


Microvesicles Are Associated with Early Veno Venous ECMO Circuit Change during Severe ARDS: A Prospective Observational Pilot Study

 , , and
, , and
Abstract
:1. Background
2. Methods
2.1. Study Design
2.2. ECMO Management
2.3. Anti-Coagulation Management and Transfusions Thresholds
2.4. Mechanical Ventilation Management
2.5. Sedation and Neuromuscular Blockers Utilization
2.6. Indications for ECMO Circuit Change
2.7. Blood Samples and Microparticles Cytometry Analysis
2.8. Statistical Analysis
3. Results
3.1. Patients
3.2. Membrane Oxygenator Efficiency during ECMO Run
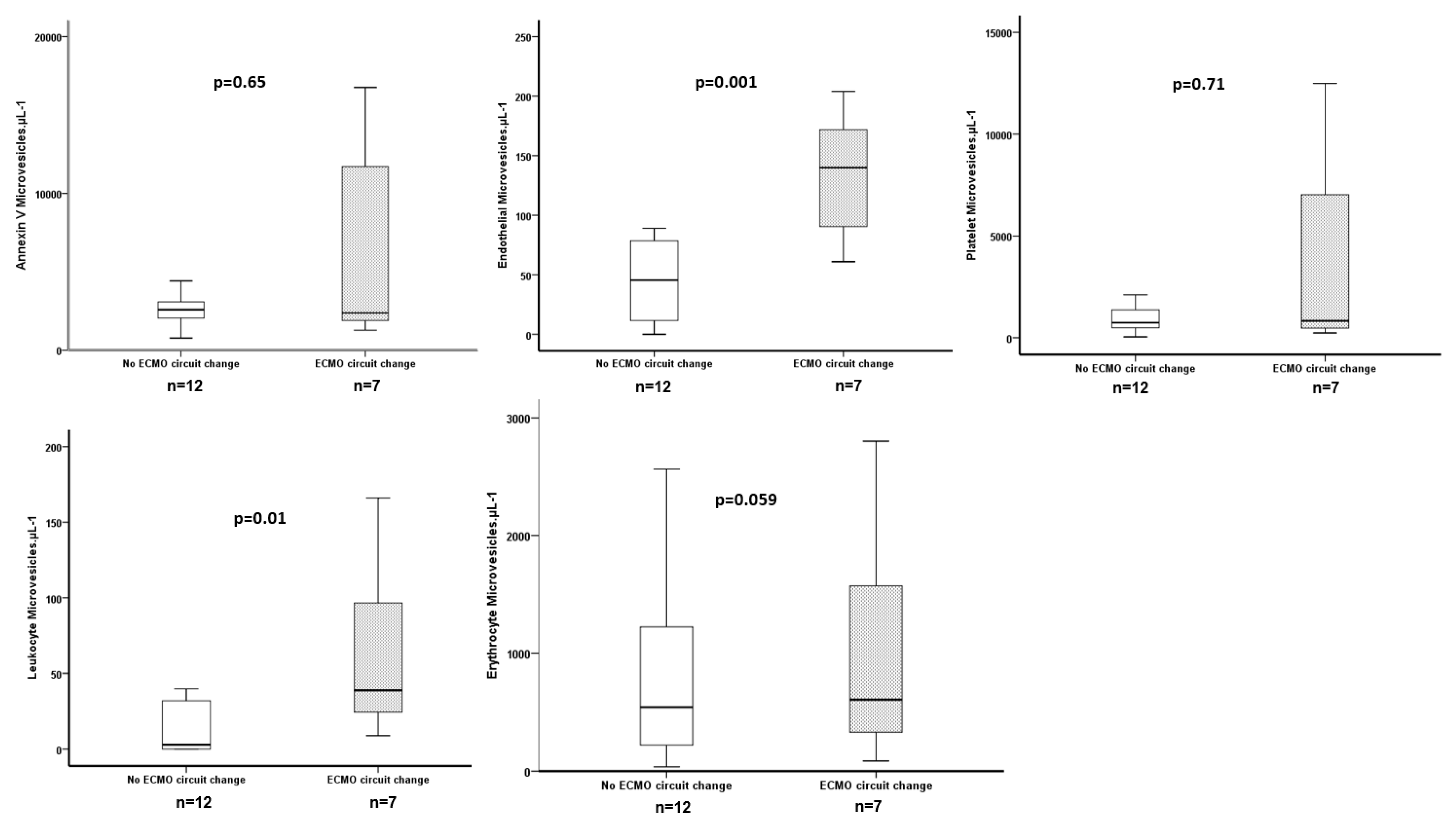
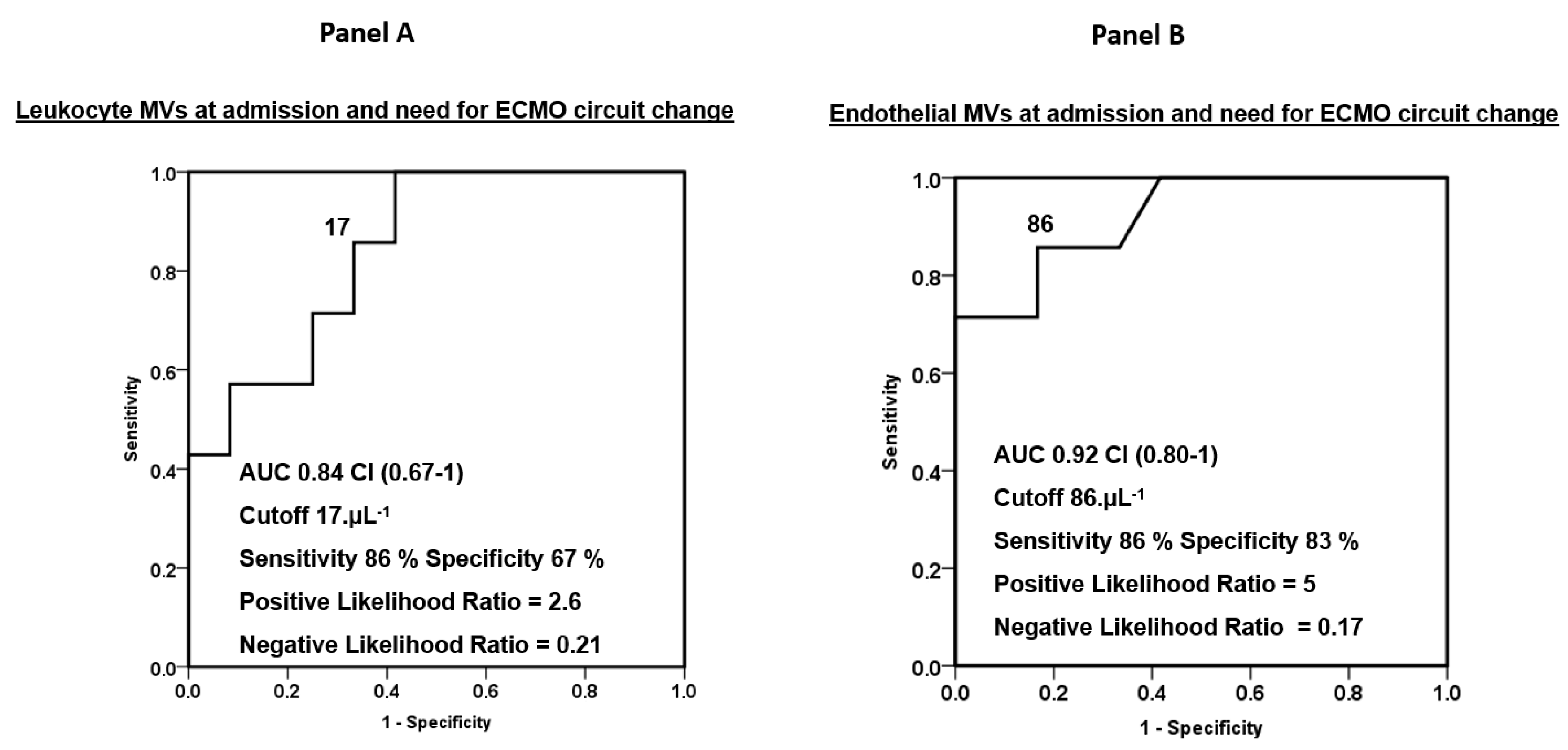
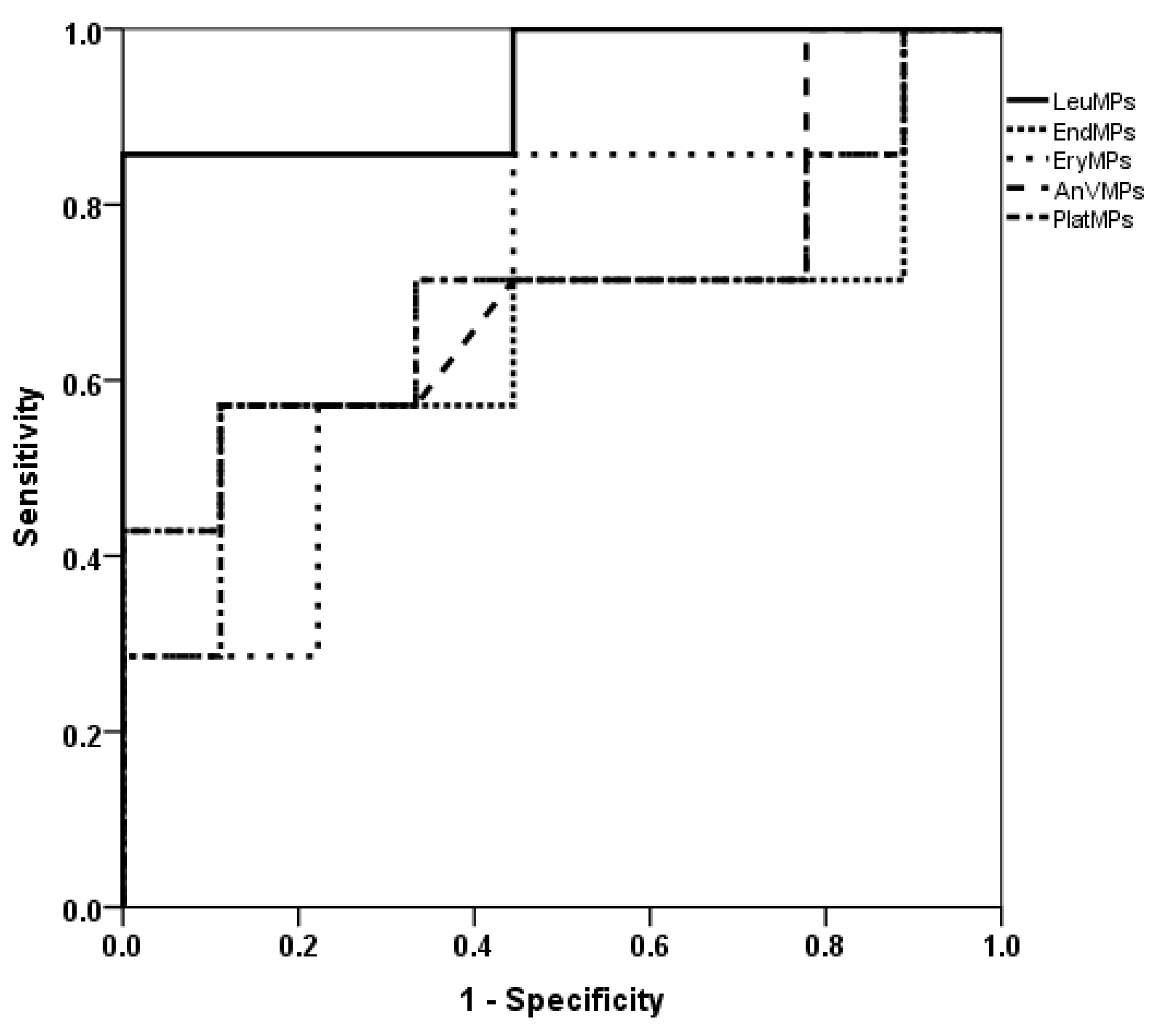
3.3. ECMO Circuit Change and Subpopulations of MPs
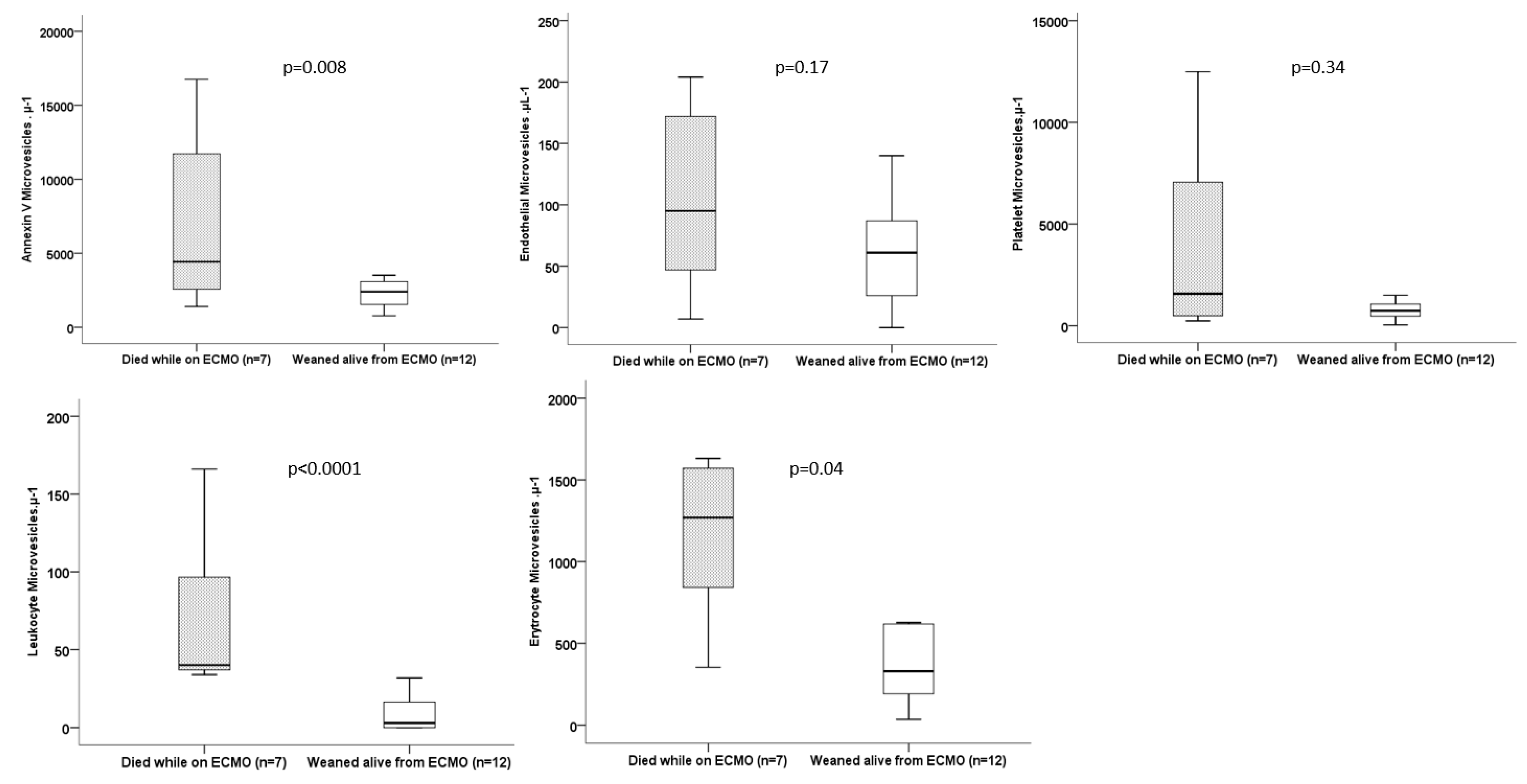
3.4. Outcomes and Subpopulations of MVs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef] [PubMed]
- Aubron, C.; DePuydt, J.; Belon, F.; Bailey, M.; Schmidt, M.; Sheldrake, J.; Murphy, D.; Scheinkestel, C.; Cooper, D.J.; Capellier, G.; et al. Predictive factors of bleeding events in adults undergoing extracorporeal membrane oxygenation. Ann. Intensiv. Care 2016, 6, 97. [Google Scholar] [CrossRef] [PubMed]
- Šoltés, J.; Skribuckij, M.; Říha, H.; Lipš, M.; Michálek, P.; Balík, M.; Pořízka, M. Update on Anticoagulation Strategies in Patients with ECMO-A Narrative Review. J. Clin. Med. 2023, 12, 6067. [Google Scholar] [CrossRef]
- Lehle, K.; Philipp, A.; Zeman, F.; Lunz, D.; Lubnow, M.; Wendel, H.P.; Göbölös, L.; Schmid, C.; Müller, T. Technical induced hemolysis in patients with respiratory failure supported with venovenous ECMO-prevalence and risk factors. PLoS ONE 2015, 10, e0143527. [Google Scholar] [CrossRef]
- Valladolid, C.; Yee, A.; Cruz, M.A. von Willebrand Factor, Free Hemoglobin and Thrombosis in ECMO. Front. Med. 2018, 5, 228. [Google Scholar] [CrossRef] [PubMed]
- Delabranche, X.; Quenot, J.P.; Lavigne, T.; Mercier, E.; François, B.; Severac, F.; Grunebaum, L.; Mehdi, M.; Zobairi, F.; Toti, F.; et al. Early Detection of Disseminated Intravascular Coagulation During Septic Shock: A Multicenter Prospective Study. Crit. Care Med. 2016, 44, e930–e939. [Google Scholar] [CrossRef] [PubMed]
- Ohuchi, M.; Fujino, K.; Kishimoto, T.; Yamane, T.; Hamamoto, T.; Tabata, T.; Tsujita, Y.; Matsushita, M.; Takahashi, K.; Matsumura, K.; et al. Association of the Plasma Platelet-Derived Microparticles to Platelet Count Ratio with Hospital Mortality and Disseminated Intravascular Coagulopathy in Critically Ill Patients. J. Atheroscler. Thromb. 2015, 22, 773–782. [Google Scholar] [CrossRef]
- Densmore, J.C.; Signorino, P.R.; Ou, J.; Hatoum, O.A.; Rowe, J.J.; Shi, Y.; Kaul, S.; Jones, D.W.; Sabina, R.E.; Pritchard, K.A.; et al. Endothelium-derived microparticles induce endothelial dysfunction and acute lung injury. Shock 2006, 26, 464–471. [Google Scholar] [CrossRef]
- Guervilly, C.; Lacroix, R.; Forel, J.M.; Roch, A.; Camoin-Jau, L.; Papazian, L.; Dignat-George, F. High levels of circulating leukocyte microparticles are associated with better outcome in acute respiratory distress syndrome. Crit. Care 2011, 15, R31. [Google Scholar] [CrossRef]
- Guervilly, C.; Bonifay, A.; Burtey, S.; Sabatier, F.; Cauchois, R.; Abdili, E.; Arnaud, L.; Lano, G.; Pietri, L.; Robert, T.; et al. Dissemination of extreme levels of extracellular vesicles: Tissue factor activity in patients with severe COVID-19. Blood Adv. 2021, 5, 628–634. [Google Scholar] [CrossRef]
- Meyer, A.D.; Gelfond, J.A.; Wiles, A.A.; Freishtat, R.J.; Rais-Bahrami, K. Platelet-derived microparticles generated by neonatal extracorporeal membrane oxygenation systems. ASAIO J. 2015, 61, 37–42. [Google Scholar] [CrossRef]
- Nieuwland, R.; Berckmans, R.J.; Rotteveel-Eijkman, R.C.; Maquelin, K.N.; Roozendaal, K.J.; Jansen, P.G.; Have, K.T.; Eijsman, L.; Hack, C.E.; Sturk, A. Cell-derived microparticles generated in patients during cardiopulmonary bypass are highly procoagulant. Circulation 1997, 96, 3534–3541. [Google Scholar] [CrossRef] [PubMed]
- Siegel, P.M.; Hentschel, D.; Bojti, I.; Wengenmayer, T.; Helbing, T.; Moser, M.; Duerschmied, D.; Trummer, G.; Bode, C.; Diehl, P. Annexin V positive microvesicles are elevated and correlate with flow rate in patients receiving veno-arterial extracorporeal membrane oxygenation. Interact. Cardiovasc. Thorac. Surg. 2020, 31, 884–891. [Google Scholar] [CrossRef]
- ARDS Definition of Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Roch, A.; Hraiech, S.; Masson, E.; Grisoli, D.; Forel, J.M.; Boucekine, M.; Morera, P.; Guervilly, C.; Adda, M.; Dizier, S.; et al. Outcome of acute respiratory distress syndrome patients treated with extracorporeal membrane oxygenation and brought to a referral center. Intensiv. Care Med. 2014, 40, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Robert, S.; Lacroix, R.; Poncelet, P.; Harhouri, K.; Bouriche, T.; Judicone, C.; Wischhusen, J.; Arnaud, L.; Dignat-George, F. High-sensitivity flow cytometry provides access to standardized measurement of small-size microparticles—Brief report. Arter. Thromb. Vasc. Biol. 2012, 32, 1054–1058. [Google Scholar] [CrossRef]
- Genty, T.; Burguburu, S.; Imbert, A.; Roman, C.; Camille, W.; Thès, J.; Stéphan, F. Circuit change during extracorporeal membrane oxygenation: Single-center retrospective study of 48 changes. Crit. Care 2023, 27, 219. [Google Scholar] [CrossRef]
- Lubnow, M.; Philipp, A.; Foltan, M.; Enger, T.B.; Lunz, D.; Bein, T.; Haneya, A.; Schmid, C.; Riegger, G.; Müller, T.; et al. Technical complications during veno-venous extracorporeal membrane oxygenation and their relevance predicting a system-exchange--retrospective analysis of 265 cases. PLoS ONE 2014, 9, e112316. [Google Scholar] [CrossRef]
- Hafezi, N.; Markel, T.A.; Mark, N.M.; Colgate, C.L.; Shah, S.; Ninad, N.; Masso Maldonado, S.; Gray, B.W. Circuit change in neonatal and pediatric extracorporeal membrane oxygenation is associated with adverse outcomes. Perfusion 2023, 2676591231199718, epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Dalton, H.J.; Reeder, R.; Garcia-Filion, P.; Holubkov, R.; Berg, R.A.; Zuppa, A.; Moler, F.W.; Shanley, T.; Pollack, M.M.; Newth, C.; et al. Factors Associated with Bleeding and Thrombosis in Children Receiving Extracorporeal Membrane Oxygenation. Am. J. Respir. Crit. Care Med. 2017, 196, 762–771. [Google Scholar] [CrossRef] [PubMed]
- Dornia, C.; Philipp, A.; Bauer, S.; Hoffstetter, P.; Lehle, K.; Schmid, C.; Lubnow, M.; Stroszczynski, C.; Schreyer, A.G. Visualization of thrombotic deposits in extracorporeal membrane oxygenation devices using multidetector computed tomography: A feasibility study. ASAIO J. 2013, 59, 439–441. [Google Scholar] [CrossRef] [PubMed]
- Dornia, C.; Philipp, A.; Bauer, S.; Lubnow, M.; Müller, T.; Lehle, K.; Schmid, C.; Müller-Wille, R.; Wiggermann, P.; Stroszczynski, C.; et al. Analysis of thrombotic deposits in extracorporeal membrane oxygenators by multidetector computed tomography. ASAIO J. 2014, 60, 652–656, Erratum in ASAIO J. 2015, 61, e13. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N = 19 |
|---|---|
| Age (years) | 3 ± 17 |
| Gender (male), n (%) | 14 (74) |
| Body mass index (kg·m−2) | 27 ± 6 |
| Simplified Acute Physiologic Score II at admission | 46 ± 14 |
| Sequential Organ Failure Assessment Score at inclusion | 10 ± 3 |
| ARDS main risk factor, n | |
| Bacterial pneumonia | 10 |
| Viral pneumonia | 2 |
| Aspiration pneumonia | 2 |
| Grade 3 primary graft dysfunction following lung transplantation | 2 |
| Alveolar hemorrhage | 1 |
| Pancreatitis | 1 |
| Peritonitis | 1 |
| ECMO duration (days) | 12 ± 7 |
| ECMO circuit change, n (%) | 7 (37) |
| Weaning from ECMO, n (%) | 12 (63) |
| Mechanical ventilation duration (days) | 25 ± 17 |
| ICU length of stay (days) | 25 ± 17 |
| ICU survival, n (%) | 11 (58) |
| Blood products consumption during ECMO run | |
| Red packed blood cells | 11 ± 9 |
| Plasma concentrates | 1.4 ± 2.8 |
| Platelet concentrates | 1.4 ± 1.8 |
| Fibrinogen, g | 0.4 ± 1.4 |
| Recombinant antithrombin III, IU | 950 ± 2275 |
| All Population N = 19 | Died While on ECMO N = 7 | Weaned Alive from ECMO N = 12 | p Value | |
|---|---|---|---|---|
| Configuration | 1 | |||
| Femoro-jugular, n (%) | 18 (95) | 7 (100) | 11 (92) | |
| Femoro-femoral, n (%) | 1 (5) | 0 (0) | 1 (8) | |
| ECMO flow, L·min−1 | 4.7 (4–4.9) | 4.4 (3.9–4.9) | 4.7 (4.4–5) | 0.2 |
| Revolutions per minute | 2830 (2625–3080) | 2740 (2680–3130) | 2885 (2437–3067) | 0.8 |
| Sweep gas flow, L·min−1 | 6 (5–7) | 6 (5–6.5) | 6 (5–7) | 0.8 |
| PaO2 post oxy (mmHg) | 494 (453–510) | 513 (488–538) | 471 (450–499) | 0.08 |
| All Population N = 19 | Died While on ECMO N = 7 | Weaned Alive from ECMO N = 12 | p Value | |
|---|---|---|---|---|
| Leucocytes, Giga/L | 18 (10–24) | 20 (10–36) | 16 (10–24) | 0.5 |
| Red blood cells, Tera/L | 3 (2.8–3.6) | 3 (2.9–3.3) | 3.2 (2.6-3.6) | 0.9 |
| Hemoglobin, g/dL | 9.1 (8.4–10.3) | 8.7 (8.4–9) | 9.7 (8.3–11.1) | 0.2 |
| Platelet, Giga/L | 206 (111–275) | 170 (45–333) | 213 (114–258) | 0.7 |
| Prothrombin activity, % | 62 (49–69) | 55 (39–66) | 68 (53–70) | 0.04 |
| Fibrinogen, g/L | 5.5 (4.3–7.6) | 5.2 (2.4–6.4) | 6.4 (4.6–8.2) | 0.07 |
| aPTT, s | 45 (36–50) | 38 (34–52) | 45 (40–50) | 0.6 |
| Antithrombin activity, % | 51 (48–84) | 50 (34–85) | 52 (49–87) | 0.4 |
| lactate dehydrogenase (IU/L) | 1348 (876–2550) | 2550 (647–3818) | 1309 (928–2222) | 0.5 |
| Lactate, mmol/L | 2.4 (1.6–5.2) | 2.4 (1.5–5.8) | 2.2 (1.6–4.9) | 0.7 |
| Procalcitonin, µg/L | 1.8 (0.8–5.4) | 1.8 (1.1–19) | 2.4 (0.4–5.2) | 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guervilly, C.; Bousquet, G.; Arnaud, L.; Gragueb-Chatti, I.; Daviet, F.; Adda, M.; Forel, J.-M.; Dignat-George, F.; Papazian, L.; Roch, A.; et al. Microvesicles Are Associated with Early Veno Venous ECMO Circuit Change during Severe ARDS: A Prospective Observational Pilot Study. J. Clin. Med. 2023, 12, 7281. https://doi.org/10.3390/jcm12237281
Guervilly C, Bousquet G, Arnaud L, Gragueb-Chatti I, Daviet F, Adda M, Forel J-M, Dignat-George F, Papazian L, Roch A, et al. Microvesicles Are Associated with Early Veno Venous ECMO Circuit Change during Severe ARDS: A Prospective Observational Pilot Study. Journal of Clinical Medicine. 2023; 12(23):7281. https://doi.org/10.3390/jcm12237281
Chicago/Turabian StyleGuervilly, Christophe, Giovanni Bousquet, Laurent Arnaud, Ines Gragueb-Chatti, Florence Daviet, Mélanie Adda, Jean-Marie Forel, Françoise Dignat-George, Laurent Papazian, Antoine Roch, and et al. 2023. "Microvesicles Are Associated with Early Veno Venous ECMO Circuit Change during Severe ARDS: A Prospective Observational Pilot Study" Journal of Clinical Medicine 12, no. 23: 7281. https://doi.org/10.3390/jcm12237281
APA StyleGuervilly, C., Bousquet, G., Arnaud, L., Gragueb-Chatti, I., Daviet, F., Adda, M., Forel, J.-M., Dignat-George, F., Papazian, L., Roch, A., Lacroix, R., & Hraiech, S. (2023). Microvesicles Are Associated with Early Veno Venous ECMO Circuit Change during Severe ARDS: A Prospective Observational Pilot Study. Journal of Clinical Medicine, 12(23), 7281. https://doi.org/10.3390/jcm12237281