
Can the Modified Frailty Index (mFI) Predict Intraoperative and Postoperative Complications in Older Women with Endometrial Cancer Undergoing Laparoscopic or Robotic Surgery? A Multicenter Observational Study

 ,
,  ,
,  ,
,  ,
, 
 , , ,
, , ,  ,
,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
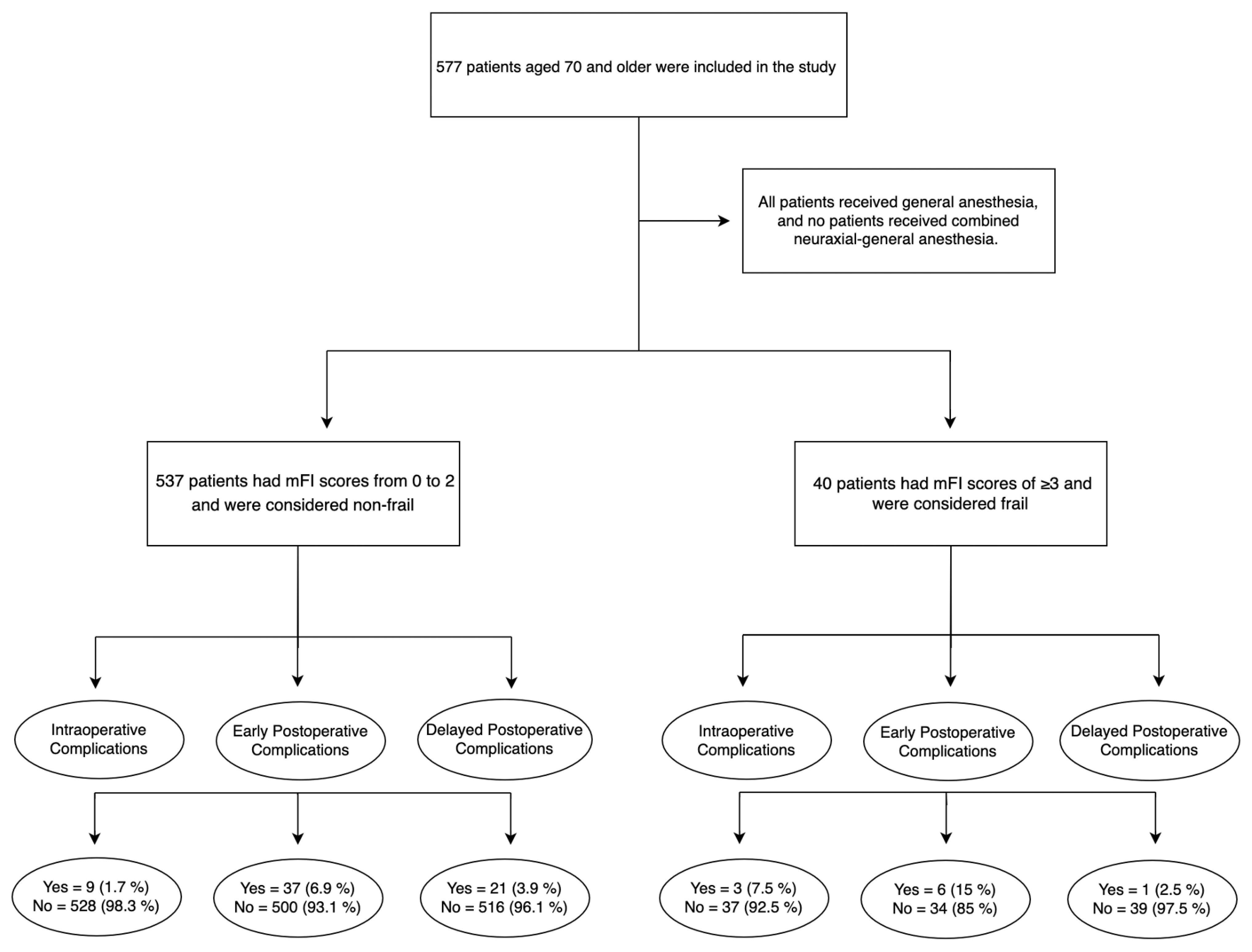
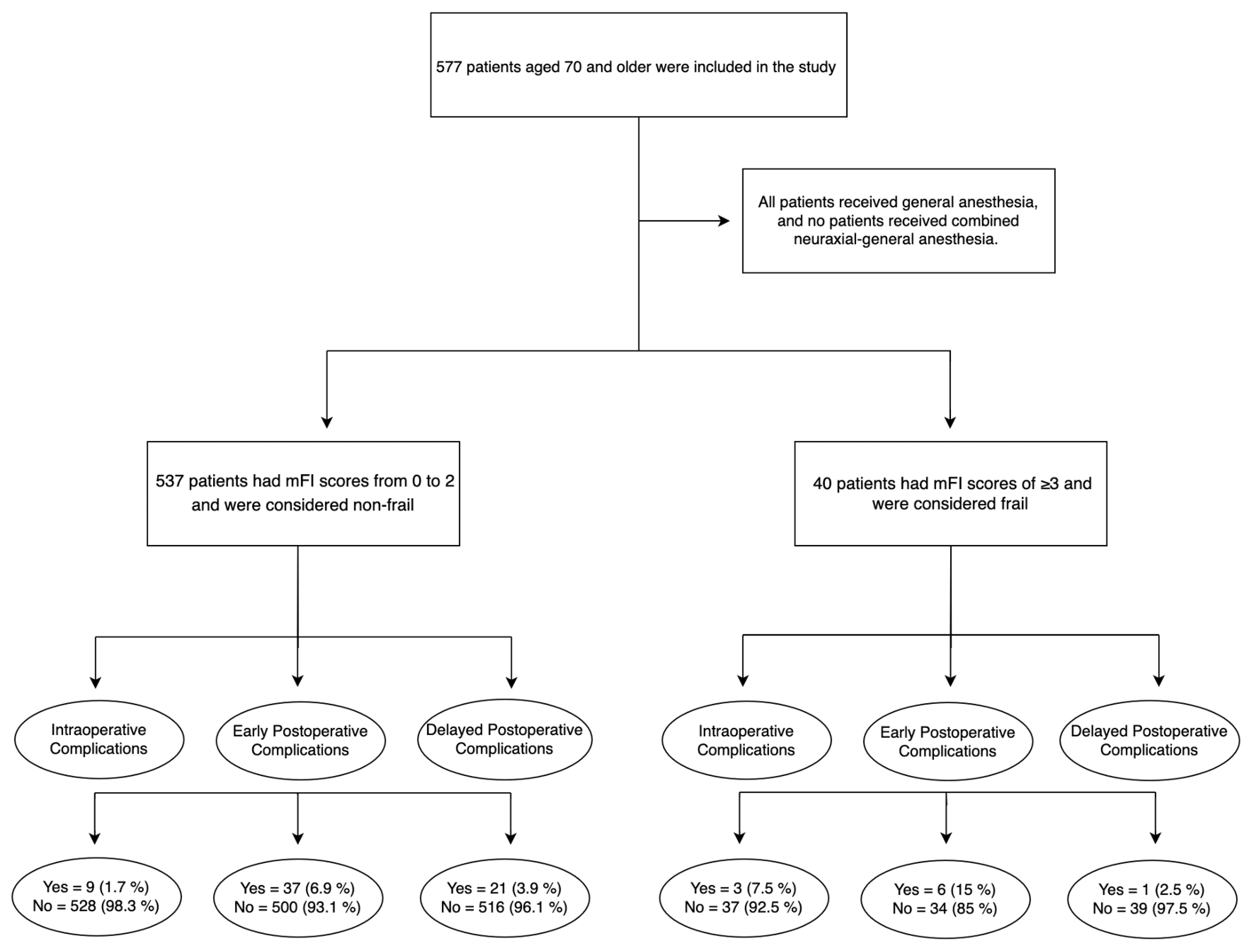
2.1. Study Design and Population
2.2. Intraoperative Anesthesiological Management
2.3. mFI-11
2.4. Statistical Analysis
3. Results
3.1. Patient Clinical Characteristics
3.2. Perioperative Outcomes
3.3. Multiple Logistic Regression Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaul, E.; Barron, J. Characterizing the Heterogeneity of Aging: A Vision for a Staging System for Aging. Front. Public Health 2021, 9, 513–557. [Google Scholar] [CrossRef]
- Watt, J.; Tricco, A.C.; Talbot-Hamon, C.; Pham, B.; Rios, P.; Grudniewicz, A.; Wong, C.; Sinclair, D.; Straus, S.E. Identifying older adults at risk of harm following elective surgery: A systematic review and meta-analysis. BMC Med. 2018, 16, 2. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, C.A.; Placide, S.; Lipsitz, L.A.; Marcantonio, E.R. Preoperative Frailty Assessment and Outcomes at 6 Months or Later in Older Adults Undergoing Cardiac Surgical Procedures: A Systematic Review. Ann. Intern. Med. 2016, 165, 650–660. [Google Scholar] [CrossRef]
- Lin, H.S.; Watts, J.N.; Peel, N.M.; Hubbard, R.E. Frailty and post-operative outcomes in older surgical patients: A systematic review. BMC Geriatr. 2016, 16, 157. [Google Scholar] [CrossRef]
- Ripa, M.; Schipa, C.; Rizzo, S.; Sollazzi, L.; Aceto, P. Is the visual impairment a risk factor for frailty in older adults? A systematic review and meta-analysis of 10-year clinical studies. Aging Clin. Exp. Res. 2023, 35, 227–244. [Google Scholar] [CrossRef]
- George, E.M.; Burke, W.M.; Hou, J.Y.; Tergas, A.I.; Chen, L.; Neugut, A.I.; Ananth, C.V.; Hershman, D.L.; Wright, J.D. Measurement and validation of frailty as a predictor of outcomes in women undergoing major gynaecological surgery. BJOG 2016, 123, 455–461. [Google Scholar] [CrossRef]
- Velanovich, V.; Antoine, H.; Swartz, A.; Peters, D.; Rubinfeld, I. Accumulating deficits model of frailty and postoperative mortality and morbidity: Its application to a national database. J. Surg. Res. 2013, 183, 104–110. [Google Scholar] [CrossRef]
- Aceto, P.; Bassi, P.; Sollazzi, L.; Racioppi, M.; Fortunato, G.; Di Gianfrancesco, L.; Marusco, I.; Ragonese, M.; Cataldo, A.; Palermo, G. Implementation of frailty preoperative assessment to predict outcome in patients undergoing urological surgery: A systematic review and meta-analysis. BJU Int. 2021, 127, 507–517. [Google Scholar] [CrossRef]
- Aceto, P.; Antonelli Incalzi, R.; Bettelli, G.; Carron, M.; Chiumiento, F.; Corcione, A.; Crucitti, A.; Maggi, S.; Montorsi, M.; Pace, M.C.; et al. Perioperative Management of Elderly patients (PriME): Recommendations from an Italian intersociety consensus. Aging Clin. Exp. Res. 2020, 32, 1647–1673. [Google Scholar] [CrossRef]
- Aceto, P.; Perilli, V.; Luca, E.; Schipa, C.; Calabrese, C.; Fortunato, G.; Marusco, I.; Lai, C.; Sollazzi, L. Predictive power of modified frailty index score for pulmonary complications after major abdominal surgery in the elderly: A single centre prospective cohort study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3798–3802. [Google Scholar]
- Di Donato, V.; Caruso, G.; Bogani, G.; Giannini, A.; D’Oria, O.; Perniola, G.; Palaia, I.; Plotti, F.; Angioli, R.; Muzii, L.; et al. Preoperative frailty assessment in patients undergoing gynecologic oncology surgery: A systematic review. Gynecol. Oncol. 2021, 161, 11–19. [Google Scholar] [CrossRef]
- Inci, M.G.; Anders, L.; Heise, K.; Richter, R.; Woopen, H.; Sehouli, J. Can Fried Frailty Score predict postoperative morbidity and mortality in gynecologic cancer surgery? Results of a prospective study. J. Geriatr. Oncol. 2021, 12, 428–433. [Google Scholar] [CrossRef]
- Chambers, L.M.; Chalif, J.; Yao, M.; Chichura, A.; Morton, M.; Gruner, M.; Costales, A.B.; Horowitz, M.; Chau, D.B.; Vargas, R.; et al. Modified frailty index predicts postoperative complications in women with gynecologic cancer undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Gynecol. Oncol. 2021, 162, 368–374. [Google Scholar] [CrossRef]
- Adedayo, P.; Resnick, K.; Singh, S. Preoperative frailty is a risk factor for non-home discharge in patients undergoing surgery for endometrial cancer. J. Geriatr. Oncol. 2018, 9, 513–515. [Google Scholar] [CrossRef]
- Vaknin, Z.; Perri, T.; Lau, S.; Deland, C.; Drummond, N.; Rosberger, Z.; Gourdji, I.; Gotlieb, W.H. Outcome and quality of life in a prospective cohort of the first 100 robotic surgeries for endometrial cancer, with focus on elderly patients. Int. J. Gynecol. Cancer 2010, 20, 1367–1373. [Google Scholar]
- Lavoue, V.; Zeng, X.; Lau, S.; Press, J.Z.; Abitbol, J.; Gotlieb, R.; How, J.; Wang, Y.; Gotlieb, W.H. Impact of robotics on the outcome of elderly patients with endometrial cancer. Gynecol. Oncol. 2014, 133, 556–562. [Google Scholar] [CrossRef]
- Daix, M.; Martinez Gomez, C.; Angeles, M.A.; Tock, S.; Gladieff, L.; Gabiache, E.; Mery, E.; Martinez, A.; Cibula, D.; Ferron, G. Extended pelvic resection for gynecological malignancies: A review of out-of-the-box surgery. Gynecol. Oncol. 2022, 165, 393–400. [Google Scholar] [CrossRef]
- European Society of Gynaecological Oncology Guidelines, ESGO-ESTRO-ESP Endometrial Cancer Guidelines. Available online: https://guidelines.esgo.org/uterine-cancer/guidelines/advanced-stage-algorithms/ (accessed on 25 March 2023).
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Nag, K.; Singh, D.R.; Shetti, A.N.; Kumar, H.; Sivashanmugam, T.; Parthasarathy, S. Sugammadex: A revolutionary drug in neuromuscular pharmacology. Anesth. Essays Res. 2013, 7, 302–306. [Google Scholar]
- Uppal, S.; Igwe, E.; Rice, L.W.; Spencer, R.J.; Rose, S.L. Frailty index predicts severe complications in gynecologic oncology patients. Gynecol. Oncol. 2015, 137, 98–101. [Google Scholar] [CrossRef]
- Kumar, A.; Langstraat, C.L.; DeJong, S.R.; McGree, M.E.; Bakkum-Gamez, J.N.; Weaver, A.L.; LeBrasseur, N.K.; Cliby, W.A. Functional not chronologic age: Frailty index predicts outcomes in advanced ovarian cancer. Gynecol. Oncol. 2017, 147, 104–109. [Google Scholar] [CrossRef]
- Bossy, M.; Nyman, M.; Madhuri, T.K.; Tailor, A.; Chatterjee, J.; Butler-Manuel, S.; Ellis, P.; Feldheiser, A.; Creagh-Brown, B. The need for post-operative vasopressor infusions after major gynae-oncologic surgery within an ERAS (Enhanced Recovery After Surgery) pathway. Perioper. Med. 2020, 9, 26. [Google Scholar] [CrossRef]
- Mullen, M.M.; Porcelli, B.P.; Cripe, J.; Massad, L.S.; Kuroki, L.M.; Novetsky, A.P.; Wan, L.; Powell, M.A.; Mutch, D.G.; Thaker, P.H. Modified frailty index is predictive of wound complications in obese patients undergoing gynecologic surgery via a midline vertical incision. Gynecol. Oncol. 2020, 157, 287–292. [Google Scholar] [CrossRef]
- Giannini, A.; Di Donato, V.; Schiavi, M.C.; May, J.; Panici, P.B.; Congiu, M.A. Predictors of postoperative overall and severe complications after surgical treatment for endometrial cancer: The role of the fragility index. Int. J. Gynaecol. Obstet. 2020, 148, 174–180. [Google Scholar] [CrossRef]
- Pichatechaiyoot, A.; Thannil, S.; Boonyapipat, S.; Buhachat, R. Preoperative modified frailty index to predict surgical complications in endometrial cancer patients. Obstet. Gynecol. Sci. 2022, 65, 513–521. [Google Scholar] [CrossRef]
- Courtney-Brooks, M.; Tellawi, A.R.; Scalici, J.; Duska, L.R.; Jazaeri, A.A.; Modesitt, S.C.; Cantrell, L.A. Frailty: An outcome predictor for elderly gynecologic oncology patients. Gynecol. Oncol. 2012, 126, 20–24. [Google Scholar] [CrossRef]
- Driver, J.A.; Viswanathan, A.N. Frailty measure is more predictive of outcomes after curative therapy for endometrial cancer than traditional risk factors in women 60 and older. Gynecol. Oncol. 2017, 145, 526–530. [Google Scholar] [CrossRef]
- Nakhla, M.; Eakin, C.M.; Mandelbaum, A.; Karlan, B.; Benharash, P.; Salani, R.; Cohen, J.G. Frailty is independently associated with worse outcomes and increased resource utilization following endometrial cancer surgery. Int. J. Gynecol. Cancer 2022, 32, 1135–1140. [Google Scholar] [CrossRef]
- Sia, T.Y.; Wen, T.; Cham, S.; Friedman, A.M.; Wright, J.D. The effect of frailty on postoperative readmissions, morbidity, and mortality in endometrial cancer surgery. Gynecol. Oncol. 2021, 161, 353–360. [Google Scholar] [CrossRef]
- Anic, K.; Flohr, F.; Schmidt, M.W.; Krajnak, S.; Schwab, R.; Schmidt, M.; Westphalen, C.; Eichelsbacher, C.; Ruckes, C.; Brenner, W.; et al. Frailty assessment tools predict perioperative outcome in elderly patients with endometrial cancer better than age or BMI alone: A retrospective observational cohort study. J. Cancer Res. Clin. Oncol. 2023, 149, 1551–1560. [Google Scholar] [CrossRef]
- Erekson, E.A.; Yip, S.O.; Ciarleglio, M.M.; Fried, T.R. Postoperative complications after gynecologic surgery. Obstet. Gynecol. 2021, 118, 785–793. [Google Scholar] [CrossRef]
- Homes, R.A.P.; Giddens, F.; Francis, R.S.; Hubbard, R.E.; Gordon, E.H.; Midwinter, M.J. The sublingual microcirculation and frailty index in chronic kidney disease patients. Microcirculation 2023, 30, e12819. [Google Scholar] [CrossRef]
- Schipa, C.; Luca, E.; Ripa, M.; Sollazzi, L.; Aceto, P. Preoperative evaluation of the elderly patient. Saudi J. Anaesth. 2023, 17, 482–490. [Google Scholar]
- Aceto, P.; Beretta, L.; Cariello, C.; Claroni, C.; Esposito, C.; Forastiere, E.M.; Guarracino, F.; Perucca, R.; Romagnoli, S.; Sollazzi, L.; et al. Joint consensus on anesthesia in urologic and gynecologic robotic surgery: Specific issues in management from a task force of the SIAARTI, SIGO, and SIU. Minerva Anestesiol. 2019, 85, 871–885. [Google Scholar] [CrossRef]
- Aloisi, A.; Tseng, J.; Kuhn, T.; Feinberg, J.; Chi, D.S.; Brown, C.L.; Mueller, J.J.; Gardner, G.J.; Zivanovic, O.; Jewell, E.L.; et al. Robotic Surgery in the Frail Elderly: Analysis of Perioperative Outcomes. Ann. Surg. Oncol. 2020, 27, 3772–3780. [Google Scholar] [CrossRef]
- Corrado, G.; Vizza, E.; Perrone, A.M.; Mereu, L.; Cela, V.; Legge, F.; Hilaris, G.; Pasciuto, T.; D’Indinosante, M.; La Fera, E.; et al. Comparison Between Laparoscopic and Robotic Surgery in Elderly Patients With Endometrial Cancer: A Retrospective Multicentric Study. Front. Oncol. 2021, 11, 724886. [Google Scholar] [CrossRef]
- Gallotta, V.; Conte, C.; D’Indinosante, M.; Federico, A.; Biscione, A.; Vizzielli, G.; Bottoni, C.; Carbone, M.V.; Legge, F.; Uccella, S.; et al. Robotic Surgery in Elderly and Very Elderly Gynecologic Cancer Patients. J. Minim. Invasive Gynecol. 2018, 25, 872–877. [Google Scholar] [CrossRef]
- Hall, D.E.; Youk, A.; Allsup, K.; Kennedy, K.; Byard, T.D.; Dhupar, R.; Chu, D.; Rahman, A.M.; Wilson, M.; Cahalin, L.P.; et al. Preoperative Rehabilitation Is Feasible in the Weeks Prior to Surgery and Significantly Improves Functional Performance. J. Frailty Aging 2022, 1, 10. [Google Scholar] [CrossRef]
- Kenig, J.; Olszewska, U.; Zychiewicz, B.; Barczynski, M.; Mituś-Kenig, M. Cumulative deficit model of geriatric assessment to predict the postoperative outcomes of older patients with solid abdominal cancer. J. Geriatr. Oncol. 2015, 6, 370–379. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Overall (n = 577) | Non-Frail (n = 537) | Frail (n = 40) | p Value |
|---|---|---|---|---|
| Mean Age (yrs.) | 76.45 ± 4.72 | 76.44 ± 4.75 | 76.55 ± 4.27 | 0.89 |
| BMI (Kg/m2) | 29.39 ± 5.92 | 29.35 ± 6.99 | 29.91 ± 4.93 | 0.56 |
| Medical Comorbidities | ||||
| HTN (n%) | 377 (65.3%) | 343 (63.9%) | 34 (85%) | <0.01 * |
| DM (n%) | 130 (22.5%) | 105 (19.6%) | 25 (62.5%) | <0.01 * |
| TIA (n%) | 8 (1.4%) | 3 (0.6%) | 5 (12.5%) | <0.01 * |
| CAD (n%) | 18 (3.1%) | 1 (0.2%) | 17 (42.5%) | <0.01 * |
| VTE (n%) | 26 (4.5%) | 17 (3.2%) | 9 (22.5%) | <0.01 * |
| Stroke (n%) | 6 (1.0%) | 1 (0.2%) | 5 (12.5%) | <0.01 * |
| COPD (n%) | 22 (3.8%) | 16 (3%) | 6 (15%) | 0.01 * |
| Sensorial Deficits (n%) | 28 (4.9%) | 17 (3.2%) | 11 (27.5%) | <0.01 * |
| Heart Failure | 39 (6.8%) | 19 (3.5%) | 20 (50%) | <0.01 * |
| Variable | Overall (n = 577) | Non-Frail (n = 537) | Frail (n = 40) | p Value |
|---|---|---|---|---|
| Histology | 0.68 | |||
| Serous (n%) | 38 (6.6%) | 35 (6.1%) | 3 (7.5%) | |
| Endometroid (n%) | 491 (85.1%) | 458 (79.4%) | 33 (82.5%) | |
| Clear Cell (n%) | 14 (2.4%) | 11 (2%) | 3 (7.5%) | |
| Carcinosarcoma (n%) | 10 (1.7%) | 9 (1.7%) | 1 (2.5%) | |
| “Mixed” (n%) | 8 (1.4%) | 8 (1.5%) | 0 | |
| Neuroendocrine (n%) | 1 (0.2%) | 1 (0.2%) | 0 | |
| Adenosquamous Carcinoma | 3 (0.5%) | 3 (0.6%) | 0 | |
| Undifferentiated Carcinoma | 4 (0.7%) | 4 (0.7%) | 0 | |
| Adenocarcinoma | 7 (1.2%) | 7 (1.3%) | 0 | |
| Adenosarcoma | 1 (0.2%) | 1 (0.2%) | 0 | |
| Grade | 0.96 | |||
| IA (n%) | 263 (45.6%) | 246 (45.7%) | 17 (42.5%) | |
| IB (n%) | 195 (33.8%) | 181(33.7%) | 14 (35%) | |
| II (n%) | 55 (9.5%) | 50 (9.3%) | 5 (12.5%) | |
| III A (n%) | 11 (1.9%) | 10 (1.9%) | 1 (2.5%) | |
| III B (n%) | 9 (1.55%) | 8 (1.5%) | 1 (2.5%) | |
| III C1 (n%) | 23 (3.9%) | 21 (3.9%) | 2 (5%) | |
| III C2 (n%) | 7 (1.2%) | 7 (1.3%) | 0 | |
| IV A (n%) | 3 (0.5%) | 3 (0.6%) | 0 | |
| IV B (n%) | 11 (1.9%) | 11 (2%) | 0 |
| Variable | Overall (n = 577) | Non-Frail (n = 537) | Frail (n = 40) | p Value |
|---|---|---|---|---|
| Intraoperative Complications | 0.01 * | |||
| Yes (n%) | 12 (2.1%) | 9 (1.7%) | 3 (7.5%) | |
| No (n%) | 565 (98%) | 528 (98.3%) | 33 (82.5%) | |
| Early PC | 0.06 | |||
| Yes (n%) | 43 (7.5%) | 37 (6.9%) | 17 (42.5%) | |
| No (n%) | 534 (92.5%) | 500 (93.1%) | 14 (35%) | |
| Delayed PC | 0.65 | |||
| Yes (n%) | 22 (3.8%) | 21 (3.9%) | 1 (2.5%) | |
| No (n%) | 555 (96.2%) | 516 (96.1%) | 39 (97.5%) |
| Variable | Odd Ratio | 95% CI | SE | p Value |
|---|---|---|---|---|
| Intraoperative Complications | ||||
| Frailty | 4.54 | 1.18–17.60 | 0.69 | 0.028 * |
| Age | 1.07 | 0.95–1.20 | 0.67 | 0.265 |
| BMI | 1.04 | 0.95–1.20 | 0.05 | 0.458 |
| Early PC | ||||
| Frailty | 2.34 | 0.92–6.00 | 0.47 | 0.075 |
| Age | 1.07 | 1.00–1.15 | 0.71 | 0.032 * |
| BMI | 1.04 | 0.98–1.09 | 0.35 | 0.201 |
| Delayed PC | ||||
| Frailty | 0.69 | 0.09–5.28 | 1.04 | 0.719 |
| Age | 0.99 | 0.90–1.01 | 0.05 | 0.902 |
| BMI | 0.47 | 0.90–1.05 | 0.04 | 0.468 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schipa, C.; Ripa, M.; Gallotta, V.; Russo, A.; Polidori, L.; Fanfani, F.; Capomacchia, F.M.; Corrado, G.; Vizza, E.; Perrone, A.M.; et al. Can the Modified Frailty Index (mFI) Predict Intraoperative and Postoperative Complications in Older Women with Endometrial Cancer Undergoing Laparoscopic or Robotic Surgery? A Multicenter Observational Study. J. Clin. Med. 2023, 12, 7205. https://doi.org/10.3390/jcm12237205
Schipa C, Ripa M, Gallotta V, Russo A, Polidori L, Fanfani F, Capomacchia FM, Corrado G, Vizza E, Perrone AM, et al. Can the Modified Frailty Index (mFI) Predict Intraoperative and Postoperative Complications in Older Women with Endometrial Cancer Undergoing Laparoscopic or Robotic Surgery? A Multicenter Observational Study. Journal of Clinical Medicine. 2023; 12(23):7205. https://doi.org/10.3390/jcm12237205
Chicago/Turabian StyleSchipa, Chiara, Matteo Ripa, Valerio Gallotta, Andrea Russo, Lorenzo Polidori, Francesco Fanfani, Filippo Maria Capomacchia, Giacomo Corrado, Enrico Vizza, Anna Myriam Perrone, and et al. 2023. "Can the Modified Frailty Index (mFI) Predict Intraoperative and Postoperative Complications in Older Women with Endometrial Cancer Undergoing Laparoscopic or Robotic Surgery? A Multicenter Observational Study" Journal of Clinical Medicine 12, no. 23: 7205. https://doi.org/10.3390/jcm12237205
APA StyleSchipa, C., Ripa, M., Gallotta, V., Russo, A., Polidori, L., Fanfani, F., Capomacchia, F. M., Corrado, G., Vizza, E., Perrone, A. M., Mereu, L., Cela, V., Legge, F., Hilaris, G., Pasciuto, T., D’Indinosante, M., La Fera, E., Certelli, C., Bruno, V., ... Aceto, P. (2023). Can the Modified Frailty Index (mFI) Predict Intraoperative and Postoperative Complications in Older Women with Endometrial Cancer Undergoing Laparoscopic or Robotic Surgery? A Multicenter Observational Study. Journal of Clinical Medicine, 12(23), 7205. https://doi.org/10.3390/jcm12237205