
K-Wire Osteosynthesis for Arthrodesis of the Paediatric Foot Is a Good and Valid Procedure

 and
and
Abstract
:1. Introduction
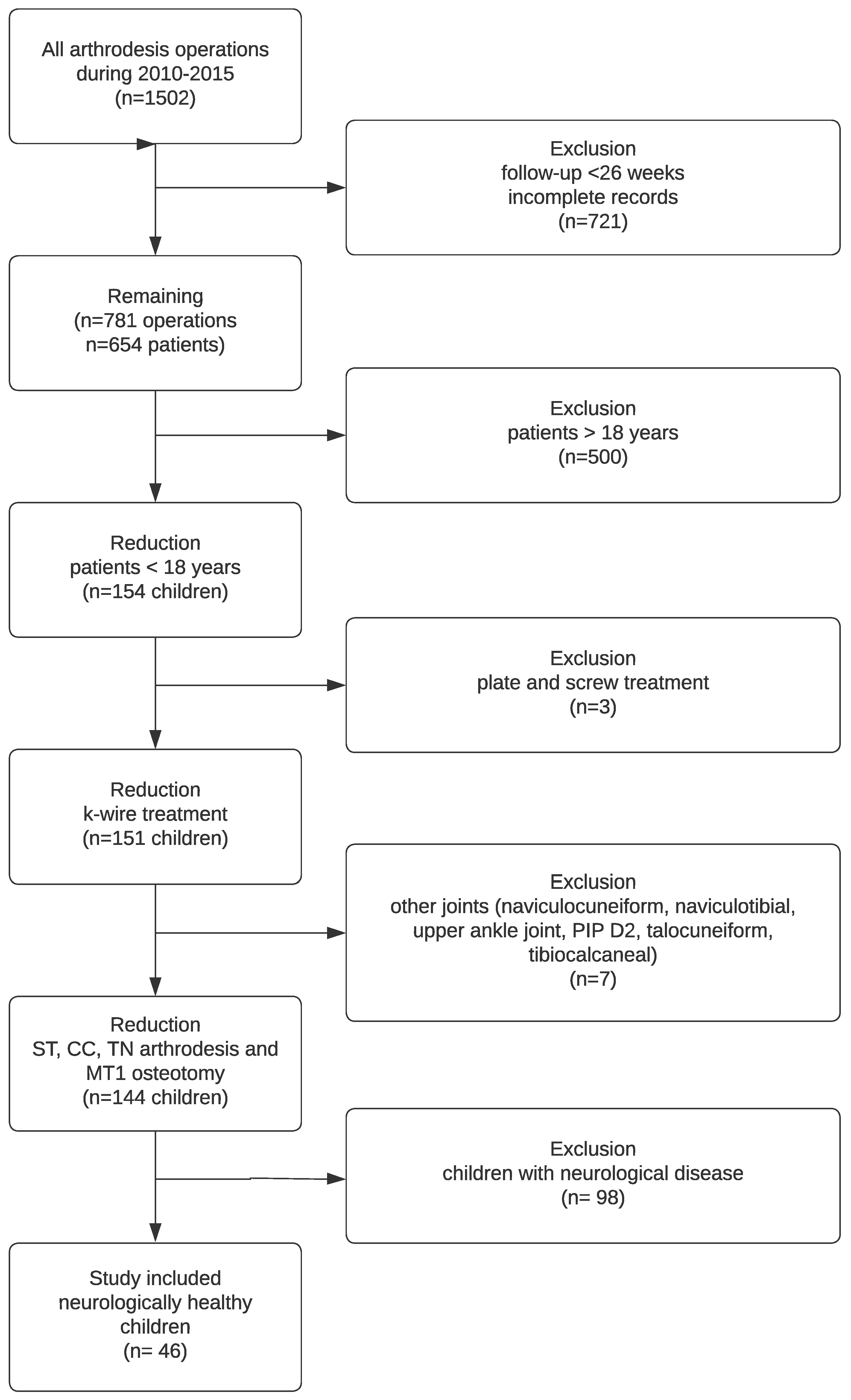
2. Materials and Methods
2.1. Operative Procedure
2.2. Clubfoot
2.3. Pes Cavovarus
2.4. Pes Planovalgus
2.4.1. Modified Evans Procedure
2.4.2. Calcaneocuboid Distraction-Fusion
2.4.3. Grice Procedure
2.4.4. Triple Fusion
2.4.5. Skewfoot
2.4.6. Pes Equinus
2.4.7. Pes Calcaneus
2.4.8. Hallux Valgus
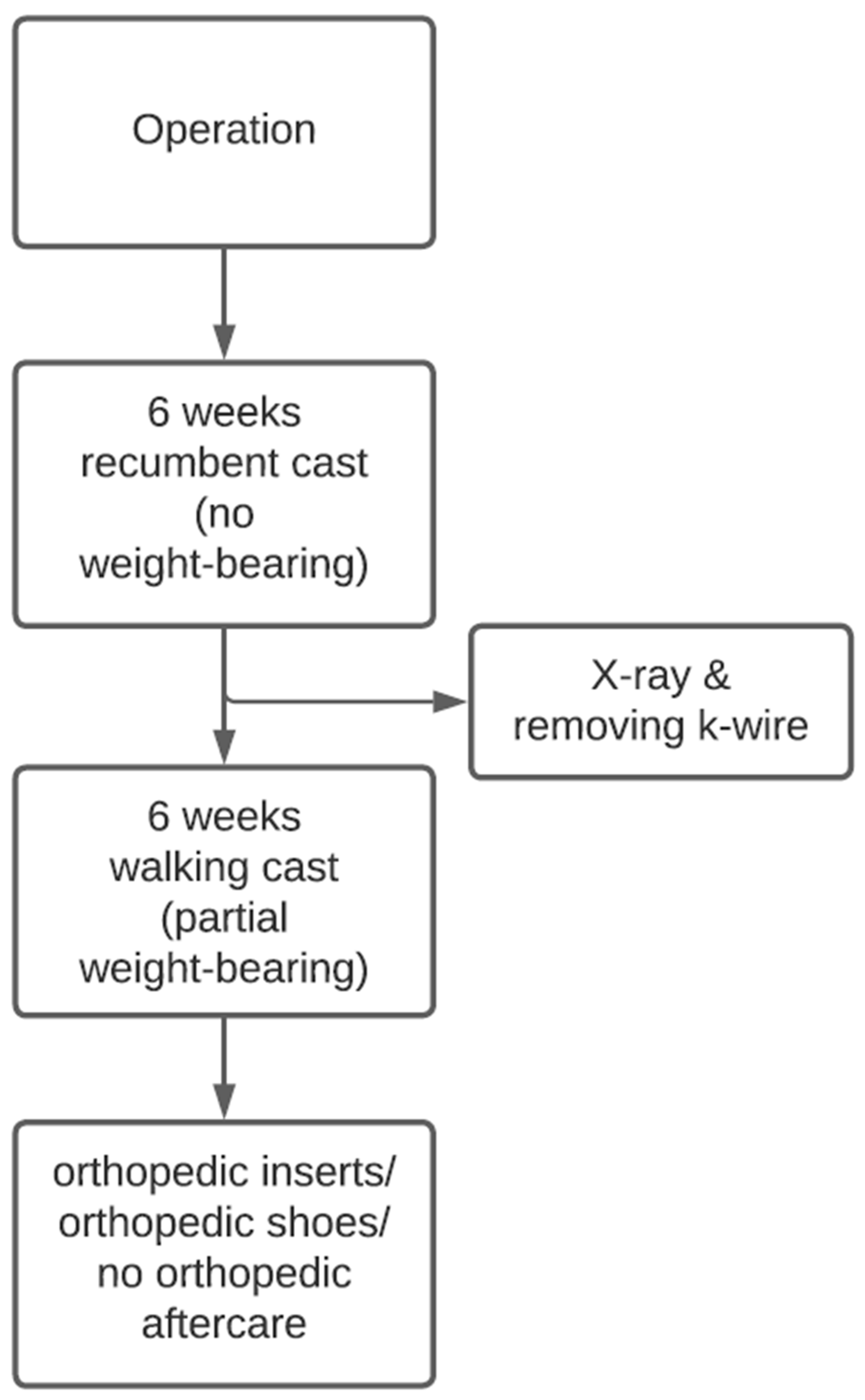
2.4.9. Postoperative Treatment
2.4.10. Statistics
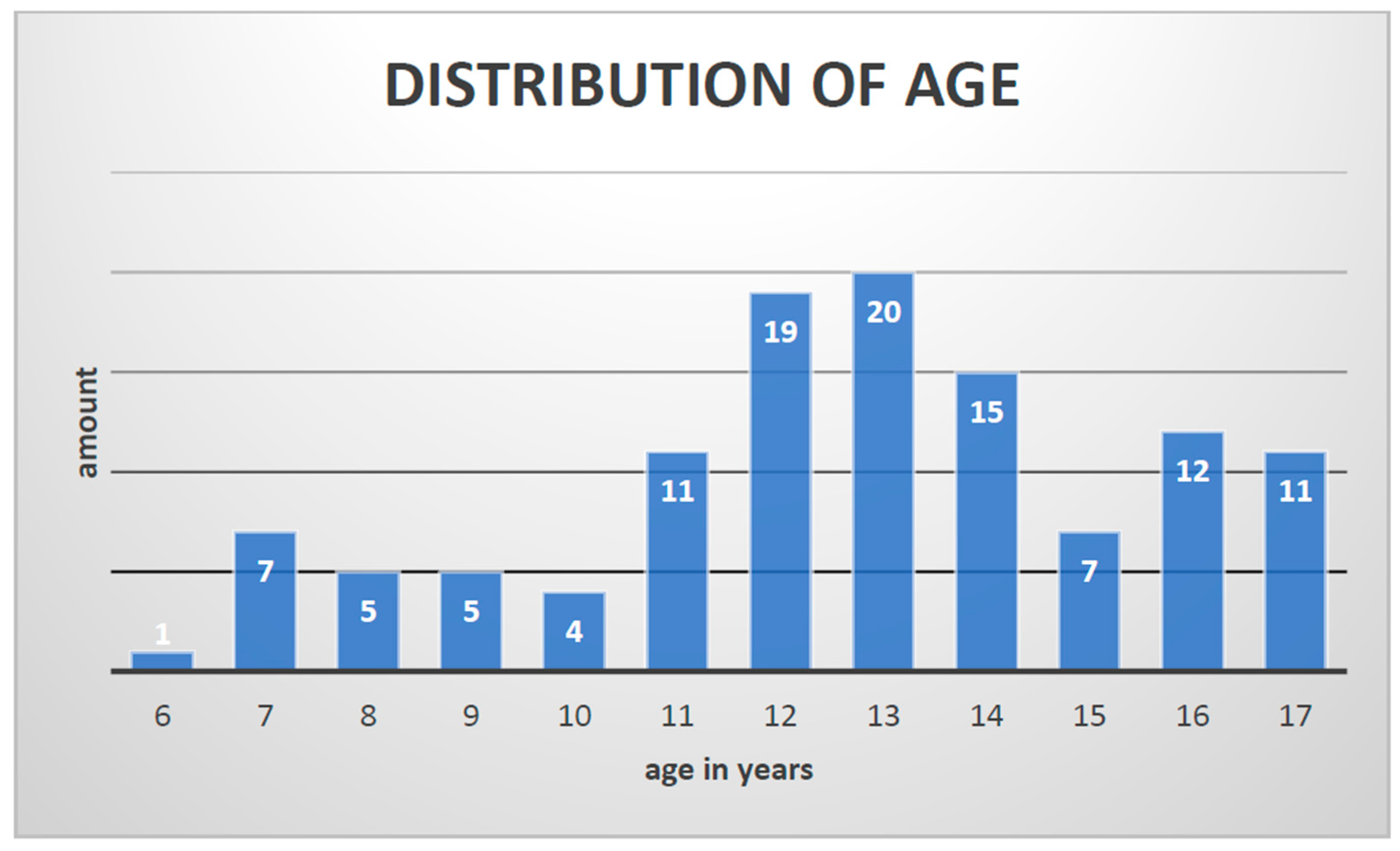
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biz, C.; Cerchiaro, M.; Mori, F.; Rossin, A.; Ponticiello, M.; Crimì, A.; Ruggieri, P. Flatfoot over the centuries: The background of current conservative and operative treatments. Int. Orthop. 2023, 47, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Krauspe, R.; Weimann-Stahlschmidt, K.; Westhoff, B. The Current State of Treatment for Clubfoot in Europe. In European Instructional Lectures; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar] [CrossRef]
- Hefti, F.; Brunner, R. Das abgeflachte Fußlängsgewölbe. Der Orthopäde 1999, 28, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Myerson, M.S.; Badekas, A. Hypermobility of the first ray. Foot Ankle Clin. 2000, 5, 469–484. [Google Scholar]
- Ganesan, B.; Luximon, A.; Al-Jumaily, A.; Balasankar, S.K.; Naik, G.R. Ponseti method in the management of clubfoot under 2 years of age: A systematic review. PLoS ONE 2017, 12, e0178299. [Google Scholar] [CrossRef] [PubMed]
- Dreher, T.; Hagmann, S.; Wenz, W. Reconstruction of Multiplanar Deformity of the Hindfoot and Midfoot with Internal Fixation Techniques. Foot Ankle Clin. 2009, 14. [Google Scholar] [CrossRef] [PubMed]
- Bresnahan, P.J.; Juanto, M.A. Pediatric Flatfeet—A Disease Entity That Demands Greater Attention and Treatment. Front. Pediatr. 2020, 8. [Google Scholar] [CrossRef]
- Blitz, N.M.; Stabile, R.J.; Giorgini, R.J.; DiDomenico, L.A. Flexible Pediatric and Adolescent Pes Planovalgus: Conservative and Surgical Treatment Options. Clin. Podiatr. Med. Surg. 2010, 27, 59–77. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Pupp, G.R.; Harkless, L.B. Our fixation with fixation: Are screws clinically superior to external wires in distal first metatarsal osteotomies? J. Foot Ankle Surg. 1997, 36, 353–355. [Google Scholar] [CrossRef]
- Kim, J.S.; Cho, H.K.; Young, K.W.; Kim, J.S.; Lee, K.T. Biomechanical comparison study of three fixation methods for proximal chevron osteotomy of the first metatarsal in hallux valgus. CiOS Clin. Orthop. Surg. 2017, 9, 514–520. [Google Scholar] [CrossRef]
- Seitz, D.G.; Carpenter, E.B. Triple arthrodesis in children: A ten-year review. South. Med. J. 1974, 67, 1420–1424. [Google Scholar] [CrossRef]
- Wilson, F.C.; Fay, G.F.; Lamotte, P.; Williams, J.C. Triple arthrodesis. A study of the factors affecting fusion after three hubdred and one procedures. J. Bone Jt. Surgery. Am. Vol. 1965, 47, 340–348. [Google Scholar] [CrossRef]
- Wicks, E.D.; Morscher, M.A.; Newton, M.; Steiner, R.P.; Weiner, D.S. Partial or non-union after triple arthrodesis in children: Does it really matter? J. Child. Orthop. 2016, 10, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Nagy, M.; Kholeif, A.; Mansour, A.M.R.; Abdelhameed, S.; Radwan, Y.A.; Khedr, A.; Elhalawany, A.S.; Samir, A.; Sarhan, I.; Zein, A.B. Comparison between Malerba osteotomy and combined Evans/medial displacement calcaneal osteotomies for the management of flexible pes planus in young adults: A prospective randomised control trial, three years follow-up. Int. Orthop. 2021, 45, 2579–2588. [Google Scholar] [CrossRef] [PubMed]
- Nejib, K.; Delpont, M. Medium-term results of calcaneus lengthening in idiopathic symptomatic flat foot in children and adolescents. J. Child. Orthop. 2020, 14, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Adelaar, R.S.; Dannelly, E.A.; Meunier, P.A.; Stelling, F.H.; Goldner, J.L.; Colvard, D.F. A long term study of triple arthrodesis in children. Orthop. Clin. N. Am. 1976, 7, 895–908. [Google Scholar] [CrossRef]
- Galindo, M.J.; Siff, S.J.; Butler, J.E.; Cain, T.E. Triple Arthrodesis in Young Children: A Salvage Procedure After Failed Releases in Severely Affected Feet. Foot Ankle Int. 1987, 7, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Zwipp, H.; Rammelt, S. Modified evans osteotomy for the operative treatment of acquired pes planovalgus. Oper. Orthop. Und Traumatol. 2006, 18, 182–197. [Google Scholar] [CrossRef] [PubMed]
- Lambrinudi, C. New operation on drop-foot. Br. J. Surg. 1927, 15, 193–200. [Google Scholar] [CrossRef]
- Complete Tendon Transfer and Inverse Lambrinudi Arthrodesis: Preliminary Results of a New Technique for the Treatment of Paralytic Pes Calcaneus. Fuß Sprunggelenk 2009, 7, 683–689. [CrossRef]
- Grice, D.S. An extra-articular arthrodesis of the subastragalar joint for correction of paralytic flat feet in children. J. Bone Jt. Surg. Am. Vol. 1952, 34, 927–940. [Google Scholar] [CrossRef]
- Steindler, A. The treatment of pes cavus (Hollow claw foot). Arch. Surg. 1921, 2, 117–128. [Google Scholar] [CrossRef]
- Cole, W.H. The classic. The treatment of claw-foot. By Wallace, H. Cole. 1940. Clin. Orthop. Relat. Res. 1983, 181, 3–6. [Google Scholar]
- Lamm, B.M.; Knight, J.; Ernst, J.J. Evans Calcaneal Osteotomy: Assessment of Multiplanar Correction. J. Foot Ankle Surg. 2022, 61, 700–705. [Google Scholar] [CrossRef]
- Hyer, L.C.; Carpenter, A.M.; Swetenburg, J.R.; Westberry, D.E. Calcaneocuboid distraction arthrodesis for children with symptomatic pes planovalgus: Does fixation improve outcomes? J. Pediatr. Orthop. Part B 2021, 30, 273–281. [Google Scholar] [CrossRef]
- Osateerakun, P.; Cheewasukanon, S.; Limpaphayom, N. Grice extra-articular subtalar fusion for spastic pes planovalgus. Int. Orthop. 2022, 46, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Evans, D. Calcaneo valgus deformity. J. Bone Jt. Surg. Ser. B 1975, 57, 270–278. [Google Scholar] [CrossRef]
- Hagmann, S.; Dreher, T.; Wenz, W. Skewfoot. Foot Ankle Clin. 2009, 14. [Google Scholar] [CrossRef] [PubMed]
- So, L.W.N.; Kuong, E.E.; To, K.T.M.; Leong, J.C.Y.; Chow, W. Long-term outcome after Lambrinudi arthrodesis: How they’re doing after three decades. J. Orthop. Surg. 2019, 27, 2309499019826492. [Google Scholar] [CrossRef] [PubMed]
- Elsner, A.; Barg, A.; Stufkens, S.; Knupp, M.; Hintermann, B. Modified Lambrinudi arthrodesis with additional posterior tibial tendon transfer in adult drop foot. Oper. Orthop. Traumatol. 2011, 23, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Smyth, N.A.; Aiyer, A.A. Introduction: Why Are There so Many Different Surgeries for Hallux Valgus? Foot Ankle Clin. 2018, 23, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Crevoisier, X. The Isolated Talonavicular Arthrodesis. Foot Ankle Clin. 2011, 16, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Turriago, C.A.; Arbeláez, M.F.; Becerra, L.C. Talonavicular joint arthrodesis for the treatment of pes planus valgus in older children and adolescents with cerebral palsy. J. Child. Orthop. 2009, 3, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Arumugam, V.; Ranjit, S.; Patel, S.; Welck, M. What is the best fixation technique for isolated talonavicular arthrodesis? —A systematic review. Foot 2023, 54, 101966. [Google Scholar] [CrossRef] [PubMed]
- Moore, B.E.; Wingert, N.C.; Irgit, K.S.; Gaffney, C.J.; Cush, G.J. Single-Incision Lateral Approach for Triple Arthrodesis. Foot Ankle Int. 2014, 35, 896–902. [Google Scholar] [CrossRef] [PubMed]
- Martone, J.; Poel, L.V.; Levy, N. Complications of Arthrodesis and Nonunion. Clin. Podiatr. Med. Surg. 2012, 29, 11–18. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Osteosynthesis | Advantages and Disadvantages | Cost | Indication |
|---|---|---|---|
| K-wires | Easy to use Temporary Transcutaneous infection | Low | All deformities up to 60 years Contraindication is Charcot’s foot |
| Staples | Additional fixation system High costs to explant | Lower-mid | Forefoot corrections Additive fixation, combined with other osteosynthesis |
| Cannulated screws | More stable than wires Compression option Costs to implant and explant | Medium-high | All deformities Non-unions Smokers Charcot’s foot Reduced bone quality |
| Locking plates | More stable than screws Polyaxial fixation expensive | High | Ankle fusion Long-distance fusion Non-unions Smokers Charcot’s foot Reduced bone quality |
| Nails | More stable than screws and plates expensive | High | Non-unions Ankle/pantalar fusion |
| Arthrodesis/ Osteotomy | Date of Birth | Surgery | Age (Years) | Joint | Sex | Body Weight (kg) | Foot Deformity | Side | K-Wires | K-Wire Removal | Bone Healing | Last X-ray (Weeks) | Follow Up (Weeks) | Complications | Comorbidity |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N = 1 | 13 March 2002 | 26 January 2010 | 7 | subtalar | m | 25 | pes planovalgus | r | 2 | 26 February 2010 | good | 224 | 224 | n | hypothyroidism |
| N = 2 | 21 October 1993 | 31 March 2010 | 16 | subtalar | m | 73 | clubfoot | r | 1 | 10 May 2010 | good | 84 | 84 | n | n |
| N = 3 | 06 August 1998 | 11 January 2011 | 12 | subtalar | m | 60 | clubfoot | r | 2 | 18 February 2011 | good | 46 | 46 | n | n |
| N = 4 | 31 July 1994 | 03 February 2011 | 16 | subtalar | m | 60 | pes planovalgus | l | 2 | 14 March 2011 | good | 79 | 130 | 1; 2 | n |
| N = 5 | 19 December 1993 | 25 May 2011 | 17 | subtalar | m | 60 | clubfoot | l | 1 | 04 July 2011 | good | 58 | 58 | n | n |
| N = 6 | 17 February 1998 | 04 October 2011 | 13 | subtalar | f | 37 | clubfoot | r | 2 | 10 November 2011 | good | 159 | 159 | n | n |
| N = 7 | 29 August 1999 | 27 October 2011 | 12 | subtalar | f | 24 | pes planovalgus | r | 2 | 12 December 2011 | good | 30 | 30 | n | n |
| N = 8 | 29 August 1999 | 27 October 2011 | 12 | subtalar | f | 24 | pes planovalgus | l | 2 | 12 December 2011 | good | 30 | 30 | n | n |
| N = 9 | 26 May 2004 | 05 January 2012 | 7 | subtalar | m | 15 | pes planovalgus | l | 2 | 07 February 2012 | good | 420 | 420 | 3; 4; 5 | n |
| N = 10 | 02 November 1998 | 19 September 2012 | 13 | subtalar | m | 55 | pes planovalgus | l | 4 | 05 November 2012 | good | 26 | 89 | n | n |
| N = 11 | 20 November 1999 | 19 March 2013 | 13 | subtalar | m | 38 | clubfoot | r | 2 | 02 May 2013 | good | 186 | 186 | n | n |
| N = 12 | 20 December 1997 | 18 June 2013 | 15 | subtalar | m | 100 | clubfoot | l | 2 | 25 July 2013 | good | 30 | 30 | n | n |
| N = 13 | 05 September 2001 | 27 August 2013 | 11 | subtalar | m | 62 | pes planovalgus | r | 1 | 07 October 2014 | good | 119 | 119 | n | n |
| N = 14 | 13 October 1997 | 01 July 2014 | 16 | subtalar | m | 130 | pes planovalgus | r | 2 | 14 August 2014 | good | 53 | 53 | n | n |
| N = 15 | 17 June 2003 | 23 June 2015 | 12 | subtalar | f | 54 | pes planovalgus | l | 2 | 03 August 2015 | good | 310 | 310 | n | n |
| N = 16 | 20 March 2007 | 11 August 2015 | 8 | subtalar | m | 30 | pes calcaneus | l | 3 | 10 September 2015 | good | 47 | 47 | n | n |
| N = 17 | 20 March 2007 | 17 August 2015 | 8 | subtalar | m | 30 | pes calcaneus | r | 3 | 14 September 2015 | good | 46 | 46 | n | n |
| N = 18 | 24 July 1992 | 05 January 2010 | 17 | TN | m | 50 | pes cavus | l | 2 | 15 February 2010 | good | 142 | 142 | n | n |
| N = 19 | 13 March 2002 | 26 January 2010 | 7 | TN | m | 25 | pes planovalgus | r | 2 | 26 February 2010 | good | 224 | 224 | n | hypothyroidism |
| N = 20 | 24 July 1997 | 18 March 2010 | 12 | TN | m | 36 | clubfoot | r | 3 | 26 April 2010 | good | 103 | 103 | n | n |
| N = 21 | 21 October 1993 | 31 March 2010 | 16 | TN | m | 73 | clubfoot | r | 2 | 10 May 2010 | good | 84 | 84 | n | n |
| N = 22 | 24 July 1992 | 13 April 2010 | 17 | TN | m | 51 | pes cavus | r | 2 | 26 May 2010 | good | 110 | 110 | n | n |
| N = 23 | 10 July 1995 | 29 July 2010 | 15 | TN | m | 50 | clubfoot | r | 2 | 16 September 2010 | good | 127 | 127 | n | n |
| N = 24 | 04 October 1995 | 20 September 2010 | 14 | TN | m | 72 | clubfoot | r | 2 | 04 November 2010 | good | 37 | 37 | n | n |
| N = 25 | 11 January 2001 | 06 October 2010 | 9 | TN | f | 27 | skewfoot | l | 2 | 08 November 2010 | good | 62 | 107 | n | n |
| N = 26 | 21 January 1997 | 13 October 2010 | 13 | TN | m | 93 | clubfoot | r | 2 | 13 December 2010 | pseudarthrosis | 147 | 147 | 1; 4 | n |
| N = 27 | 26 October 1996 | 03 January 2011 | 14 | TN | f | 59 | pes cavus | l | 2 | 07 February 2011 | good | 41 | 63 | 1; 2 | n |
| N = 28 | 06 August 1998 | 11 January 2011 | 12 | TN | m | 60 | clubfoot | r | 2 | 18 February 2011 | good | 46 | 46 | n | n |
| N = 29 | 24 July 1997 | 02 February 2011 | 13 | TN | m | 41 | clubfoot | l | 3 | 17 March 2011 | good | 57 | 57 | n | n |
| N = 30 | 31 July 1994 | 03 February 2011 | 16 | TN | m | 60 | pes planovalgus | l | 4 | 14 March 2011 | good | 79 | 130 | 1; 2 | n |
| N = 31 | 24 May 1996 | 14 February 2011 | 14 | TN | f | 62 | pes cavus | r | 2 | 31 March 2011 | good | 63 | 63 | n | n |
| N = 32 | 09 August 1995 | 07 March 2011 | 15 | TN | m | 38 | skewfoot | l | 2 | 21 April 2011 | good | 102 | 102 | n | n |
| N = 33 | 03 January 2000 | 28 April 2011 | 11 | TN | f | 52 | clubfoot | r | 2 | 10 June 2011 | good | 507 | 507 | 3; 4; 6 | n |
| N = 34 | 19 December 1993 | 25 May 2011 | 17 | TN | m | 60 | clubfoot | l | 3 | 04 July 2011 | good | 58 | 58 | n | n |
| N = 35 | 16 September 1999 | 15 June 2011 | 11 | TN | m | 34 | pes cavus | r | 2 | 25 July 2011 | good | 56 | 56 | n | n |
| N = 36 | 23 April 2001 | 20 July 2011 | 10 | TN | f | 37 | clubfoot | l | 4 | 01 September 2011 | pseudarthrosis | 31 | 31 | 1; 2 | n |
| N = 37 | 11 June 2003 | 21 September 2011 | 8 | TN | m | 27 | clubfoot | l | 2 | 24 October 2011 | pseudarthrosis | 372 | 477 | n | asthma |
| N = 38 | 17 February 1998 | 04 October 2011 | 13 | TN | f | 37 | clubfoot | r | 2 | 10 November 2011 | good | 159 | 159 | n | n |
| N = 39 | 29 August 1999 | 27 October 2011 | 12 | TN | f | 24 | pes planovalgus | r | 2 | 12 December 2011 | good | 30 | 30 | n | n |
| N = 40 | 29 August 1999 | 27 October 2011 | 12 | TN | f | 24 | pes planovalgus | l | 2 | 12 December 2011 | good | 30 | 30 | n | n |
| N = 41 | 21 January 1997 | 01 December 2011 | 14 | TN | m | 101 | clubfoot | l | 3 | 05 January 2012 | good | 88 | 88 | n | n |
| N = 42 | 13 February 2002 | 14 December 2011 | 9 | TN | f | 37 | clubfoot | l | 2 | 23 January 2012 | good | 210 | 238 | n | n |
| N = 43 | 26 May 2004 | 05 January 2012 | 7 | TN | m | 15 | pes planovalgus | l | 2 | 07 February 2012 | good | 420 | 420 | 3; 4; 5 | n |
| N = 44 | 02 April 1997 | 08 February 2012 | 14 | TN | m | 58 | clubfoot | r | 2 | 26 March 2012 | good | 85 | 85 | n | n |
| N = 45 | 13 August 2000 | 02 May 2012 | 11 | TN | m | 40 | pes calcaneus | l | 2 | 13 June 2012 | good | 32 | 32 | n | n |
| N = 46 | 02 April 1996 | 08 May 2012 | 16 | TN | m | 40 | pes cavus | l | 2 | 22 June 2012 | good | 46 | 98 | n | n |
| N = 47 | 13 February 2002 | 09 May 2012 | 10 | TN | f | 43 | clubfoot | r | 3 | 18 June 2012 | good | 170 | 170 | n | n |
| N = 48 | 13 August 2000 | 13 June 2012 | 11 | TN | m | 35 | pes planovalgus | r | 2 | 20 July 2012 | good | 26 | 26 | 1 | n |
| N = 49 | 19 May 2000 | 18 December 2012 | 12 | TN | f | 44 | pes cavus | r | 2 | 01 February 2013 | good | 26 | 26 | n | n |
| N = 50 | 20 November 1999 | 19 March 2013 | 13 | TN | m | 38 | clubfoot | r | 2 | 02 May 2013 | good | 186 | 186 | n | n |
| N = 51 | 05 September 2001 | 27 August 2013 | 11 | TN | m | 62 | pes planovalgus | r | 2 | 07 October 2014 | good | 119 | 119 | n | n |
| N = 52 | 13 October 1997 | 01 July 2014 | 16 | TN | m | 130 | pes planovalgus | r | 2 | 14 August 2014 | good | 53 | 53 | n | n |
| N = 53 | 09 March 2000 | 11 February 2015 | 14 | TN | m | 64 | clubfoot | l | 2 | 23 March 2015 | good | 279 | 279 | n | n |
| N = 54 | 25 August 2001 | 02 April 2015 | 13 | TN | f | 67 | clubfoot | l | 4 | 18 May 2015 | good | 189 | 189 | n | n |
| N = 55 | 17 June 2003 | 23 June 2015 | 12 | TN | f | 54 | pes planovalgus | l | 3 | 03 August 2015 | good | 310 | 310 | n | n |
| N = 56 | 29 June 2002 | 19 August 2015 | 13 | TN | m | 53 | clubfoot | r | 2 | 17 September 2015 | good | 198 | 198 | n | n |
| N = 57 | 24 July 1992 | 05 January 2010 | 17 | CC | m | 50 | pes cavus | l | 2 | 15 February 2010 | good | 142 | 142 | n | n |
| N = 58 | 13 March 2002 | 26 January 2010 | 7 | CC | m | 25 | pes planovalgus | r | 2 | 26 February 2010 | good | 224 | 224 | n | hypothyroidism |
| N = 59 | 15 July 2003 | 11 March 2010 | 6 | CC | f | 20 | pes planovalgus | l | 4 | 09 April 2010 | good | 44 | 44 | n | n |
| N = 60 | 24 July 1997 | 18 March 2010 | 12 | CC | m | 36 | clubfoot | r | 2 | 26 April 2010 | good | 103 | 103 | n | n |
| N = 61 | 21 October 1993 | 31 March 2010 | 16 | CC | m | 73 | clubfoot | r | 2 | 10 May 2010 | good | 84 | 84 | n | n |
| N = 62 | 24 July 1992 | 13 April 2010 | 17 | CC | m | 51 | pes cavus | r | 2 | 26 May 2010 | good | 110 | 110 | n | n |
| N = 63 | 17 February 1998 | 18 May 2010 | 12 | CC | f | 35 | clubfoot | l | 2 | 05 July 2010 | pseudarthrosis | 231 | 231 | 1; 2 | n |
| N = 64 | 10 July 1995 | 29 July 2010 | 15 | CC | m | 50 | clubfoot | r | 2 | 16 September 2010 | good | 127 | 127 | n | n |
| N = 65 | 04 October 1995 | 20 September 2010 | 14 | CC | m | 72 | clubfoot | r | 2 | 04 November 2010 | good | 37 | 37 | n | n |
| N = 66 | 11 January 2001 | 06 October 2010 | 9 | CC | f | 27 | skewfoot | l | 1 | 08 November 2010 | good | 62 | 107 | n | n |
| N = 67 | 21 January 1997 | 13 October 2010 | 13 | CC | m | 93 | clubfoot | r | 2 | 13 December 2010 | pseudarthrosis | 147 | 147 | 1; 4 | n |
| N = 68 | 26 October 1996 | 03 January 2011 | 14 | CC | f | 59 | pes cavus | l | 2 | 07 February 2011 | good | 41 | 63 | 1; 2 | n |
| N = 69 | 06 August 1998 | 11 January 2011 | 12 | CC | m | 60 | clubfoot | r | 2 | 18 February 2011 | good | 46 | 46 | n | n |
| N = 70 | 24 July 1997 | 02 February 2011 | 13 | CC | m | 41 | clubfoot | l | 2 | 17 March 2011 | good | 57 | 57 | n | n |
| N = 71 | 31 July 1994 | 03 February 2011 | 16 | CC | m | 60 | pes planovalgus | l | 2 | 14 March 2011 | good | 79 | 130 | 1; 2 | n |
| N = 72 | 24 May 1996 | 14 February 2011 | 14 | CC | f | 62 | pes cavus | r | 2 | 31 March 2011 | good | 63 | 63 | n | n |
| N = 73 | 03 January 2000 | 28 April 2011 | 11 | CC | f | 52 | clubfoot | r | 2 | 10 June 2011 | good | 507 | 507 | 3; 4; 6 | n |
| N = 74 | 19 December 1993 | 25 May 2011 | 17 | CC | m | 60 | clubfoot | l | 4 | 04 July 2011 | good | 58 | 58 | n | n |
| N = 75 | 16 September 1999 | 15 June 2011 | 11 | CC | m | 34 | pes cavus | r | 2 | 25 July 2011 | good | 56 | 56 | n | n |
| N = 76 | 23 April 2001 | 20 July 2011 | 10 | CC | f | 37 | clubfoot | l | 2 | 01 September 2011 | pseudarthrosis | 31 | 31 | 1; 2 | n |
| N = 77 | 21 September 1997 | 20 September 2011 | 13 | CC | m | 50 | clubfoot | l | 2 | 07 November 2011 | good | 38 | 38 | 1 | n |
| N = 78 | 17 February 1998 | 04 October 2011 | 13 | CC | f | 37 | clubfoot | r | 2 | 10 November 2011 | good | 159 | 159 | n | n |
| N = 79 | 21 January 1997 | 01 December 2011 | 14 | CC | m | 101 | clubfoot | l | 2 | 05 January 2012 | good | 88 | 88 | n | n |
| N = 80 | 13 February 2002 | 14 December 2011 | 9 | CC | f | 37 | clubfoot | l | 2 | 23 January 2012 | good | 210 | 238 | n | n |
| N = 81 | 26 May 2004 | 05 January 2012 | 7 | CC | m | 15 | pes planovalgus | l | 3 | 07 February 2012 | good | 420 | 420 | 3; 4; 5 | n |
| N = 82 | 25 February 2004 | 24 January 2012 | 7 | CC | m | 27 | clubfoot | l | 4 | 22 February 2012 | good | 197 | 197 | 1; 2 | n |
| N = 83 | 02 April 1997 | 08 February 2012 | 14 | CC | m | 58 | clubfoot | r | 2 | 26 March 2012 | good | 85 | 85 | n | n |
| N = 84 | 23 March 1997 | 01 March 2012 | 14 | CC | m | 74 | pes cavus | r | 4 | 16 April 2012 | good | 27 | 46 | n | n |
| N = 85 | 13 August 2000 | 02 May 2012 | 11 | CC | m | 40 | pes calcaneus | l | 1 | 13 June 2012 | good | 32 | 32 | n | n |
| N = 86 | 02 April 1996 | 08 May 2012 | 16 | CC | m | 40 | pes cavus | l | 2 | 22 June 2012 | good | 46 | 98 | n | n |
| N = 87 | 13 February 2002 | 09 May 2012 | 10 | CC | f | 43 | clubfoot | r | 2 | 18 June 2012 | good | 170 | 170 | n | n |
| N = 88 | 13 August 2000 | 13 June 2012 | 11 | CC | m | 35 | pes planovalgus | r | 2 | 20 July 2012 | good | 26 | 26 | 1 | n |
| N = 89 | 19 May 2000 | 18 December 2012 | 12 | CC | f | 44 | pes cavus | r | 2 | 01 February 2013 | good | 26 | 26 | n | n |
| N = 90 | 20 November 1999 | 19 March 2013 | 13 | CC | m | 38 | clubfoot | r | 2 | 02 May 2013 | good | 186 | 186 | n | n |
| N = 91 | 05 September 2001 | 27 August 2013 | 11 | CC | m | 62 | pes planovalgus | r | 2 | 07 October 2014 | good | 119 | 119 | n | n |
| N = 92 | 07 December 2003 | 11 November 2013 | 9 | CC | m | 20 | pes planovalgus | l | 3 | 12 December 2013 | good | 61 | 61 | n | n |
| N = 93 | 12 June 1999 | 12 May 2014 | 14 | CC | m | 38 | pes planovalgus | l | 3 | 30 June 2014 | good | 183 | 183 | n | n |
| N = 94 | 13 October 1997 | 01 July 2014 | 16 | CC | m | 130 | pes planovalgus | r | 2 | 14 August 2014 | good | 53 | 53 | n | n |
| N = 95 | 05 September 2001 | 21 October 2014 | 13 | CC | m | 70 | pes planovalgus | l | 2 | 24 November 2014 | good | 59 | 59 | n | hypothyroidism |
| N = 96 | 06 January 1997 | 03 December 2014 | 17 | CC | m | 84 | clubfoot | r | 2 | 15 January 2014 | good | 62 | 62 | n | n |
| N = 97 | 25 August 2001 | 02 April 2015 | 13 | CC | f | 67 | clubfoot | l | 4 | 18 May 2015 | good | 189 | 189 | n | n |
| N = 98 | 17 June 2003 | 23 June 2015 | 12 | CC | f | 54 | pes planovalgus | l | 2 | 03 August 2015 | good | 310 | 310 | n | n |
| N = 99 | 20 March 2007 | 11 August 2015 | 8 | CC | m | 30 | pes calcaneus | l | 2 | 10 September 2015 | good | 47 | 47 | n | n |
| N = 100 | 20 March 2007 | 17 August 2015 | 8 | CC | m | 30 | pes calcaneus | r | 2 | 14 September 2015 | good | 46 | 46 | n | n |
| N = 101 | 06 November 2003 | 24 November 2015 | 12 | CC | f | 40 | skewfoot | r | 2 | 04 January 2015 | good | 31 | 31 | n | n |
| N = 102 | 06 August 2002 | 16 December 2015 | 13 | CC | m | 43 | pes cavus | l | 2 | 27 January 2016 | good | 104 | 130 | n | scoliosis |
| N = 103 | 24 July 1992 | 05 January 2010 | 17 | MT1 | m | 50 | pes cavus | l | 1 | 15 February 2010 | good | 142 | 142 | n | n |
| N = 104 | 24 July 1992 | 13 April 2010 | 17 | MT1 | m | 51 | pes cavus | r | 1 | 26 May 2010 | good | 110 | 110 | n | n |
| N = 105 | 17 February 1998 | 18 May 2010 | 12 | MT1 | f | 35 | clubfoot | l | 2 | 05 July 2010 | pseudarthrosis | 231 | 231 | 1 | n |
| N = 106 | 26 October 1996 | 03 January 2011 | 14 | MT1 | f | 59 | pes cavus | l | 1 | 07 February 2011 | good | 41 | 63 | 1; 2 | n |
| N = 107 | 09 August 1995 | 07 March 2011 | 15 | MT1 | m | 38 | skewfoot | l | 2 | 21 April 2011 | good | 102 | 102 | n | n |
| N = 108 | 21 September 1997 | 20 September 2011 | 13 | MT1 | m | 50 | clubfoot | l | 1 | 07 November 2011 | good | 38 | 38 | 1 | n |
| N = 109 | 23 March 1997 | 01 March 2012 | 14 | MT1 | m | 74 | pes cavus | r | 1 | 16 April 2012 | good | 27 | 46 | n | n |
| N = 110 | 02 April 1996 | 08 May 2012 | 16 | MT1 | m | 40 | pes cavus | l | 1 | 22 June 2012 | good | 46 | 98 | n | n |
| N = 111 | 19 May 2000 | 18 December 2012 | 12 | MT1 | f | 44 | pes cavus | r | 2 | 01 February 2013 | good | 26 | 26 | n | n |
| N = 112 | 20 December 1997 | 18 June 2013 | 15 | MT1 | m | 100 | clubfoot | l | 2 | 25 July 2013 | good | 30 | 30 | n | n |
| N = 113 | 28 September 1997 | 24 July 2013 | 15 | MT1 | f | 53 | hallux valgus | l | 2 | 02 September 2013 | good | 27 | 29 | n | n |
| N = 114 | 06 January 1997 | 03 December 2014 | 17 | MT1 | m | 84 | clubfoot | r | 1 | 15 January 2014 | good | 62 | 62 | n | n |
| N = 115 | 29 June 2002 | 19 August 2015 | 13 | MT1 | m | 53 | clubfoot | r | 1 | 17 September 2015 | good | 198 | 198 | n | n |
| N = 116 | 06 November 2003 | 24 November 2015 | 12 | MT1 | f | 40 | skewfoot | r | 1 | 04 January 2015 | good | 31 | 31 | n | n |
| N = 117 | 06 August 2002 | 16 December 2015 | 13 | MT1 | m | 43 | pes cavus | l | 2 | 27 January 2016 | good | 104 | 130 | n | scoliosis |
| Osteotomy and Surgical Technique | Indication |
|---|---|
| Evans osteotomy (lengthening osteotomy of the calcaneal neck) [18] | Planovalgus, skewfoot |
| Subtalar fusion (lateral or medial open or closed wedge) | Hindfoot varus/valgus with instability Severe bony fixed varus/valgus |
| Triple arthrodesis (Chopart’s and subtalar joint fusion) | Severe planovalgus, cavovarus with severe hindfoot varus, severe clubfoot (residual) |
| Lambrinudi procedure (triple fusion subtalar ventral-based wedge resection) [19] | (Bony) fixed hindfoot equinus |
| Inverse lambrinudi (additive triple fusion and subtalar dorsal-based wedge resection) [20] | Severe calcaneal foot |
| Chopart’s arthrodesis | Clubfoot, cavovarus foot |
| Grice procedure [21] | Planovalgus foot |
| Calcaneocuboid distraction fusion | Planovalgus foot |
| Patient | Non-Union | Gender | Weight | Age | Underlying Condition | Number of K-wires | Diagnosis | Surgery | Other |
|---|---|---|---|---|---|---|---|---|---|
| N = 1 | TN + CC | Male | 93 kg | 13 years | No | 2 | Clubfoot | Chopart-Arthrodesis | 3 Revision surgery due to wound healing disorders |
| N = 2 | TN + CC | Female | 37 kg | 10 years | No | 4 | Clubfoot relapse | Chopart-Arthrodesis | Antibiotics, Wound healing disorder |
| N = 3 | TN | Male | 27 kg | 8 years | Respiratory disease | 2 | Clubfoot | Chopart-Arthrodesis | Previous surgery pantalare release |
| N = 4 | MT I + CC | Female | 35 kg | 12 years | No | 2 | Clubfoot | Chopart-Arthrodesis + Correction MT I | Wound healing disorder |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kreher, J.; Putz, C.; Fackler, S.; Müller, S.; Horsch, A.; Geisbüsch, A. K-Wire Osteosynthesis for Arthrodesis of the Paediatric Foot Is a Good and Valid Procedure. J. Clin. Med. 2023, 12, 7478. https://doi.org/10.3390/jcm12237478
Kreher J, Putz C, Fackler S, Müller S, Horsch A, Geisbüsch A. K-Wire Osteosynthesis for Arthrodesis of the Paediatric Foot Is a Good and Valid Procedure. Journal of Clinical Medicine. 2023; 12(23):7478. https://doi.org/10.3390/jcm12237478
Chicago/Turabian StyleKreher, Jannes, Cornelia Putz, Susanne Fackler, Sebastian Müller, Axel Horsch, and Andreas Geisbüsch. 2023. "K-Wire Osteosynthesis for Arthrodesis of the Paediatric Foot Is a Good and Valid Procedure" Journal of Clinical Medicine 12, no. 23: 7478. https://doi.org/10.3390/jcm12237478
APA StyleKreher, J., Putz, C., Fackler, S., Müller, S., Horsch, A., & Geisbüsch, A. (2023). K-Wire Osteosynthesis for Arthrodesis of the Paediatric Foot Is a Good and Valid Procedure. Journal of Clinical Medicine, 12(23), 7478. https://doi.org/10.3390/jcm12237478