

Clinical Implication of Supra-Normal Left Ventricular Ejection Fraction in Patients Undergoing Transcatheter Aortic Valve Replacement

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
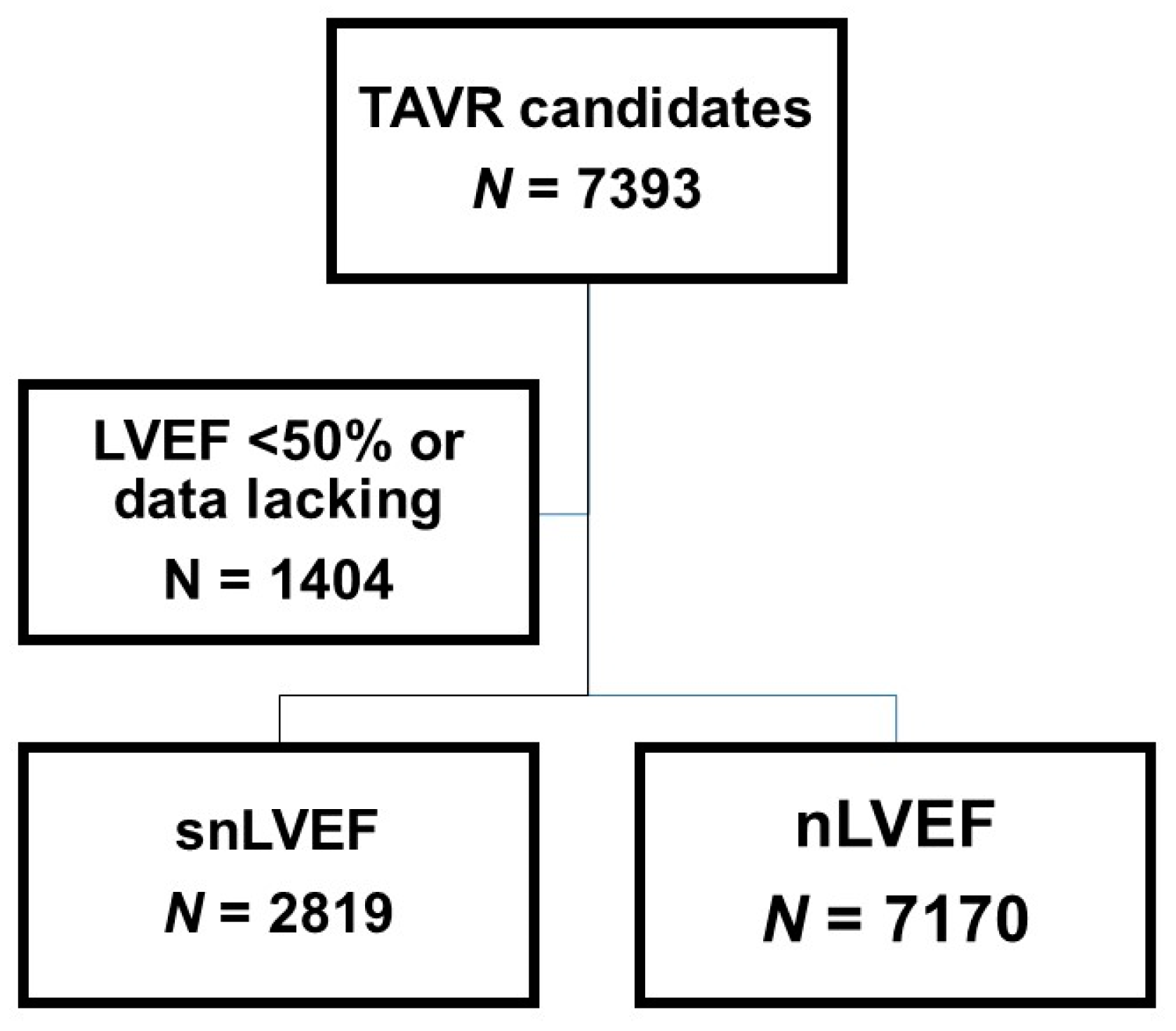
2.1. Patient Selection
2.2. Study Design
2.3. TAVR Procedure
2.4. Variables Evaluated
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
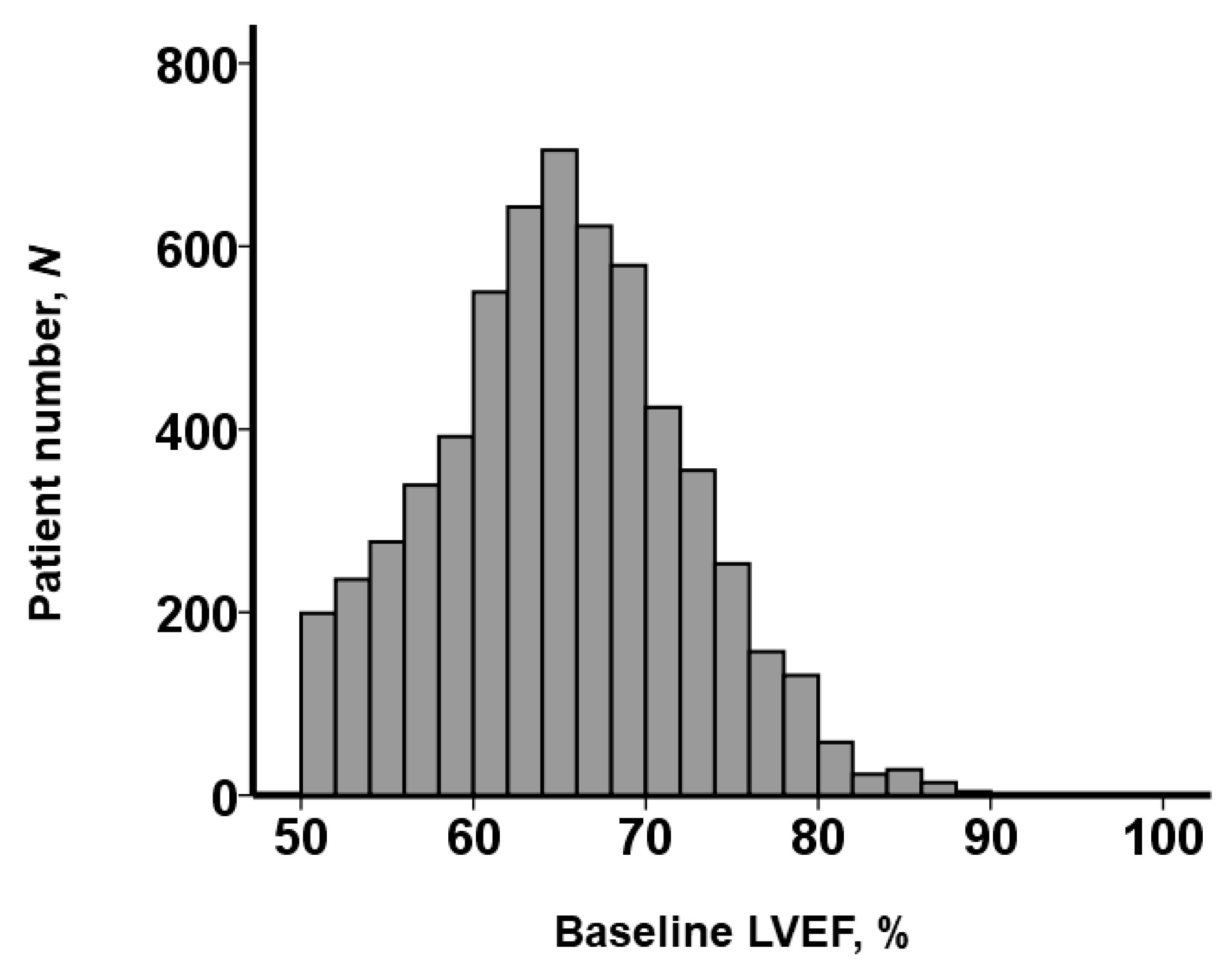
3.2. Baseline LVEF Distribution
3.3. Peri-Procedural Complication
3.4. One-Year Follow-Up of Echocardiography
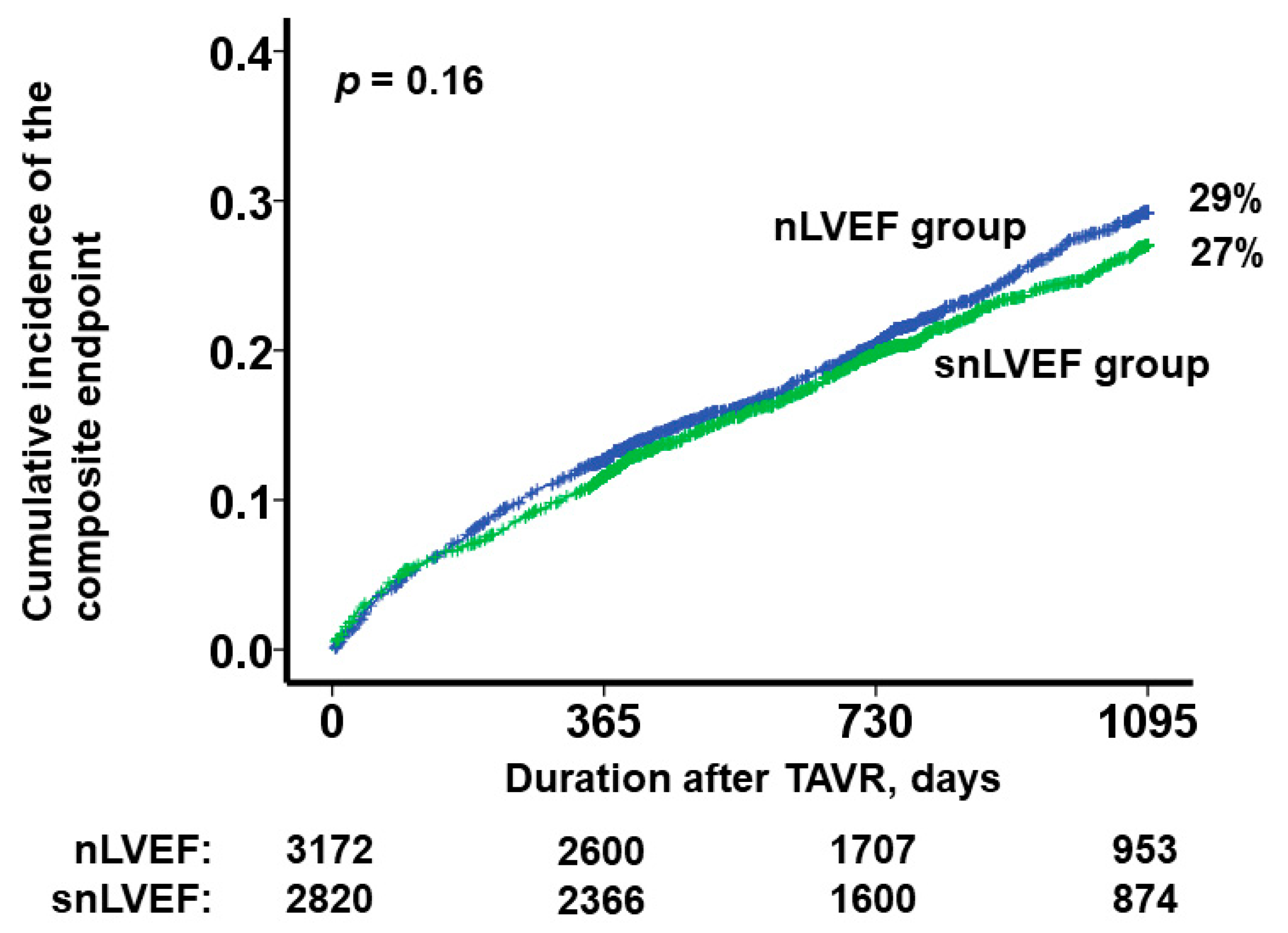
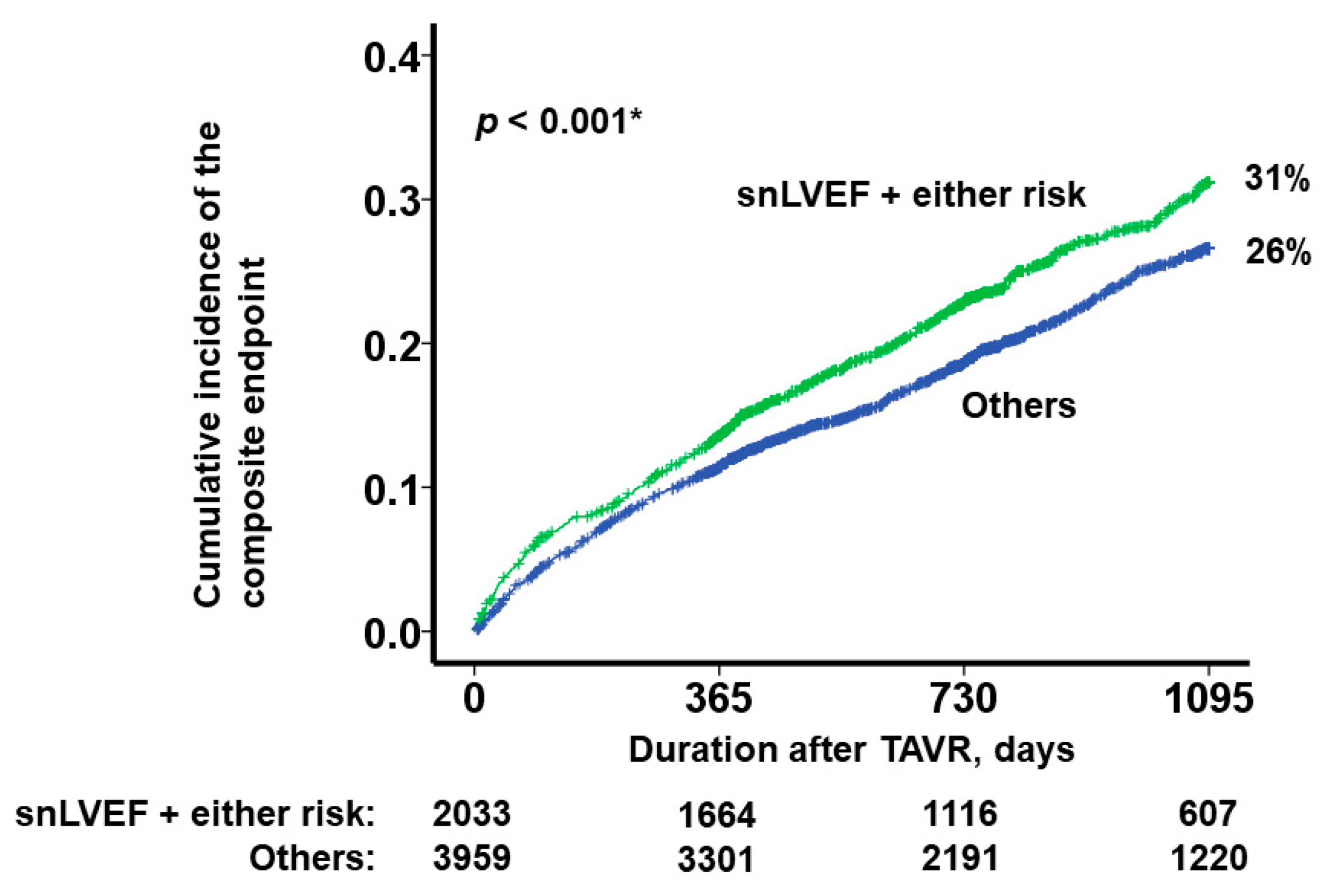
3.5. Mid-Term Clinical Outcome
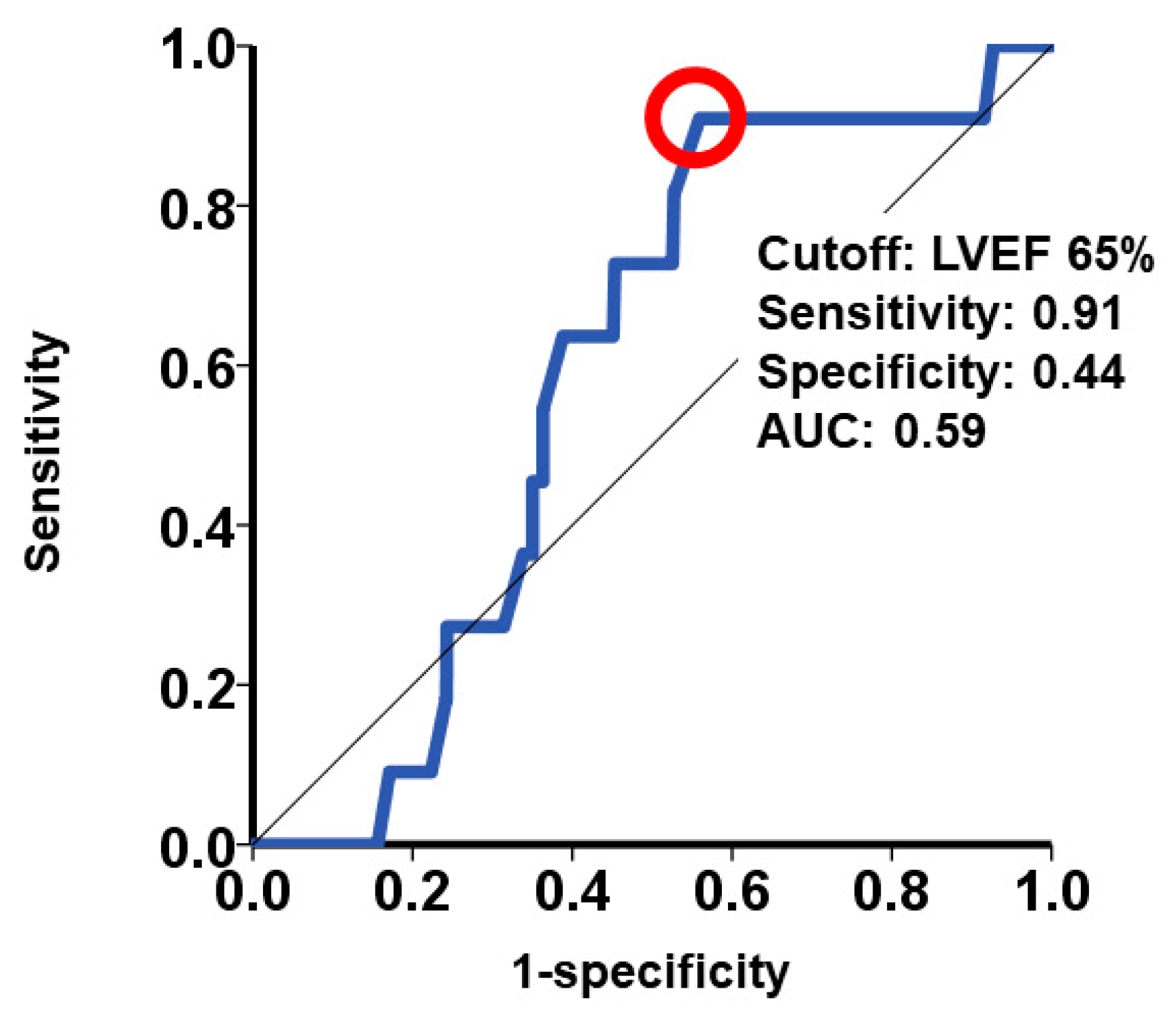
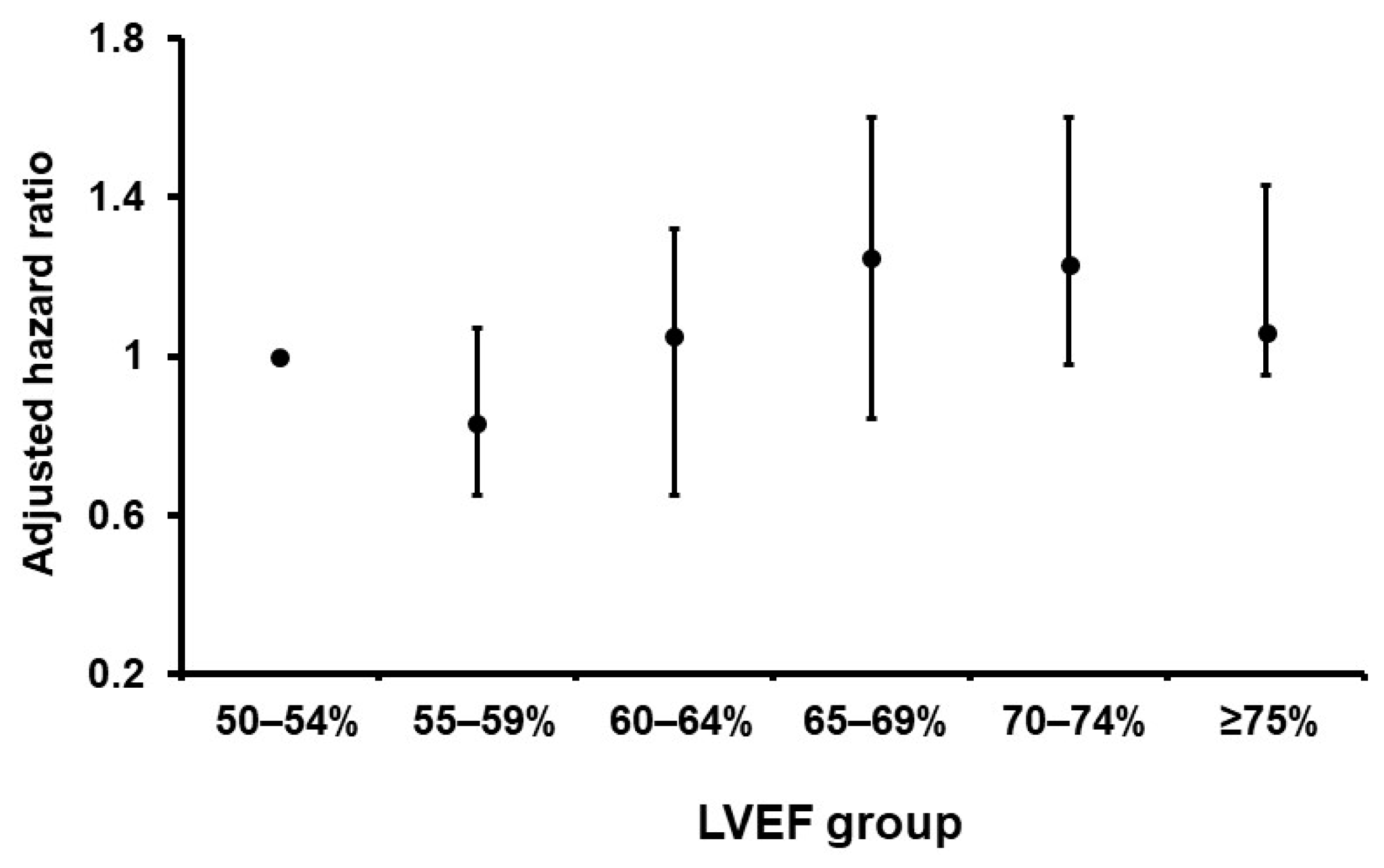
3.6. Further Risk Stratification
4. Discussion
4.1. The Concept and Cutoff of snLVEF
4.2. The Unique Profile of the TAVR Candidates with snLVEF
4.3. Prognostic Impact of snLVEF after TAVR
4.4. Estimated Underlying Mechanism of Our Findings
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, H.; Ide, T.; Ito, H.; Kihara, Y.; Kinugawa, K.; Kinugawa, S.; Makaya, M.; Murohara, T.; Node, K.; Saito, Y.; et al. JCS/JHFS 2021 Guideline Focused Update on Diagnosis and Treatment of Acute and Chronic Heart Failure. J. Card. Fail. 2021, 27, 1404–1444. [Google Scholar] [CrossRef]
- Bozkurt, B.; Coats, A.J.S.; Tsutsui, H.; Abdelhamid, C.M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Bohm, M.; Butler, J.; et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur. J. Heart Fail. 2021, 23, 352–380. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Vaduganathan, M.L.; Claggett, B.; Packer, M.; Zile, M.; Swedberg, K.; McMurray, J.J. Sacubitril/Valsartan Across the Spectrum of Ejection Fraction in Heart Failure. Circulation 2020, 141, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.; Packer, M.; Filippatos, G.; Ferreira, J.P.; Zeller, C.; Schnee, J.; Brueckmann, M.; Pocock, S.J.; Zannad, F.; Anker, S.D. Effect of empagliflozin in patients with heart failure across the spectrum of left ventricular ejection fraction. Eur. Heart J. 2022, 43, 416–426. [Google Scholar] [CrossRef]
- Jhund, P.S.; Kondo, T.; Butt, J.H.; Docherty, K.F.; Claggett, B.L.; Desai, A.S.; Vaduganathan, M.; Gasparyan, S.B.; Bengtsson, O.; Lindholm, D.; et al. Dapagliflozin across the range of ejection fraction in patients with heart failure: A patient-level, pooled meta-analysis of DAPA-HF and DELIVER. Nat. Med. 2022, 28, 1956–1964. [Google Scholar] [CrossRef]
- Wehner, G.J.; Jing, L.; Haggerty, C.M.; Suever, J.D.; Leader, J.B.; Hartzel, D.N.; Kirchner, H.L.; Manus, J.N.A.; James, N.; Ayar, Z.; et al. Routinely reported ejection fraction and mortality in clinical practice: Where does the nadir of risk lie? Eur. Heart J. 2020, 41, 1249–1257. [Google Scholar] [CrossRef]
- Horiuchi, Y.; Asami, M.; Ide, T.; Yahagi, K.; Komiyama, K.; Yuzawa, H.; Tanaka, J.; Aoki, J.; Matsushima, S.; Tohyama, T.; et al. Prevalence, characteristics and cardiovascular and non-cardiovascular outcomes in patients with heart failure with supra-normal ejection fraction: Insight from the JROADHF study. Eur. J. Heart Fail. 2023, 25, 989–998. [Google Scholar] [CrossRef]
- van Essen, B.J.; Tromp, J.; Ter Maaten, J.M.; Greenberg, B.H.; Gimpelewicz, C.; Felker, G.M.; Davison, B.A.; Severin, T.; Pang, P.S.; Cotter, G.; et al. Characteristics and clinical outcomes of patients with acute heart failure with a supranormal left ventricular ejection fraction. Eur. J. Heart Fail. 2023, 25, 35–42. [Google Scholar] [CrossRef]
- Sinagra, G.; Paldino, A.; Dal Ferro, M. Heart failure with supra-normal left ventricular ejection fraction: Distinct polygenic bases of an unrecognized phenotype. Eur. J. Heart Fail. 2022, 24, 2128–2130. [Google Scholar] [CrossRef]
- Kamperidis, V.; Delgado, V.; van Mieghem, N.M.; Kappetein, A.P.; Leon, M.B.; Bax, J.J. Diagnosis and management of aortic valve stenosis in patients with heart failure. Eur. J. Heart Fail. 2016, 18, 469–481. [Google Scholar] [CrossRef]
- Genereux, P.; Pibarot, P.; Redfors, B.; Mack, M.J.; Makkar, R.R.; Jaber, W.A.; Svensson, L.G.; Kapadia, S.; Tuzcu, E.M.; Thourani, V.H.; et al. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur. Heart J. 2017, 38, 3351–3358. [Google Scholar] [CrossRef]
- Hamm, C.W.; Arsalan, M.; Mack, M.J. The future of transcatheter aortic valve implantation. Eur. Heart J. 2016, 37, 803–810. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef]
- Maredziak, M.; Bengs, S.; Portmann, A.; Haider, A.; Wijnen, W.J.; Warnock, G.I.; Etter, D.; Froehlich, S.; Fiechter, M.; Meisel, A.; et al. Microvascular dysfunction and sympathetic hyperactivity in women with supra-normal left ventricular ejection fraction (snLVEF). Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 3094–3106. [Google Scholar] [CrossRef] [PubMed]
- Gebhard, C.; Maredziak, M.; Messerli, M.; Buechel, R.R.; Lin, F.; Gransar, H.; Achenbach, S.; Al-Mallah, M.H.; Andreini, D.; Bax, J.J.; et al. Increased long-term mortality in women with high left ventricular ejection fraction: Data from the CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes: An InteRnational Multicenter) long-term registry. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Kerkhof, P.L.M.; Kuznetsova, T.; Ali, R.; Handly, N. Left ventricular volume analysis as a basic tool to describe cardiac function. Adv. Physiol. Educ. 2018, 42, 130–139. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; Melenovsky, V.; Redfield, M.M.; Nishimura, R.A.; Borlaug, B.A. High-Output Heart Failure: A 15-Year Experience. J. Am. Coll. Cardiol. 2016, 68, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Tsuruta, H.; Hayashida, K.; Yashima, F.; Yanagisawa, R.; Tanaka, M.; Arai, T.; Minakata, Y.; Itabashi, Y.; Murata, M.; Kohsaka, S.; et al. Incidence, predictors, and midterm clinical outcomes of left ventricular obstruction after transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2018, 92, E288–E298. [Google Scholar] [CrossRef]
- Forrest, I.S.; Rocheleau, G.; Bafna, S.; Argulian, E.; Narula, J.; Natarajan, P.; Do, R. Genetic and phenotypic profiling of supranormal ejection fraction reveals decreased survival and underdiagnosed heart failure. Eur. J. Heart Fail. 2022, 24, 2118–2127. [Google Scholar] [CrossRef] [PubMed]
- Ternacle, J.; Krapf, L.; Mohty, D.; Magne, J.; Nguyen, A.; Galat, A.; Gallet, R.; Teiger, E.; Cote, N.; Clavel, M.A.; et al. Aortic Stenosis and Cardiac Amyloidosis: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 2638–2651. [Google Scholar] [CrossRef] [PubMed]
- Strange, G.; Playford, D.; Scalia, G.M.; Celermajer, D.S.; Prior, D.; Codde, J.; Chan, Y.K.; Bulsara, M.K.; Stewart, S.; Investigators, N. Change in ejection fraction and long-term mortality in adults referred for echocardiography. Eur. J. Heart Fail. 2021, 23, 555–563. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 5989) | snLVEF (N = 2819) | nLVEF (N = 3170) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 84.4 ± 5.1 | 84.2 ± 5.1 | 84.6 ± 5.1 | 0.002 * |
| Male sex | 1783 (30%) | 742 (26%) | 1041 (33%) | <0.001 * |
| Body mass index | 22.5 ± 3.8 | 22.6 ± 3.8 | 22.5 ± 3.7 | 0.24 |
| New York Heart Association class III/IV | 2187 (37%) | 891 (32%) | 1296 (41%) | <0.001 * |
| Comorbidity | ||||
| Hypertension | 5063 (85%) | 2343 (83%) | 2720 (86%) | 0.002 * |
| Diabetes mellitus | 1557 (26%) | 709 (25%) | 848 (27%) | 0.085 |
| Dyslipidemia | 3339 (56%) | 1594 (57%) | 1745 (55%) | 0.13 |
| Atrial fibrillation | 1202 (20%) | 501 (18%) | 701 (22%) | <0.001 * |
| Chronic kidney disease | 4078 (68%) | 1859 (66%) | 2219 (70%) | <0.001 * |
| History of stroke | 667 (11%) | 326 (12%) | 341 (11%) | 0.17 |
| Peripheral artery disease | 644 (11%) | 288 (10%) | 356 (11%) | 0.11 |
| Chronic obstructive pulmonary disease | 569 (10%) | 245 (9%) | 324 (10%) | 0.024 * |
| History of percutaneous coronary intervention | 1267 (21%) | 531 (19%) | 736 (23%) | <0.001 * |
| History of coronary artery bypass graft | 213 (4%) | 83 (3%) | 130 (4%) | 0.009 * |
| History of myocardial infarction | 192 (3%) | 49 (2%) | 143 (5%) | <0.001 * |
| Laboratory data | ||||
| Hemoglobin, g/dL | 11.4 ± 1.6 | 11.4 ± 1.6 | 11.4 ± 1.7 | 0.70 |
| Serum albumin, g/dL | 3.8 ± 0.5 | 3.8 ± 0.5 | 3.7 ± 0.5 | <0.001 * |
| Serum sodium, mEq/L | 140.0 ± 3.3 | 140.0 ± 3.4 | 140.1 ± 3.3 | 0.26 |
| eGFR, mL/min/1.73m2 | 52.1 ± 18.9 | 53.1 ± 18.7 | 51.1 ± 19.0 | <0.001 * |
| Logarithm of plasma BNP, pg/mL | 2.28 ± 0.46 | 2.20 ± 0.45 | 2.37 ± 0.45 | <0.001 * |
| Echocardiographic data | ||||
| LVDd, mm | 42.7 ± 5.7 | 41.8 ± 5.4 | 43.5 ± 5.8 | <0.001 * |
| LVEF, % | 64.8 ± 7.3 | 71.0 ± 4.5 | 59.4 ± 4.2 | <0.001 * |
| Left atrial diameter, mm | 41.8 ± 7.3 | 41.3 ± 7.4 | 42.2 ± 7.2 | <0.001 * |
| Interventricular septum diameter, mm | 11.9 ± 2.2 | 11.9 ± 2.2 | 11.9 ± 2.1 | 0.96 |
| Posterior wall diameter, mm | 11.3 ± 2.0 | 11.3 ± 2.0 | 11.4 ± 2.0 | 0.64 |
| Moderate or greater AR | 569 (10%) | 235 (8%) | 334 (11%) | 0.002 * |
| Moderate or greater MR | 543 (9%) | 236 (8%) | 307 (10%) | 0.043 * |
| Moderate or greater TR | 494 (8%) | 238 (8%) | 256 (8%) | 0.32 |
| Peak velocity at aortic valve, m/s | 4.59 ± 0.77 | 4.62 ± 0.75 | 4.57 ± 0.79 | 0.10 |
| Mean pressure gradient at aortic valve, mmHg | 50.6 ± 18.2 | 50.6 ± 17.8 | 50.5 ± 18.6 | 0.82 |
| STS score | 7.1 ± 4.8 | 6.7 ± 4.5 | 7.4 ± 5.0 | <0.001 * |
| snLVEF (N = 2819) | nLVEF (N = 3170) | p-Value | |
|---|---|---|---|
| Peri-procedural complication | |||
| Acute kidney injury | 209 (7%) | 253 (8%) | 0.22 |
| Cardiac tamponade | 30 (1%) | 28 (0.9%) | 0.28 |
| Valve embolization | 11 (0.4%) | 5 (0.2%) | 0.068 |
| In-hospital complication | |||
| Coronary obstruction | 12 (0.4%) | 24 (0.8%) | 0.067 |
| Ischemic stroke | 54 (2%) | 76 (2%) | 0.12 |
| Hemorrhagic stroke | 5 (0.2%) | 6 (0.2%) | 0.58 |
| Disabling stroke | 23 (0.8%) | 35 (1%) | 0.16 |
| Transient ischemic attack | 3 (0.1%) | 6 (0.2%) | 0.32 |
| Major bleeding | 201 (7%) | 199 (6%) | 0.10 |
| Pacemaker implantation | 227/2691 (8%) | 261/3006 (9%) | 0.39 |
| New atrial fibrillation | 63 (2%) | 97 (3%) | 0.029 * |
| Major vascular complication | 102 (4%) | 103 (3%) | 0.24 |
| snLVEF (N = 405) | nLVEF (N = 252) | p Value | |
|---|---|---|---|
| LVDd, mm | 41.6 ± 5.0 | 43.1 ± 5.3 | <0.001 * |
| LVEF, % | 71.8 ± 7.2 | 67.5 ± 9.8 | <0.001 * |
| Interventricular septum diameter, mm | 10.3 ± 2.3 | 10.2 ± 2.1 | 0.47 |
| Posterior wall diameter, mm | 9.8 ± 2.0 | 9.8 ± 1.7 | 0.79 |
| Moderate or greater AR | 17 (4%) | 18 (7%) | 0.074 |
| Moderate or greater MR | 30 (7%) | 26 (10%) | 0.12 |
| Moderate or greater TR | 32 (8%) | 28 (11%) | 0.11 |
| Peak velocity at aortic valve, m/s | 2.40 ± 0.51 | 2.23 ± 0.44 | <0.001 * |
| Mean pressure gradient at aortic valve, mmHg | 12.6 ± 5.6 | 10.8 ± 4.7 | <0.001 * |
| LVOT peak velocity, m/s | 1.07 ± 0.32 | 0.98 ± 0.23 | 0.017 * |
| LVOT peak velocity > 2.0 m/s | 9 (2%) | 0 (0%) | 0.017 * |
| Unadjusted Analyses | Adjusted Analyses | |||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| Death or heart failure readmission | ||||
| snLVEF versus nLVEF | 0.93 (0.83–1.03) | 0.16 | 1.16 (1.02–1.31) | 0.023 * |
| LVEF, % | 0.99 (0.98–1.00) | 0.047 * | 1.01 (1.00–1.02) | 0.030 * |
| Death | ||||
| snLVEF versus nLVEF | 0.91 (0.81–1.04) | 0.16 | 1.20 (1.04–1.38) | 0.014 * |
| LVEF, % | 0.99 (0.98–1.00) | 0.021 * | 1.01 (0.99–1.02) | 0.055 |
| Heart failure readmission | ||||
| snLVEF versus nLVEF | 0.87 (0.72–1.04) | 0.12 | 0.95 (0.77–1.18) | 0.64 |
| LVEF, % | 0.99 (0.98–1.01) | 0.091 | 1.01 (0.99–1.02) | 0.097 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, T.; Hida, Y.; Ueno, H.; Kinugawa, K.; Yashima, F.; Tada, N.; Yamawaki, M.; Shirai, S.; Naganuma, T.; Yamanaka, F.; et al. Clinical Implication of Supra-Normal Left Ventricular Ejection Fraction in Patients Undergoing Transcatheter Aortic Valve Replacement. J. Clin. Med. 2023, 12, 7429. https://doi.org/10.3390/jcm12237429
Imamura T, Hida Y, Ueno H, Kinugawa K, Yashima F, Tada N, Yamawaki M, Shirai S, Naganuma T, Yamanaka F, et al. Clinical Implication of Supra-Normal Left Ventricular Ejection Fraction in Patients Undergoing Transcatheter Aortic Valve Replacement. Journal of Clinical Medicine. 2023; 12(23):7429. https://doi.org/10.3390/jcm12237429
Chicago/Turabian StyleImamura, Teruhiko, Yuki Hida, Hiroshi Ueno, Koichiro Kinugawa, Fumiaki Yashima, Norio Tada, Masahiro Yamawaki, Shinichi Shirai, Toru Naganuma, Futoshi Yamanaka, and et al. 2023. "Clinical Implication of Supra-Normal Left Ventricular Ejection Fraction in Patients Undergoing Transcatheter Aortic Valve Replacement" Journal of Clinical Medicine 12, no. 23: 7429. https://doi.org/10.3390/jcm12237429
APA StyleImamura, T., Hida, Y., Ueno, H., Kinugawa, K., Yashima, F., Tada, N., Yamawaki, M., Shirai, S., Naganuma, T., Yamanaka, F., Noguchi, M., Mizutani, K., Takagi, K., Watanabe, Y., Yamamoto, M., Asami, M., Izumo, M., Ohno, Y., Nishida, H., ... on behalf of the OCEAN-TAVI Investigators. (2023). Clinical Implication of Supra-Normal Left Ventricular Ejection Fraction in Patients Undergoing Transcatheter Aortic Valve Replacement. Journal of Clinical Medicine, 12(23), 7429. https://doi.org/10.3390/jcm12237429