV-2 Infection, Triage Organization in Emergency Department and the Association of VOCs/VOI with Pulmonary Embolism. Viruses 2022, 14, 2453. [Google Scholar] [CrossRef] [PubMed]
- Korevaar, D.A.; Aydemir, I.; Minnema, M.W.; Azijli, K.; Beenen, L.F.; Heijmans, J.; van Es, N.; al Masoudi, M.; Meijboom, L.J.; Middeldorp, S.; et al. Routine screening for pulmonary embolism in COVID-19 patients at the emergency department: Impact of D-dimer testing followed by CTPA. J. Thromb. Thrombolysis 2021, 52, 1068–1073. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, D.; García-Sanchez, A.; Rali, P.; Muriel, A.; Bikdeli, B.; Ruiz-Artacho, P.; Le Mao, R.; Rodríguez, C.; Hunt, B.J.; Monreal, M. Incidence of VTE and Bleeding Among Hospitalized Patients With Coronavirus Disease 2019. Chest 2021, 159, 1182–1196. [Google Scholar] [CrossRef] [PubMed]
- Grillet, F.; Behr, J.; Calame, P.; Aubry, S.; Delabrousse, E. Acute Pulmonary Embolism Associated with COVID-19 Pneumonia Detected with Pulmonary CT Angiography. Radiology 2020, 296, E186–E188. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Kruisman, E.; Spaan, J.; Nijkeuter, M.; Righini, M.; Aujesky, D.; Roy, P.M.; Perrier, A.; LE Gal, G.; Huisman, M.V. Comparison of the revised Geneva score with the Wells rule for assessing clinical probability of pulmonary embolism. J. Thromb. Haemost. 2008, 6, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Ceriani, E.; Combescure, C.; LE Gal, G.; Nendaz, M.; Perneger, T.; Bounameaux, H.; Perrier, A.; Righini, M. Clinical prediction rules for pulmonary embolism: A systematic review and meta-analysis. J. Thromb. Haemost. 2010, 8, 957–970. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, B.; Aziz, M.; Kumar, S.; Burke, M.; Webster, T.; Immadi, A.; Sam, M.; Lal, A.; Estrada-Y-Martin, R.M.; Cherian, S.; et al. Wells Score to Predict Pulmonary Embolism in Patients with Coronavirus Disease 2019. Am. J. Med. 2021, 134, 688–690. [Google Scholar] [CrossRef] [PubMed]
- Salas, E.; Farm, M.; Pich, S.; Onelöv, L.; Guillen, K.; Ortega, I.; Antovic, J.P.; Soria, J.M. Predictive Ability of a Clinical-Genetic Risk Score for Venous Thromboembolism in Northern and Southern European Populations. TH Open 2021, 05, e303–e311. [Google Scholar] [CrossRef] [PubMed]
- Porfidia, A.; Mosoni, C.; Talerico, R.; Porceddu, E.; Lupascu, A.; Tondi, P.; Landi, F.; Pola, R. Pulmonary Embolism in COVID-19 Patients: Which Diagnostic Algorithm Should We Use? Front. Cardiovasc. Med. 2021, 8, 714003. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhang, H.; Khanal, M.K. Development of scoring system for risk stratification in clinical medicine: A step-by-step tutorial. Ann. Transl. Med. 2017, 5, 436. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD Statement. Eur. Urol. 2015, 67, 1142–1151. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Jehangir, Q.; Lin, C.-H.; Li, P.; Sule, A.A.; Poisson, L.; Balijepally, V.; Halabi, A.R.; Patel, K.; Krishnamoorthy, G.; et al. 3D-PAST: Risk Assessment Model for Predicting Venous Thromboembolism in COVID-19. J. Clin. Med. 2022, 11, 3949. [Google Scholar] [CrossRef]
- Linkins, L.-A.; Bates, S.M.; Ginsberg, J.S.; Kearon, C. Use of different D-dimer levels to exclude venous thromboembolism depending on clinical pretest probability. J. Thromb. Haemost. 2004, 2, 1256–1260. [Google Scholar] [CrossRef] [PubMed]
- Quintana-Díaz, M.; Andrés-Esteban, E.M.; Ramírez-Cervantes, K.L.; Olivan-Blázquez, B.; Juárez-Vela, R.; Gea-Caballero, V. Coagulation Parameters: An Efficient Measure for Predicting the Prognosis and Clinical Management of Patients with COVID-19. J. Clin. Med. 2020, 9, 3482. [Google Scholar] [CrossRef] [PubMed]
- FaFarouk, N.; Ashry, W.M.O.; El-Hagrasy, H.A.; Mohamed, E.F.; Eltrawy, H.H.; El-Nasser, A.M.; Shipl, W.; El Attar, S.; Sakr, L.K.; Wahab, M.A.A.; et al. Admission Levels of Serum P-Selectin and IL-6 Can Predict Development of Deep Venous Thrombosis in Hospitalized Covid-19 Patients. Int. J. Gen. Med. 2022, 15, 5599–5607. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-reactive protein and clinical outcomes in patients with COVID-19. Eur. Heart J. 2021, 42, 2270–2279. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Age, Years, Median | 62.4 (IQR 51.5–70) |
| Sex | % (n) |
| Female | 28.1 (84) |
| Male | 79.9 (215) |
| Race | |
| Caucasian | 51.6 (154) |
| Latin American | 11 (33) |
| Asian | 0.3 (1) |
| African | 1 (3) |
| Arabic | 2.7 (8) |
| Unknown | 33.4 (100) |
| Smoking habit | 3.3 (10) |
| Comorbidities at hospital admission | |
| Hypertension | 40.8 (122) |
| Diabetes | 22.7 (68) |
| Asthma | 3 (9) |
| COPD | 4 (12) |
| Ischemic heart disease | 6.7 (20) |
| Valvular heart disease | 1 (3) |
| Auricular fibrillation | 3 (9) |
| Obesity | 36.1 (108) |
| Class 1 | 23.4 (70) |
| Class 2 | 8.7 (26) |
| Class 3 | 4 (12) |
| Hospitalization | Median (IQR) |
| Days from COVID-19 symptoms onset to hospital admission | 7 (5–9) |
| Length of hospital stay, days | 28 (18–42) |
| Time from hospital admission to ICU admission, days | 2 (0–5) |
| Length of ICU stay, days | 14 (7–28) |
| Blood tests results | |
| D-dimer | 1676 (779–4084) |
| Fibrinogen | 719 (608–861) |
| Leucocytes | 8.2 (IQR 5.6–12.4) |
| Lymphocytes | 0.6 (0.4–0.95) |
| Platelets | 201 (147–259) |
| Ferritin | 974 (482.1–1634) |
| C-reactive protein | 126 (69.6–207.6) |
| Prothrombin time (PT) | 12.9 (11.9–15.6) |
| IL6 | 71.3 (36.5–167.8) |
| Creatinine | 0.83 (0.68–1.23) |
| Procalcitonin | 0.25 (0.13–0.75) |
| Lactate dehydrogenase | 493.2 (315.5–734.5) |
| Aspartate dehydrogenase | 49 (30.1–80.2) |
| Alanine transaminase | 37.6 (22–71.2) |
| Doppler ultrasounds of the lower limb veins | 77.5 (232) |
| Thrombosis | 20.06 (60) |
| Deep vein thrombosis (DVT) | 10.6 (31) |
| Pulmonary embolism (PE) | 3.67 (11) |
| DVT + PE | 5.01 (15) |
| Stroke + DVT | 0.33 (1) |
| Stroke | 0.66 (2) |
| Anticoagulant therapy received | % (n) |
| Prophylactic-dose anticoagulation | 44.1 (132) |
| Intermediate-dose anticoagulation | 9.03 (27) |
| Therapeutic-dose anticoagulation | 23.4 (70) |
| Bleeding | 5 (15) |
| Transfusions | |
| Transfusion of blood components | 30.4 (91) |
| Platelet’s transfusion | 7 (21) |
| Fresh-frozen plasma transfusion | 5 (15) |
| ICU | |
| Noninvasive mechanical ventilation | 58.5 (175) |
| Invasive mechanical ventilation | 70.9 (212) |
| Tracheotomy | 47.2 (141) |
| Prone positions | 59.2 (177) |
| Sepsis | 15.4 (46) |
| Deaths | 29 (87) |
| Thrombosis n = 60 * | No Thrombosis n = 239 | |||
|---|---|---|---|---|
| Median (IQR) | Median (IQR) | Median Difference (95% CI) | p-Value | |
| Age, years | 60 (51–65.9) | 63.2 (53–72) | −2.3 (−5.5–0.95) | 0.043 |
| Blood test results | ||||
| D-dimer | 1859.5 (1151–5970) | 1605 (772–3335) | 280 (−2039.3–2600.8) | 0.786 |
| Fibrinogen | 813 (567–1020) | 781 (625–903) | 27.2 (−38.1–92.6) | 0.410 |
| Leucocytes | 7.85 (5.2–12.1) | 7.30 (5.32–10.3) | 0.39 (−1.50–0.79) | 0.527 |
| Lymphocytes | 0.77 (0.47–1.2) | 0.70(0.40–1.0) | −0.02 (−0.17–0.10) | 0.511 |
| Platelets | 239 (173–283) | 210 (160–274) | 2.6 (−24.9–30.21) | 0.851 |
| Ferritin | 1006.5 (528–1573.2) | 925.4 (474–1634) | 138.5 (−624.6–901.8) | 0.721 |
| C-reactive protein | 120.1 (64.7–277.4) | 128.7 (82.4–206.7) | 7.32 (−26.5–41.1) | 0.668 |
| Prothrombin time | 13.1 (12–16.1) | 13.4 (11.9–58) | 3.5 (−10.9–3.07) | 0.268 |
| IL6 | 95.2 (42–238.2) | 71.1 (38–167.8) | 10.5 (−73.3–94.4) | 0.803 |
| Creatinine | 0.86 (0.62–1.01) | 0.82 (0.69–1.2) | 0.07 (−0.11–0.25) | 0.479 |
| Procalcitonin | 0.25 (0.14–1.08) | 0.22 (0.09–0.53) | −0.045 (−0.137–0.030) | 0.303 |
| Lactate dehydrogenase | 392 (325–557) | 384 (301–559) | −12 (−63.9–39) | 0.665 |
| Aspartate dehydrogenase | 49.5 (32.5–70.8) | 43.5 (29.8–74) | −7.7 (−15.000–13.0) | 0.995 |
| Alanine transaminase | 43 (29–75) | 41 (24.8–72.5) | −3.0 (−17.0–9.0) | 0.566 |
| Hospitalization | ||||
| Days from COVID-19 onset to hospital admission | 6 (4–7) | 7 (IQR 5–10) | −1.5 (−3.8–1.1) | 0.139 |
| Length of hospital stay, days | 35.5 (25–53) | 27 (17–37) | 10 (2.1–17.9) | 0.013 |
| Length of ICU stay | 27.5 (15–40) | 12 (7–24) | 12.8 (5.8–19.9) | 0.001 |
| % (n) | % (n) | Crude OR (95% CI) | ||
| Gender | ||||
| Male | 82 (49) | 69 (166) | 1.95 (0.96–3.98) | 0.060 |
| Female | 18 (11) | 31 (73) | ||
| Race | ||||
| Caucasian | 56.6 (34) | 50.2 (120) | ||
| Latin American | 13.3 (8) | 10.4 (25) | 0.88 (0.36–2.14) | 0.819 |
| Lifestyle habits | ||||
| Smoker | 3.3 (2) | 3.3 (8) | 0.97 (0.18–4.45) | 0.914 |
| Previous comorbidities | ||||
| Hypertension | 50 (30) | 38.4 (92) | 1.4 (0.81–2.6) | 0.203 |
| Diabetes mellitus | 21.6 (13) | 23 (55) | 0.82 (0.41–1.6) | 0.578 |
| Asthma | 0 (0) | 3.7 (9) | 0.79 (0.74–0.84) | 0.127 |
| COPD | 5 (3) | 3.7 (9) | 1.3 (0.35–5.1) | 0.712 |
| Ischemic heart disease | 3.3 (2) | 7.5 (18) | 0.42 (0.09–1.8) | 0.386 |
| Valvular heart disease | 1.6 (1) | 0.83 (2) | 2.0 (0.17–22.5) | 0.491 |
| Auricular fibrillation | 1.6 (1) | 3.3 (8) | 0.48 (0.06–3.9) | 0.693 |
| Obesity | 38.3 (23) | 35.1 (84) | 0.96 (0.53–1.75) | 0.911 |
| Class 1 | 25 (15) | 23 (55) | 0.95 (0.48–1.86) | 0.894 |
| Class 2 | 11.6 (7) | 7.9 (19) | 1.28 (0.50–3.32) | 0.598 |
| Class 3 | 1.6 (1) | 4.6 (11) | 0.31 (0.04–2.55) | 0.257 |
| Bleeding | 16.3 (8) | 3.8 (7) | 4.9 (1.7–14.5) | 0.004 |
| Transfusions | ||||
| Transfusion of blood components | 50 (30) | 25.5 (61) | 2.9 (1.62–5.23) | 0.000 |
| Platelet’s transfusion | 13.3 (8) | 5.4 (13) | 2.6 (1.05–6.78) | 0.032 |
| Fresh-frozen plasma transfusion | 8.3 (5) | 4.1 (10) | 2.0 (0.68–6.33) | 0.188 |
| ICU management | ||||
| Noninvasive mechanical ventilation | 60 (36) | 58.1 (139) | 1.09 (0.60–1.97) | 0.764 |
| Invasive mechanical ventilation | 88.3 (53) | 66.5 (159) | 3.8 (1.65–8.76) | 0.001 |
| Tracheotomy | 60 (36) | 43.9 (105) | 1.9 (1.06–3.38) | 0.028 |
| Prone positions | 81.6 (49) | 53.5 (128) | 3.8 (1.79–8.18) | 0.000 |
| Sepsis | 33.3 (20) | 17.9 (43) | 3.06 (1.46–6.39) | 0.002 |
| Deaths | 38.3 (23) | 26.7 (64) | 1.70 (0.93–3.07) | 0.078 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez Cervantes, K.L.; Mora, E.; Campillo Morales, S.; Huerta Álvarez, C.; Marcos Neira, P.; Nanwani Nanwani, K.L.; Serrano Lázaro, A.; Silva Obregón, J.A.; Quintana Díaz, M. A Clinical Prediction Rule for Thrombosis in Critically Ill COVID-19 Patients: Step 1 Results of the Thromcco Study. J. Clin. Med. 2023, 12, 1253. https://doi.org/10.3390/jcm12041253
Ramírez Cervantes KL, Mora E, Campillo Morales S, Huerta Álvarez C, Marcos Neira P, Nanwani Nanwani KL, Serrano Lázaro A, Silva Obregón JA, Quintana Díaz M. A Clinical Prediction Rule for Thrombosis in Critically Ill COVID-19 Patients: Step 1 Results of the Thromcco Study. Journal of Clinical Medicine. 2023; 12(4):1253. https://doi.org/10.3390/jcm12041253
Chicago/Turabian StyleRamírez Cervantes, Karen L., Elianne Mora, Salvador Campillo Morales, Consuelo Huerta Álvarez, Pilar Marcos Neira, Kapil Laxman Nanwani Nanwani, Ainhoa Serrano Lázaro, J. Alberto Silva Obregón, and Manuel Quintana Díaz. 2023. "A Clinical Prediction Rule for Thrombosis in Critically Ill COVID-19 Patients: Step 1 Results of the Thromcco Study" Journal of Clinical Medicine 12, no. 4: 1253. https://doi.org/10.3390/jcm12041253
APA StyleRamírez Cervantes, K. L., Mora, E., Campillo Morales, S., Huerta Álvarez, C., Marcos Neira, P., Nanwani Nanwani, K. L., Serrano Lázaro, A., Silva Obregón, J. A., & Quintana Díaz, M. (2023). A Clinical Prediction Rule for Thrombosis in Critically Ill COVID-19 Patients: Step 1 Results of the Thromcco Study. Journal of Clinical Medicine, 12(4), 1253. https://doi.org/10.3390/jcm12041253