
Negative Pressure Wound Therapy with Instillation: Analysis of the Rinsing Fluid as a Monitoring Tool and Approach to the Inflammatory Process: A Pilot Study


 and
and
Abstract
1. Introduction
2. Materials and Methods
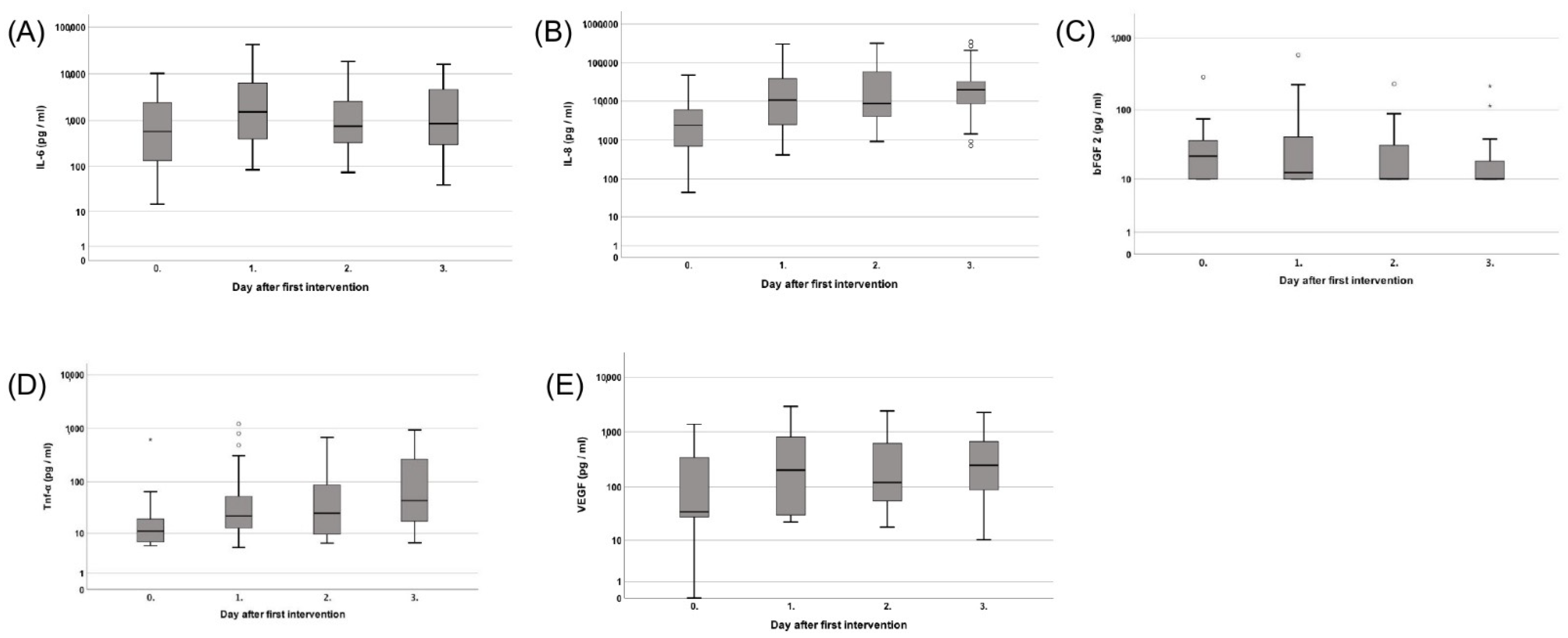
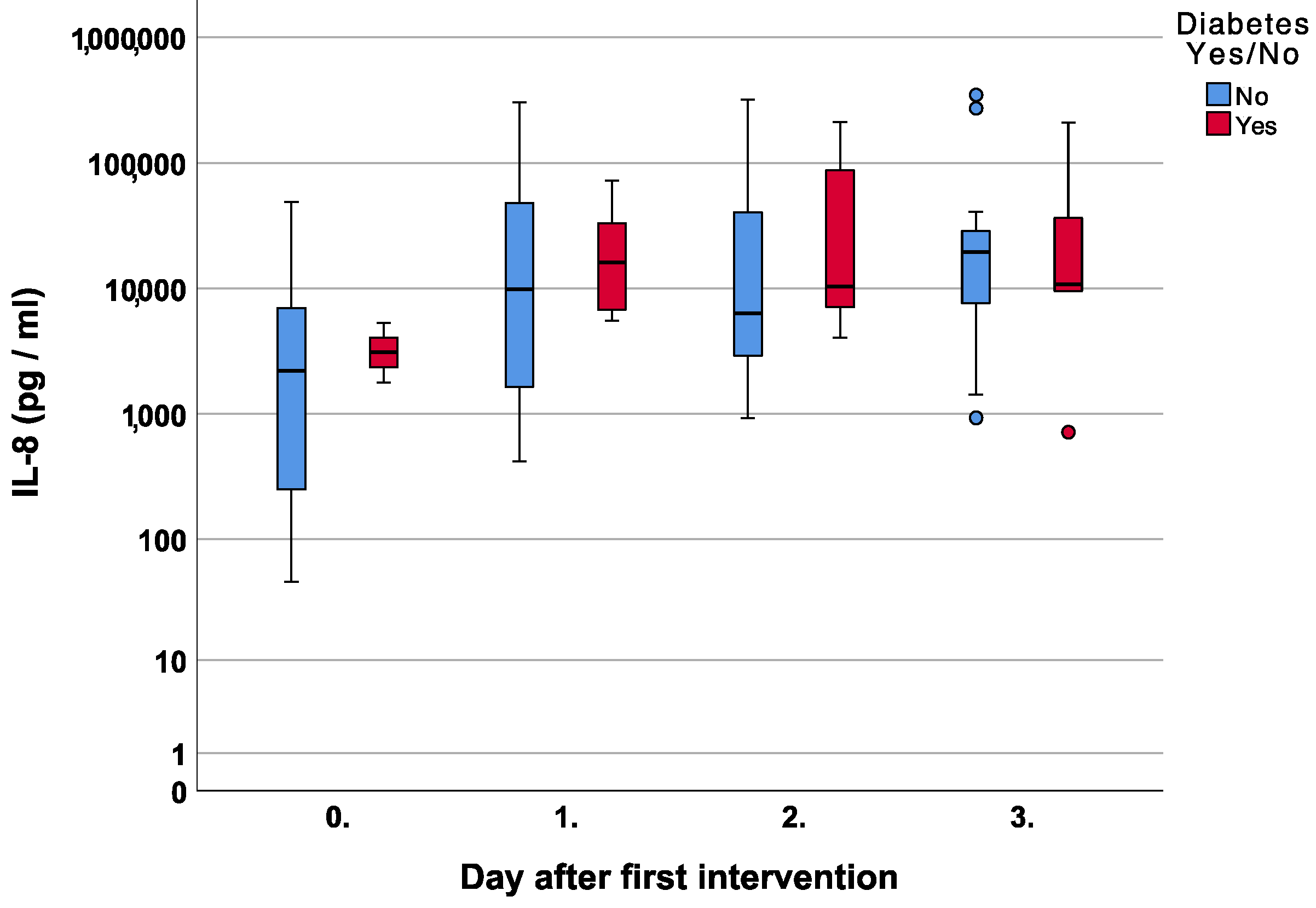
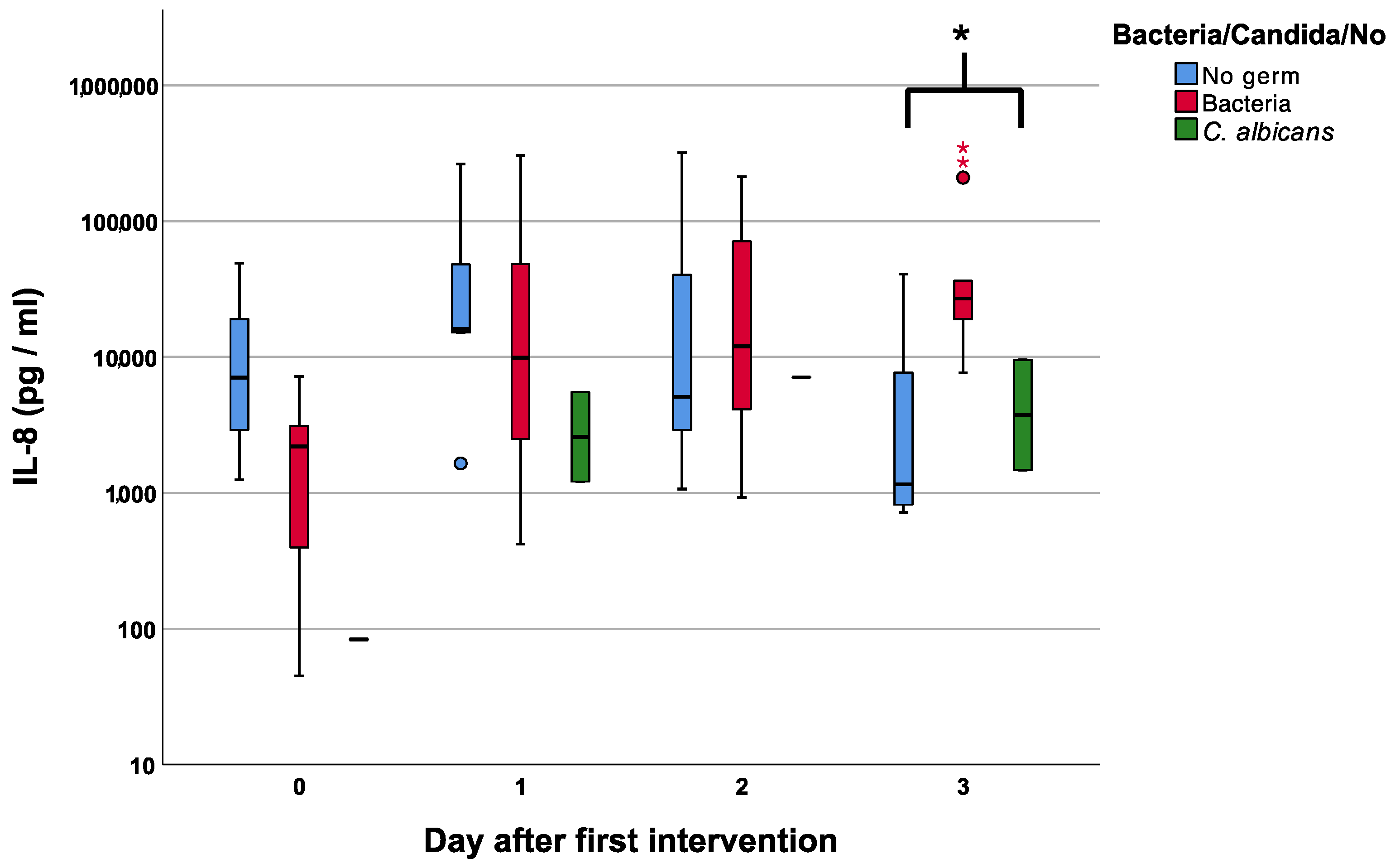
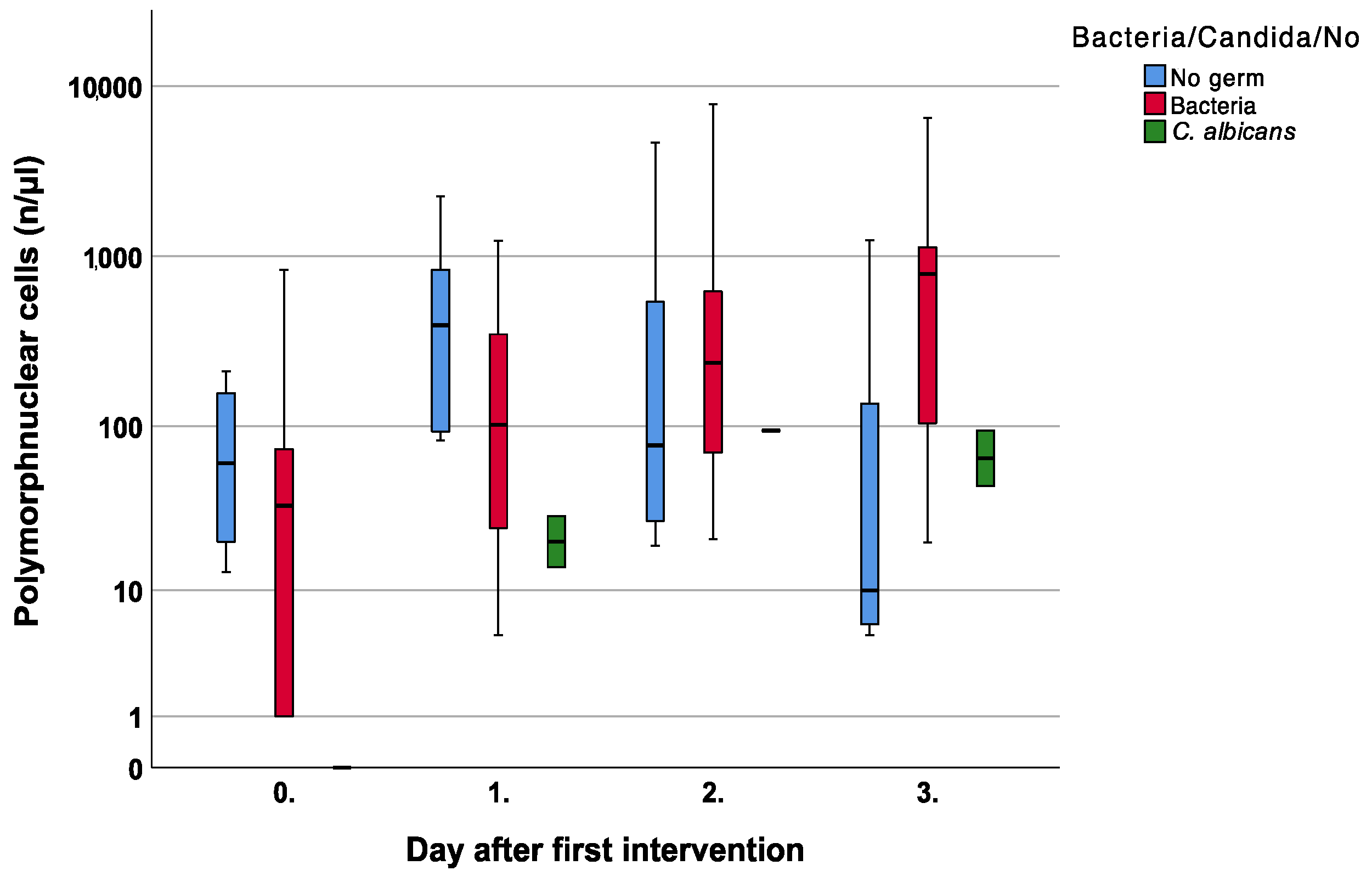
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mousavi, S.-M.; Nejad, Z.M.; Hashemi, S.A.; Salari, M.; Gholami, A.; Ramakrishna, S.; Chiang, W.-H.; Lai, C.W. Bioactive Agent-Loaded Electrospun Nanofiber Membranes for Accelerating Healing Process: A Review. Membranes 2021, 11, 702. [Google Scholar] [CrossRef] [PubMed]
- Mouës, C.M.; Vos, M.C.; Bemd, G.-J.C.M.V.D.; Stijnen, T.; Hovius, S.E.R. Bacterial load in relation to vacuum-assisted closure wound therapy: A prospective randomized trial. Wound Repair Regen. 2004, 12, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Pliakos, I.; Michalopoulos, N.; Papavramidis, T.S.; Arampatzi, S.; Diza-Mataftsi, E.; Papavramidis, S. The Effect of Vacuum-Assisted Closure in Bacterial Clearance of the Infected Abdomen. Surg. Infect. 2014, 15, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Goss, S.G.; Alcantara, S.; Schultz, G.; Ii, J.C.L. Effect of Negative Pressure Wound Therapy With Instillation on Bioburden in Chronically Infected Wounds. Wounds 2017, 29, 240–246. [Google Scholar] [PubMed]
- Bradley, B.H.; Cunningham, M. Biofilms in Chronic Wounds and the Potential Role of Negative Pressure Wound Therapy: An integrative review. J. Wound Ostomy Cont. Nurs. 2013, 40, 143–149. [Google Scholar] [CrossRef]
- Gabriel, A.; Shores, J.; Heinrich, C.; Baqai, W.; Kalina, S.; Sogioka, N.; Gupta, S. Negative pressure wound therapy with instillation: A pilot study describing a new method for treating infected wounds. Int. Wound J. 2008, 5, 399–413. [Google Scholar] [CrossRef] [PubMed]
- Goss, S.; Schwartz, J.; Facchin, F.; Avdagic, E.; Gendics, C.; Lantis, J., 2nd. Negative Pressure Wound Therapy With Instillation (NPWTi) Better Reduces Post-debridement Bioburden in Chronically Infected Lower Extremity Wounds Than NPWT Alone. J. Am. Coll. Clin. Wound Spéc. 2012, 4, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Kairinos, N.; Voogd, A.M.; Botha, P.H.; Kotze, T.; Kahn, D.; Hudson, D.A.; Solomons, M. Negative-Pressure Wound Therapy II: Negative-Pressure Wound Therapy and Increased Perfusion. Just an Illusion? Plast. Reconstr. Surg. 2009, 123, 601–612. [Google Scholar] [CrossRef]
- Kairinos, N.; Solomons, M.; Hudson, D.A. Negative-Pressure Wound Therapy I: The Paradox of Negative-Pressure Wound Therapy. Plast. Reconstr. Surg. 2009, 123, 589–598; discussion 599–600. [Google Scholar] [CrossRef]
- Kairinos, N.; Mc Kune, A.; Solomons, M.; Hudson, D.A.; Kahn, D. The flaws of laser Doppler in negative-pressure wound therapy research. Wound Repair Regen. 2014, 22, 424–429. [Google Scholar] [CrossRef]
- Kairinos, N.; Holmes, W.J.M.; Solomons, M.; Hudson, D.A.; Kahn, D. Does a Zone of Increased Perfusion Exist around Negative-Pressure Dressings? Plast. Reconstr. Surg. 2013, 132, 978–987. [Google Scholar] [CrossRef] [PubMed]
- Derrick, K.L.; Lessing, M.C. Genomic and Proteomic Evaluation of Tissue Quality of Porcine Wounds Treated With Negative Pressure Wound Therapy in Continuous, Noncontinuous, and Instillation Modes. Eplasty 2014, 14, e43. [Google Scholar] [PubMed]
- Li, X.; Liu, J.; Liu, Y.; Hu, X.; Dong, M.; Wang, H.; Hu, D. Negative pressure wound therapy accelerates rats diabetic wound by promoting agenesis. Int. J. Clin. Exp. Med. 2015, 8, 3506–3513. [Google Scholar] [PubMed]
- Wynn, M.; Freeman, S. The efficacy of negative pressure wound therapy for diabetic foot ulcers: A systematised review. J. Tissue Viability 2019, 28, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Polykandriotis, E.; Horch, R.E.; Jost, M.; Arkudas, A.; Kees, F.; Schmitz, M. Can systemically administered antibiotics be detected in wound tissues and surfaces under negative pressure wound therapy? Int. Wound J. 2019, 16, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Taeger, C.; Wallner, S.; Martini, T.; Schiltz, D.; Kehrer, A.; Prantl, L.; Biermann, N. Analysis of Rinsing Fluid during Negative Pressure Wound Therapy with Instillation: A Potential Monitoring Tool in Acute and Chronic Wound Treatment. A Pilot Study. Cells 2021, 10, 732. [Google Scholar] [CrossRef] [PubMed]
- Mouës, C.M.; Van Toorenenbergen, A.W.; Heule, F.; Hop, W.C.; Hovius, S.E.R. The role of topical negative pressure in wound repair: Expression of biochemical markers in wound fluid during wound healing. Wound Repair Regen. 2008, 16, 488–494. [Google Scholar] [CrossRef]
- Faes, S.; Hübner, M.; Demartines, N.; Hahnloser, D. Cytokine clearance in serum and peritoneal fluid of patients undergoing damage control surgery with abdominal negative pressure therapy for abdominal sepsis. Pleura Peritoneum 2021, 6, 31–38. [Google Scholar] [CrossRef]
- Jiang, W.G.; Sanders, A.J.; Ruge, F.; Harding, K.G. Influence of interleukin-8 (IL-8) and IL-8 receptors on the migration of human keratinocytes, the role of PLC-γ and potential clinical implications. Exp. Ther. Med. 2012, 3, 231–236. [Google Scholar] [CrossRef]
- Rennekampff, H.O.; Hansbrough, J.F.; Kiessig, V.; Dore, C.; Sticherling, M.; Schroder, J.M. Bioactive interleukin-8 is expressed in wounds and enhances wound healing. J. Surg. Res. 2000, 93, 41–54. [Google Scholar] [CrossRef]
- Meng, L.; Guo, X.; Yang, X.; Liu, H.; Yu, M.; Wu, Y.; Zhu, Z. Human α defensins promote the expression of the inflammatory cytokine interleukin-8 under high-glucose conditions: Novel insights into the poor healing of diabetic foot ulcers. J. Biochem. Mol. Toxicol. 2019, 33, e22351. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, R.M.; Simeonova, P.P.; Matheson, J.M.; Kommineni, C.; Guriel, J.L.; Sugawara, T.; Luster, M.I. Impaired cutaneous wound healing in interleukin-6-deficient and immunosuppressed mice. FASEB J. 2000, 14, 2525–2531. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, R.M.; Sugawara, T.; Yucesoy, B.; Berryann, K.; Simeonova, P.P.; Matheson, J.M.; Luster, M.I. Interleukin-6 Treatment Augments Cutaneous Wound Healing in Immunosuppressed Mice. J. Interf. Cytokine Res. 2001, 21, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.G.; Luckett-Chastain, L.R.; Calhoun, K.N.; Frempah, B.; Bastian, A.; Gallucci, R.M. Interleukin 6 Function in the Skin and Isolated Keratinocytes Is Modulated by Hyperglycemia. J. Immunol. Res. 2019, 2019, 5087847. [Google Scholar] [CrossRef] [PubMed]
- Blann, A.D.; Belgore, F.M.; McCOLLUM, C.N.; Silverman, S.; Lip, P.L.; Lip, G.Y.H. Vascular endothelial growth factor and its receptor, Flt-1, in the plasma of patients with coronary or peripheral atherosclerosis, or Type II diabetes. Clin. Sci. 2002, 102, 187–194. [Google Scholar] [CrossRef]
- Kikuchi, R.; Nakamura, K.; MacLauchlan, S.; Ngo, D.T.-M.; Shimizu, I.; Fuster, J.J.; Katanasaka, Y.; Yoshida, S.; Qiu, Y.; Yamaguchi, T.P.; et al. An antiangiogenic isoform of VEGF-A contributes to impaired vascularization in peripheral artery disease. Nat. Med. 2014, 20, 1464–1471. [Google Scholar] [CrossRef]
- Xuan, Y.H.; Bin Huang, B.; Tian, H.S.; Chi, L.S.; Duan, Y.M.; Wang, X.; Zhu, Z.X.; Cai, W.H.; Zhu, Y.T.; Wei, T.M.; et al. High-Glucose Inhibits Human Fibroblast Cell Migration in Wound Healing via Repression of bFGF-Regulating JNK Phosphorylation. PLoS ONE 2014, 9, e108182. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, M.F.; Li, J.; Chehab, L.; Desta, T.; Chino, T.; Krothpali, N.; Behl, Y.; Alikhani, M.; Yang, J.; Braasch, C.; et al. Impaired wound healing in mouse models of diabetes is mediated by TNF-α dysregulation and associated with enhanced activation of forkhead box O1 (FOXO1). Diabetologia 2010, 53, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Fahey, T.J.; Turbeville, T.; McIntyre, K. Differential TNF Secretion by Wound Fibroblasts Compared to Normal Fibroblasts in Response to LPS. J. Surg. Res. 1995, 58, 759–764. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | |||
| Sex | Male n = 20 | Female n = 11 | |
| Reason | Chronic n = 23 Ischemic n = 2 Post-traumatic/post-infection n = 12 Decubital ulceration n = 6 Carcinoma-associated n = 3 Diabetes = 6 Peripheral Artery Disease = 8 | Acute n= 8 Traumatic n = 4 Ischemic/compartment n = 3 Burns n = 1 | |
| Microbiological contamination | Bacteria S. aureus n = 10 MRSA n = 2 S. epidermidis n = 4 S.pyogenes n = 2 S. anginosus/massilensis n = 1 E. coli n = 3 E. faecalis n = 6 P. aeruginosa n = 3 Proteus spp. n = 4 Klepsiella spp. n = 2 Polymicrobial (≤2) n = 5 Polymicrobial (≥3) n = 2 | Fungus Candida albicans n = 3 | No contamination n = 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biermann, N.; Wallner, S.; Martini, T.; Spoerl, S.; Prantl, L.; Taeger, C.D. Negative Pressure Wound Therapy with Instillation: Analysis of the Rinsing Fluid as a Monitoring Tool and Approach to the Inflammatory Process: A Pilot Study. J. Clin. Med. 2023, 12, 711. https://doi.org/10.3390/jcm12020711
Biermann N, Wallner S, Martini T, Spoerl S, Prantl L, Taeger CD. Negative Pressure Wound Therapy with Instillation: Analysis of the Rinsing Fluid as a Monitoring Tool and Approach to the Inflammatory Process: A Pilot Study. Journal of Clinical Medicine. 2023; 12(2):711. https://doi.org/10.3390/jcm12020711
Chicago/Turabian StyleBiermann, Niklas, Stefan Wallner, Teresa Martini, Steffen Spoerl, Lukas Prantl, and Christian D. Taeger. 2023. "Negative Pressure Wound Therapy with Instillation: Analysis of the Rinsing Fluid as a Monitoring Tool and Approach to the Inflammatory Process: A Pilot Study" Journal of Clinical Medicine 12, no. 2: 711. https://doi.org/10.3390/jcm12020711
APA StyleBiermann, N., Wallner, S., Martini, T., Spoerl, S., Prantl, L., & Taeger, C. D. (2023). Negative Pressure Wound Therapy with Instillation: Analysis of the Rinsing Fluid as a Monitoring Tool and Approach to the Inflammatory Process: A Pilot Study. Journal of Clinical Medicine, 12(2), 711. https://doi.org/10.3390/jcm12020711